
Abstract
The aim of the study was to evaluate selected angiogenic factors in patients with essential thrombocythemia (ET) depending on JAK2V617F, calreticulin gene (CALR) and myeloproliferative leukemia virus oncogene (MPL) mutations. Sixty ET patients and 20 healthy volunteers were enrolled in the study. The following tests were performed: vascular endothelial growth factor- A (VEGF-A), soluble vascular endothelial growth factor receptor-1 (sVEGFR-1),soluble vascular endothelial growth factor receptor-2 (sVEGFR-2), platelet-derived growth factor( PDGF-BB), and stromal-derived factor-1α (SDF-1α). We observed an increased PDGF-BB level in patients with ET compared to the controls. Patients with CALR mutation had significantly higher concentration of PDGF-BB and lower concentration of SDF-1α than patients with JAK2V617F mutation. High concentration of PDGF-BB and low concentration of SDF-1α in patients with CALR(+) ET may indicate a contribution of these chemokines in disturbed Ca2+ metabolism in platelets.
Introduction
The JAK2V617F mutation, discovered in 2005, has become one of the major criteria for diagnosis of myeloproliferative neoplasms Philadelphia negative. Janus kinase 2 (JAK2) consists of a pseudokinase domain (JH2) and a tyrosine kinase domain (JH1). Physiological function of the JH2 domain is an inhibition of catalytic activity of JH1 domain. JAK2V617F mutation is associated with the substitution of valine for phenylalanine at position 617 located in the pseudokinase JH2 domain. JAK2V617F mutation leads to constitutive activation of JAK-STAT signaling pathway that results in uncontrolled proliferation of hematopoietic stem cells. JAK2V617F mutation is found in ∼95% of patients with polycythemia vera, whereas it occurs in only half of patients with essential thrombocythemia (ET) and primary myelofibrosis (PMF). 1
About 5% of patients with JAK2V617F(−) ET present other mutations: MPLW515K and W515L. Both mutations, W515K and W515L lead to constitutive activation of thrombopoietin receptor protein, which results in the overproduction of abnormal megakaryocytes and an increased number of platelets. 2 MPL mutations are much less prevalent but more specific than JAK2V617F in ET and PMF.
Recently, new somatic mutations in calreticulin gene (CALR) in JAK2V617F(−) and MPL(−) patients were identified. CALR mutations were first discovered in patients with ET by Nangalia et al 3 and Klampfl et al 4 in 2013. According to studies conducted by Rotunno et al and Rumi et al, CALR mutations were identified in 15.5% of patients with ET and in 22.7% of patients with PMF. 5,6 For this reason, CALR mutation seems to be the second, after JAK2V617F, most prevalent acquired nucleotide change in these 2 myeloproliferative neoplasms.
At present, biological significance of calreticulin mutations remains unknown. Rotunno et al found that patients with CALR(+) ET have lower values of hemoglobin (HGB) and white blood cells as well as lower risk of thrombosis, despite significantly higher platelet counts compared to patients with JAK2V617F(+) or MPL(+).
The relationship between JAK2V617F mutation and increased level of VEGF, the major stimulator of bone marrow angiogenesis in myeloproliferative neoplasms, is well established. Contrary to JAK2V617F mutation, the connection between CALR mutations and angiogenesis remains still unknown and requires elucidation. The aim of the study was to evaluate selected angiogenic factors in patients with ET depending on JAK2V617F, CALR, and MPL mutations.
Materials and Methods
Between 2010 and 2015, 60 patients with ET (mean age: 61 years) were recruited from a Department of Hematology and Malignant Diseases of Hematopoietic System, University Hospital No. 2 in Bydgoszcz, Poland. Essential thrombocythemia was diagnosed according to the World Health Organization (2008) criteria 7 and the exclusion of other malignant and nonmalignant diseases manifesting with thrombocythemia. Additional exclusion criteria were as follows: newly diagnosed thrombosis, New York Heart Association (NYHA) functional class III-IV, type 1 or type 2 diabetes, and pregnancy. All patients were newly diagnosed and previously untreated with cytoreductive drugs. The control group consisted of 20 healthy volunteers (mean age: 47 years).
The study was approved by the Bioethics Committee of Collegium Medicum in Bydgoszcz, the Nicolaus Copernicus University in Toruń. The written informed consent was obtained from all participants.
Blood Collection
Blood samples were taken from an antecubital vein, after overnight fasting, into 2 tubes containing EDTA 2 K (plasma) and clot activator (serum). Samples were centrifuged at 3000 rev/min for 20 minutes at 4°C. The obtained plasma and serum were divided into aliquots and stored at −80°C until analysis, but not longer than 6 months. Peripheral blood counts were performed on Advia 120 hematology analyzer (Siemens).
Enzyme-Linked Immunosorbent Assays
In serum, the following tests were performed using the immunoenzymatic method: concentration of VEGF-A, sVEGFR-1, sVEGFR-2, and PDGF-BB (R&D Systems, Inc, Minneapolis, Minnesota). Concentration of SDF-1α was measured in plasma using enzyme-linked immunosorbent assays kit (R&D Systems, Inc).
JAK2 V617F and MPL W515K/L Mutation Analysis
The JAK2V617F and MPLW515K/L mutations were detected using allele-specific polymerase chain reaction (PCR) (ang. allele-specific PCR amplification [AS-PCR]). Genomic DNA was isolated from peripheral blood (QIAamp DNA Mini Kit; Qiagen, Hilden, Germany)) of all patients. The JAK2V617F PCR reaction was performed using 100 ng of DNA, according to the method of Baxter et al. 8 The products of AS-PCR reaction were 203 bp (V617F mutation) and 364 bp (internal control) in length. The MPLW515K/L mutations were screened by 2 allele-specific PCR reactions (the first for MPLW515 K and the second for MPLW515 L). Wild-type (internal control) PCR products were 218 bp, while additional PCR product of 176-bp length indicated W515K or W515L mutation.
CALR Mutation Analysis
The CALR exon 9 was screened for insertion and deletion mutations by direct sequencing. Polymerase chain reaction amplifications were performed with 100 ng of genomic DNA, using primers according to Klampfl et al. 4 The PCR products were sequenced with Applied Biosystems (ABI) 3130 genetic analyzer. Received electropherograms were compared to reference sequence of CALR gene (NC_000019.10).
Statistical Analysis
The statistical analysis was performed with the use of Statistica 10.1 software (StatStoft, Kraków, Poland)). The Shapiro-Wilk test was used to assess the normality of the distribution. For the parameters with a normal distribution, arithmetic mean (X) and standard deviation were determined, and the parameters with the nonnormal distribution were presented as a median (Me) and quartiles: lower (Q1) and upper (Q3). Student t test or Mann-Whitney U test was used to compare the differences between 2 groups. Kruskal-Wallis analysis of variance was used for multiple group comparison. The P values <.05 were considered significant.
Results
VEGF-A level was significantly higher in patients with ET (mean age: 60 years) in comparison to the control group (mean age: 47 years; Me = 104.65 vs Me = 26.87; P = .000003); however, sVEGFR-2 concentration was significantly lower in patients with ET (Me = 8240.99 vs Me = 10693.09; P = .000028). We also observed an increased PDGF-BB level in patients with ET compared to the controls (Me = 321.6 vs Me = 178.90; P = .032830; Table 1).
Selected Angiogenic Factors in Patients With Essential Thrombocythemia in Comparison to the Control Group.
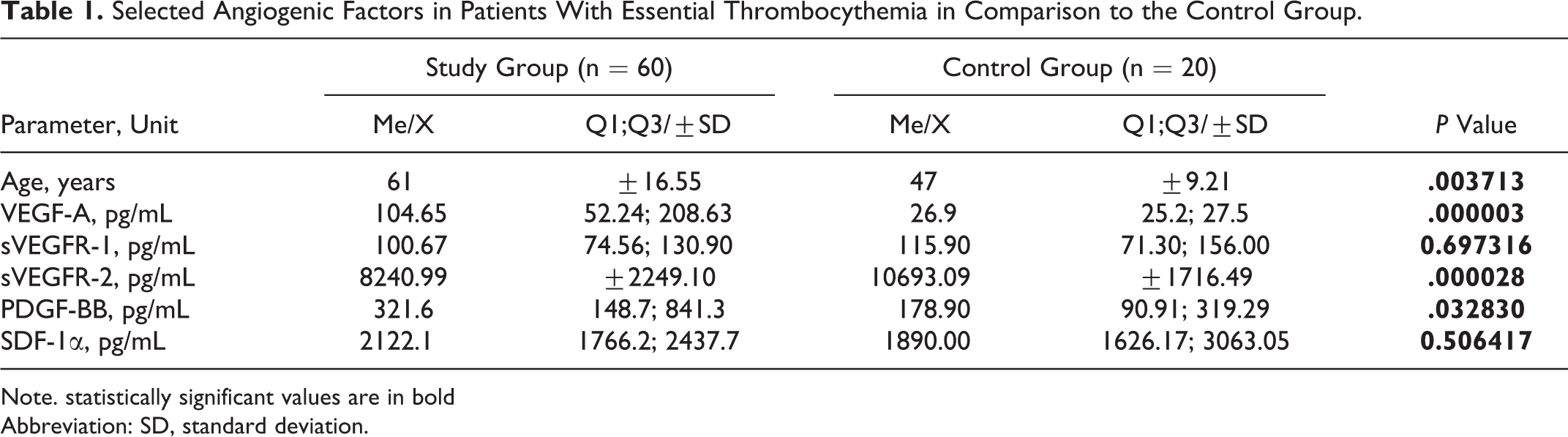
Note. statistically significant values are in bold
Abbreviation: SD, standard deviation.
JAK2V617F mutation was found in 37 (61.7%) patients with ET. Among 23 patients without JAK2V617F mutation, 7 (11.7%) had CALR mutation and 1 (1.7%) had MPL mutation. Fifteen (25.0%) patients were negative for all 3 mutations: JAK2V617F(−), CALR(−), and MPL(−).
Table 2 shows clinical characteristics of patients with ET depending on the mutations identified at diagnosis. Mean age in the group of patients with JAK2617F mutation was similar to the one observed in the group of patients with CALR mutation. Triple mutation-negative patients were younger than other patients, but without statistical significance. A comparison of interview data indicates that thrombotic events were most common in patients with JAK2 V617F mutation (32.4%) than in other groups of patients (Table 2).
Clinical and Laboratory Characteristics at Diagnosis of Patients With Essential Thrombocythemia According to Type of Mutation.
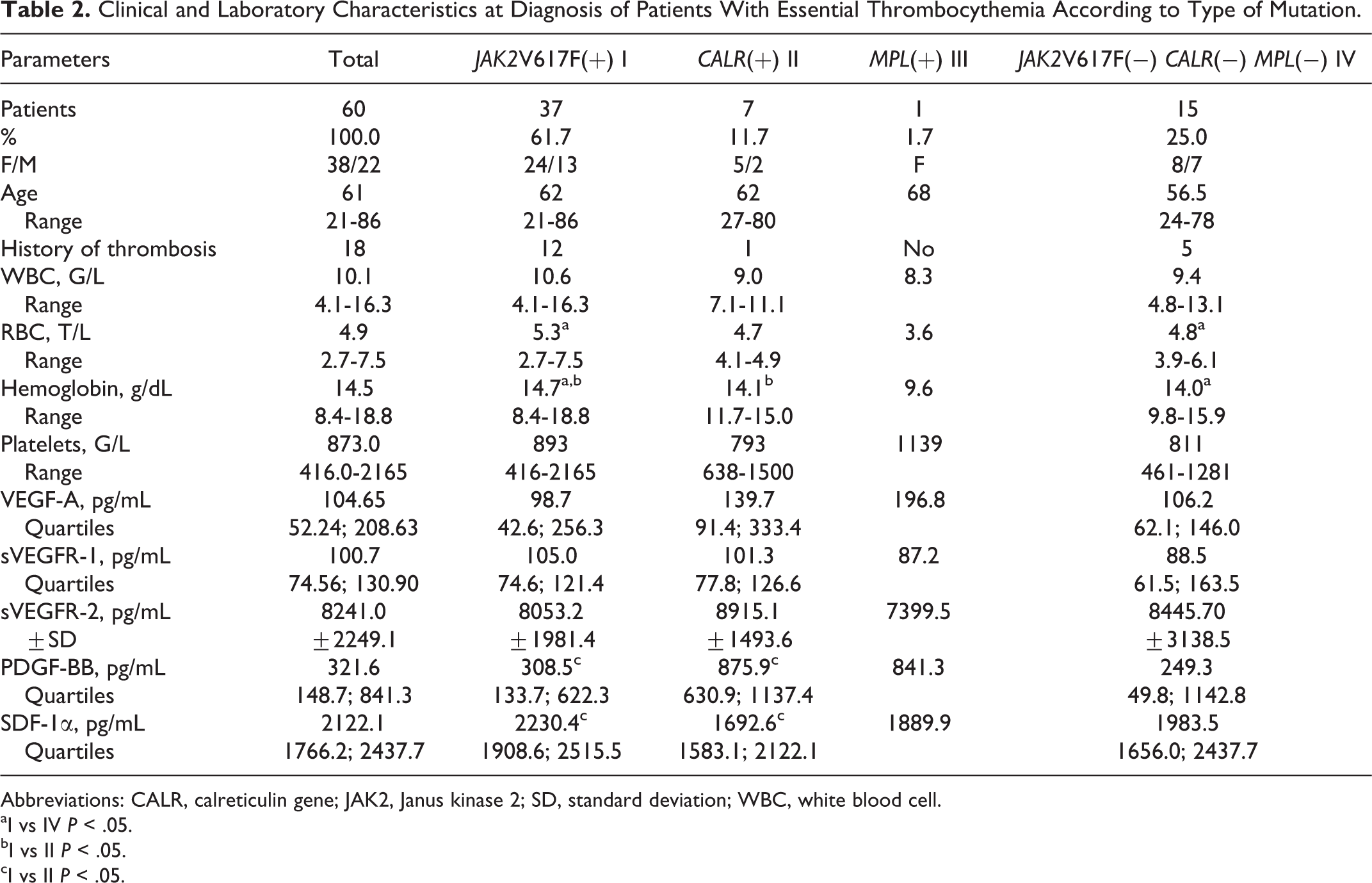
Abbreviations: CALR, calreticulin gene; JAK2, Janus kinase 2; SD, standard deviation; WBC, white blood cell.
aI vs IV P < .05.
bI vs II P < .05.
cI vs II P < .05.
The analysis of hematologic parameters showed significantly higher number of red blood cells (RBCs) and HGB concentration in patients with JAK2V617F mutation compared to the group of triple negative patients. Hemoglobin concentration was also significantly higher in JAK2V617F(+) patients compared to the CALR(+) (Table 2). White blood cell was also higher in JAK2V617F(+) group than in other groups but without statistical significance.
According to Table 2, patients with CALR mutation had significantly higher concentration of PDGF-BB and lower concentration of SDF-1α than patients with JAK2V617F mutation. PDGF-BB concentration was also much lower in triple negative group than in JAK2V617F(+), but without statistical significance.
Discussion
In the present study, the concentrations of proangiogenic parameters such as VEGF-A, PDGF-BB, and SDF-1α and the levels of soluble receptors sVEGFR-1 and sVEGFR-2 (with antiangiogenic properties) were assessed. We observed increased VEGF-A levels in the blood of patients with ET, which is consistent with the values obtained by Treliński et al. 9 Moreover, we noticed that sVEGFR-2 concentration in patients with ET was significantly lower than in the control group. A similar research was conducted by Treliński et al, but they found no significant difference in sVEGFR2 levels between group of patients with ET and controls. 9 What’s more, in our study, we found a significantly higher level of PDGF-BB in patients with ET as compared to the control group. Lev et al showed increased PDGF concentration in the blood of 15 patients with ET, which was normalized in remission after using anagrelide. 10 Gersuk et al observed higher level of PDGF in platelet-poor plasma and in urine of 5 patients with ET. 11
In the present study, angiogenic factors were analyzed in ET according to the presence or absence of JAK2V617F, as well as CALR and MPL mutations. There were no significant differences in VEGF-A, sVEGFR-1, and sVEGFR-2 concentrations between all subgroups. In CALR(+) patients, we found almost 3-fold higher concentration of PDGF-BB and substantially lower SDF-1α concentration than in patients with JAK2V617F.
Calreticulin is present on the surface of platelets where it regulates Ca2+ homeostasis and the endoplasmic reticulum stress response, which is an important phenomenon during the maturation of megakaryocytes and platelets. The antibodies against calreticulin cause platelet activation and aggregation. 12,13
A spontaneous CALR mutation causes defective structure and function of calreticulin concerning predominantly calcium metabolism. It has been shown that overexpression of calreticulin can lead to increased accumulation of intracellular Ca2+, while calreticulin deficiency is associated with lower calcium-binding capacity. 14,15 Predictably, patients with ET with CALR mutation have reduced calcium level in platelets, which leads to their dysfunction in the process of hemostasis (disturbed adhesion and aggregation).
High concentration of PDGF-BB, produced mainly by platelets, can also be related to CALR mutations. Studies on the pathogenesis of myeloproliferative neoplasms indicate that PDGF participates in the creation of fibrous connective tissue in the course of PMF. 16 Nangalia et al observed that patients with ET with somatic CALR mutation have significantly higher frequency of transformation to PMF than patients with ET with JAK2V617F mutation. 3 It is possible that PDGF-BB may be involved in the process of transformation to myelofibrosis. However, further studies are needed to confirm this hypothesis.
In the present study, we found substantially lower concentration of SDF-1α in patients with ET with a CALR mutation. Lane et al have shown that SDF-1α is responsible for the transendothelial migration of mature megakaryocytes, which contributes to increased production of blood platelets. Mature platelets receive SDF-1α from megakaryocytes and release this chemokine into the blood after cell stimulation. 17
The significantly lower SDF-1α concentration in the blood of patients with CALR(+) ET compared to patients with JAK2V617F(+) may indicate additional abnormality of platelet related to somatic mutation of CALR. The lower concentration of SDF-1α may result from reduced content of this chemokine in α granules or its impaired activity. Previous studies by Roland et al and Henschler et al indicate the involvement of the SDF-1α in inducing transient changes of intracellular calcium concentrations by CXCR4 receptor, which has an impact on migration of hematopoietic stem and progenitor cells. 18,19 A limitation of the current study is a relatively small number of patients with ET and thus even smaller number of patients with CALR mutation.
Conclusions
High concentration of PDGF-BB and low concentration of SDF-1α in patients with CALR(+) ET may indicate a contribution of these chemokines in disturbed Ca2+metabolism in platelets.
Footnotes
Authors’ Note
GG contributed to study design, data analysis, and final revision. JB contributed to analysis and interpretation of data, drafting the article, and final approval of the version to be submitted. KZ contributed to acquisition of data, statistical analysis, and data interpretation. ABK contributed to laboratory analysis and data interpretation. KM contributed to laboratory analysis and data interpretation. OH contributed to final approval and drafting the article. DR contributed to the concept and design of the study, drafting the article, and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.