
Abstract
Brucellosis is a multisystem disease with a broad spectrum of clinical manifestations; hematological abnormalities ranging from fulminant as of disseminated intravascular coagulation (DIC) to anaemia, leucopoenia, thrombocytopenia, and clotting disorders. In this report, we present DIC in a case of brucellosis because of rare presentation. A 3-year-old boy was admitted with the complaints of continuous fever, vomiting, abdominal pain, and bruise on leg. He looked pale and his physical examination revealed purpuric skin lesions on both legs. A mild hepatosplenomegaly was noted on palpation. Laboratory tests showed hematocrit 21%, hemoglobin 7 g/dL, platelet count 20,000/mm3, prothrombin time 19 seconds, activated partial thromboplastin time 48 seconds, plasma fibrinogen level 20 mg/dL, and
Introduction
Brucellosis remains an important public health problem in Turkey and it can affect people at any age, including children, representing 20% to 25% of cases. 1 In most of the children with brucellosis, the isolated bacteria is Brucella melitensis, which is endemic in Turkey. 2 Human infection with Brucella species shows several patterns of presentation, and the majority of patients have normal hematological features. Although pancytopenia may occur in the presence of hepatomegaly, splenomegaly, lymphadenopathy, and fever, the degree of this abnormality is usually mild. 3 Brucella infection as a causative agent of disseminated intravascular coagulation (DIC) has been a few reported in the literature.3–5
In this report, we present DIC in a case of brucellosis because of rare presentation. According to our knowledge, this is the first pediatric case reporting brucellosis associated with DIC.
Case Report
A 3-year-old boy was admitted to our medical unit with a 5-day history of continuous fever, vomiting, abdominal pain, and bruise on leg. On personal history, we learned that living in rural area, consumption of unpasteurized dairy products, and contact with infected animals are the main routes of infection.
On physical examination, body temperature was 39°C, blood pressure 90/70 mm Hg, and heart rate 104 beats per minute (bpm). He looked acutely ill and pale, and his physical examination revealed purpuric skin lesions on both legs. A mild hepatosplenomegaly was noted on palpation. Laboratory tests showed the following values: hematocrit 21% (normal range: 35%-45%); hemoglobin 7 g/dL (normal range: 11.5-15.5 g/dL); white blood cells 2 × 109/mm3 (normal range: 5.5-15.5 × 109 /mm3); platelet count 20,000 × 109/mm3 (normal range: 150-450 × 109/mm3); prothrombin time 19 seconds (normal range: 11-14 seconds); and activated partial thromboplastin time 48 seconds (normal range: 31-40 seconds). Plasma fibrinogen level was 20 mg/dL (200-400 mg/dL).
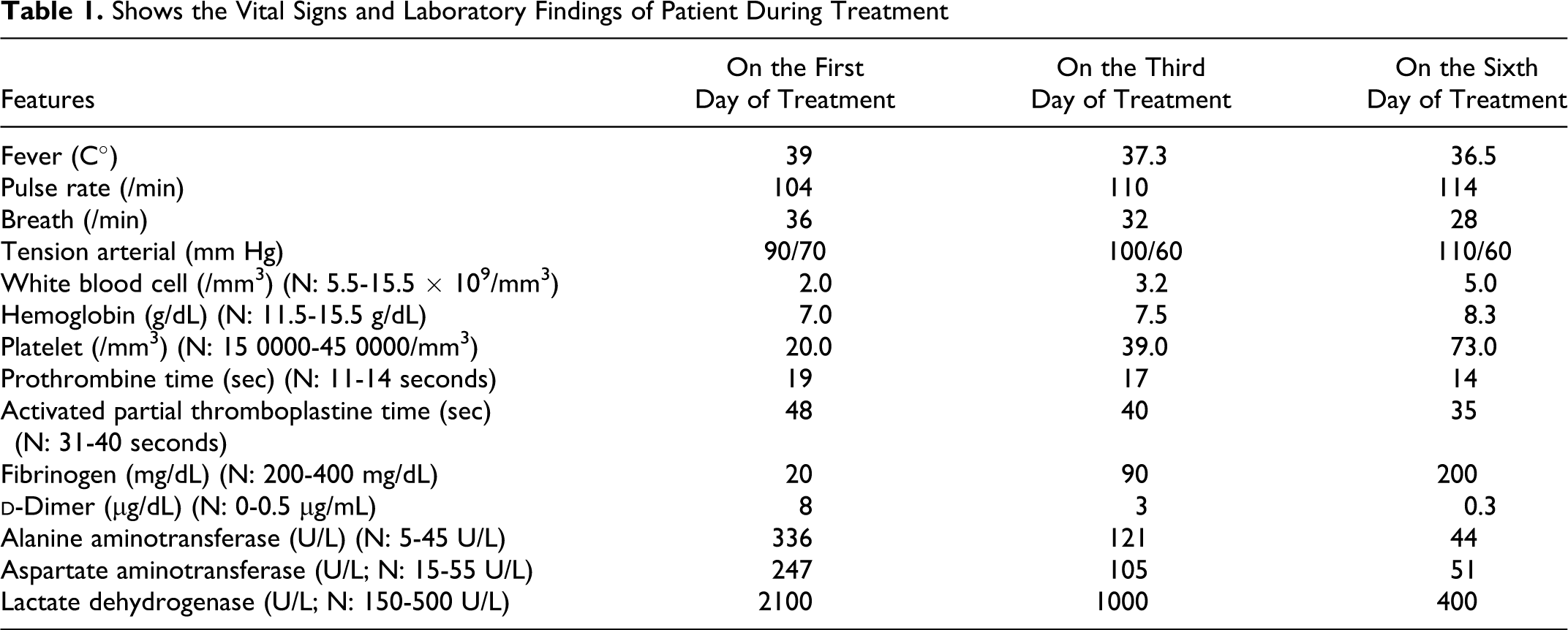
The patient was started on a combination of rifampisin (20 mg/kg per day) and trimethoprim-sulfamethoxazole (trimethoprim 10 mg/kg per day) for brucellosis. In addition, he received platelet transfusion and fresh-frozen plasma. Three days later, the platelet count had increased. There was clinical improvement and remission of fever and echimotic lesion. The vital signs and laboratory findings of patient during treatment are given in Table 1. Serum
Shows the Vital Signs and Laboratory Findings of Patient During Treatment
Discussion
Brucellosis is a multisystem disease with a broad spectrum of clinical manifestations; hematological abnormalities ranging from fulminant as of disseminated intravascular coagulation to anemia, leucopoenia, thrombocytopenia, and clotting disorders. 6
Disseminated intravascular coagulation (DIC) is common in patients with bacterial septicemia; however, it is rare in patients with brucellosis.
4
Bacterial products such as endotoxin can cause endothelial damage or bind to platelets, causing them to aggregate and be removed from the circulation.
7
Moreover, the presence of platelet-associated antibodies has been documented in patients with septicemia and thrombocytopenia in the absence of overt DIC.
8
Coagulopathy and purpura are especially common in meningococcemia, perhaps because of the greater propensity for meningococcal endotoxin to elicit the dermal Shwartzman reaction.9,10 However, brucella endotoxin appears to be less toxic than are lipopolysaccharides from other gram-negative bacteria, and it does not induce the Shwartzman reaction.
11
Another possible examination is hypercytokinemia. In recent years, some patients with DIC, in which hypercytokinemia plays a main role, have been reported.12,13 Interferon γ (IFN-γ), which is released by activated T cells, and tumor necrosis factor α (TNF-α), which is released by macrophages activated by IFNγ, play an important role in the host’s protective mechanism against infection.
14
TNF-α, granulocyte-colony-stimulating factor (G-CSF), macrophage-colony-stimulating factor, and IFN-γ levels were increased in the acute stage in patients with infection. In recent years, some patients with severe infection complicated by hemophagocytic syndrome (HPS), in which hypercytokinemia plays a main role, have been reported.
15
Furthermore, a high level of IFN promotes the growth of infection agents.
16
Therefore, excessive production of cytokines (ie, the presence of hypercytokinemia) may contribute to exacerbation of disease severity and development of DIC. In our patient, we could not determine the cytokine level due to laboratory difficulties. But, we think that in patients with brucella infection and DIC, hypercytokinemia may be an explanation of DIC development and disease severity. Our patient had a dramatic onset of brucella sepsis with clinical and hematological features of DIC, as indicated by the prolonged prothrombin and activated partial thromboplastin time, low fibrinogen, and elevated
In conclusion, diagnosis of brucellosis may be delayed, particularly if uncommon features such as pancytopenia and DIC are present. So, brucellosis must be considered in the differential diagnosis of conditions leading to pancytopenia and DIC in areas endemic for brucellosis.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.