
Abstract
The aim of this study is to evaluate the plasma total homocysteine level in patients with venous thromboembolism (VTE) and to investigate the effect of different risk factors on plasma levels. Ninety-three-patients with VTE and 37-control participants diagnosed with other than VTE were included in the study. Plasma homocysteine levels and the factors affecting plasma homocysteine levels were evaluated. Plasma homocysteine level was higher among patients with VTE compared to the controls independent from vitamin B12 and folate levels. The prevalence of hyperhomocysteinemia in VTE was 63%. Plasma homocysteine level was higher in patients with PE than deep venous thrombosis (DVT; 23 ± 13.7 vs 16 ± 5.8 μmol/L, P = .018). With regression analysis hyperhomocysteinemia was found to be associated with a 4.8-fold increased risk of VTE. Hyperhomocysteinemia is a common and possibly modifiable risk factor that should be considered when screening patients with VTE. Secondary causes of hyperhomocysteinemia especially vitamin B12 deficiency should be monitored in patients with VTE to prevent recurrences.
Introduction
Venous thromboembolism (VTE) including deep venous thrombosis (DVT) and pulmonary embolism (PE) is a frequent disorder. The average annual incidence of VTE is approximately 100 per 100 000 person-years with about 250 000 incident cases annually in the United States. 1,2 Approximately one third of the patients with symptomatic VTE have pulmonary embolism, while two-thirds manifest with DVT alone. 3 The natural prognosis of untreated VTE is poor, especially in patients with PE. Although the introduction of anticoagulant therapy significantly reduced the mortality and morbidity due to VTE, long-term follow-up studies indicate an increased risk of mortality in VTE up to 6 months after initial diagnosis. 4
There are numerous risk factors of VTE including acquired risk factors such as surgery, cancer/cancer therapy or pregnancy, and inherited risk factors such as antithrombin, protein S, and protein C deficiencies. 5 Furthermore, modifiable risk factors such as obesity and hyperhomocysteinemia are remarkable from a preventive point of view.
Homocysteine is a sulphur-containing amino acid that is formed by demethylation of the essential amino acid methionine. 6 There are numerous reasons for hyperhomocysteinemia, including vitamin deficiency (vitamin B6, B12, and folate), renal failure, and several drugs including antihyperlipidemics, anticonvulsants, and physiological factors such as increased age or male gender. 7 Genetic deficiency of the enzyme activities including methylene tetrahydrofolate reductase (MTHFR), methylene tetrahydrofolate dehydrogenase, methionine synthase, methionine synthase reductase, and cystathionine β-synthase are also important as the causes of hyperhomocysteinemia. 8 The most commonly investigated genetic abnormality is the MTHFR gene polymorphism. A meta-analysis including 40 observational studies and 11 162 people with coronary heart disease and 12 758 healthy controls showed that individuals with the MTHFR 677 TT genotype have 20% higher plasma total homocysteine levels and 16% greater risk of ischemic heart disease compared to those with CC polymorphism. 9
Plasma concentrations of homocysteine vary widely but intracellular concentrations are preserved within a narrow range. 10 About 80% to 90% of homocysteine is protein bounded while 10% to 20% is present as the cysteine-mixed disulphide and less than 1% is present in the free reduced form. Total plasma level includes an entire amount of the all homocysteine forms in circulation. 11
Hyperhomocysteinemia has been associated with a wide spectrum of disorders including cardiovascular diseases, stroke, and venous thromboembolism. 8,12 A meta-analysis by the Homocysteine Studies Collaboration including 16 786 healthy individuals demonstrated that an even 25% increase of plasma homocysteine level was associated with an 11% greater odds ratio of ischemic heart disease and 19% greater odds of stroke after adjusting other well-known vascular risk factors. 13 Another meta-analysis of 20 prospective studies found that a 5-µmol/L increase in total plasma homocysteine level was associated with a 32% increase in odds of ischemic heart disease and 59% increase in odds of stroke. 14 A recent meta-analysis that summarized data from 24 retrospective and 3 prospective studies indicated a relationship between increased homocysteine level and VTE. 15
The aim of this study is to evaluate the plasma total homocysteine levels in Turkish patients with VTE and to investigate the effect of different risk factors on plasma homocysteine levels.
Materials and Methods
Setting
The study was conducted in the Department of Pulmonary Medicine in a university hospital in Ankara, Turkey, from May 2004 to January 2007. The local ethical committee of the institution approved the study and written informed consents were obtained from all of the participants.
Patients and Data Collection
Consecutive adults older than 18 years who were diagnosed with VTE were included as the study population while the subjects with alternative diagnosis such as community acquired pneumonia (CAP) and asthma were enrolled as the controls. Patients who had any conditions that may interfere with the blood level of homocysteine including concomitant drug (ie, methotrexate, phenitoin, vitamin B12 and vitamin B6 antagonists, antiepileptics, hormone replacement therapy,
Diagnostic Criteria
The diagnosis of PE was performed according to high or moderate probability ventilation-perfusion scan obtained according to previously published protocol by Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) investigators 16 or diagnostic computerized tomographic angiography (CT-angio) findings with appropriate clinical probability. Deep venous thrombosis is diagnosed with deep venous doppler ultrasonography of the extremities. An acute illness with respiratory symptoms and infiltrate on chest X-ray or auscultatory findings consistent with pneumonia was defined as CAP according to Infectious Diseases Society of America (IDSA) guidelines. 17 Patients with CAP who were included in the study were treated with appropriate antibiotic therapy according to guidelines. The diagnosis of asthma was established according to the Global Initiative for Asthma (GINA) guidelines. 18
Demographic data, symptoms and findings, and the history of possible risk factors for VTE were recorded prospectively. Complete blood count, routine biochemistry,
Venous samples were obtained from the whole study group after a 12-hours fasting and homocysteine level was measured with high performance liquid chromatography (HPLC) method with fluorescence detection using Chromosystem kits (Germany). The normal plasma level ranges from 5 to 15 µmol/L. Plasma homocysteine levels 15 to 30 µmol/L, 30 to 100 µmol/L, and more than 100 µmol/L are defined as moderate, intermediate, and severe hyperhomocysteinemia, respectively. 19 In addition to homocystein level, blood vitamin B12 and folate levels were measured with Immulite 2000 analyzer (Diagnostic Products Corp, Los Angeles, California) with the chemiluminescence method and the Tosoh analyzer (Tokyo, Japan), respectively.
Statistical Analysis
The results were expressed as mean ± SD. Continuous variables were compared using the Student t test for normally distributed variables and the Wilcoxon rank-sum test for nonnormally distributed variables. The chi-square test or the Fisher exact test was used to compare categorical variables. Multiple binary logistic regression analyses were used to control for potential confounding effects on VTE. Any variable whose univariable test had a P value less than .25 was accepted as a candidate for the multivariable model along with all variables of known clinical importance. Odds ratio and 95% confidence intervals for all independent variables were also calculated. SPSS version 11 for Windows; Chicago, Illinois were used for analysis.
Results
Over a period of 30 months, a total of 130 participants with the mean age of 54 ± 18 years met the inclusion criteria and enrolled in the study. Sixty-nine patients with the diagnosis of PE and 24 patients with the diagnosis of sole DVT were admitted as the study group. Eighteen patients with the diagnosis of asthma and 19 patients with CAP were served as the control group.
Perfusion scintigraphy of the lungs were performed in 52 (56%) participants of the patient group and resulted as high, moderate, and low probability in 44 (84%), 4 (8%), and 4 (8%) patients, respectively. Thorax CT was performed in 27 participants (29%) of the patient group and thrombus was identified in 21 (78%) of them. Ten of the patients (10.7%) underwent both perfusion scintigraphy and thorax CT.
Among the diagnostic tests, deep venous doppler ultrasonography of the lower extremities was performed in 75 (81%) participants in the study and in only 1 (3%) patient in the control group.
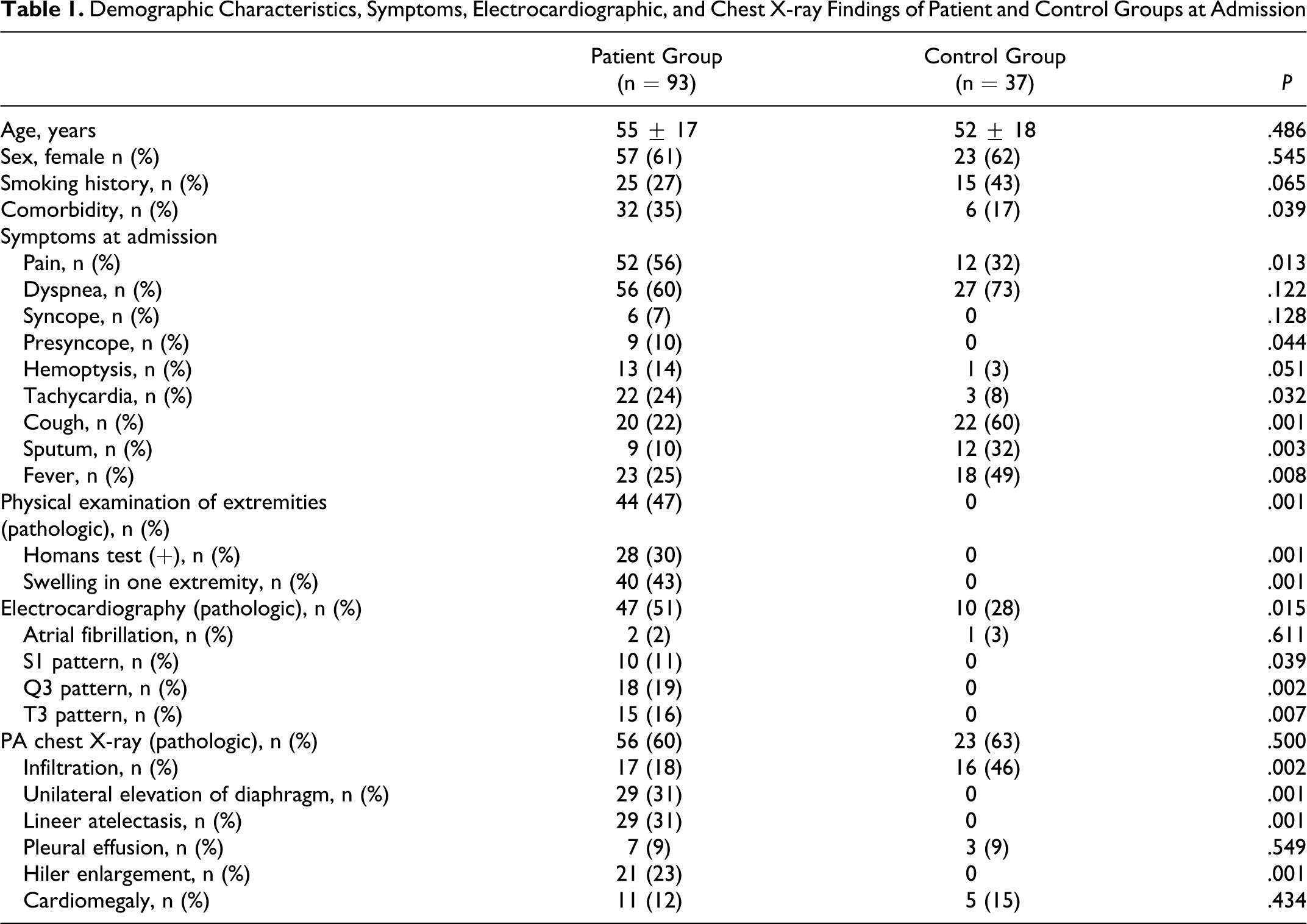
Demographic characteristics, symptoms, electrocardiographic, and chest X-ray findings of both groups at admission were compared and are summarized in Table 1 . Risk factors for the development of VTE were evaluated in study group. Identified risk factors determined in a total of 77 (83%) participants with VTE are as follows: obesity in 28 (30%), previous VTE in 11 (12%), travel history in 18 (19%), immobility in 29 (31%), malignancy in 3 (3%), pregnancy in 1 (1%), postpartum period in 2 (2%), oral contraceptive use in 4 (4%), operation in 27 (29%), and trauma in 9 (10%). Among the 27 patients having an operation and developing VTE, 13 (48%) had an orthopaedic surgery, 5 (19 %) had neurosurgery, 4 had abdominal surgery (15%).
Demographic Characteristics, Symptoms, Electrocardiographic, and Chest X-ray Findings of Patient and Control Groups at Admission
After diagnosis, 61 (66%) participants in the study group were treated with unfractioned heparin and warfarin, 24 (26%) with low molecular weight heparin and warfarin, 6 (7%) with low molecular weight heparin only, and 2 (2%) with thrombolytic therapy. Among the study group, 87 (93%) recovered and 6 (7%) were dead.
Among the laboratory parameters, no significant difference was identified between the study and control groups. The proportion of the participants who had higher level of
Homocysteine levels were found as 21 ± 12 μmol/L in study group and as 15 ± 8 μmol/L in the control group (P = .007). No significant difference was identified in vitamin B12 and folate levels between the study and control groups (P = .364 and P = .781, respectively). Moderate hyperhomocysteinemia and intermediate hyperhomocysteinemia was diagnosed, respectively, in 43 and 16 patients. None of the patients and the controls had severe hyperhomocysteinemia. Homocysteine, vitamin B12 and folate levels were summarized in Table 2 . No correlation was found between age and plasma homocysteine levels in both the patient and the control groups, respectively (r = .188, P = .072, and r = .153, P = .193). Plasma homocysteine levels were compared between patients with PE and DVT and were found significantly different (23 ± 13.7 and 16 ± 5.8 μmol/L consequently, P = .018). With regression analysis hyperhomocysteinemia was found to be associated with a 4.8-fold increased risk of VTE (95% CI, 1.254-18.863, P < .05). When the logistic regression analysis was performed for the subgroups of hyperhomocysteinemia, moderate hyperhomocysteinemia was related with a 4.2-fold increased risk of VTE (95 % CI, 1.721-10.585, P = .002) and 2.7-fold increased risk of sole PE (95 % CI, 1.275-5.920, P = .01). Additionally, intermediate hyperhomocysteinemia was associated with a 6.3-fold increased risk of VTE (95% CI, 1.343-30.063, P = .020) and 14.1-fold increased risk of PE (95% CI, 2.980-67.496, P = .001).
Homocysteine, Vitamin B12, and Folate Levels in Patient and Control Groups

When the patients with and without hyperhomocysteinemia were compared according to demographic, clinical, and laboratory data, total cholesterol level was found to be higher while vitamin B12 level was lower among patients with hyperhomocysteinemia and VTE. Smoking status was similar among patients with and without hyperhomocysteinemia (Table 3 ).
Characteristics of Patients with VTE with or without Hyperhomocysteinemia
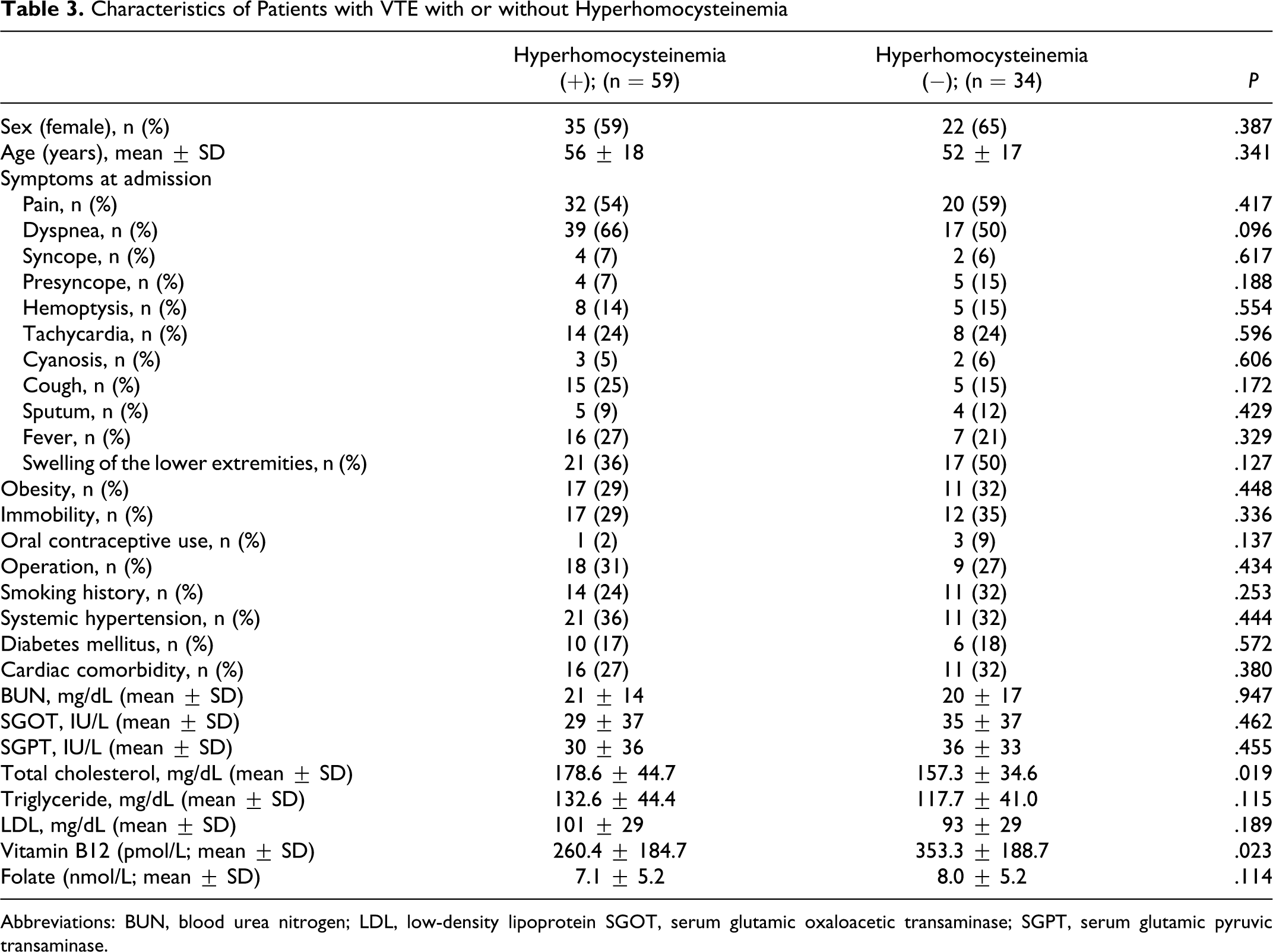
Abbreviations: BUN, blood urea nitrogen; LDL, low-density lipoprotein SGOT, serum glutamic oxaloacetic transaminase; SGPT, serum glutamic pyruvic transaminase.
Although it was not planned during prospective design of the study, later on Factor V Leiden (FVL) mutation analysis were retrospectively evaluated from the medical cards of patients with PE if they had genetic analysis results and the results were acquired in only 45% of the patients with PE, which was homozygote mutation in 2 and heterozygote mutation in 8 patients; the remaining 21 patients showed normal results.
Travel history or oral contraceptive use was present in 22 of the patients with PE but only 7 of them (31.8%) revealed FVL mutation (P = .582). Factor V Leiden mutation was not investigated in DVT patients and control participants.
Discussion
The main finding of the current study is the 63% prevalence of hyperhomocysteinemia in 93 patients of VTE. Plasma homocysteine level was found to be significantly higher among patients with VTE compared to the controls (P < .05). When the patients with VTE compared according to the prominence of hyperhomocysteinemia, the baseline demographical parameters, clinical symptoms, risk factors, and the laboratory findings were found similar except total cholesterol level which was significantly higher and vitamin B12 level which was significantly lower in patients with hyperhomocysteinemia (P < .05). We could not comment on the relationship between hyperhomocysteinemia and FVL mutation results because of the limited data, which was beyond the scope of the present study.
As first shown by McCully et al, several studies indicated that hyperhomocysteinemia is concentration-dependently related with increased cardiovascular risk and thrombosis. 10 –12,20 Rapidly growing evidence indicates that one of the major mechanisms of the homocysteine-induced vascular damage is by intimal thickening, elastic lamina damage, and smooth muscle hypertrophy. 21 Although the mechanisms underlying this effect of homocysteine are still in debate, the strongest evidence indicates the role of impaired nitric oxide and oxidative stress. 21 –23
Because it is thought to be modifiable, hyperhomocysteinemia is a clinically important risk factor of VTE. The prevalence of hyperhomocysteinemia in our study group was found to be higher than that of the controls (63% vs 27%, P < .05). The most important issue about evaluating plasma homocysteine level is the proposed cut-off value. The cut-off point of hyperhomocysteinemia is usually set at the 95th percentile of the homocysteine level in healthy individuals, which corresponds to nearly 15 µmol/L. Normal levels range very widely in different populations due to the special lifestyle factors that affect plasma homocysteine levels, such as smoking history, coffee use, and diet. 24 In this study, the prevalence of hyperhomocysteinemia is found to be higher than the prevalence that was presented in several previous reports that varied between 7.9% and 25% in patients with VTE. 25 –27 As well, the mean plasma total homocysteine level of the control group was slightly higher than some of the previous reports, which showed plasma homocysteine levels between 10 and 12 µmol/L in Turkish healthy individuals. 28,29 There may be several reasons for the higher plasma homocysteine levels in our patient and control study population. At first, 28% of our patients who had hyperhomocysteinemia were current smokers. As a limitation, we did not evaluate ex-smokers in this patient population. Moreover, several lifestyle factors such as exercise, alcohol consumption, coffee intake, and protein intake, which could not be particularly investigated in the study, may be the reasons of increased homocysteine levels. Some drugs such as lipid-lowering agents and proton pump inhibitors were not recorded in the study, which may cause the higher prevalence. Another important reason for increased homocysteine level in our study group may be the racial differences. To the best of our knowledge, there is only 1 study that evaluates hyperhomocysteinemia prevalence in patients with VTE from our country. In that study, Okumus et al reported the prevalence of hyperhomocysteinemia similar among patients with VTE and the control group (11.5% vs 8.9%, P > .05). 30 However, mean serum total homocysteine levels were not documented in that report. In addition, there are some other authors who demonstrated comparable levels of mean serum homocysteine in healthy population from the different regions. 31 –33 These results also may indicate the possible role of geographical heterogeneity beside racial differences.
Besides environmental features, factors that determine plasma homocysteine levels may also be genetic. The most commonly studied genetic abnormality responsible for hyperhomocysteinemia is MTHFR 677 C→T mutation. Although there are conflicting results between MTHFR 677 C→T mutation and increased risk of venous thrombosis, this genetic appearance indicated that some racial differences may be present among different populations. 15,34 In a study of Ozarda et al, the MTHFR 677 C→T mutation was found in 50.7% of the healthy Turkish individuals. In addition, in homozygote participants with MTHFR 677 C→T mutation, serum folate concentration was lower and serum total homocysteine level was higher than those in the wild genotype. 28
Increased age is another previously reported risk factor of hyperhomocysteinemia, although we could not document a correlation between age and plasma total homocysteine levels in the present study. 35 As well, this might be one of the underlying cause otherwise result of increased VTE incidence at the older age.
Our study indicated that hyperhomocysteinemia is associated with a 4.8-fold increased risk of VTE. Our results are in accordance with previous reports that observed an increased risk of VTE in hyperhomocysteinemia between 2.1- and 5.6-fold. 26,36 Another interesting result of the current study is the increased levels of plasma homocysteine among patients with PE compared with DVT (23 ± 13.7 vs 16 ± 5.8; P < .05). There is limited data comparing plasma homocysteine levels among patients with DVT and PE in the current literature. In the study of Okumus et al, there was no significant difference between the patients with DVT and PE. 30 Because hyperhomocysteinemia is known to be a dose-dependent thrombotic factor, the difference may be a result rather than a reason.
Vitamin B6 and vitamin B12 deficiencies are an important cause of hyperhomocysteinemia because both of these play a central role in homocysteine metabolism. The conventional treatment of hyperhomocysteinemia is folate supplementation, usually with vitamin B6 and/or vitamin B12. Although the largest randomized controlled study Norwegian Vitamin trial which evaluates the effect of vitamin supplementation on plasma homocysteine levels and clinical outcomes failed to indicate a risk reduction for myocardial infarction and stroke, 2 ongoing trials in larger populations are expected to enlighten the effect of vitamin supplementation on clinical outcome. 37 In the current study, we have found hyperhomocysteinemia as the only risk factor of VTE independent from vitamin B6, vitamin B12, and folate levels.
In conclusion, this study shows the high prevalence of hyperhomocysteinemia in Turkish patients with VTE. Hyperhomocysteinemia was associated with a 4.8-fold increased risk of VTE independent from the other confounding factors. Hyperhomocysteinemia is possibly modifiable risk factor that should be considered when screening patients with VTE. Secondary factors such as vitamin B12 deficiency that may influence homocysteine levels should be identified to make an attempt to reverse the conditions.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.