
Abstract
Keywords
Background
Venous thromboembolism (VTE), consisting of deep vein thrombosis (DVT) and pulmonary embolism (PE), is associated with significant morbidity, mortality, and resource expenditure in hospitalized patients. As many as 8% of hospital deaths can be attributed to PE 1 and fewer than 20% of patients are estimated to survive 3 months following a nonfatal PE. 2 An episode of VTE predisposes patients to recurrence 3 and is associated with self-reported reduced quality of life. 4
Venous thromboembolism predominantly complicates the care of nonsurgical patients. 5,6 The reported incidence 7 –10 of venographically detected DVT in hospitalized medical patients not receiving prophylaxis has ranged from 10% and 50%. A number of extrinsic and intrinsic features are recognized to predispose patients to the development of VTE. Adult internal medicine populations are generally very diverse with many known risk factors, including myocardial infarction, stroke, infection, lung disease, heart failure, or malignancy. 7,11 –14
The American College of Chest Physicians (ACCP) has outlined therapeutic recommendations for medical patients at risk of VTE, specifically advocating thromboprophylaxis in this population with either low-dose unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH). 6
A meta-analysis of randomized controlled clinical trials evaluating VTE prophylaxis in medicine patients identified 9 studies comparing LMWH to low-dose UFH. 15 Although no significant difference between groups was observed in the incidence of DVT, PE, or death, LMWH therapy was associated with a 52% reduction in major bleeding (P = .049).
Cost-effective strategies have been identified to prevent VTE following surgery, 16 knee and hip arthroplasty, 17,18 and trauma. 19,20 Conversely, thromboprophylaxis is not well characterized for hospitalized medicine patients. A previous study attempted to determine the most cost-effective regimen in this population but failed to include all relevant studies comparing low-dose UFH with LMWH or distinguish these 2 therapies from control. 21 Other groups found LMWH to be cost neutral or cost saving when compared to thromboprophylaxis with UFH, but these were evaluations from British, 22,23 European, 24 and American 25 economic perspectives and did not describe any unique risks or benefits among specific subgroups of internal medicine patients.
Determining the optimal strategy for thromboprophylaxis in medicine patients is of growing importance. The prevention of VTE in hospitals has been identified internationally as a priority to improve patient outcomes. 26,27 Health care agencies have developed education programs and implemented policies to improve guideline adherence and increase the use of proven prophylactic regimens currently notoriously underused. 28 –30 Reports are emerging, describing institutional policies for therapeutic interchange among heparin agents that may inadvertently result in increased health care costs without offering improved clinical benefit or greater patient safety. 31,32
It would appear that although LMWHs are as effective as low-dose UFH for thromboprophylaxis, less frequent administration and potentially safer adverse effect profile associated with LMWHs might offset the difference in drug acquisition cost. 33 –35 Conversely, familiarity and low acquisition cost has made UFH the default thromboprophylaxis alternative for medicine patients in many institutions. It is important to determine whether the small decrease in major bleeding observed with LMWH in clinical trials improves overall patient safety and outcome. Similarly, the heterogeneity of the adult internal medicine population necessitates specific evaluation of thromboprophylactic outcomes according to a hospitalized individual’s unique disease- or patient-related risks.
The objective of this study was to develop a probabilistic decision analytic model, incorporating both efficacy and safety outcomes from randomized controlled trials and other resources, to determine the incremental cost-effectiveness of LMWH relative to low-dose UFH therapy for the prevention of VTE in a Canadian internal medicine population.
Methods
Study Design
A probabilistic decision analytic model was used to assess the costs and outcomes of administration of a LMWH (enoxaparin 40 mg subcutaneously [SC] once daily) compared to UFH (5000 U SC twice daily) for the prevention of VTE in hospitalized adult internal medicine patients (Figures 1, 2, and 3 ). Costs and outcomes were evaluated from the institutional perspective and the time horizon was duration of hospital stay. The model was created with DataPro 2008 (Treeage Software Inc, Williamstown, Maryland).
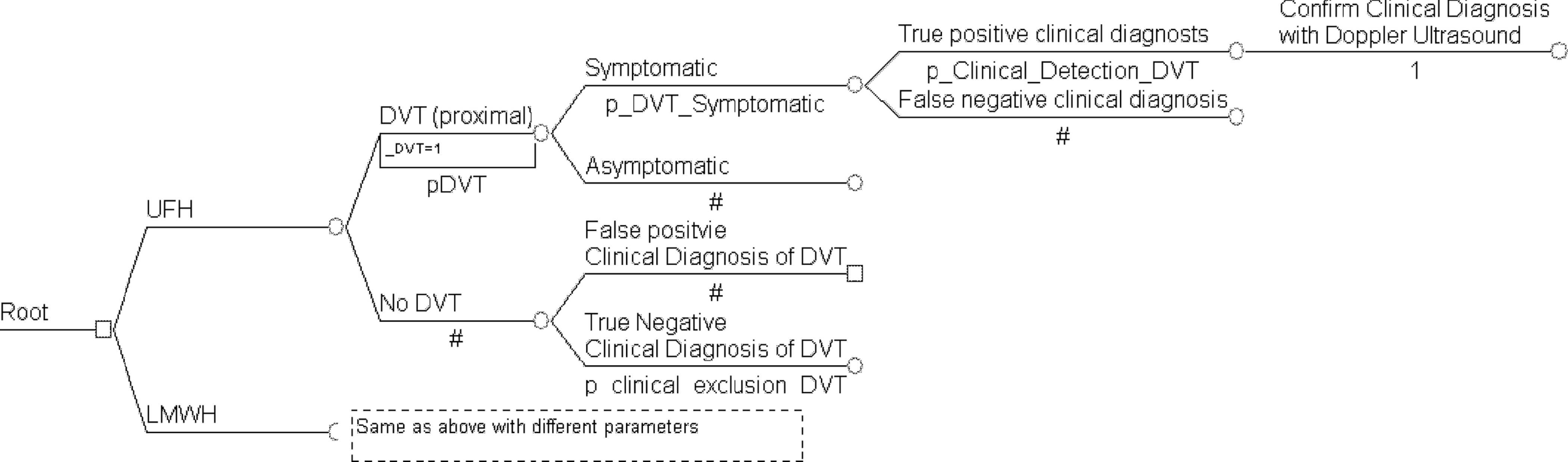
Schematic illustration of the decision tree. LMWH indicates low-molecular-weight heparin; UFH, unfractionated heparin; DVT, deep vein thrombosis.
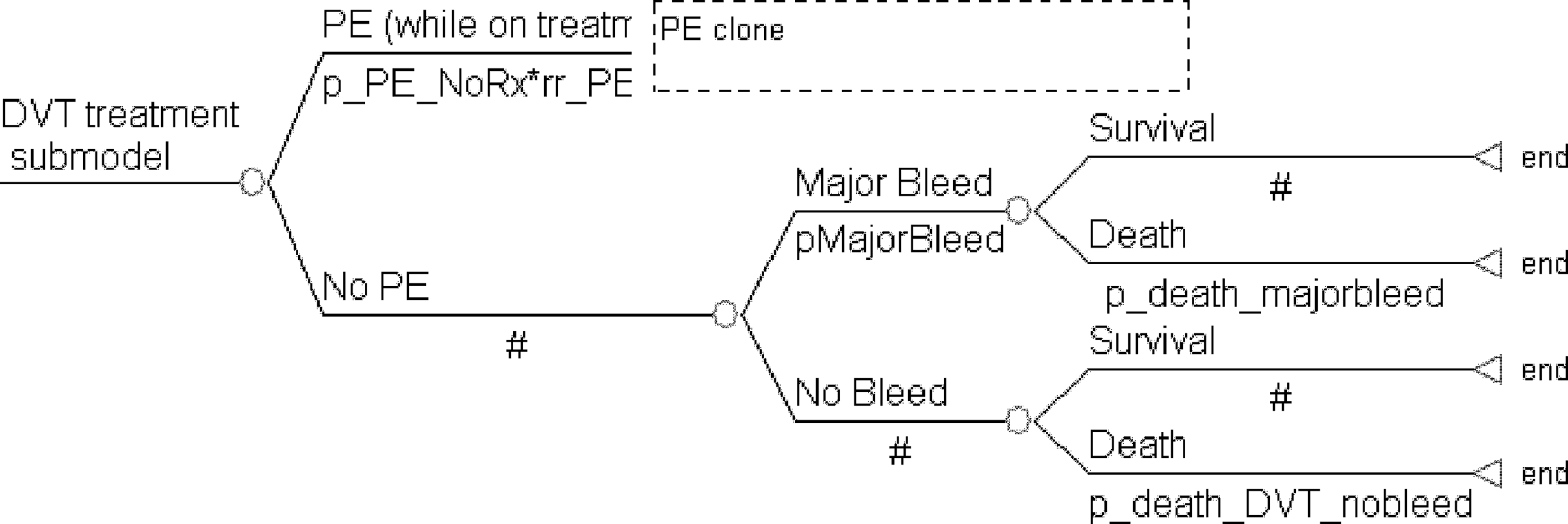
DVT treatment model. DVT indicates deep vein thrombosis; PE, pulmonary embolism.
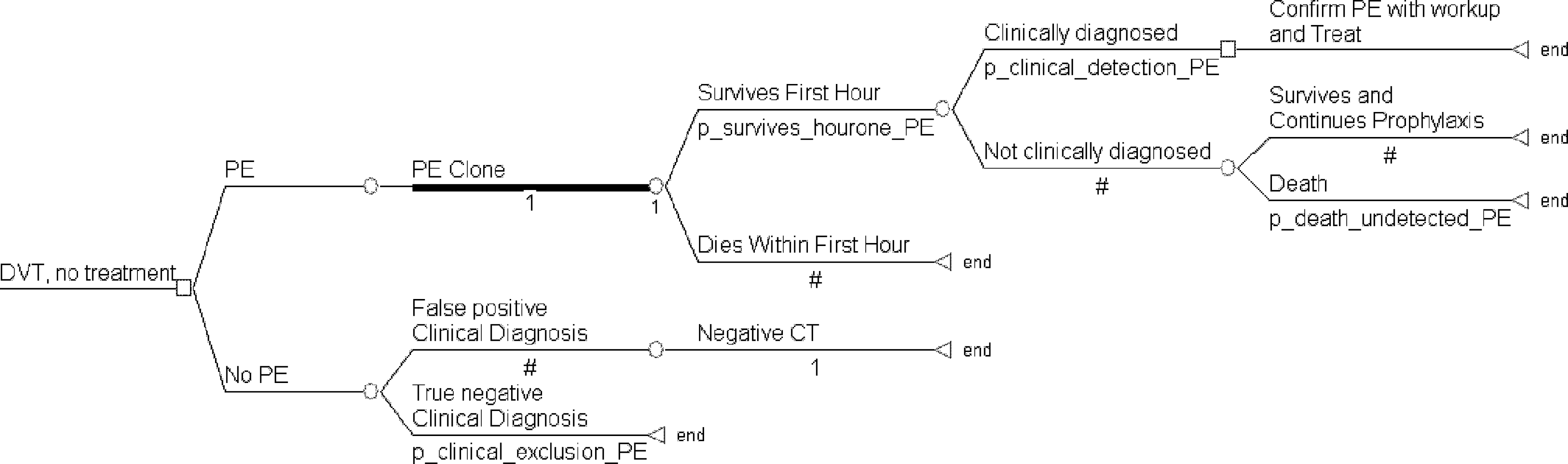
DVT, no treatment submodel. DVT indicates deep vein thrombosis; PE, pulmonary embolism; CT, computed tomography.
Probability estimates and assumptions
It was assumed that VTE prophylaxis would be initiated for all medical patients at risk of VTE on day 1 of hospitalization and continued for 7 days. This duration of therapy reflects the mean length of stay (LOS) of internal medicine patients at our Canadian institution and is consistent with the duration of treatment modeled in other studies. 22,36 No additional routine laboratory monitoring was included for either strategy as LMWH and low-dose UFH do not alter partial thromboplastin time (PTT), and heparin-induced thrombocytopenia (HIT) occurs rarely during 1 week of prophylaxis therapy. 21,22,37,38
The probabilities of DVT and major bleeding were obtained from the meta-analysis performed by Mismetti
15
whereas the probabilities of PE and death were derived from other published data (Table 1
).
20,24,39,40
It was assumed that 40% of proximal DVT
33
and 5% of distal DVT
24
would be symptomatic, but patients would not be routinely screened for asymptomatic VTE.
42
Any patient developing clinically detectable symptoms of DVT would undergo Doppler ultrasound (U/S) examination of the legs,
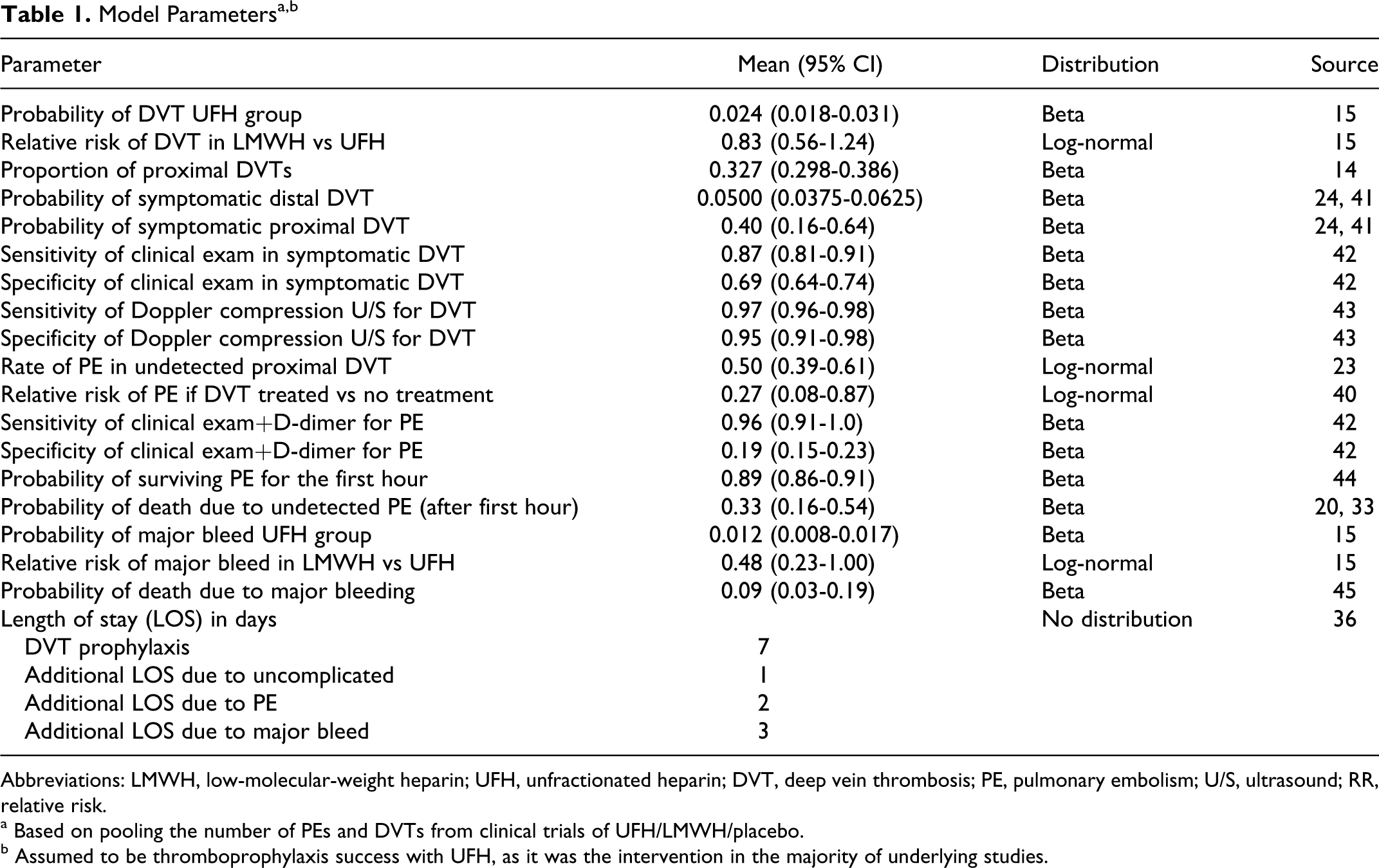
Abbreviations: LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; DVT, deep vein thrombosis; PE, pulmonary embolism; U/S, ultrasound; RR, relative risk.
a Based on pooling the number of PEs and DVTs from clinical trials of UFH/LMWH/placebo.
b Assumed to be thromboprophylaxis success with UFH, as it was the intervention in the majority of underlying studies.
It has been previously estimated that approximately 50% of patients with symptoms will have DVT or PE confirmed by objective measures. 44,46,47 A proportion of patients without VTE will have a false positive diagnosis and go on to receive treatment. Conversely, some patients with clinically relevant DVT will not exhibit symptoms or have false negative investigation and not receive treatment. A number of these patients with DVT will go on to develop PE. According to the model, if investigations for VTE are positive, the patient would be treated, regardless of initial thromboprophylaxis regimen. It is assumed that therapy for detected VTE would be LMWH and oral anticoagulation with warfarin (initiated at 5 mg orally daily and titrated to international normalized ratio [INR] 2-3). Low-molecular-weight heparin would be administered until the patient reached 5 consecutive days of therapeutic INR, after which warfarin would continue as monotherapy for at least 6 months. Alternative VTE treatment with intravenous UFH was modeled in the secondary analysis. Costs and outcomes associated with outpatient LMWH and warfarin therapy and potential long-term sequelae (bleeding adverse events, recurrent VTE, and postthrombotic syndrome) were not explicitly accounted for in the decision model, given the institutional perspective. 16,20
Major bleeding is defined as clinically overt bleeding associated with a decrease in hemoglobin by 20 g/L or transfusion requirement of at least 2 units of red blood cells. 16,48 Rates of clinically significant bleeding in studies of heparin thromboprophylaxis in medical patients vary. 48 Treatment of major bleeding may be straightforward medical or surgical management, involving relatively simple procedures like blood transfusion or hematoma evacuation, whereas intracranial, retroperitoneal, and gastrointestinal hemorrhage require more extensive investigation and intervention. 35,49 Major bleeding event rates characterized in the Mismetti meta-analysis were applied to our decision model. We assumed that each major bleeding event resulted in an increased length of hospitalization by 3 days, 50 and that the mortality associated with major bleeding was 0.9% 51 We assumed patients managed for major bleeding would continue usual VTE treatment. Minor bleeding (epistaxis, hematuria, ecchymosis, and hematemesis) was not included as the lack of significant medical intervention coupled with relatively infrequent occurrence would not contribute to the overall model. 16,17
Cost estimates
As the analysis was performed from an institutional perspective, only direct medical costs associated with VTE prophylaxis and management of untoward events were included (Table 2 ). All costs were determined in 2009 Canadian dollars. The Consumer Price Index (CPI) was used to account for inflation of all costs obtained from data reported for other years. 56 Discounting was not required, given the time horizon of the analysis. We did not include the cost of medical treatment and further management or readmission beyond the initial hospitalization period.
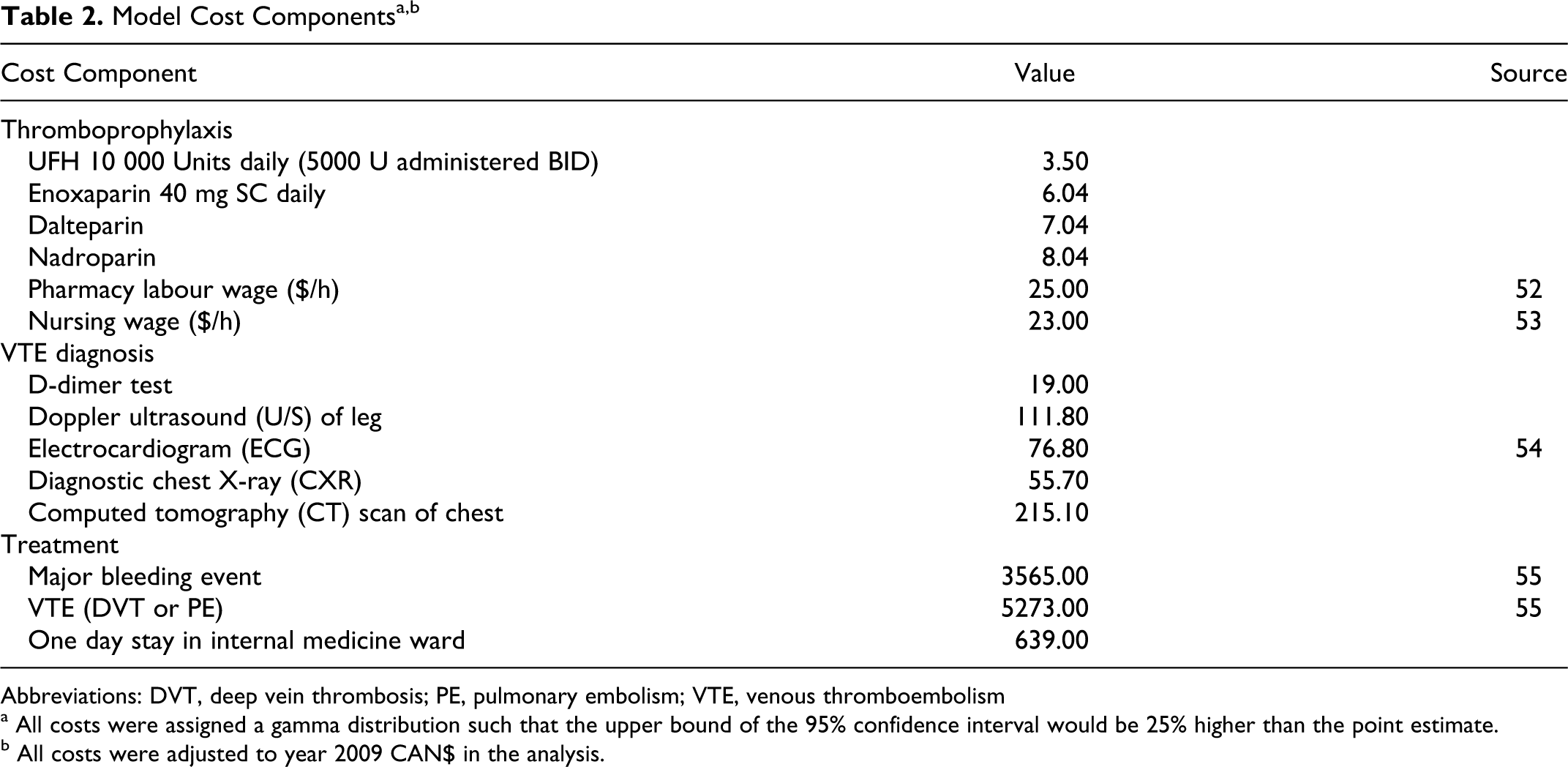
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism
a All costs were assigned a gamma distribution such that the upper bound of the 95% confidence interval would be 25% higher than the point estimate.
b All costs were adjusted to year 2009 CAN$ in the analysis.
Thromboprophylaxis drug costs were obtained from the Vancouver General Hospital inpatient pharmacy. Studies using thromboprophylaxis with 2 other LMWHs, dalteparin and nadroparin, were represented in the meta-analysis by Mismetti, 15 therefore the acquisition costs of these alternative therapies was incorporated into the sensitivity analysis. Costs of VTE investigation were obtained from the British Columbia Medical Association Guide to Fees 2008, 54 as well as other reported data. 16,18,48
Nursing and pharmacy labor costs were included in the sensitivity analysis. Unfractionated heparin is ward stock at this institution and would simply involve order entry (and not drug dispensing) from the pharmacy department. Nursing administration time involves drawing up the UFH dose from a multidose vial from ward stock twice daily and administering the injection. 53 However, enoxaparin is administered using a pre-filled syringe, which is less time-consuming. 57 As such, we assumed that the whole process of ordering, preparing, and administering of UFH and LMWH would both take 5 minutes per injection. Pharmacy time 52 required for preparing an injection dose of LMWH was 2.5 minutes at an average hourly rate of $25.00.
Hospitalization costs were calculated by multiplying the cost of daily hospital stay for internal medicine patients by the LOS. Although the true impact of VTE on the LOS has not been established in internal medicine patients, it was assumed that uncomplicated VTE would prolong the average internal medicine hospitalization by 1 day, regardless of the day diagnosed. 50,58 The costs of treating major bleeding episodes and associated prolonged hospitalization costs were obtained from published pharmacoeconomic analyses. 16,18,34,35 . A wide range of costs were included in the sensitivity analysis as there is a large disparity between the management of relatively uncomplicated major bleeding (hematoma) and more serious hemorrhage (gastrointestinal).
Cost-effectiveness analysis
In the base-case analysis, using the point estimates for all model parameters, we determined the incremental cost of LMWH relative to low-dose UFH per uncomplicated DVT and untoward event averted. An uncomplicated DVT was considered distal or proximal DVT not progressing to PE. An untoward event was any of PE, major bleed, or death. These events were combined into 1 group together to avoid reporting multiple cost-effectiveness ratios that would make ranking of strategies difficult. Multiple untoward events per person (e.g. major bleed resulting in death) were counted as one. Uncomplicated DVT was not counted as an untoward event as it is mainly the clinical consequences of DVT that affects long-term health. 39,59,60 We also calculated the numbers of DVT, PE, major bleed, and death independently associated with each treatment.
The cost-effectiveness of LMWH versus UFH for VTE prophylaxis in specific subgroups of at-risk medicine patients was calculated, including those aged greater than 75 years, individuals with a history of DVT, chronic respiratory disease, pneumonia, heart failure, or malignancy. 7,12 –14 Relative risk of DVT and thromboprophylaxis outcome in these populations was estimated from prior work. 14,61 The probability of DVT in a unique at-risk medicine population was calculated by weighted-averaging subgroup-specific probability of DVT, with weights being the number of patients with specific medical conditions in a representative North American population and then divided the subgroup-specific probabilities by this average. 61 Conditional on having DVT, the risk of PE- and VTE-related death only minimally varied across subgroups and as such we assumed that the risk of these events alongside risk of major bleed were unrelated to the underlying medical condition once DVT is developed.
To evaluate the robustness of the results with model assumptions, a series of 1-way sensitivity analyses were performed including varying the acquisition cost of LMWH and UFH, the cost of managing a PE and major bleed, changing the baseline rate of DVT and the probability of progression to PE in the absence of treatment, and assuming alternative LOS values for uncomplicated and complicated DVT.
In addition to the base-case and 1-way sensitivity analyses, a probabilistic sensitivity analysis (PSA) was performed by specifying the distribution for each model parameter to represent the uncertainty around the point estimate and then selecting values at random from those distributions using Monte Carlo simulation. 45 Beta distribution and log normal distribution were assigned to probabilities and relative risk values, respectively. Parameters of such distributions were estimated from either the sample size of the original studies or reported confidence intervals. No specific data pertaining to the uncertainty in the cost parameters were available, so it was characterized using standard deviations equal to one third the mean value. Uncertainty around LOS values was also modeled by assigning a uniform distribution covering ±25% of the original value. Results of PSA are illustrated on the cost-effectiveness planes and cost-effectiveness acceptability curves (CEACs). The cost-effectiveness plane represents the joint distribution of the incremental costs and incremental effectiveness, whereas the CEAC illustrates the probability of LMWH being cost-effective at range of values that the decision maker might pay to avoid an untoward event (willingness-to-pay). Probabilistic sensitivity analysis was conducted with untoward events averted as the effectiveness outcome.
Results
The number of DVT diagnoses (true or false), true DVT cases, PEs, major bleeds, and in-hospital deaths associated with VTE thromboprophylaxis strategies for a hypothetical cohort of 1000 patients are presented in Table 3 . Thromboprophylaxis with LMWH resulted in a lower number of suspected DVT diagnoses leading to diagnostic workup and a 14% reduction in the incidence of true DVT and PE when compared to UFH (24 and 29 VTE events, respectively). Incidence of major bleeding events with UFH thromboprophylaxis was more than twice that of LMWH. These differences eventually led to a small increase in the incidence of death due to VTE or major bleed with UFH use.
Number of VTE-Related Events During Hospitalization of a Hypothetical Cohort of 1000 Adult Internal Medicine Patients
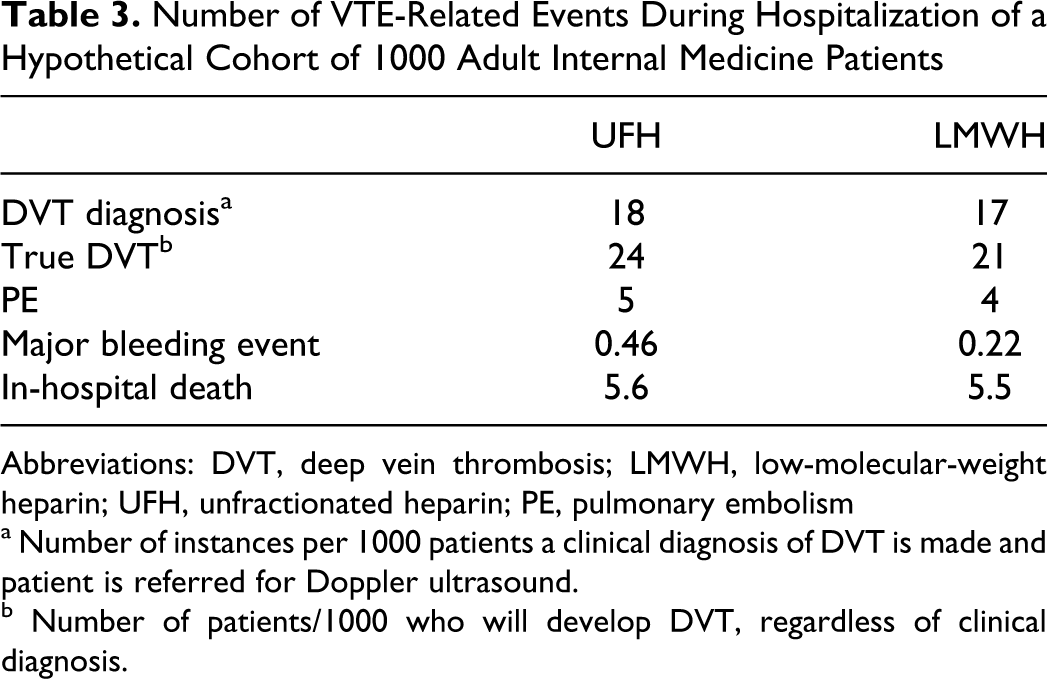
Abbreviations: DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; PE, pulmonary embolism
a Number of instances per 1000 patients a clinical diagnosis of DVT is made and patient is referred for Doppler ultrasound.
b Number of patients/1000 who will develop DVT, regardless of clinical diagnosis.
Base-case cost-effectiveness analysis results are presented in the Table 4 . In general, thromboprophylaxis with LMWH resulted in slightly higher costs but more favorable outcomes. Low-molecular-weight heparin resulted in an increased in-hospital costs by $7.40, reductions in DVT rate by 0.0036 (3.6/1000 patients), PE rate by 0.0007 (0.7/1000 patients), and major bleeding event rate by 0.0003 (0.3/1000 patients). Combined incidence of untoward events (PE, major bleed, and death) was reduced by 0.0012 (1.2/1000 patients). The resulting base-case incremental cost-effectiveness ratio (ICER) for LMWH compared to UFH was $2046 and $6832 for averting a DVT or untoward event, respectively.
Base Case Cost-Effectiveness and Sensitivity Analyses
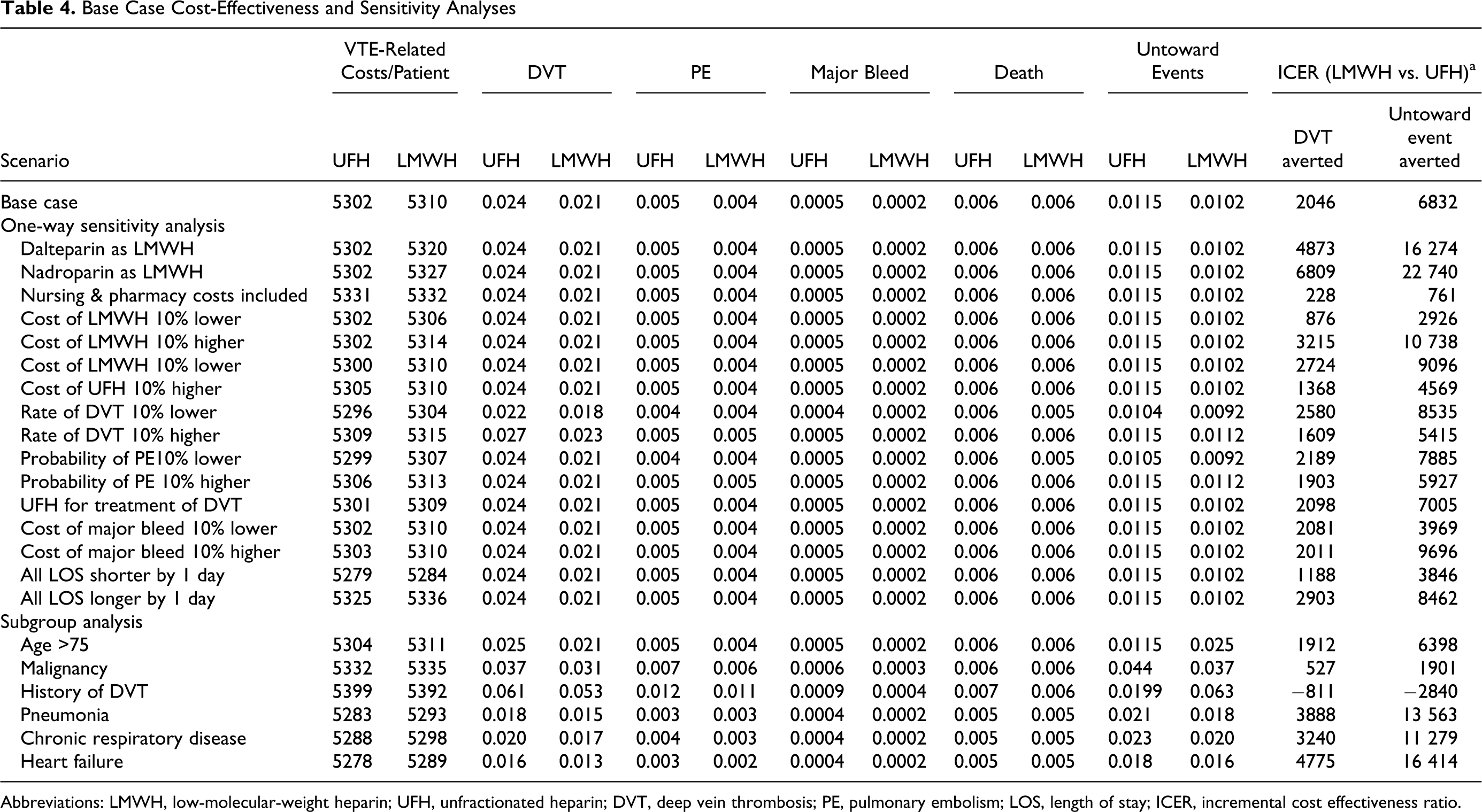
Abbreviations: LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; DVT, deep vein thrombosis; PE, pulmonary embolism; LOS, length of stay; ICER, incremental cost effectiveness ratio.
Results of the 1-way sensitivity analysis are also presented in Table 4. Overall, results were consistent across the different scenarios considered. For VTE prophylaxis with enoxaparin, ICER per DVT and untoward event averted varied from $876 (when LMWH cost was assumed to be 10% lower) and $761 (when nursing and pharmacy costs were included), respectively, to $6809 and $10 738 (when LMWH cost was assumed to be 10% higher). Use of dalteparin or nadroparin instead of enoxaparin for LMWH thromboprophylaxis resulted in a slightly increased ICER.
Results of the cost-effectiveness analysis of LMWH versus UFH in subgroups of internal medicine patients are also reported in Table 4. The highest ICER was for patients with heart failure, for whom LMWH had an ICER of $4775 for averting a DVT and $16 414 for averting an untoward event. In patients with a history of DVT, LMWH became the dominant thromboprophylaxis strategy, that is, having both lower costs and better effectiveness outcomes.
Results of the PSA are illustrated by the cost-effectiveness plane (left) and CEAC (right) for LMWH versus UFH when the outcome is prevention of any untoward events (PE, major bleed, or death) in Figure 4 . When the willingness-to-pay is close to 0, the decision maker places more emphasis on an intervention’s costs rather than on effectiveness, hence the choice of the best intervention is strictly decided by costs (ie, the least costly strategy is the preferred one). As such, because UFH is less costly, it is more likely to be the selected option for small willingness-to-pay values. The more the decision maker is willing to pay to avert untoward events, the more likely that LMWH will be preferred. At willingness-to-pay value of $50 000, there is more than 76% chance that LMWH is cost-effective. Nevertheless, this probability never reaches more than 90%, regardless of the decision makers' willingness-to-pay.
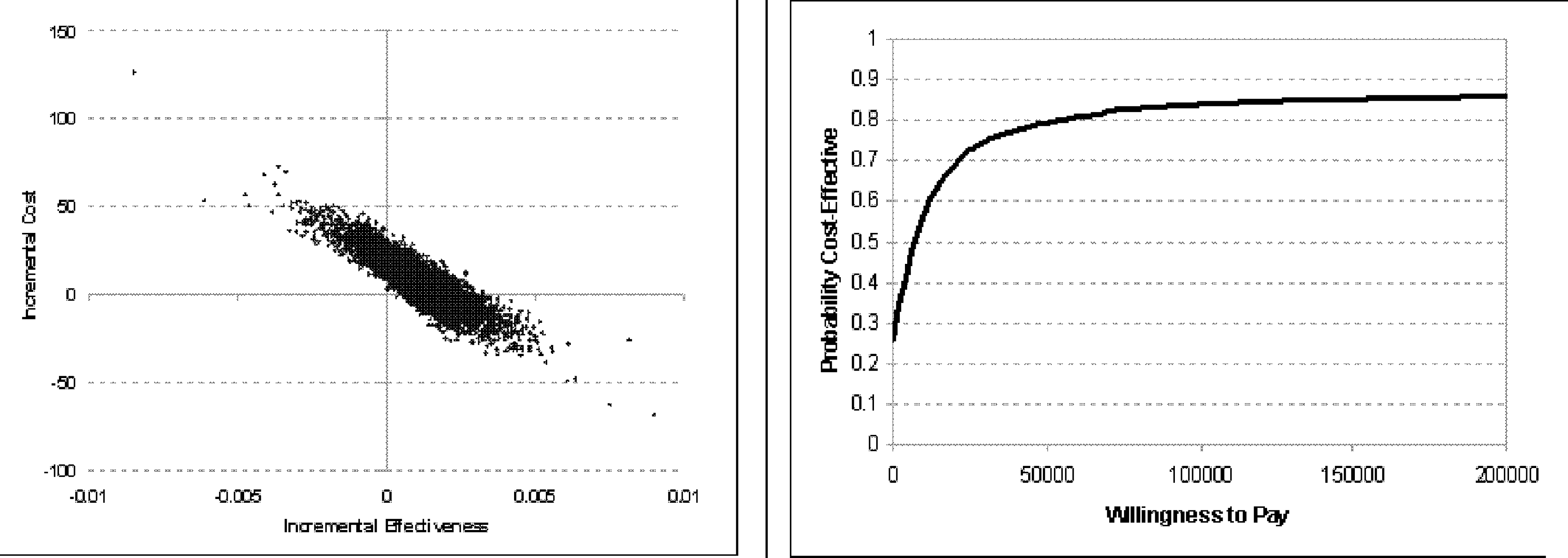
Cost-effectiveness plane (left) and acceptability curve (right) for LMWH vs UFH. LMWH indicates low-molecular-weight heparin; UFH, unfractionated heparin.
Discussion
We performed a cost-effectiveness analysis comparing LMWH and UFH for prophylaxis of VTE in hospitalized internal medicine patients from a Canadian institutional viewpoint and found that to avert an uncomplicated DVT or an untoward event (defined as any of PE, major bleed, or death), the third-party payer would have to pay $2046 and $6832, respectively. In our sensitivity analysis, this value never surpassed $6809 (DVT) or $22 740 (PE, major bleed, and death) and for selected situations, the use of LMWH was associated with decrease in both in-hospital costs and untoward events. Although the exact interpretation of the results will depend on how much the third-party payer is willing to pay to avert an untoward event as defined in our study, it appears that given the serious consequences of untoward events (PE, major bleed, and death), the willingness-to-pay will be higher than the ICERs of the base-case and alternative scenarios, indicating that LMWH is a cost-effective alternative for VTE prophylaxis in hospitalized internal medicine patients.
These findings are not entirely consistent with previous analyses from other countries. Lloyd et al found enoxaparin 40 mg SC daily to be cost neutral when compared to UFH 5000 U SC twice daily using a decision-analysis approach in hospitalized medical patients. 22 However, they modeled the implications of long-term complications of DVT (up to 15 years following index event in hospital) from a third-party payer perspective. Although sequelae of VTE can have an important impact on patient quality of life, we chose a hospital perspective and associated time horizon, which obviated the consideration of diseases or events whose natural history is inconsistent with disease detection within the hospitalization time. 62 Another British study using the same decision analysis model found LMWH to be cost saving within their specific hospitalized medicine patient population over a 110-day time horizon. 23 Base-case analysis resulted in ICER of £9922 (2003 British £) for VTE avoided with LMWH thromboprophylaxis in a 100-patient cohort compared to £9975 using UFH. Savings were attributed to increased UFH costs associated with higher VTE event rates, nursing time, and major bleeding episodes.
Schaldich et al evaluated enoxaparin 40 mg SC daily and UFH 5000 U 3 times daily in a select German inpatient medicine population. 24 Low-molecular-weight heparin was the dominant thromboprophylactic alternative from a hospital perspective across a 6- to 40-day time horizon in immobilized patients using adjunct mechanical prophylaxis (elastic compression stockings). The investigators principally used efficacy and safety outcome data from the Mismetti meta-analysis; however, unlike our study, they used more actual resource consumption prospectively obtained from their institution. Ninety percent of LMWH cost savings were accounted by reduced professional time, notably when nurse administration of UFH from multidose vials 3 times daily was considered. Of note, in addition to VTE and major bleeding events, secondary pneumonia after PE was modeled as a clinical outcome parameter, which appears to be an outcome of interest unique to this report.
Most recently, Schorr et al concluded that LMWH thromboprophylaxis (enoxaparin 40 mg SC daily) in hospitalized medicine patients ultimately resulted in cost savings when compared to twice daily UFH from an American third-party payer perspective. 25 Pulmonary embolism was not included in the model, nor were nursing costs accounted for over the brief thromboprophylaxis time period considered (5 days). Univariate analysis found that varying the rate of HIT altered potential savings with enoxaparin in this study. As described earlier, we chose not to model HIT in our decision analysis as incidence in a hospitalized medicine population receiving short-term therapy with thromboprophylaxis doses is very low. 21,22,38
This is the first pharmacoeconomic analysis to evaluate the cost-effectiveness of LMWH and UFH thromboprophylaxis in hospitalized medicine patients in Canada. Other analyses from the Canadian perspective have compared enoxaparin to no thromboprophylaxis, 36 or focused on the most cost-effective strategy for ongoing outpatient therapy once medicine patients were discharged following in-hospital development of VTE. 63,64 Although most prospective clinical data for LMWH thromboprophylaxis in medicine patients exist for enoxaparin, our sensitivity analysis altered the cost of LMWH therapy so as to sufficiently encompass the acquisition costs of other LMWH products that may be prescribed in hospitals across the country.
No other reported decision analysis has attempted to stratify the effects of heparin thromboprophylaxis alternatives among multiple subgroups of the heterogeneous at-risk medicine population. Our study assessed the unique outcomes of 6 patient groups whose modifiable or inherent characteristics predispose them to development of in-hospital VTE. The highest ICERs for both DVT and untoward event averted were identified in the heart failure subgroup. Input data for this patient population comes primarily from THE-PRINCE study 65 comparing LMWH and UFH thromboprophylaxis in patients with respiratory and heart failure. The cardiac patients tended to be older with more comorbidities contributing to greater VTE events than in the respiratory group making detection of differences between thromboprophylaxis strategies more clear. It is not immediately clear why in our subgroup analysis we found that patients with history of DVT benefit most from thromboprophylaxis with LMWH, the only scenario in our model where LMWH is out rightly dominant. It is reassuring that LMWH or UFH are similarly cost-effective, given that internal medicine patients often possess multiple comorbidities and it may be impractical to prioritize 1 condition for selection of a specific thromboprophylaxis.
Despite evidence of LMWH equivalence or superiority when compared to UFH for a number of clinical indications, including thromboprophylaxis, UFH use remains the standard of care in many institutions. Its familiarity to clinicians is incontrovertible owing to its historic role in anticoagulation over the decades. At the same time, UFH use is still fraught with difficulties encompassing accurate dosing, safe administration, labor-intensive and costly monitoring. Unfractionated heparin is categorized as a “high-alert medication” as it bears a heightened risk of significant harm due to its narrow therapeutic range and need for frequent dosing adjustment, particularly when given as treatment by infusion. 66 Still, administrators often fail to move beyond the cheap acquisition cost, perceiving UFH only as a low-cost alternative and ignoring the possible difference in the therapeutic and safety profiles of UFH and LMWH (treatment or death associated with DVT, PE, and major bleeding). 67 Suboptimal use of UFH is compounded by data demonstrating UFH dosage of 5000 U 3 times daily to be more effective in reducing DVT risk than the ubiquitous twice daily dosing. 68
It would appear that shifting hospital policy and prescribing preferences to LMWH as the most effective heparin alternative in the medicine population is a struggle when compared to the adoption of LMWH thromboprophylaxis in appropriate surgical patients, but a greater battle to modify patient in-hospital risk of VTE wages on. Reports of pharmacoeconomic analyses identifying the preferred use of LMWH are exceeded by parallel international data indicating that only one third of at-risk medicine patients receive any sort of intervention to reduce VTE risk. 69
Our analysis has a number of limitations meriting discussion. We assessed the cost-effectiveness from an institutional perspective with a constellation of clinical events as the effectiveness outcome, whereas several authorities recommend analysis based on the quality-adjusted life years (QALY) and from a societal perspective. The time horizon of the hospitalization period in our analysis might be considered too short. Such a time horizon and the definition of outcome equally weighs a mild, resolvable episode of PE with a death and does not account for the future life years or quality of life lost due to the in-hospital events. Nevertheless, we believe an analysis from an institutional viewpoint is still very relevant, as it reveals that adopting a strategy that is cost-effective from a societal perspective, as shown by other studies, is also an optimal decision from an institutional viewpoint. This congruence can encourage institutional stakeholders and assure them that in this case no “sacrifice” is involved in adopting an approach beneficial to society. This is especially relevant in this context as the lack of indomitable clinical evidence or recommendation on the superiority of thromboprophylaxis with LMWH compared to UFH might tempt the institutional stakeholders to adopt UFH as a lower cost alternative.
Given the time horizon of our analysis, we could not use QALY as the effectiveness outcome. This makes it difficult for the decision maker to compare the results of our analysis with cost-effectiveness of other health technologies. In addition, it is not clear how much the decision maker would be willing to pay for the nonstandard effectiveness outcome used. We excluded uncomplicated DVT from the set of untoward events (PE, major bleed, and death) such that this combined outcome comprised the most homogeneous group of events in terms of long-term health impact. Given the severity of such untoward events, it appears the ICERs in the base case and the majority of sensitivity analyses point favorably toward economic outcomes of LMWH thromboprophylaxis with respect to UFH.
We assumed that patients would receive 7 days of heparin thromboprophylaxis. The average LOS in our medicine population does not represent all patients; outcomes of individuals with prolonged hospitalization would be altered by increased heparin exposure, as well as direct and indirect costs. We only captured LOS ranges as short as 6 days and as long as 12 days in our sensitivity analysis. Detailed resource utilization data for the management of VTE and major bleeding events was not obtained from our institution. We used published estimates for treatment of these outcomes in both inpatient and outpatient populations, however the same estimates were used in both groups and, thus, should not affect the ICERs.
We did not model all medicine patient subgroups at increased risk of VTE, such as the obese. This group merits more attention in the future as they represent an increasing proportion of hospitalized patients. In one recent study, 70 6% of all patients (n = 4332) admitted to an American general medicine unit during a 6-month period were considered severely obese. We also did not evaluate heparin thromboprophylaxis in those with varicose veins or women receiving hormone replacement therapy. Outcome probabilities for a number of clinical end points in our model were drawn from the landmark meta-analysis reported by Mismetti in 1998. 15 Since this time, a second comprehensive meta-analysis of trials comparing LMWH and UFH for thromboprophylaxis has been published by Wein et al. 68 Although both authors included overlapping studies, there were important discrepancies. Mismetti included 2 non-English language publications as well as some data from 2 unpublished or abstract reports obtained from pharmaceutical companies. These data were not available or considered by Wein, who instead included studies of distinct medicine patients receiving heparin thromboprophylaxis following hospitalization for acute myocardial infarction or acute stroke. These patients would not be admitted to the general medicine units at our tertiary care center but would instead receive care in the acute coronary care and stroke units, respectively. However, we would not expect use of the Wein meta-analysis to alter our decision analysis, given the results and conclusions of these studies were the same as the Mismetti meta-analysis.
Conclusion
In our decision analysis, LMWH thromboprophylaxis resulted in somewhat higher costs, but less DVT, PE, major bleeding events, and death when compared to UFH administration. These results remained predominantly stable when a broad range of alternative assumptions was evaluated in the sensitivity analysis. Low-molecular-weight heparin had the most favorable economic profile in patients with a history of DVT when specific at-risk populations were considered. Low-molecular-weight heparin thromboprophylaxis is a cost-effective alternative to UFH in hospitalized Canadian internal medicine patients.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.