
Abstract
This qualitative review aims to synthesize the evidence on nurses’ experience of intervening with fathers when providing care to their young children. Five databases were searched. Inclusion criteria were (a) nurses’ experience, (b) intervention with fathers, (c) written in English or French. Data were extracted by two independent reviewers. Qualitative thematic synthesis of 17 peer-reviewed studies was performed by 12 family nurse researchers from six countries. Three analytical themes were identified: “Conceiving of the father’s role in terms of his involvement within the family”; “Working with fathers based on the nurse’s individual conception of the paternal role”; and “Developing a sense of efficacy in working with fathers.” The results highlight the importance of raising family nurses’ awareness of fathers’ individual realities. Training in this regard makes it possible to modify nurses’ perceptions of the paternal role and to promote the adoption of father inclusive practices within the family.
Introduction
The evolving landscape of family models in the West over the past three decades reflects a dynamic response to changing societal norms (Volling & Palkovitz, 2021). In response to new family realities, the father’s role has also evolved, and men are showing a desire to become involved early in their children’s lives (Gervais et al., 2021). Extensive research has documented the multifaceted positive effects of paternal involvement on various aspects of family well-being (Watkins et al., 2024). Fathers’ involvement has a beneficial and lasting influence on children’s social-emotional (Howard et al., 2006), cognitive (Howard et al., 2006), and academic development (McBride et al., 2005), as well as on the mental health of mothers (de Montigny, Gervais, Pierce, & Lavigne, 2020) and fathers themselves (Kotila & Kamp Dush, 2013), and the marital relationship (Fagan & Cabrera, 2012). These positive impacts underscore the importance of involved fatherhood in shaping the overall family well-being.
The perinatal period is a critical time for a father’s involvement with his child. The level of paternal involvement during pregnancy is a reliable predictor of postnatal paternal involvement (Lamb, 2010; Ramchandani et al., 2013). However, although fathers want to be involved and support their partners throughout pregnancy, many feel ill-equipped to do so and encounter barriers related to the organization of health services (de Montigny et al., 2016). As such, a significant number of fathers report difficulty not only in navigating services, but also in obtaining support and guidance from health professionals (Da Costa et al., 2015; de Montigny et al., 2013). Health professionals play an important role with fathers, and their support can positively influence fathers’ involvement with their child (Holtslander, 2005). Beliefs and perceptions regarding fathers play a determinant role in how health professionals engage and interact with fathers (de Montigny & Lacharité, 2012). The more positively professionals view fathers, the more they will involve fathers in the child’s care and the more effective they will feel during interactions (de Montigny et al., 2017; de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020). Despite the fact that professionals are increasingly recognizing the importance of including fathers in their practice (Alehagen et al., 2011), some are still reluctant to involve them and sometimes feel ill-equipped to interact with them (Höglund & Holmström, 2008). In this context, Dubeau et al. (2023) sought to analyze practices in the health and social services network that support paternal involvement in Quebec, Canada. The results of this research provided a portrait of father-inclusive practices, but the voice of nurses was not well represented (Dubeau et al., 2023). Since nurses play a major role with young families, and how they intervene can have a significant impact on early paternal involvement, there is a need to explore nurses’ perceptions of their practice and interactions with fathers. Although some studies have examined the benefits of adopting father-inclusive nursing practices, the experience of these professionals when working with fathers remains unclear. A better understanding of nurses’ experiences is needed to improve the support offered to men in health services.
Thus, the purpose of this review is to systematically synthesize the qualitative evidence on nurses’ experience of interacting with fathers when providing care to their children and adolescents. This review is based on two research questions:
To acknowledge the unique roles of fathers, this review specifically centers on the term “fathers” rather than referring to parenting partners.
Method
The approach chosen to develop this qualitative systematic review is the thematic synthesis of Thomas and Harden (2008). This method allows for a new interpretation of the data and the emergence of new knowledge that goes beyond the findings of previous studies. The Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) guidelines were used to report this qualitative synthesis (Tong et al., 2012).
Search Methods
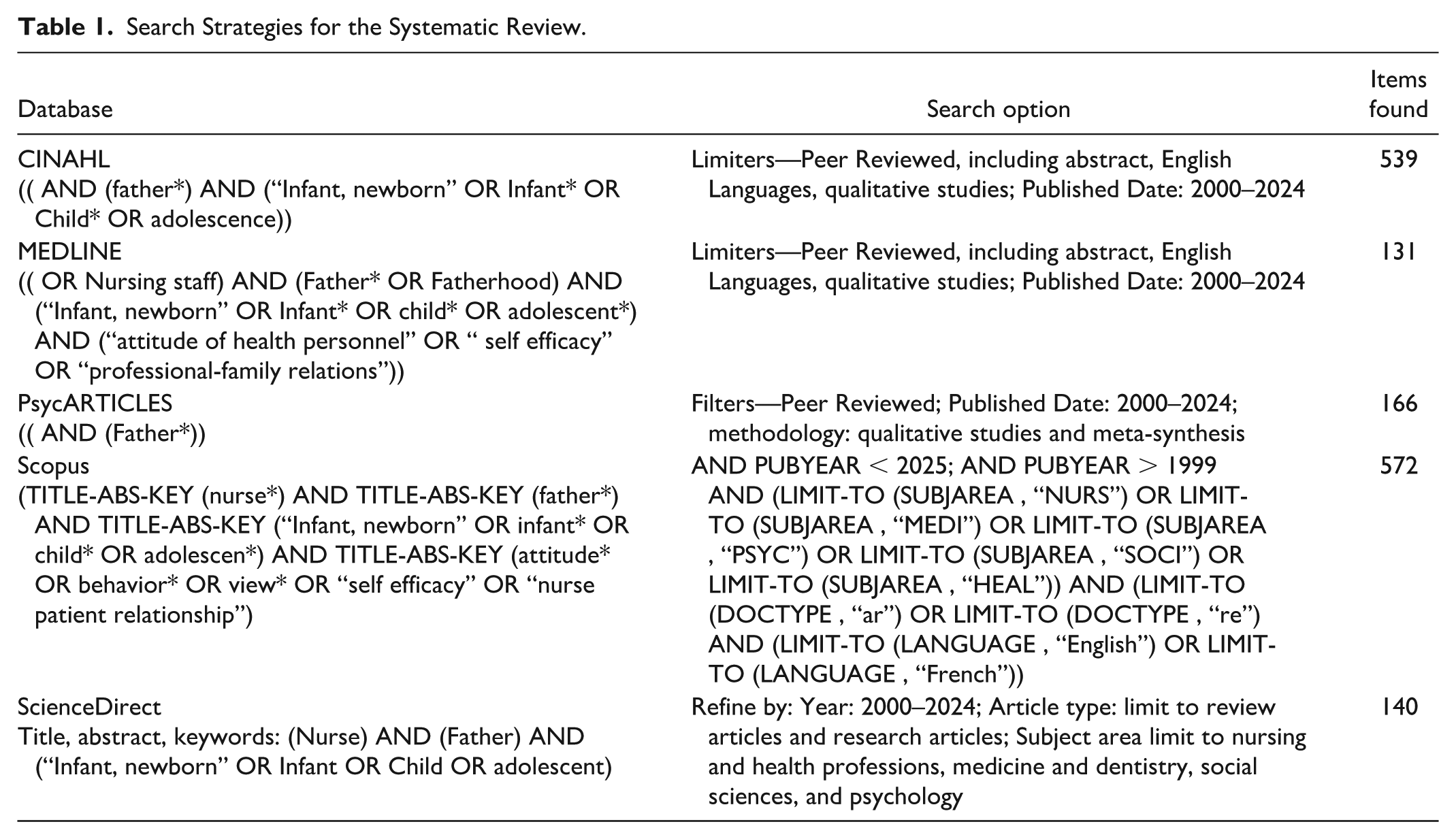
The modified population, context, outcomes (PCO) framework for qualitative methodology was used to formulate the research questions and select keywords (Butler et al., 2016). The literature search was conducted by two reviewers independently (C.R. and I.L.) in five databases (CINAHL, MEDLINE, PsycInfo, Scopus, ScienceDirect) between October and December 2020, and with an update in September 2024. The respective thesauri of the databases enabled the validation of the choice of keywords. The Boolean operators “OR” and “AND” and word truncation were used to distinguish synonyms, combine terms, and capture all possible spellings and endings (Aromataris & Riitano, 2014; Butler et al., 2016). The search was limited to studies published since 2000, as research interest in this phenomenon began during that time. No limitation was placed on country of origin. The bibliographic references of the selected articles were reviewed to identify additional relevant studies missed in the electronic search. Table 1 presents the literature search strategy for the different databases.
Search Strategies for the Systematic Review.
Inclusion and/or Exclusion Criteria
To be included in this thematic synthesis, the selected studies met five criteria: (a) a sample consisting wholly or partly of nurses whose perspectives could be distinguished from those of other participants; (b) results addressing nurses’ experiences with fathers of children and adolescents either hospitalized or receiving care and services in the community; (c) a primary study that used any type of qualitative method of data collection and analysis; mixed-method studies were excluded only if the quantitative results were predominant; (d) published in English or French, as these were the languages in which the reviewers were proficient; and (e) peer-reviewed and included an abstract. Gray literature was not explored in the selection process.
Search Outcome
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram was used to report the different stages of the study selection process; see Figure 1 (Page et al., 2021). To counteract judgment bias that can occur when there is only one reviewer, the reviewers used inter-judge agreement for all study selection steps (C.R., I.L.) (Butler et al., 2016). In total, the literature search identified 1,548 studies, which were imported into Endnote X20 software. After removing duplicates, 1,055 studies were initially screened based on title, abstract, and inclusion criteria. From this review, 44 publications were retained and read in full by the reviewers (C.R.; I.L.). Disagreements about the eligibility of an article were resolved by input from a third reviewer (F.D.), an expert in the field. As a result of this step, a total of 27 articles were excluded, either because they did not address the phenomenon of interest (20), were ineligible publication types (5), or used quantitative methodology or secondary data analysis (2). At the end of the selection process, 17 original articles were selected for the thematic synthesis. All selected articles were in English, and no articles were added after manual verification of bibliographic lists.
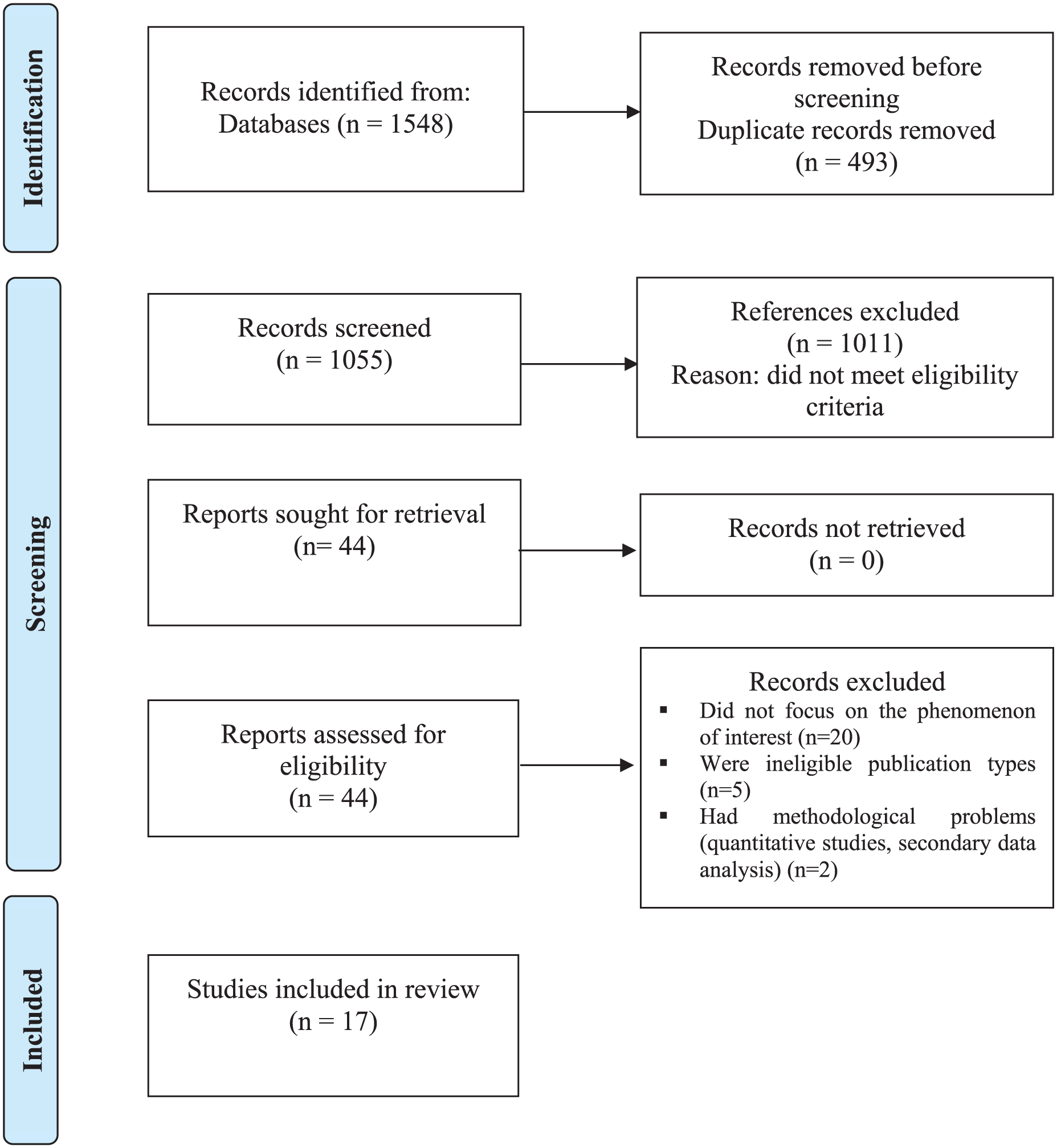
PRISMA Diagram: Study Selection Process (Page et al., 2021).
Quality Appraisal
The Critical Appraisal Skills Programme (CASP) criteria for qualitative studies were used to assess the quality of the studies included in this thematic synthesis (Critical Appraisal Skills Programme, 2018). The reviewers (C.R.; I.L.) independently assessed the studies, answering questions with “Yes,” “No,” or “Cannot say.” To ensure all relevant data were included in the synthesis, no studies were excluded based on quality assessment. The results are presented in Table 2.
Quality Assessment of Included Studies Based on CASP (Critical Appraisal Skills Programme, 2018).
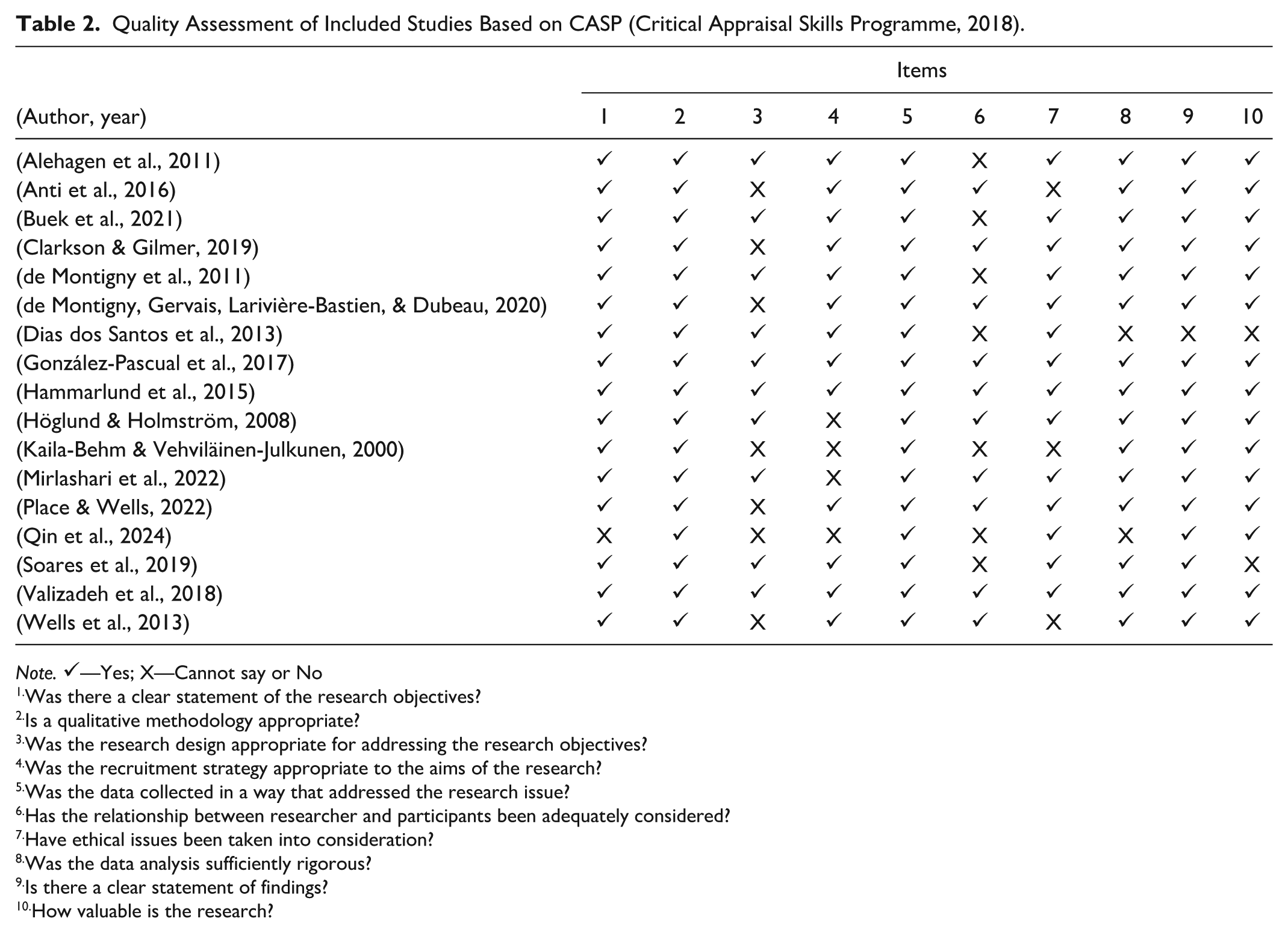
Note. ✓—Yes; X—Cannot say or No
Was there a clear statement of the research objectives?
Is a qualitative methodology appropriate?
Was the research design appropriate for addressing the research objectives?
Was the recruitment strategy appropriate to the aims of the research?
Was the data collected in a way that addressed the research issue?
Has the relationship between researcher and participants been adequately considered?
Have ethical issues been taken into consideration?
Was the data analysis sufficiently rigorous?
Is there a clear statement of findings?
How valuable is the research?
Data Extraction and Synthesis
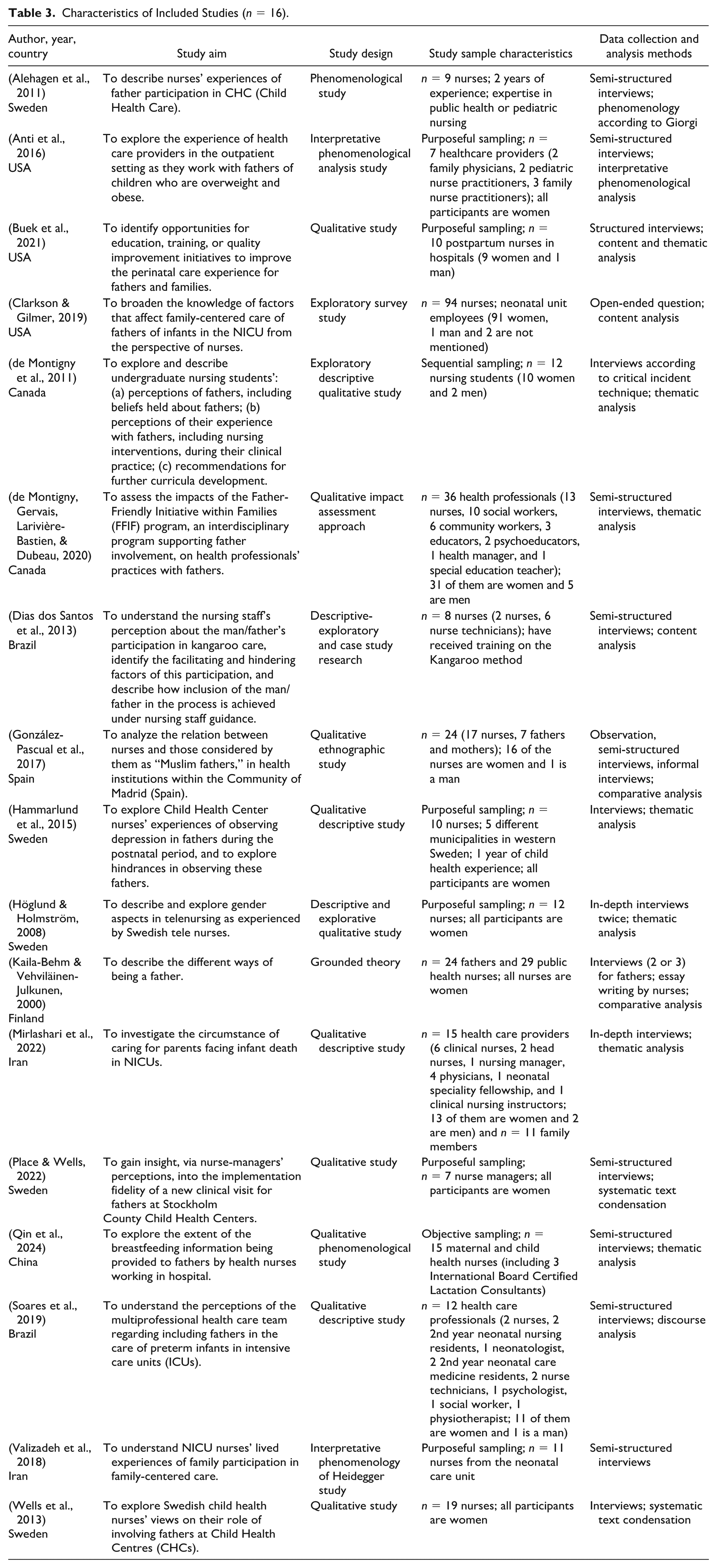
Two reviewers (C.R. and I.L.) extracted and organized the data from the selected studies into a preformatted table (Table 3) that included the following characteristics: name of first author, year and country of publication, aim of the study, study design, sample characteristics, and data collection and analysis methods.
Characteristics of Included Studies (n = 16).
Thematic synthesis, as proposed by Thomas and Harden (2008), was used to analyze the results of the selected studies. Through this approach, themes were identified and developed following a three-step process. For the first two steps, the reviewers coded the text line by line inductively to capture the meaning of each sentence. NVivo20 qualitative data analysis software (QSR International Pty Ltd, 2020) was used to collate the data presented in the “results” or “findings” sections of the included studies and facilitated coding. The reviewers then assembled the codes by similarities and differences into a tree structure that allowed the development of descriptive themes. Coding and data assembly were carried out by two reviewers (C.R. and I.L.), followed by team discussion (F.D., C.R., I.L., C.G.) to reach agreement on the descriptive themes. Analytical themes were then uncovered and discussed by the team to reach agreement on the thematic structure that best addressed the research questions and went beyond the original content of the selected studies.
Confidence in the Review Findings
The Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual) approach was used to assess confidence in the findings (Lewin et al., 2018). Thus, each finding was individually assessed for methodological limitations, consistency, adequacy, and data relevance (C.R.). The overall evaluation for each finding was subsequently ranked. To ensure robustness, a second reviewer (I.L.) validated this assessment.
Reflexivity
Reflexivity is an integral part of quality research and was used throughout this systematic review to ensure the integrity and reliability of the results (Finlay, 2002). To this end, the researchers discussed their own personal and professional experiences with fathers of young children and adolescents to be aware of the subjective and intersubjective elements that might influence their interpretation of the data. Thus, throughout the research process, potential blind spots or biases were examined (Kingdon, 2005).
Results
Study Characteristics
The studies in this thematic synthesis involved 287 nurses (n = 249 nurses, n = 8 nurse technicians, n = 8 nurse managers, n = 5 nurse practitioners, n = 2 head nurses, n = 12 student nurses, n = 2 nursing residents, and n = 1 clinical nursing instructor) from eight different countries: Sweden (n = 5), United States (n = 3), Brazil (n = 2), Canada (n = 2), Iran (n = 2), China (n=1), Finland (n = 1), and Spain (n = 1). The sample represented 224 women, 5 men, and 58 nurses whose gender was not identified in the articles (n = 6). The selected studies used a variety of qualitative research approaches, most used interviews as a data collection method. Table 3 presents details of the study characteristics.
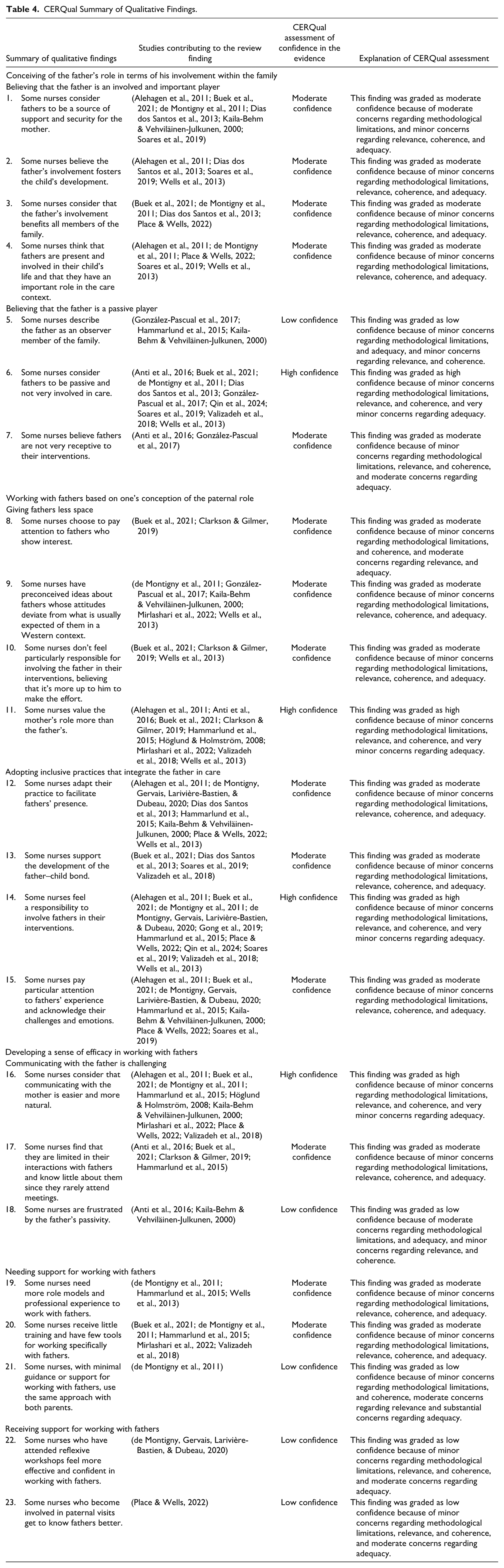
The confidence level assessments of the findings using the CERQual approach are presented in Table 4. A total of 23 statements of findings were generated, of which four had a high confidence level, 14 a moderate confidence level, and five a low confidence level.
CERQual Summary of Qualitative Findings.
Thematic Synthesis Findings
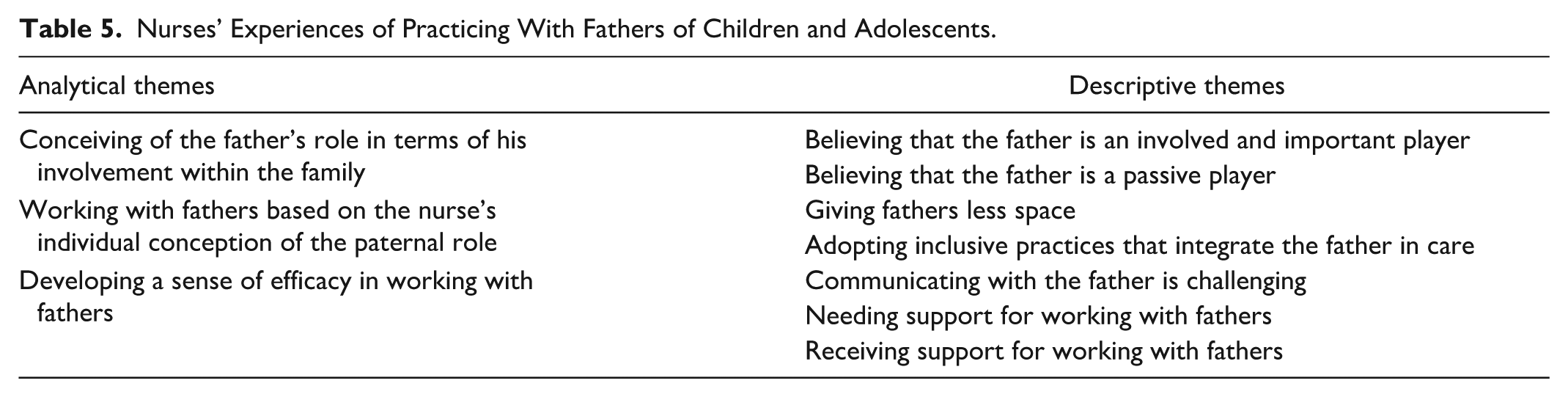
From the thematic synthesis carried out as part of this qualitative systematic review, seven descriptive themes were constructed and apprehended under three analytical themes: (a) conceiving of the father’s role in terms of his involvement within the family; (b) working with fathers based on the nurse’s individual conception of the paternal role; and (c) developing a sense of efficacy in working with fathers. These descriptive and analytical themes are illustrated in Table 5.
Nurses’ Experiences of Practicing With Fathers of Children and Adolescents.
Analytical Theme 1: Conceiving of the Father’s Role in Terms of His Involvement Within the Family
Nurses’ conception of the father’s role within the family was shaped by the beliefs they held about him. For some, the father was an involved and important player in the family unit, whereas others saw him more as a passive player.
Believing That the Father Is an Involved and Important Player
Many nurses held the belief that fathers were actively engaged and significant contributors within the family structure, deeming their involvement advantageous for all family members (Buek et al., 2021; de Montigny et al., 2011; Dias dos Santos et al., 2013; Place & Wells, 2022). According to these nurses, contemporary fathers were viewed as sharing responsibilities for childcare with mothers and actively participating in both caregiving activities and health-related appointments (Alehagen et al., 2011; de Montigny et al., 2011; Place & Wells, 2022; Soares et al., 2019; Wells et al., 2013). Furthermore, this group of nurses perceived fathers as sources of support and security for mothers, playing a crucial role in providing emotional and practical assistance (Alehagen et al., 2011; Buek et al., 2021; de Montigny et al., 2011; Dias dos Santos et al., 2013; Kaila-Behm & Vehviläinen-Julkunen, 2000; Soares et al., 2019). In addition, these nurses acknowledged the significant impact fathers had on a child’s development, emphasizing their crucial role in fostering positive growth and well-being (Alehagen et al., 2011; Dias dos Santos et al., 2013; Soares et al., 2019; Wells et al., 2013).
I think . . . that with the pregnant mother, I think dad is a very important piece, the contact with the woman [. . .] the husband accompanies the woman, they feel safer, happier. Everything is a set. Help in the development of the child, I believe so. (Neptune). (Dias dos Santos et al., 2013)
Believing That the Father Is a Passive Player
In contrast, there was a subset of nurses who perceived fathers as passive participants with limited involvement in childcare responsibilities (Anti et al., 2016; Buek et al., 2021; de Montigny et al., 2011; Dias dos Santos et al., 2013; Gong et al., 2019; González-Pascual et al., 2017; Soares et al., 2019; Valizadeh et al., 2018; Wells et al., 2013). According to their perspectives, these fathers were often described as observers who maintained a certain distance from the mother–child dyad (González-Pascual et al., 2017; Hammarlund et al., 2015; Kaila-Behm & Vehviläinen-Julkunen, 2000) and might not have been particularly receptive to nursing interventions (Anti et al., 2016; González-Pascual et al., 2017).
A lot of the moms are traditionally the ones who are usually in charge of preparing meals, so they feel more connected to being able to do something to change [their child’s weight]. This same health care professional (HCP) went on to express understanding of fathers for not taking on a more active role related to norms associated with “traditional” roles. (Rebecca) (Anti et al., 2016)
Analytical Theme 2: Working With Fathers Based on the Nurse’s Individual Conception of the Paternal Role
Nurses’ conception of fathers’ involvement differed from one nurse to another and influenced their attitudes toward fathers during their interventions. Thus, nurses who perceived fathers as having a passive role tended not to give them much space; for example, they inquired less about their needs or involved them less in care. On the other hand, nurses who perceived them as involved and important adopted more father-inclusive practices and were able to involve them more in care.
Giving Fathers Less Space
This descriptive theme revolved around the prevailing tendency among some nurses to undervalue and give less space to fathers in the care of children and adolescents (Alehagen et al., 2011; Anti et al., 2016; Buek et al., 2021; Clarkson & Gilmer, 2019; Hammarlund et al., 2015; Höglund & Holmström, 2008; Mirlashari et al., 2022; Valizadeh et al., 2018; Wells et al., 2013). Despite societal changes in family models, certain nurses continued to prioritize the mother’s role, and had specific expectations and preconceived notions of fathers that sometimes led to discriminatory behaviors, as could occur when fathers’ attitudes deviated from what was usually expected in a more Western context (de Montigny et al., 2011; González-Pascual et al., 2017; Kaila-Behm & Vehviläinen-Julkunen, 2000; Mirlashari et al., 2022; Wells et al., 2013).
I might spend less time due to talking/questions. In my practice, typically fathers talk less than mothers. They do not always want constant engagement. (Nurse participant) (Clarkson & Gilmer, 2019) They sit down, they don’t get up, the woman gets up, burdened, in pain, to change the child, to change him and he, the typical Arab, doesn’t move. (E1-P, Nurse) (González-Pascual et al., 2017)
Other nurses felt no particular responsibility for involving fathers in their interventions. Rather, they considered that it was up to the father to get involved, and they paid more attention to those who showed interest (Buek et al., 2021; Clarkson & Gilmer, 2019; Wells et al., 2013).
Just depends on the person. If the father is willing to talk, interact, learn, and be cooperative, I am more likely to spend time working with him. (Clarkson & Gilmer, 2019)
Adopting Inclusive Practices That Integrate the Father in Care
Nurses who strived to integrate fathers into care adopted inclusive attitudes that reflected the value they ascribed to the father’s role (Alehagen et al., 2011; Buek et al., 2021; Place & Wells, 2022; Wells et al., 2013). They paid close attention to fathers’ experience and acknowledged their unique challenges and emotions (Alehagen et al., 2011; Buek et al., 2021; de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020; Hammarlund et al., 2015; Kaila-Behm & Vehviläinen-Julkunen, 2000; Place & Wells, 2022; Soares et al., 2019).
That’s the most important work we have, to see and ask questions about what it like really is. It affects the child if the family is not feeling well. So it’s really important to involve the fathers—they belong to the family and the child. (Participant 7) (Hammarlund et al., 2015)
These nurses felt a responsibility to involve the father during their interventions, considered the father’s presence and involvement to be essential when performing a comprehensive family assessment (Alehagen et al., 2011; Buek et al., 2021; de Montigny et al., 2011; de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020; Gong et al., 2019; Hammarlund et al., 2015; Place & Wells, 2022; Soares et al., 2019; Valizadeh et al., 2018; Wells et al., 2013), and supported the development of the father–child bond (Buek et al., 2021; Dias dos Santos et al., 2013; Soares et al., 2019; Valizadeh et al., 2018). They also strived to adapt their professional practice and service provision to support fathers’ presence while encouraging them to be more active in childcare (Alehagen et al., 2011; de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020; Dias dos Santos et al., 2013; Hammarlund et al., 2015; Kaila-Behm & Vehviläinen-Julkunen, 2000; Place & Wells, 2022; Wells et al., 2013).
. . . [During the home visit] if the father goes to the kitchen, you can say “I’ll wait to continue until you come back.” So we [nurse and mother] just talk about something that maybe isn’t so important for both of them. (Place & Wells, 2022)
Analytical Theme 3: Developing a Sense of Efficacy in Working With Fathers
The development of a sense of efficacy in nurses working with fathers was characterized by certain communication challenges, as well as by needing and receiving support in their professional practice.
Communicating With the Father Is Challenging
When it came to communicating with fathers, access was the first challenge nurses faced (Buek et al., 2021; Clarkson & Gilmer, 2019). Nurses reported being limited in their interactions with fathers and not knowing them well, as fathers seldom attended the various meetings involving health care (Anti et al., 2016; Hammarlund et al., 2015). Moreover, nurses sometimes felt they got to know the fathers primarily through the mothers’ stories (Anti et al., 2016; Hammarlund et al., 2015).
I can’t remember the last time I had a discussion with a dad about weight and exercise because it’s been with moms. I can probably count on one hand the number of times I’ve ever had a dad involved in that kind of discussion, just because they’re not there for the visit. I have been a nurse practitioner since 1998, and in several states, and it hasn’t been any different in any of them. (Della) (Anti et al., 2016)
Then, many nurses found it easier and more natural to communicate with the mother (Buek et al., 2021; de Montigny et al., 2011; Hammarlund et al., 2015; Höglund & Holmström, 2008; Mirlashari et al., 2022; Valizadeh et al., 2018) and found some fathers’ passivity toward care frustrating (Anti et al., 2016; Kaila-Behm & Vehviläinen-Julkunen, 2000).
Of course, it’s easier to talk to a woman, we have more in common . . . it’s generally easier to understand, we have the same view on things so to speak. // It’s generally speaking easier to understand, because we share a common . . . You often get more emotions from female callers . . .// To a mum I might say “yes it’s hard to watch them [children] feeling bad with a high fever and everything, of course it is, but when it’s a virus infection there’s nothing to do about it, it takes its time but they’ll be well soon.” They need caring. But to a dad you don’t say such a thing in that tone of voice. (Nurse 1) (Höglund & Holmström, 2008)
They also added that the difficulty in establishing a connection might have stemmed from the fact that fathers were more assertive and demanding about care (de Montigny et al., 2011; Höglund & Holmström, 2008; Kaila-Behm & Vehviläinen-Julkunen, 2000). However, in some cases, fathers’ enthusiastic attitude facilitated the development of a good relationship with nurses, some of whom even considered it easier to interact with fathers than with mothers (Alehagen et al., 2011; Place & Wells, 2022).
Needing Support for Working With Fathers
Nurses reported a need for professional role models when working with fathers, especially if they were inexperienced, as they did not always know how to intervene (de Montigny et al., 2011; Hammarlund et al., 2015; Wells et al., 2013). In such situations, nurses became uncomfortable and dissatisfied with their practice (Hammarlund et al., 2015). Many nurses reported having received little specific training related to working with fathers, and the tools available to them to interact with families were primarily developed for mothers (Buek et al., 2021; de Montigny et al., 2011; Hammarlund et al., 2015; Mirlashari et al., 2022; Valizadeh et al., 2018). In the absence of specific guidelines and support for working with fathers, nurses used the same approach for both parents (de Montigny et al., 2011).
[. . .] we were told it is important to involve fathers, but we were not shown how to . . . if there were specific things we had to check with fathers, it would be easier. (Lara) (de Montigny et al., 2011) We don’t have a method for how to deal with fathers who feel bad. Today we’re doing nothing, and it doesn’t feel good. We need a methodology that involves fathers. (Participant 10) (Hammarlund et al., 2015)
Receiving Support for Working With Fathers
Nurses who had been introduced to various father-inclusive practices had learned to better understand the specific attributes of this clientele and had been able to gain more skill in working with them (de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020; Place & Wells, 2022). Attending various training programs helped nurses feel more effective and confident in their work with fathers (de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020; Place & Wells, 2022).
Well, I ask if they have questions, but obviously they never do. But I always have some for them, and I try a lot to make jokes. Humour . . . then I talk about hockey, and I tell them I’m going to check my cell phone to see the score. (Nurse clinician) (de Montigny, Gervais, Larivière-Bastien, & Dubeau, 2020) I think that now that I have another method, another way and other questions, and that is maybe why I have found them [now]. I have had many fathers who, now they have several children, I’ve now learnt that the first time, they didn’t feel good, but I didn’t see it at the time. (Nurse-manager 3) (Place & Wells, 2022)
Discussion
The purpose of this review was to systematically synthesize the qualitative evidence on nurses’ experience of interacting with fathers when providing care to their children and adolescents in various contexts. Three analytical themes were identified: (a) conceiving of the father’s role in terms of his involvement within the family, with the subthemes believing the father is an involved and important player and believing the father is a passive player; (b) working with fathers based on the nurse’s conception of the paternal role, with the subthemes giving fathers less space and adopting inclusive practices that integrate the father in care; and (c) developing a sense of efficacy in working with fathers, with the subthemes finding it challenging to communicate with the father, needing support for working with fathers, and receiving support for working with fathers. These results are discussed below under three key headings: (a) working with fathers, a way to promote diversity, equity, and inclusion in the health care; (b) nurses’ knowledge about men and fathers; and (c) culture and beliefs at the heart of nurses’ practice with fathers.
Key Point 1: Working With Fathers, a Way to Promote Diversity, Equity, and Inclusion in the Health Care
Changes in the family structure, particularly related to who are considered members of the family, have created many challenges. Recently, the conceptualization of the father’s role has taken on a new aspect with the growing worldwide movement promoting diversity, equity, and inclusion. Not only do nurses need to consider diversity in the family structure and functioning, but they also have to consider gender-based health disparities (Selwyn & Thomas, 2023) and promote health equity (Gray et al., 2023). In this study, nurses tended to maintain a traditional conception of the father’s role, often approaching the father as a passive player. By doing so, they tend to focus their attention and their care on the mother and the child, compromising father’s access, fair treatment in care and development opportunities. As a member of the systems that have an impact on the health of the fathers but also on family system, nurses should contribute to families’ capacity to fulfill their social functions (e.g., economic support; education; health and mental health; protection of vulnerable family members; affection and caring; Feetham, 2018), which they can do by promoting and supporting father involvement. This should be done with careful consideration and respect as family dynamics and gender roles are influenced by cultural and ethnical origins of both parents. Promoting and supporting father involvement, in a way coherent with the increasing diversity in family structure, functioning, and parental roles, is a powerful strategy to reach a more egalitarian distribution of family responsibilities and reduce gender-based inequalities (Secrétariat à la condition féminine, 2022). It could also contribute to disrupt the pathway between social marginalization, early life stress, and negative health outcomes for children (Taha et al., 2024) as father involvement is a protective factor against poverty during infancy (Allen & Daly, 2007). Including fathers in care includes proactively and directly asking them about how they would like to be included in the care of their child. Developing abilities to better work with men and fathers is the responsibility of the nurses and health care providers to infuse equity and address health disparities, and for this, knowledge about men and masculinities is essential, as well as about sex and gender discrimination in the health services (Selwyn & Thomas, 2023).
Key Point 2: Nurses’ Knowledge About Men and Fathers
The results showed that nurses included fathers when they perceived them as interested in being involved. In those cases, they appeared to be at ease with carrying out educational interventions perceived as suitable and useful for meeting fathers’ learning needs in relation to their child’s care. Conversely, when fathers did not spontaneously express a desire to learn or be involved, nurses felt uneasy and appeared not to know how to interact with them. They were unable to explore the fathers’ vision of their role or to encourage them to become more involved. A meta-ethnographic study showed that fathers’ caregiving experiences in medical settings continue to be shaped by health professionals’ conceptions of masculinity and fatherhood (Postavaru et al., 2021). Fathers have reported not feeling listened to or valued. They are often solely considered as a support to the mother, while their own support needs remain unaddressed. They expect nurses to be more proactive in addressing their needs for support, such as asking them how they feel about their role as father (Hrybanova et al., 2019; Postavaru et al., 2021). The findings of the present study raise questions regarding nurses’ knowledge about fathers’ involvement and masculinity issues. Generally, the nurses seemed unaware of the variety of ways in which men can express their masculinity. For example, to cope with challenging situations, fathers who adhere to traditional masculinity norms may adopt evasive strategies such as alcohol abuse, longer working hours, and hiding their emotions (Polita et al., 2023). In such cases, nurses could misinterpret fathers’ behavior and be less sensitive to how these men might express their needs or suffering. This translates into a kind of inadequacy, with nurses not knowing how to react when fathers take a different stance than what they expect. Most of the nurses in this study were women, which may also have had an impact on their interventions with fathers. Female nurses may find it easier to communicate with mothers and family members of the same gender (Buek et al., 2021), which could be considered an unconscious bias. Furthermore, fathers might be more open to expressing needs and concerns to male nurses, given that in traditional masculinity they cannot show weakness to women or within the family.
A cross-sectional study of nurses’ attitudes regarding the importance of families in nursing care showed that they do consider families to be important. However, being a younger nurse with a basic education, minimal hospital experience, and no personal experience of family illness were predictors of less supportive attitudes toward family inclusion in nursing care (Østergaard et al., 2020). Within the family-centered care approach—as recommended internationally by World Health Organization (WHO)—the fathers’ voice and involvement in family care and health are as important as the mothers. Therefore, nurses’ beliefs play an essential role in determining whether they think it is important to involve fathers or whether they consciously or unconsciously decide they do not have time to involve the fathers.
Key Point 3: Culture and Beliefs at the Heart of Nurses’ Practice With Fathers
Parenting roles, especially the role of father, are strongly influenced by culture, and nurses’ cultural background may influence their beliefs about fathers. As immigration increases, nurses are encountering a greater diversity of beliefs and behaviors related to the paternal role. Combined with their own beliefs, both about the importance of paternal involvement and about the family structure and functioning of certain ethnocultural groups, this diversity can cause uneasiness among nurses. Unable to decipher the expectations and needs of fathers from other ethnocultural groups than their own, nurses may prefer to stand back rather than risk making seemingly embarrassing comments or interactions faux pas. Beliefs regarding the importance of fathers’ role in the family can also impact nurses’ adoption of father inclusive practices, such as making space for fathers and recognizing and addressing their needs.
Relevance for Family Nursing Practice
The results of this study inspire recommendations to improve family nursing education to strengthen clinical practices. These results underscore the need to better define family nurses’ role in supporting fathers’ involvement in various care and cultural contexts across the life course. When nurses are taught about the specifics of masculinity issues and the benefits of fathers’ involvement for all family members, their unconscious biases and preconceptions regarding men and parenting roles surface more overtly. With this newfound awareness, they are better equipped to overcome biases and hesitance to interact with fathers. Nurses trained in implementing father inclusive practices have a stronger sense of efficacy and are more able to invite fathers to participate in care, to identify their needs, and to support them in their parenting role (Dubeau et al., 2023).
When developing this type of training, it is useful to actively involve fathers in co-creating interventions that address their needs. Partnering with them in the design of curriculum and innovative programs can increase awareness among students and nurses. Different teaching strategies, such as simulations, can help nurses develop competencies in exploring fathers’ role, expectations, and needs.
While nurses can, as individuals, implement father inclusive practices in their family-centered care approach, as recommended by the WHO (2015), the health organizations in which they work also need to be inclusive of paternal realities. Openness, knowledge, and institutional support are three documented elements that support the advancement of father inclusive practices (Dubeau et al., 2023). For example, it is known that when health organizations value father inclusion, this positively influences nurses’ practices. As such, nurses and health care managers need to work together to foster father friendly health care environments. Developing father inclusive communities of practice can provide a valuable tool for implementing change on a broader scale.
Limitations
This study has some limitations. One is the limited quality level of certain themes due to the fact that some themes were only informed by one article. However, these themes were important in providing a comprehensive perspective and could not be ignored. A second limitation is that the majority of studies surveyed were carried out with female nurses. Thus, the results might not adequately reflect male nurses’ attitudes and beliefs regarding fathers of children and adolescents, nor the male perspective regarding their sense of efficacy in collaborating with fathers.
Conclusion
Globally, there is a movement to promote diversity, equity, and inclusivity. Nurses are on the forefront of embracing the family unit as a whole and directly addressing each family member’s role to identify and involve the significant players in the child’s health care. As such, nurses are in a privileged position to promote fathers’ status as being on equal footing with mothers within a family-centered care approach and to act as ambassadors for fathers, mothers, and co-parents.
Footnotes
Acknowledgements
The authors wish to acknowledge Mrs Donna Riley, editor and translator, for her assistance in translating the manuscript into English.
Author Contributions
DE MONTIGNY was responsible for conceptualization, formal analysis, funding acquisition, project management, supervision, validation, visualization, and writing of the original draft and review & editing.
RENÉ and LANDRY were responsible for data curation and contributed to formal analysis, investigation, project management, validation, visualization, and writing of the original draft and review & editing.
Brødsgaard, POLITA, DANFORD, SHEPPARD-LEMOINE, IKEDA, NASCIMENTO, SOMANADHAN, and ALVARENGA contributed to validation and writing (review & editing).
GERVAIS was co-responsible for conceptualization, funding acquisition, supervision and contributed to validation and writing of the original draft and review & editing.
Data Availability
The data used in this qualitative systematic review are derived from primary articles cited in the manuscript. Full references for these studies are available in the References section, and interested readers can access the original data by consulting these sources.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Fonds de recherche du Québec—Société et culture, through funding attributed to the Paternity, Family and Society Research Group as well as a grant from the Pole of expertise and research on men’s health and well-being.
Ethical Considerations
The research presented in this manuscript was approved on December 23rd 2020 by the Université du Québec en Outaouais Research Ethics Committee (protocol number 2021-1516) and has ongoing ethic certification.
Consent to Participate
Not applicable
Consent for Publication
Not applicable