
Abstract
A child’s cancer diagnosis has a significant impact on the lives of grandparents. Grandparents experience the stress of worrying about both their adult children and their grandchildren. Our study aimed to explore the lived experience of grandparents of children diagnosed with cancer. A qualitative design involving semi-structured interviews was used and data were analyzed using reflexive thematic analysis. Twenty grandparents aged 41 to 77 years were interviewed. Six themes were identified: (a) Diagnosis: changing everything; (b) Aspects of treatment: A different world; (c) Sandwich generation; (d) Family: Worrying about everyone; (e) Balancing work; and (f) It’s like suddenly a door opens. Our study demonstrates the life-changing impact of having a grandchild diagnosed with cancer. It expands on existing knowledge and shows that, due to an aging population and demographic changes, some grandparents must juggle the demands of caring for aging family members and working while supporting adult children and grandchildren.
The diagnosis of childhood cancer is a life-changing event that profoundly affects both the child and their family members (Kearney et al., 2015). Due to the complexities of treatment, families need to alter many aspects of their lives to accommodate treatments and care for a child with cancer (Wakefield et al., 2014a). Grandparents often play a pivotal role when a child is diagnosed with cancer, taking on additional responsibilities, and in some cases, moving in with the family to care for siblings and providing care for the child in the hospital (Kelada et al., 2019; Wakefield et al., 2014a, 2017).
These additional responsibilities significantly disrupt grandparents “normal” life (Moules et al., 2012b). Wakefield et al. (2017) found that grandparents experience a lower quality of life (QOL) and lower physical health compared with controls and have higher rates of depression, anger, and anxiety. Many grandparents also have their own health conditions which can impact how they manage the changes in lifestyle (Wakefield et al., 2014a).
Grandparents’ experiences have been described as “double grief,” worrying about their grandchild diagnosed with cancer (GDWC) and their adult children (AC) (Hall, 2004; Moules et al., 2012a). Family communication changes after a child is diagnosed with cancer and grandparents must negotiate the complexity of their new roles (Wakefield et al., 2014b). Moreover, as their focus is on caring for their AC (the parents of the child with cancer) and their grandchildren, grandparents have revealed that they cannot express their distress as they are reluctant to place additional burdens on their AC (Charlebois & Bouchard, 2007; Moules et al., 2012a; Wakefield et al., 2014b). Grandparents have also been found to have concerns about the information provided to them related to their grandchildren’s cancer (Wakefield et al., 2014b). Grandparents reported that they needed more direct information from health care professionals (HCP) so they would not have to rely on parents for information (Findler, 2014; Moules et al., 2012b; Wakefield et al., 2014b).
Much of the research on childhood cancer focuses on the impact on the nuclear family, and there are limited qualitative studies that have examined the experiences of grandparents of children with cancer (Findler, 2014). There is a need to further explore grandparents’ experiences of childhood cancer to gain a better understanding of how the cancer diagnosis and treatment of their grandchild impacts their lives (Charlebois & Bouchard, 2007; Moules, et al., 2012a; Wakefield et al., 2014a, 2017). This must include a specific focus on how changing demographics have impacted their experiences. In this study, we aimed to explore the lived experience of grandparents of children diagnosed with cancer.
Research Design
The hermeneutic phenomenological approach was used to explore what people “think” about their experiences (Wojnar & Swanson, 2007). This approach was chosen as it aims to develop insight into how people make meaning from their experiences, with a focus on capturing “what it [is] like” to be a grandparent of a child with cancer (Eddles-Hirsch, 2015). We used a qualitative method involving interviews of grandparents as it recognizes the importance of individuals’ experiences being described in their own words (Denzin & Lincoln, 2013). Semi-structured interviews were used, enabling a more natural form of communication and allowing for the gathering of clear information regarding how participants felt about their experiences (Leavy, 2017).
In this study, we were informed by ecological systems theory. This theory posits that a person’s well-being is dependent on interrelated and complex factors within the social system within which they are situated (Bronfenbrenner, 1979). It emphasizes the interconnectedness of people and that the well-being of one person affects others (Murrell, 1978). Ecological systems theory provides a conceptual framework for articulating the necessity to look at the context surrounding the child and highlights the need for analysis of childhood cancer to include an examination of those who are proximal to the child, such as parents and extended family including grandparents (Darling, 2007; Murrell, 1978).
We conducted this study in accordance with ethics approval attained through the Curtin Human Research Ethics Committee (HRE2021-0119) in March 2021.
Recruitment and Procedure
Participants were drawn from various childhood cancer networks throughout Australia. They were initially recruited by convenience sampling as the population is small and recruitment can be difficult. We then moved to purposive sampling to reach participants from different groups, including grandparents whose grandchildren had received varying cancer diagnoses. Recruitment notices were placed on closed oncology families’ Facebook pages. Access to these closed groups was facilitated by (JD’s) status as an insider researcher and a parent of a child who was diagnosed with cancer. Childhood cancer organizations also assisted by placement of recruitment notices on social media. We also used snowball sampling, whereby initial participants were asked to nominate other eligible participants (Parker et al., 2019).
Inclusion/Exclusion Criteria
Participants were grandparents whose grandchild was 17 years or younger and who were currently receiving or had completed cancer treatment within the previous 15 months. Adults who functioned in the role of grandparent were included. Both biological and step-grandparents and multiple grandparents from the same family were included. Bereaved grandparents were ineligible for our study.
Data Collection
Interviews were conducted by (JD), either by video teleconferencing (Teams or Zoom) or at a location suitable to participants between August 2021 and December 2021. Audio recordings of the interviews were made with a digital recorder. Before the interview, all participants were given a study participant information sheet, a consent form, and a demographic questionnaire which included participants’ education levels, ethnicity, and work status. We used a flexible interview guide to inform the interview process; an example of an interview question is “How has your grandchild’s cancer diagnosis impacted your family roles and responsibilities?” Prompt questions were also used to elicit further information. We developed interview questions from a review of previous research and consultation with consumer representatives. A preliminary analysis of initial interviews was also used to refine questions with minor amendments made to prompt questions. At the commencement of the interview, (JD) provided a summary of the research topic before confirming the participant had read and understood the participant information sheet. Consent to audio-record the interview was sought. We provided participants with options to cease/pause the interview. Participants were given support services details and offered a $20 gift card as an honorarium.
We continued recruitment until it was deemed that the data being analyzed contained an in-depth exploration of participants’ experiences. Data collection can never be “complete,” and qualitative research seeks to obtain rich data that achieves an in-depth understanding (Guest et al., 2020). We relied on the concept of information power, which outlines that the more in-depth and richer the data, the fewer the number of participants needed (Malterud et al., 2016). As such, we ceased recruitment when it was believed that in-depth and rich information had been provided (Guest et al., 2020).
Data Analysis
We conducted data collection and thematic analysis concurrently (Braun & Clarke, 2019). We completed transcription as soon as possible after each interview via the online transcription service rev.com, or manually by (JD). All interviews were transcribed verbatim, and all individual identifiers were removed. Data were analyzed using Braun and Clarke’s six-phase reflexive thematic analysis process (Braun & Clarke, 2019). First, we sought to develop familiarization and immersion with the data, so after transcription, all interviews were listened to by (JD; with any necessary amendments made to transcripts for accuracy). The transcripts were then read and re-read by (JD) to look for common patterns, and notes completed on initial responses. Second, after reading transcripts, codes were developed using a manual paper-based process with codes attached in the margins. The third phase involved codes being reviewed and analyzed by (JD) to develop initial themes across the data. The fourth phase involved the development and review of themes by all authors. To assist in the fourth phase, a thematic map was developed to graphically represent findings and review themes. In the fifth phase, themes were reviewed and revised by all authors to ensure unnecessary themes were excluded, and names were given to each theme. Finally, themes were converted into a report by (JD) and this was reviewed by all authors.
The guidelines for Consolidated Criteria for Reporting Qualitative Research (COREQ) were followed to ensure quality and rigor (Tong et al., 2007). As outlined by Braun and Clarke (2019), the reflexive approach aims to acknowledge the researcher’s active role in interpreting data, and during the process, the researchers were aware of their reflexive responses. As an insider researcher, (JD) was mindful to reflect on their experiences and how this impacted the research. (JD) kept a reflexive journal to record personal observations (Braun & Clarke, 2020). During the research process, (JD) also kept logs of research decisions and modifications to the research protocol. This measure aimed to improve the dependability of the research process (Johnson et al., 2020; Tong et al., 2007). We consulted with two consumer representatives who were grandparents with lived experience as grandparents of a child with cancer. They provided direct input on research methods and provided input on interview questions and forms to ensure the study materials were easy to understand. Involving consumers ensures that the research is inclusive and designed to appropriately reflect participants’ views (Happell & Roper, 2007). To achieve member checking, we also randomly selected seven participants and emailed them an overview of the final themes (Happell & Roper, 2007). Five participants provided feedback that the themes were an accurate reflection of their experiences. Two participants did not respond to the email. These measures in combination ensured that the analysis was credible, transferable, confirmable, and dependable (Johnson et al., 2020).
Research Findings
A total of 20 grandparents—13 grandmothers (GM) and 7 grandfathers (GF)—were interviewed as part of our study. Grandparents were aged between 41 and 77 (median=65 years, SD=9). Fifteen grandparents were still working either part-time or full-time and 5 were retired. The interviews were completed either face-to-face (10) or via teleconferencing (10). Each interview was on average 61 min long (35–79 min). Additional demographic details are provided in Table 1.
Sample Sociodemographics (N=20 Participants).
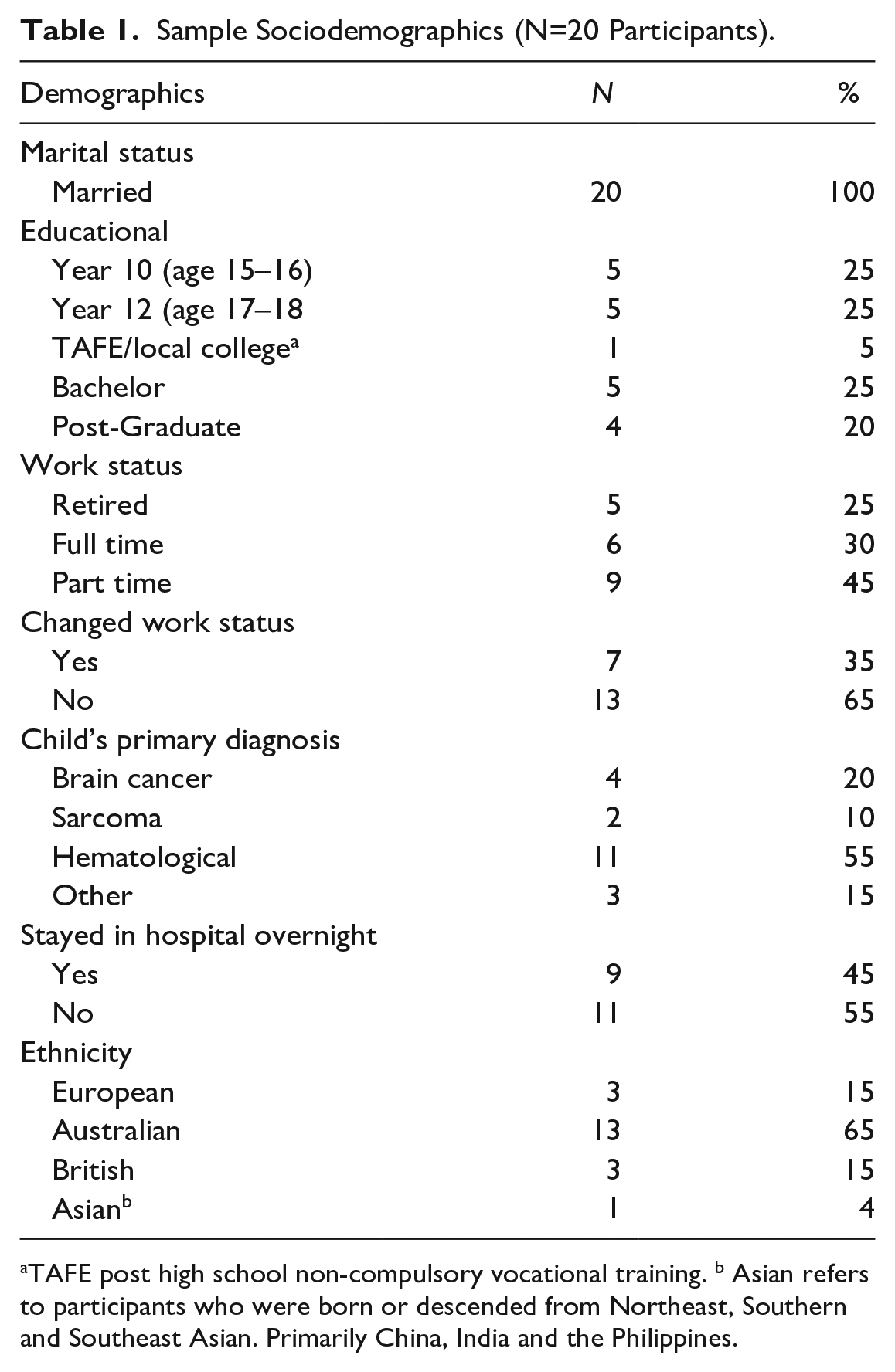
TAFE post high school non-compulsory vocational training. b Asian refers to participants who were born or descended from Northeast, Southern and Southeast Asian. Primarily China, India and the Philippines.
Themes
Six major themes were identified (listed below). Due to the complexity of human emotions, there are some overlaps between themes, but all outline specific aspects of grandparents’ lived experiences.
Diagnosis: Changing Everything
This theme captured the grandparents’ reactions and feelings about hearing about their grandchild’s cancer diagnosis. Many grandparents described it as a shocking and life-changing moment, saying that “the minute they said oncology . . . my heart sunk because I knew oncology is cancer . . . our whole life is going to change forever” (GM). Many grandparents explained that a child’s cancer diagnosis was different to cancer they had experienced among adults, describing that having a child diagnosed with cancer “was wrong, so very wrong . . . it’s different in adults to when it’s children . . . Although you don’t cope you cope a whole lot better when it’s adults than when it’s children” (GM). As one GF described: Everything is going to go in a natural process . . . I’m going to get old and die, and then my kids are going to get old. That suddenly being flipped around to this tiny, little baby who had only just started this life was suddenly faced with dying in front of us . . . this was just not how it’s supposed to be. (GF)
Several participants also talked about how their grandchild’s cancer threatened their ability to think about the future, as described by one grandparent who said, “My family wouldn’t be complete without [GDWC] . . . how do [you] . . . think about future when such a precious child might not be part of it” (GM). Childhood cancer impacted not only the present but their ability to envision their families’ future.
Aspects of Treatment: A Different World
This theme describes grandparents’ responses to aspects of their grandchild’s treatment.
Sub-Theme: The Ward
This theme describes grandparents’ responses to attending the ward and witnessing their grandchildren receiving treatment. Visiting the ward appears to have been extremely distressing, as highlighted by one grandparent saying, “Every time I went to the hospital, I’d get there and walk through the door and be sick in the toilet” (GM). The complexities of the ward were difficult for grandparents to process; one GF stated, “Being on the ward, that’s an experience and half . . . with alarms going off all the time and the lines everywhere . . . and nurses changing this and that.” This response was even more pronounced for those grandparents who were directly involved in assisting the parents to care for their grandchild on the ward. One grandparent stated, “I had to hold [GDWC] down a lot because mother of the child wasn’t well enough . . . Holding her, knowing how scared she was and how angry she was with me” (GM). It appears that being directly involved with caring for the GDWC was emotionally distressing for grandparents, and while they stepped in to provide support, the experience came at a high cost for some grandparents.
Sub-Theme: Hyperalert—Keeping Your Grandchild Safe
This theme reflects grandparents’ concerns regarding their grandchild’s risk of infection. Many grandparents, particularly those who spent time on the ward, noted that they were fearful of spreading an infection to their grandchild. One GM described that “I would go home [from the ward] and think, ‘Oh my god I’ve got a sore throat now . . . he is going to catch something, and he is going to die and it’s going to be my fault.” This fear of infection resulted in grandparents adjusting their lifestyle to reduce risk to their grandchildren; for example, one GM described arrangements where, “if my husband’s sick, I move into the front of the house. He stays at the back of the house so that I’m less likely to get sick so that I can continue to . . . provide support.” Another GM described how continuing to work posed additional challenges: Another staff member was coughing so I just . . . showed her a photo of [GDWC] . . . and just said “have you got a cold?” . . . and explained to her if they have a cold and I catch it and go and see [GDWC] I can kill her. (GM)
Fear of infection impacted all aspects of their life: one grandparent said, “We’re very conscious of not being very social . . . and collecting germs to take to the hospital” (GF). In these quotes, it is evident that childhood cancer was an experience that impacts all facets of grandparents’ lives.
Sub-Theme: Steroids—Witnessing Changes to the Grandchildren
This theme explores grandparents’ perceptions of the negative impact of steroid treatment on their grandchildren. Grandparents highlighted that the steroids changed their grandchildren, as seen in one GM’s reflection that “the worst, worst part of it was watching [GDWC] disappear, her personality. She was gone.” Grandparents found it challenging to see their grandchildren change so much and the discomfort caused but this aspect of treatment was hard to witness: I hated seeing it . . . my little special boy being so upset . . . so hungry . . . so angry and there was nothing I could do to help him . . . I felt so helpless. And then I had to watch [AC] to cope with it all (GM).
Steroids were seen as a necessary part of treatment, but they still lamented their impact, saying that “I know he had to have the drugs . . . but gosh they came as such a high cost . . . the impact . . . on my grandchild and [AC] was just horrible” (GF). Grandparents appear to have witnessed the full impact of steroids, and the side effects of these treatments were difficult for them to process knowing it hurt both the GDWC and their AC.
Family: Worrying About Everyone
This theme explores how grandparents worry about all their family members.
Sub-Theme: Double Whammy
This theme captures grandparents’ feelings that having a GDWC meant that there were two levels of worry for both their AC and their grandchildren. Grandparents expressed what several grandparents termed the “double whammy.” Explaining how difficult it was having to worry about two loved ones, one grandparent said, “It’s a double blow . . . I think as grandparents it’s very hard because you got your children, you are concerned about . . . how they are coping, and then the grandchildren as well” (GF). Witnessing their AC having to care for a child with cancer and not being able to prevent the distress was difficult, as one grandparent recalled, “The hardest bit for me dealing with it . . . is that [AC] is my baby, and I can’t protect my baby . . . it’s how she feels because she can’t protect her baby, but she’s my baby” (GM). Grandparents appeared to have felt a sense of helplessness that they couldn’t protect their AC from the trauma. Several grandparents expressed concern about the long-term impact on their AC, as seen in this quote: This has to have an impact and I worry about [my adult daughter’s] health . . . it takes such a toll on her . . . she doesn’t eat properly and hardly sleeps . . . I try to help as much as I can, but he [GDWC] is so very, very sick, she never takes time to look after herself . . . so I have to worry about them both being sick . . . but only one is being taken care of . . . what is the long-term impact? (GM)
The complexity of the emotions that grandparents experience is evident, showing they worry for both the long-term health of their grandchildren and their AC.
Sub-Theme: Siblings—Adjusting to New Roles
This theme outlines grandparents’ thoughts regarding the impact on siblings of having a brother/sister diagnosed with cancer and their changed relationship with grandchildren. Many grandparents highlighted that they worried about the effect on siblings, with one stating, “It’s so hard on [the sibling], she misses her mum and her brother and worries so much . . . It’s horrendous . . . and then she [sibling] is often upset with me for taking her away from her mum” (GM). Several grandparents in our study moved into their AC’s home or had the sibling(s) of the GDWC move in with them to provide care. Other grandparents provided care for long periods when the child’s parents were at the hospital. These grandparents described how the change in roles (from grandparent to having to provide parental responsibilities) was difficult and they missed the pure grandparent role: Look, the hardest bit for me as a nana is taking on that parent role . . . I’ve always been close to these kids. . . . Once [sibling] said to me, “Oh, nana never says no.” Suddenly I had to say no. . . I’m doing the parenting role . . . so, when she needs to have rules, I have to say no. (GM)
Several grandparents also noted that it was difficult for siblings to have both grandparents and parents taking care of siblings as they often had different discipline styles. One grandparent who had moved in with their AC and grandchildren stated, “It’s really difficult for children, dealing with dad telling them one thing and grandparents telling them another thing” (GM). In these quotes, we can see that the grandparents were aware that they had different ways of caring for the siblings and that having two different routines created stress for the siblings.
Sandwich Generation
This theme details the experiences of grandparents who found themselves caring for multiple generations: their grandchildren with cancer, their AC, and their elderly parents. Some grandparents discussed the challenges of worrying and caring for their AC and grandchildren but also having to care for their elderly parents: I’m the one that’s always strong for everyone. I’m supporting the family. I’m the one that takes care of my mum and my dad and every appointment, doctors, this and that, powers of attorney . . . I seem to be the one that is helping everyone . . . That seems to be my role in the family. (GM)
These roles of having to care for different generations left some grandparents exhausted both emotionally and physically, with one GM reflecting: . . . there is no time for me to do anything but look after everyone else . . . some days I feel I’m going to collapse . . . but I can’t do that everyone needs me . . . I should go to the doctor to deal with my [medical condition] . . . but I just don’t have time. (GM)
Several grandparents also talked about the challenges of elderly parents with neurocognitive disorders who no longer could process the grandchild’s diagnosis. One GM described how “[my] mother understands, but she doesn’t remember. We talk today and she [participants’ mother] . . . gets upset because she’d never heard.” This grandparent also discussed the need to “protect my parents [great grandparents]” from the stress of the cancer diagnosis. The challenge of worrying about the impact of childhood cancer on the different generations and “protecting everyone” left grandparents feeling, as one GF described it, as though they were “carrying such a large burden . . . it’s so many roles.”
Balancing Work
This theme details the experiences of the 15 grandparents who were still working while their grandchild had cancer. Many expressed that it was difficult to combine working while worrying about their grandchild. Work was difficult on both an emotional and practical level. Emotionally, the juxtaposition of witnessing childhood cancer treatment and the normal routines of work was difficult. As one GM recalled: Emotionally, I found it quite difficult to leave there [the hospital], go to the office, and sit at my desk and think, how can I get back into work . . .. Some nights when I’d been . . . at the hospital [overnight] and had to go to work [in the morning] it just felt weird, and I thought, I’m not sure I can do both. (GM)
On a practical level, the demands of being in the hospital assisting with care and then going to work were exhausting for grandparents. One grandmother stated, “I was working and then going to the hospital till late at night and then repeat . . . I was exhausted but I had no choice . . . I had to do both . . . but at my age it was hard.” Grandparents also reported that it was often challenging to deal with routine aspects of work life: I found it really hard to go back to work. It took me four weeks to stop being tearful . . . I just didn’t engage in small talk. I found talking about mundane things like, “I have to buy [an] outfit” . . . I just couldn’t participate in that small talk. (GM)
The grandchild’s cancer diagnosis impacted the grandparents’ work life, with some grandparents indicating that they took time off from work to help care for their GDWC. This included taking “three months off . . . [because] I can’t do this and work as well” (GM). Others reported reducing work “I take my long service leave one day a week so I can be there [at the hospital]” (GM). They also adjusted work hours to enable availability to support their AC and grandchildren, with one GF explaining, “I just spoke to my boss about less hours and told him family come first . . . that meant less money, but you know . . . it’s what you do.” Many grandparents had the stress of juggling conflicting work and family responsibilities.
It’s Like Suddenly a Door Opened
This theme covers grandparents’ emotions regarding knowing children who had died from cancer. Grandparents who spent extended time on the ward were exposed to the loss of other children, and this had a profound impact on grandparents, with one explaining, “I’ve known so many children that have died now. It’s hideous that I have known children so well and they are dead, and I’ve been to children’s funerals” (GM). Grandparents reflected that they felt unprepared, stating that, “I see updates [Facebook] when another kid goes from the ward [dies] . . . It’s like suddenly a door opened and I know of this world that always existed, but we are not aware of it unless you really know somebody” (GM). Many indicated that they saw social media pages of children that they met on the ward and that reading about children they knew who were dying was hard: “I saw the [Facebook] update on [child in palliative care] . . . I just can’t see that without crying . . . I cry when I read [mother of a deceased child]’s posts” (GM). Some grandparents reflected that their friends did not understand, stating, “I think they’re taboo in western culture, or not just western [culture], in a lot of cultures. You don’t talk about certain things like that [death]” (GF). Grandparents appear to have felt isolated due to the lack of understanding by friends and the social taboos regarding death and children’s deaths specifically. Some grandparents experienced multiple deaths: The little girl [with cancer] that [GDWC] shared a room with, passed away and that was devastating . . . your heart breaks, no child should die . . . then after the first [death] you put up a bit of a barrier . . . and you move on to the next one and the next one and the next one and all the time hoping that it wasn’t going to be your grandchild. (GM)
We can see in this quote that the death of children from cancer impacts grandparents on two levels: first, from the sadness of seeing a child die, and second, because it increased their fear about the possible outcome for their grandchildren.
Discussion
In this study, we have explored the lived experience and multiple ramifications of having a grandchild diagnosed with cancer. We highlighted the emotional distress that grandparents encounter when their grandchildren are diagnosed and treated for cancer and how it impacts their lives. Ecological systems theory explains that individual family members do not exist in isolation and that each person’s experiences affect those around them (Bronfenbrenner, 1979). In our study, we can see that the diagnosis of the grandchild’s cancer impacts grandparents, and they experience many similar reactions to parents, including distress at witnessing their GDWC’s treatment. The ecological systems theory also posits that individuals sit within a larger socio-cultural macrosystem that influences their experiences. In our study, we can see that changes in demographics and cultural attitudes to workforce participation at the macro level have increased the negative impacts of a grandchild’s diagnosis, with grandparents now having to care for multiple generations and combine work with supporting their families (Bronfenbrenner, 1979; Buchanan & Rotkirch, 2018).
Many of the existing studies exploring grandparents’ experiences have not included data on grandparents’ work status or discussed the experiences of work (Kelada et al., 2019; Wakefield et al., 2014b). More than 75% of grandparents in our study were working either part-time or full-time. In recent decades, due to the aging population and the subsequent pressure on pension systems, the mandatory retirement age has increased labor force participation among older workers (Nagarajan & Sixsmith, 2023; Pilipiec et al., 2021). This coupled with cultural changes which have seen the increasing participation of women in the workforce has meant that more grandparents will still be in the workforce when their grandchildren are diagnosed with cancer (Moussa, 2019a). The balancing act for grandparents of combining both work and assisting in caring for their family was an issue raised frequently by grandparents and one of the major challenges.
Grandparents described both practical and emotional challenges. Practically, grandparents described the challenges of working during the day and then spending time caring for either siblings or GDWC. Emotionally, those grandparents who worked explained that it was difficult to deal with the mundane aspects of work when dealing with the trauma of childhood cancer. Previous research observed that grandparents often find it difficult to talk to friends and that this creates tension in friendships (Moules et al., 2012a). Our study expands this aspect to show that, for those in the workforce, normal office communication between colleagues is challenging. In addition, many grandparents altered work hours to accommodate their grandchild’s treatment. Research has shown that parents of sick children must modify work patterns and that families can face a loss of income due to changed work hours (Kelada et al., 2020). In our study, we can see that the financial impact of childhood cancer is not isolated to the immediate nuclear family and affects grandparents.
An important and novel finding of our study is the role that grandparents play in caring for three generations. Changing demographics and an aging population exacerbate the stress grandparents of children with cancer experience, as they are now often required to juggle caregiving for their elderly parents/relatives as well as assisting in caring for GDWC and supporting their AC (Moussa, 2019). Our participants highlighted the emotional toll that these differing roles caused and the difficulties in trying to care for multiple generations. They also observed that these conflicting demands meant that there was often no opportunity to engage in self-care. Previous research has shown that grandparents rarely seek support for their own needs, and it can be theorized that the need to care for multiple generations will only exacerbate this lack of self-care (Wakefield et al., 2014a).
Grandparents in our study outlined the overwhelming impact of their grandchild’s cancer diagnosis and treatment. This aligns with previous reports that grandparents described childhood cancer as one of the worst experiences when compared with other life events (Charlebois & Bouchard, 2007; Moules et al., 2012a). Despite not being the primary carer of their GDWC, grandparents experienced many emotions that were like those experienced by parents, including feeling devastated and having trouble accepting the diagnosis (Davies et al., 2023; Kahriman et al., 2020; West et al., 2015). The grandparents in our study played an important role in helping to provide care for the GDWC, including assisting with care on the ward. In this study, we have expanded on current knowledge to thoroughly explore the impact of assisting in providing care for GDWC.
Childhood cancer results in a crisis in the family, and parents often rely on grandparents to step in to provide support in multiple ways (Findler, 2014; Kelada et al., 2019). In our study, grandparents described providing practical support for the whole family, particularly in caring for siblings (Flury et al., 2021). Aligning with previous research, grandparents described feeling concerned about the impact on siblings and were worried about the disruption to their “normal” childhood (Flury et al., 2021; Wakefield et al., 2014a).
Our study adds to our understanding regarding siblings and demonstrates the negative impact on those grandparents who provided live-in or frequent care for siblings. All family members sit within social systems and have set roles within the family, and when a child is diagnosed with cancer, these roles and responsibilities often change (Tan et al., 2010). In modern society, grandparents normally spend time with grandchildren without the normal “strict routines” of everyday life. This normal role of grandparents has been described as “pleasure without responsibility” (Backhouse & Graham, 2011). In our study, the need for grandparents to move in or take over the parental roles for siblings appeared to have a negative impact on their role as grandparents, with grandchildren often seeing them in the “strict” parental role. The change in roles and shift to “parental role” appears to have created tension, and grandparents appeared cognizant that the shifting roles within the family created stress for siblings. They also highlighted that they missed the grandparenting role.
The grandchild’s cancer diagnosis significantly impacted the grandparents’ lives at multiple levels of the ecological system, including their social functioning. There has been conflicting research on the impact of childhood cancer on grandparents, with Findler (2014) finding that grandparents were able to maintain normal social support activities. In contrast, Hall (2004) showed that grandparents put their lives on hold to support grandchildren, including limiting social activities. An important insight that our study has revealed is that many grandparents modify their social functioning in response to their GDWC’s compromised immune system. Grandparents observed that their lives changed not only due to time commitments of supporting their AC and grandchildren but also due to concerns about spreading infections to their grandchildren. It appears that grandparents experience many similar responses to parents as seen in their reactions to the need for infection control (Davies et al., 2022; Young et al., 2002). Research about parents has shown that fear of infections was a cause of anxiety, and in our study, we can see that grandparents shared similar feelings regarding limiting their social life to protect their grandchildren (Yildirim Sari et al., 2013). Immune suppression experienced by children with cancer affects not only the nuclear family of parents and children but also those who are proximal to the family.
Consistent with previous studies, a major finding of our study was that grandparents experienced worry on two levels, both for their grandchild and for their AC the so-called “double grief” phenomenon (Charlebois & Bouchard, 2007; Flury et al., 2021; Hall, 2004; Wakefield, 2014a). Grandparents worried about the child with cancer and the sense they could not protect their AC from the pain of witnessing the cancer treatment. Previous researchers have found that parents, particularly mothers, experience distress after their child’s cancer treatment and worry about the long-term impacts on their children (Davies & O’Connor, 2023). Our study adds to our understanding of grandparents’ experiences of childhood cancer, showing that grandparents are cognizant of the potential for negative long-term psychological and physical impacts, not only on their grandchildren but also on their AC. Again, we demonstrate that grandparents’ worry occurs at multiple levels, with concern not limited to their GDWC.
Many grandparents described feeling that having a GDWC who could die was against the natural order of things. Bury’s theory of “biographical disruption” can be used to understand this reaction (Bury, 1982). This theory proposes that people have a predetermined vision for how their lives should be and that illness can “disrupt this vision.” Grandparents described how it should not be their grandchildren facing death, and that the “natural order of things” is that they should die before their grandchildren. This aligns with existing research that reported that grandparents felt a “sense of injustice” that their grandchildren were suffering (Charlebois & Bouchard, 2007).
In our study, grandparents were often involved in caring for grandchildren and were thus exposed to many of the realities of childhood cancer, including the death of children (Flury et al., 2021). We can see in our sample that individuals do not exist in isolation, and the larger social values in the macro system toward death and grief influence how grandparents experience childhood cancer (Bronfenbrenner, 1979). Current societal taboos around discussing death, particularly that of children, exacerbated the negative effects of child mortality from cancer. For some grandparents in our study, witnessing the death of children increased their fears regarding the outcomes for their grandchildren. Consistent with previous research, grandparents fear the long-term recurrence of their grandchild’s cancer, and seeing children die whom they had often become close to while attending the ward exacerbated this fear (Charlebois & Bouchard, 2007). Grandparents commented that they followed the Facebook pages of other children on the ward, and it could be suggested that the increase in exposure due to social media may have increased the level of distress when children die.
Limitations
A potential limitation of our study is that there may have been a selection bias, as only those grandparents who were involved in their grandchild’s care may have volunteered to participate. This may mean that it does not reflect the experiences of those who are less involved in a GDWC’s care. To address this concern, we used snowball sampling, requesting that participants passed on study information to other grandparents, including grandparents who visited the ward but did not provide respite care for their grandchildren. There were also no participants from culturally and linguistically diverse backgrounds. This lack of diversity may mean that the study findings are less transferable. Attempts were made to address this and two participants from non-English-speaking backgrounds expressed interest, but they withdrew before the interview, explaining that they felt nervous about the interview. This may be reflective of their language skills, and further studies are warranted to explore the needs of grandparents from non-English speaking backgrounds.
Clinical Implications
There are currently limited supports available to grandparents of children with illness/disabilities, with many health care services considering them external to the nuclear family (Novak-Pavlic et al., 2021). Grandparents play a vital role in the family of children with cancer, and they experience many of the same stressors as parents, including balancing work and care of the children—both that of siblings and the child with cancer. Importantly, we have shown that some grandparents now must manage juggling caring for multiple generations. It is therefore vital to provide psychological support to grandparents that recognizes the distinct impact of childhood cancer, particularly the impact of stress from worrying about multiple generations. Grandparents find it difficult to witness their grandchildren receiving treatment and need to be provided with appropriate psychosocial support to adjust to the realities and complexities of childhood cancer treatment. This should include providing information and advice on the impacts of specific aspects of treatment such as steroid treatment. The findings of our study would be beneficial to HCP in allowing them to understand the multiple demands on grandparents. Family members are interdependent and supporting grandparents helps the whole family. Care provided to families of children with cancer needs to be family-focused and include a consideration of the impact on grandparents.
Conclusion
In our study, we demonstrate that childhood cancer has a ripple effect, and its impacts are not limited to the nuclear family. Here, we have provided a thorough exploration of the impact of a grandchild’s cancer diagnosis, increasing our understanding of the ways in which grandparents’ lives are changed at multiple levels of the ecological model, including work, friends, social life, and roles within the family. Importantly, we have expanded upon existing knowledge to show that with an aging population, some grandparents now must juggle competing demands in both working and caring for aging families while trying to support their AC and grandchildren. Grandparents find themselves “sandwiched” between having to care not only for their AC and their grandchildren with cancer but also for their elderly parents. This burden created anxiety for grandparents as they feel squeezed between competing demands. These findings reflect changing demographics within society and the need to be aware of these issues when providing support to families and grandparents of children with cancer. We have highlighted the need for care provided to families of children with cancer to be aware of the role grandparents play and the need for support to include an acknowledgment of their role in the family.
Supplemental Material
sj-docx-1-jfn-10.1177_10748407231213862 – Supplemental material for Grandparents’ Experiences of Childhood Cancer: A Qualitative Study
Supplemental material, sj-docx-1-jfn-10.1177_10748407231213862 for Grandparents’ Experiences of Childhood Cancer: A Qualitative Study by Jenny Davies, Moira O’Connor, Georgia K. B. Halkett, Lauren Kelada and Nicholas G. Gottardo in Journal of Family Nursing
Footnotes
Acknowledgements
The research team would like to thank the Kids Cancer Support Group: Australian Hospital Childhood Oncology Families Facebook pages, Children’s Leukemia and Cancer Research Foundation, Sock it to Sarcoma, Leukemia Kids Australia, Rare Cancers Australia, Childhood Cancer Support, and the Other C-Word Child for assistance with recruitment of participants and provision of interview venues. Finally, and most importantly we would like to thank all the grandparents who so kindly contributed their time and shared their experiences to help develop a better understanding of childhood cancer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A/Prof Georgia Halkett is supported by a Cancer Council of WA Research Fellowship. The Behavioral Sciences Unit is proudly supported by the Kids Cancer Alliance. Dr Nicholas Gottardo is supported by the Perth Children’s Hospital Foundation Stan Perron Chair in Pediatric Oncology and Hematology. Jenny Davies is supported by Commonwealth Research Funding.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.