
Abstract
Family or friend caregivers’ concerns about assisted living (AL) residents’ mental health are reflective of poor resident and caregiver mental health. COVID-19-related visiting restrictions increased caregiver concerns, but research on these issues in AL is limited. Using web-based surveys with 673 caregivers of AL residents in Western Canada, we assessed the prevalence and correlates of moderate to severe caregiver concerns about residents’ depressed mood, loneliness, and anxiety in the 3 months before and after the start of the COVID-19 pandemic. Caregiver concerns doubled after the start of the pandemic (resident depressed mood: 23%–50%, loneliness: 29%–62%, anxiety: 24%–47%). Generalized linear mixed models identified various modifiable risk factors for caregiver concerns (e.g., caregivers’ perception that residents lacked access to counseling services or not feeling well informed about and involved in resident care). These modifiable factors can be targeted in efforts to prevent or mitigate caregiver concerns and resident mental health issues.
Keywords
COVID-19 has led to higher rates of death and suffering among nursing home and assisted living (AL) residents, compared with the general older adult population (Chu et al., 2021; Dykgraaf et al., 2021; Werner et al., 2020). Visitor restrictions intended to protect resident safety have been associated with deteriorated resident, family or friend caregiver, and care staff mental health (Gaugler & Mitchell, 2022; Hindmarch et al., 2021; Kemp, 2021; Sorrell, 2021; Veiga-Seijo et al., 2022). Residents’ families and friends are more than visitors—they are caregivers (Kemp, 2021). They serve critical roles as advocates and legal decision makers for residents with cognitive impairment and they provide essential care and support, including emotional and social care, engaging residents in activities, providing information to care staff, facilitating access to health care services, and assisting with daily activities (Kemp, 2021).
Being unable to visit residents to provide these essential supports increased caregivers’ concerns about deteriorating resident mental because of residents’ prolonged social isolation, decreasing physical health and functioning, and residents dying without their caregiver’s support (Gaugler & Mitchell, 2022; Hindmarch et al., 2021; Kemp, 2021; Veiga-Seijo et al., 2022). This may be especially true in assisted living, a congregate care setting intended to serve older adults with lower care needs than those in nursing homes that aim to promote resident autonomy and privacy in a home-like environment (American Geriatrics Society, 2020; Coe & Van Houtven, 2020; Zimmerman et al., 2020). Assisted living offers fewer services than nursing homes, has lower staffing and skill mix levels, and no onsite 24-hr registered nursing care (Dys et al., 2021; Gibbons & Kowalewski, 2021; Hogan et al., 2012, 2014; Maxwell et al., 2013, 2015). Consequently, more caregiver involvement in resident care is expected in assisted living than in nursing homes (Baumbusch & Phinney, 2014; Dys et al., 2021; Gibbons & Kowalewski, 2021; Puurveen et al., 2018). At the same time, assisted living and nursing home residents share a high degree of vulnerability (Hogan et al., 2012, 2014; Maxwell et al., 2013, 2015). Assisted living residents are of advanced age (average 84 years) and exhibit high rates of dementia (≥60%), mental health conditions (34% with depression), and multimorbidity (average of five conditions; Hogan et al., 2012, 2014; Maxwell et al., 2013, 2015). However, far less research is available on the impact of COVID-19 in assisted living, compared with nursing homes (American Geriatrics Society, 2020; Coe & Van Houtven, 2020; Zimmerman et al., 2020). This is a critical knowledge gap given that assisted living spaces make up more than 40% of all publicly funded facility-based continuing care spaces (Statistics Canada, 2016; Zimmerman et al., 2020) and that the growth of publicly funded assisted living has outpaced that of nursing homes (Alberta Health Services [AHS], 2020; Grabowski et al., 2012).
Qualitative and descriptive studies (largely in nursing homes or including, but not separately analyzing, assisted living and nursing home settings; Hindmarch et al., 2021; Mitchell et al., 2021; Nash et al., 2021; O’Caoimh et al., 2020; Parmar et al., 2021; Wammes et al., 2020; Yeh et al., 2020) suggest high rates of caregiver concerns about resident mental health during the pandemic. Between 76% (Wammes et al., 2020) and 90% (Mitchell et al., 2021) of caregivers expressed concerns about resident loneliness, 50% (O’Caoimh et al., 2020) to 66% (Wammes et al., 2020) about mood issues, 62% about poor quality of life (Wammes et al., 2020), and 39% about psychological stress (39%; Yeh et al., 2020). Caregiver concerns about resident care can indicate unmet care needs that care staff may be unaware of and that residents may not be willing or able to express (Reader & Gillespie, 2013). Failing to act upon these concerns can lead to resident neglect and harm (Reader & Gillespie, 2013). Furthermore, caregiver concerns about resident care and difficulties staying involved in resident care can negatively affect caregivers’ mental health (Puurveen et al., 2018). In our own research (Lane et al., 2022), we surveyed 673 caregivers of AL residents in the Canadian provinces of Alberta and British Columbia between October 2020 and March 2021 and found significant anxiety in 29% and clinically meaningful depressive symptoms in 39% of the participants. Those whose concerns about the resident being depressed increased or remained consistently high in the 3 months after (vs. before) the start of the pandemic were more likely (risk ratios between 1.6 and 2.1) to experience moderate or severe depressive and anxiety symptoms (Lane et al., 2022). During the Severe Acute Respiratory Syndrome (SARS) outbreaks in Toronto, Canada, in 2003, caregivers of nursing home residents experienced fear, worry, loss of control, frustration, and guilt as a consequence of visiting restrictions (McCleary et al., 2006). We lack research on these issues in AL, including robust quantitative evidence on modifiable factors associated with caregiver concerns during the COVID-19 pandemic.
This study aimed to assess the prevalence of caregiver concerns about AL residents’ depressive symptoms, loneliness, and anxiety in the 3 months before and after the start of the pandemic in Canada and modifiable factors associated with these concerns during the pandemic. Informed by recent qualitative and descriptive findings (Hindmarch et al., 2021; Mitchell et al., 2021; Nash et al., 2021; O’Caoimh et al., 2020; Yeh et al., 2020), our hypothesis was that adjusting for sociodemographic characteristics, the following caregiver reported outcomes would be significantly associated with decreased levels of caregivers’ concerns about residents’ mental health: (a) residents’ access to care services, (b) adequate information communicated by the assisted living home about restrictions and resident care, and (c) caregivers’ involvement in resident care.
Method
This cross-sectional analysis used baseline data from a prospective cohort study (COVID-19 and Caregivers of Assisted living Residents: their Experiences and Support needs; COVCARES-AB/BC). The Survey Research Center (SRC) at the University of Waterloo administered an online survey to caregivers of assisted living residents in Alberta and British Columbia, Canada (October 28, 2020 to March 31, 2021). Participants received a $25 coffee gift card.
Setting and Sample
We invited all eligible assisted living homes in Alberta (n = 163) and British Columbia (n = 137) to participate. Homes were eligible if they (a) were licensed and publicly subsidized, (b) had been in operation for 6+ months, (c) served a minimum number of residents aged 65+ years (four in homes below and 10 in homes above regional median bedsize), and (d) did not primarily serve psychiatric clients. Participating homes shared our recruitment materials and online survey link with their caregivers (e.g., via mailing lists, social media, printed hardcopies). We also shared the survey link via social media, websites, mailing lists, and newsletters. Caregivers were eligible if they (a) were 18+ years old, (b) cared for an assisted living resident aged 65+ years who had lived in the assisted living home for 3+ months prior to March 1, 2020, and (c) were the person most informed about or most involved in the resident’s care. Our sample size of 673 participants was sufficient to detect differences in our binary outcomes (moderate to extreme caregiver concerns) as small as 10% with 82% power at a 5% significance level (two-sided z test).
Measures
Our survey was based on a prior, validated assisted living caregiver survey in Alberta (Strain et al., 2011; Wanless et al., 2011). COVID-19-related items were from national COVID-19 surveys (Raina et al., 2021; Statistics Canada, 2020; Wister et al., 2022) with some modifications for the AL context. The survey assessed caregivers’ sociodemographic characteristics, types and frequency of care activities they were involved in, residents’ access to care services, concerns about residents’ physical and mental health, caregivers’ physical and mental health, caregivers’ social support, perceived information about the residents’ situation communicated by the assisted living home, and opportunities to stay well informed and engaged in the care of the resident. Caregivers rated the outcomes in the 3 months before versus after March 1, 2020, because Alberta and British Columbia initiated visitor restrictions to AL in March 2020 (University of Toronto, 2020).
Concerns About Resident Mental Health
We asked caregivers about their level of concern with the resident’s depressed mood, loneliness, or anxiety in the 3 months pre versus post-March 1, 2020. Caregivers rated each of the three items for each of the two time periods on a 5-point scale ranging from extremely concerned to not at all concerned. Moderate to extreme versus lower levels of concerns post March 1, 2020 were our dependent variables.
Independent Variables and Covariates
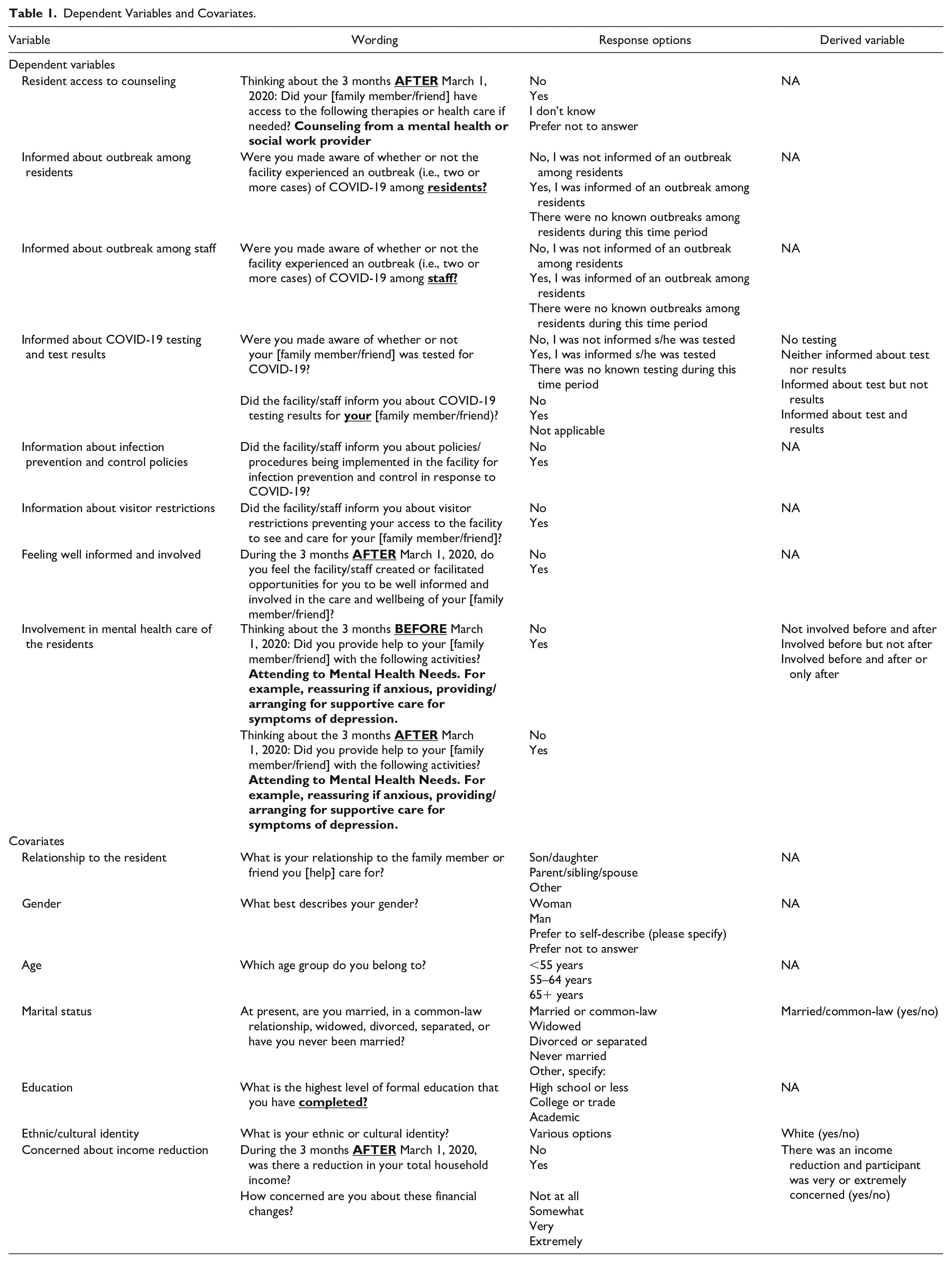
We selected the main independent variables (Table 1) based on previous qualitative and descriptive studies (mostly in long-term care; Hindmarch et al., 2021; Mitchell et al., 2021; Nash et al., 2021; O’Caoimh et al., 2020; Yeh et al., 2020) that suggested possible associations of these variables with assisted living caregiver concerns about resident care. We included demographic variables, caregivers’ relationship with the resident, and pandemic-related changes in income as covariates (Table 1).
Dependent Variables and Covariates.
Statistical Analyses
We used SAS software version 9.4 (Copyright © 2016 by SAS Institute Inc., Cary, NC, USA) for all analyses. We compared the frequency and proportion of caregivers who were moderately to extremely concerned about resident mental health (depressed mood, loneliness, anxiety) in the 3 months pre- versus post-March 1, 2020, using MacNemar’s test. We report the frequency and proportion of study outcomes and covariates overall, and we assessed bivariate differences in study variables between caregivers who were moderately/severely versus less concerned about resident depressed mood, loneliness, or anxiety after March 1, 2020.
To assess the association of covariates with each of the three dichotomous concern variables, we specified generalized linear mixed models with a log link and a binary distribution. Therefore, model estimates are risk ratios (Zou, 2004), which are less biased than odds ratios if outcomes are not rare in all strata (Cummings, 2009). We first ran unadjusted models and then added covariates one at a time, starting with our independent variables, followed by caregiver characteristics. Multicollinearity assessments did not suggest any issues. We excluded 3 covariates from our adjusted models due to a lack of variance (assisted living homes informing caregivers about infection control policies and measures, and assisted living homes informing caregivers about visitor restrictions) or lack of an association (p ≥ .1) with either of the three caregiver concern variables in our bivariate analyses (assisted living homes informing caregivers about COVID-19 outbreaks among residents). We included all other covariates in all three adjusted models for comparability. Missing data rates were generally small (well below 5%) for most variables but relatively higher for caregiver relationship to the resident (13.4%) and household income (13.7%), and responses were not missing completely at random. Therefore, we performed multiple imputations (16 imputed data sets, corresponding to the proportion of records with missing data), using the fully conditional method (van Buuren, 2007) and a generalized logit distribution (Rubin, 1987).
We conducted sensitivity analyses to assess whether adding facility-level variables (province, for-profit vs. not-for-profit ownership, and large vs. small size) to the models, and adding a facility-level random intercept (based on a multilevel model to account for clustering of caregivers within assisted living homes and to assess the level of intracluster correlation) altered our conclusions.
Ethics Approval
Our study received ethics approval from the Research Ethics Boards at the Universities of Alberta (Pro00101048), Calgary (REB20-1544), British Columbia (H20-01732), and Waterloo (ORE#42494). We obtained operational approvals from participating assisted living homes and health regions (five Health Zones in Alberta and five Regional Health Authorities in British Columbia) as needed. The study information was provided to participants at the beginning of the survey and participants agreed to participate in the study by submitting their survey.
Results
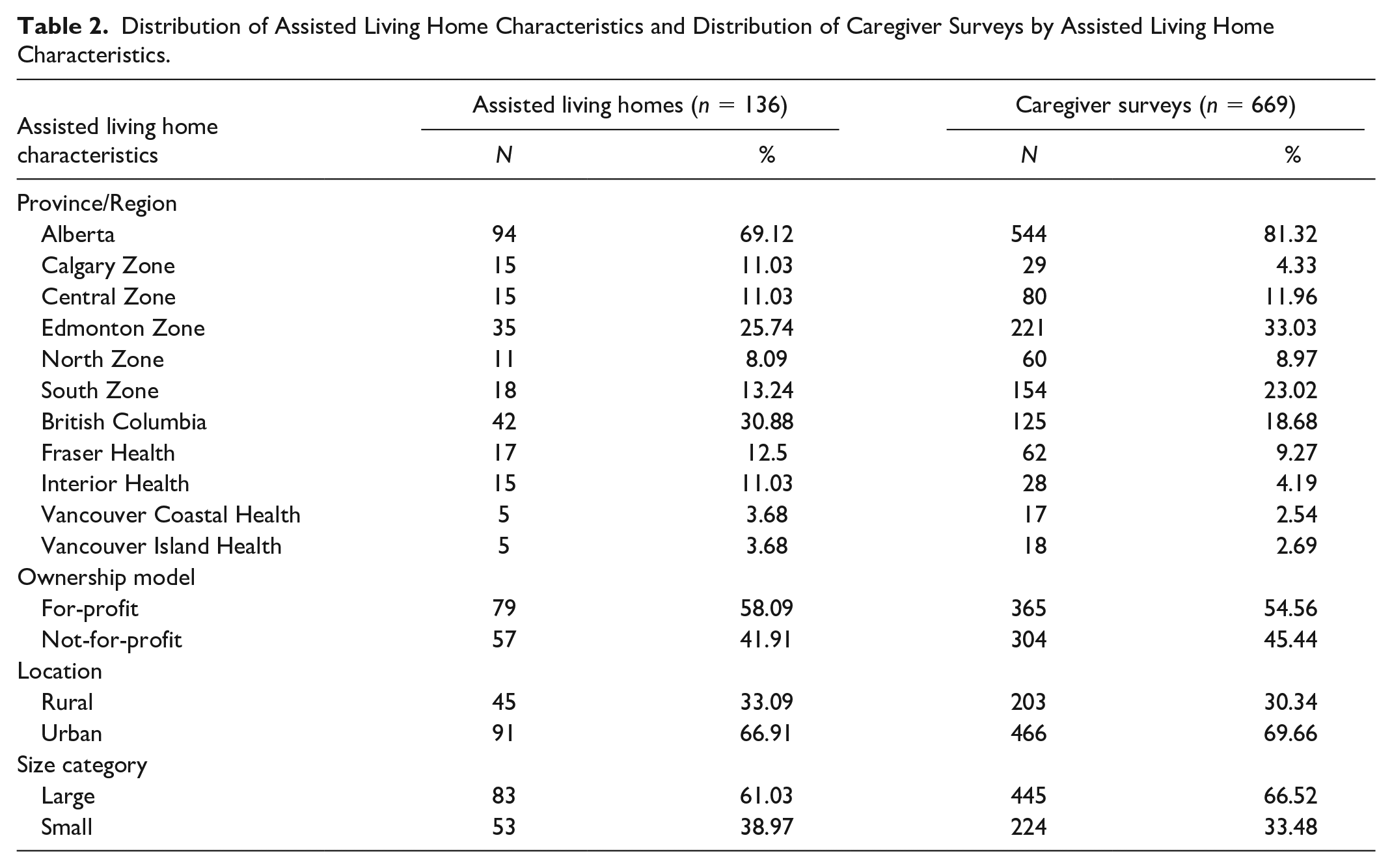
Our sample included 673 caregivers who cared for residents in one of 136 identified AL homes (45% of all eligible homes). Due to our sampling and recruitment approach, we have no information on the number of caregivers who received our online survey link and cannot provide an accurate caregiver response rate. AL homes (Table 2) included small/large, urban/rural, and for-profit/not-for-profit facilities in 5/5 Health Zones in Alberta and 4/5 Regional Health Authorities in British Columbia. Most caregivers (Table 3) were women, 55 years or older, married, White, had higher levels of education, and reported a household income of $50,000 or more.
Distribution of Assisted Living Home Characteristics and Distribution of Caregiver Surveys by Assisted Living Home Characteristics.
Caregiver Characteristics, Caregiver Involvement in the Resident’s Mental Health Care, and Caregiver-Reported Information and Support by Assisted Living Homes—Overall and by Presence/Absence of Caregiver Concerns About the Resident’s Mental Health.
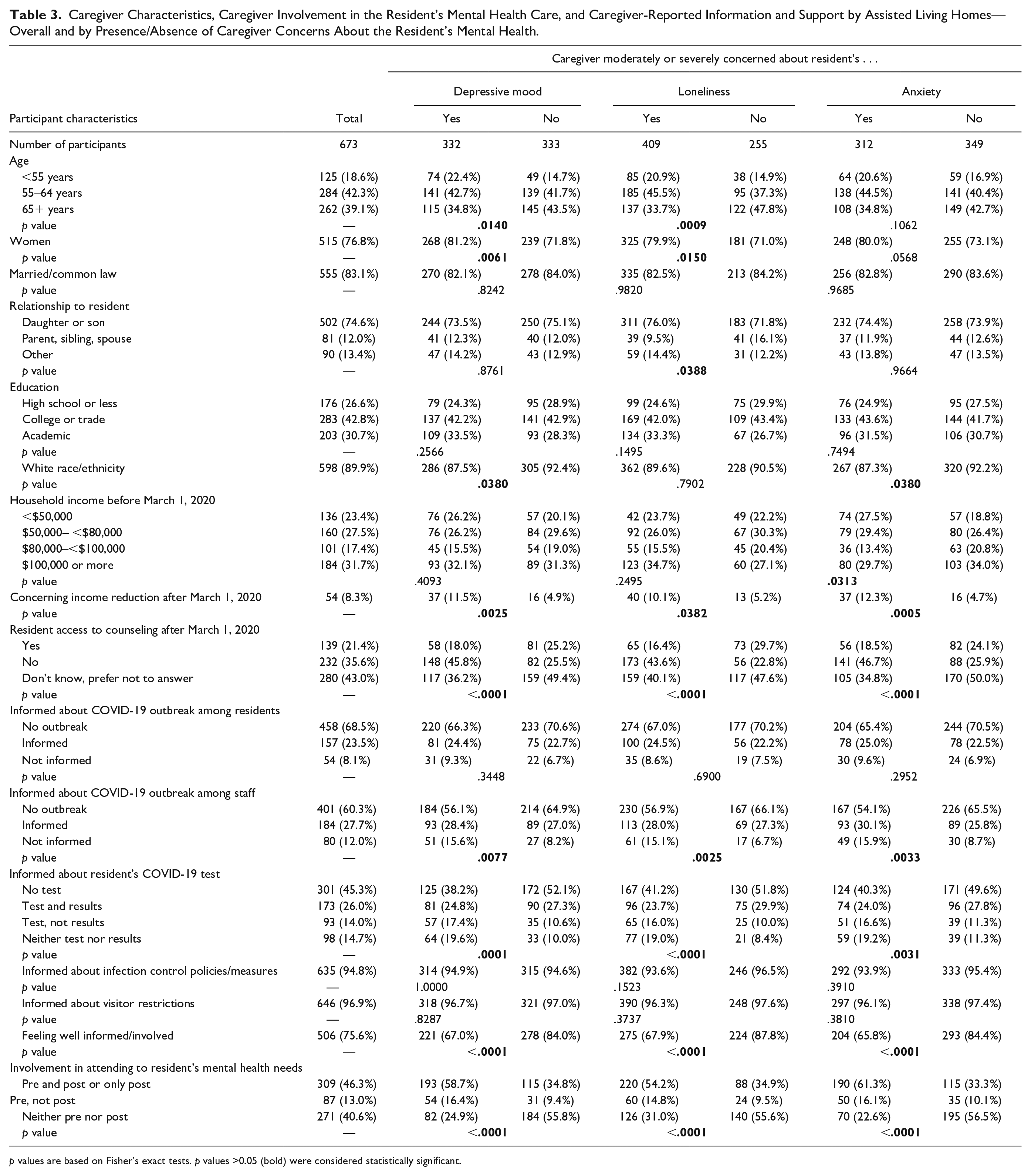
p values are based on Fisher’s exact tests. p values >0.05 (bold) were considered statistically significant.
Almost 36% of the participants indicated that the resident did not have access to counseling during the first wave of the pandemic. Of those who reported outbreaks among residents (n = 211) or staff (n = 264) in their resident’s home, more than 25% and 30%, respectively, were not informed about the outbreak. Of the 364 caregivers whose resident was tested for COVID-19, more than 50% said they were not informed about the test being done, the test result, or both. Although almost all caregivers were informed about infection control policies and visitor restrictions, 25% of the caregivers felt the AL home did not create opportunities for them to be well informed or involved in the resident’s care. Almost half of the caregivers were involved in attending to the resident’s mental health needs before and after the start of the pandemic, whereas 13% were involved before but not after.
Caregiver concerns about all three mental health conditions of interest were high before the start of the pandemic (Figure 1) and substantially increased during Wave 1 of the pandemic. In all three adjusted models (Table 4), caregivers’ reports about residents’ lack of access to counseling and their involvement in resident mental health care (pre- and/or both pre–post March 1, 2020) were strong positive correlates of their concern about resident mental health. After adjustment, women were more likely to be concerned about the resident’s depressed mood, and non-White caregivers were more concerned about the resident’s depressed mood and anxiety. Not being informed about COVID-19 outbreaks among care staff, relationship to the resident, caregiver age, and concerns about changes in income were statistically nonsignificant in the adjusted models. Learning that the resident received a COVID-19 test increased caregiver likelihood of being concerned about the resident’s depressed mood (but not loneliness and anxiety) regardless of the extent of information provided by the AL home.
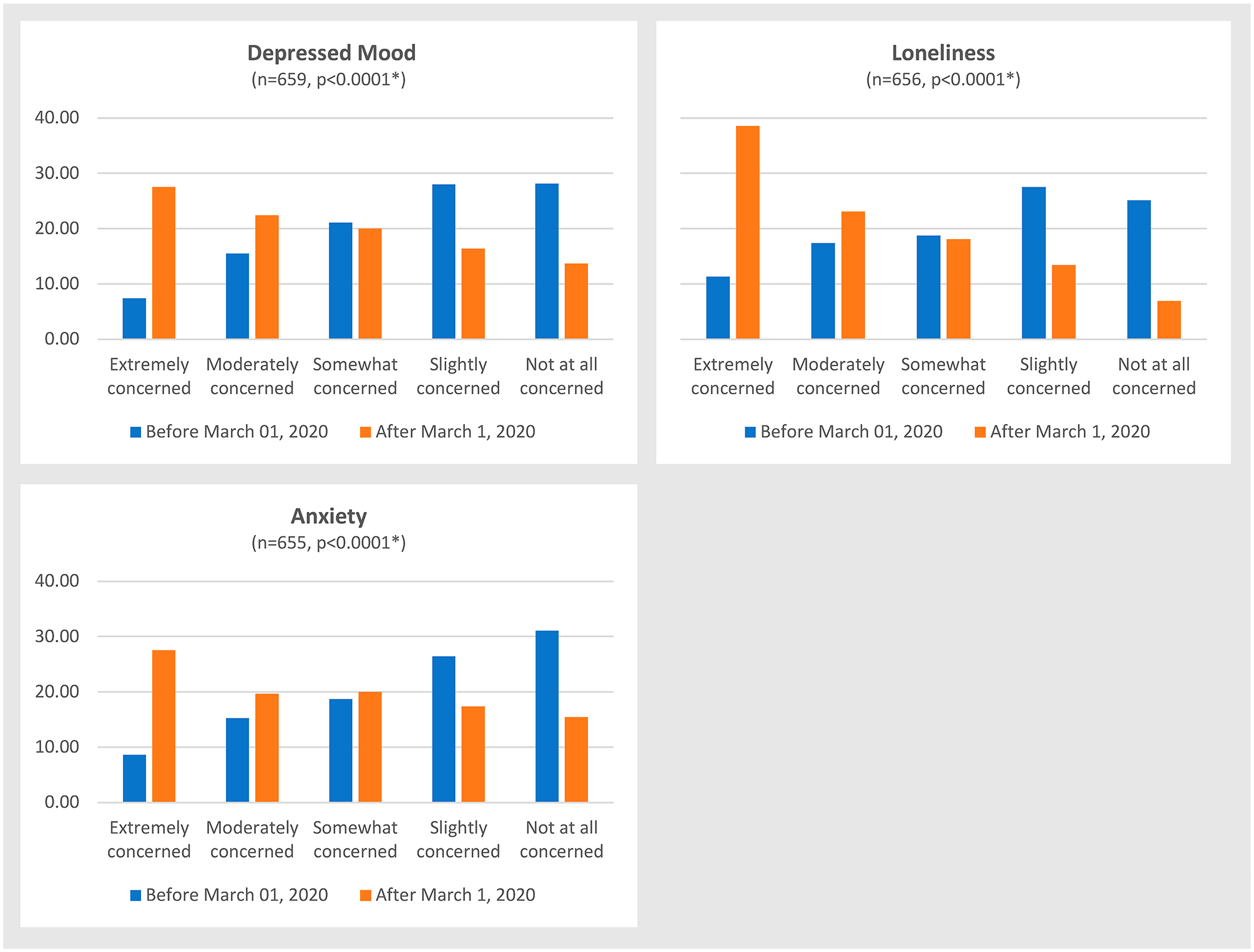
Distribution of caregiver concerns about the resident’s depressed mood, loneliness and anxiety in the 3 months before and after March 1, 2020.
Unadjusted and Adjusted Associations (Risk Ratios [95% Confidence Intervals]) of Caregiver-Reported Communication and Support by Assisted Living Homes, Caregiver Involvement in the Resident’s Mental Health Care, and Caregiver Characteristics With Caregiver Concerns About Resident Mental Health.
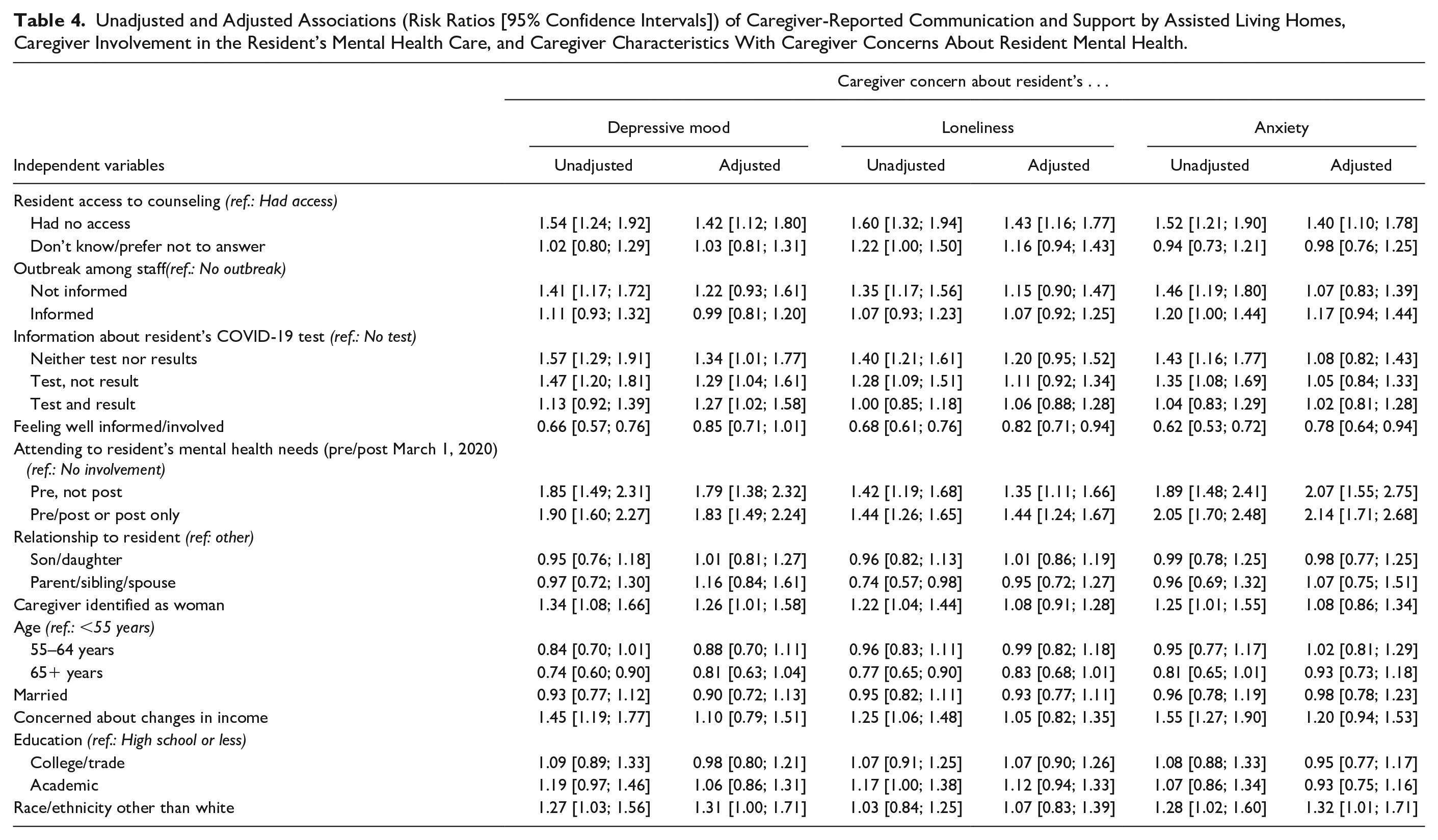
No facility variables were associated with caregiver concerns. Their addition to the models decreased model fit and did not change our conclusions. The same is true for adding a facility-level random intercept. The intracluster correlations were small and statistically nonsignificant (depressed mood: 0.000, p = 1.000; loneliness: 0.010, p = .390, anxiety: 0.003, p = .454).
Discussion
This study examined caregiver concerns about assisted living residents’ depressed mood, loneliness and anxiety, and associated factors in the 3 months after the start of the COVID-19 pandemic (March 1, 2020) in Canada. We found high levels of caregiver concerns about residents’ depressed mood (23%), loneliness (29%), and anxiety (24%) in the 3 months before the start of the pandemic, and these doubled to 50%, 62%, and 47%, respectively, in the 3 months after. Modifiable factors, including residents’ access to counseling services and keeping caregivers informed about and involved in resident care, reduced caregivers’ risk for concerns. Caregivers who attended to the resident’s mental health needs before and/or after the start of the pandemic were more likely to express concerns than those not involved in such activities. Caregivers who learned that the resident was tested for COVID-19 and those who identified as women were more likely to be concerned about residents’ depressed mood. Non-White caregivers reported more concerns about residents’ depressed mood and anxiety than white caregivers.
Two other studies focusing on assisted living assessed caregiver concerns about resident care during the COVID-19 pandemic. Semi-structured interviews with 32 caregivers of older adults (including five caregivers of assisted living residents) in Alberta, Canada, suggested that caregivers were generally more concerned about the resident’s situation than about their own (Parmar et al., 2021). They raised concerns about residents’ emotional, social, and physical care needs, but the study focused on the support needs of caregivers and did not discuss caregiver concerns about the resident in more detail. A U.S. study (Nash et al., 2021) surveyed 512 caregivers of nursing home and assisted living residents but did not report results by care setting. Almost half of the participants expressed concerns about the residents’ isolation, 40% about rapid decline (open text responses mostly referring to emotional decline), and 30% about inhumane care (Nash et al., 2021). Rates of caregiver concerns reported in nursing homes are similar. In a U.S. study (Jun 2020 to Aug 2021; Mitchell et al., 2021), 30% of the 125 caregivers were concerned about the resident’s social isolation and 26% about deteriorating mental, physical, or cognitive health. In a Taiwanese study (April 2020; Yeh et al., 2020), 38% of the 156 caregivers were concerned about the resident’s psychological stress. Caregivers in a Dutch study (n = 1,997, April to May 2020; Wammes et al., 2020) reported concerns about residents’ increased loneliness (76%), sadness (66%), and decreased quality of life (62%). These high rates of caregiver concerns about resident mental health in both, AL and nursing home settings, point to the need to develop public health measures that (a) better balance residents’ mental health needs with safety concerns and (b) ensure continued inclusion of caregivers in resident care (Dys et al., 2021; Hindmarch et al., 2021; Mitchell et al., 2021; Nash et al., 2021; Parmar et al., 2021; Prins et al., 2021; Wammes et al., 2020).
A Dutch study surveyed 958 caregivers of nursing home residents between April and May 2020 and measured the level of caregiver worries using a 9-item scale ranging from 0 (never worried) to 5 (almost always worried; Prins et al., 2021). Similar to our study, the authors found that caregivers with greater involvement before the pandemic were more worried during the pandemic. The authors also found that at least minimal weekly contact during the pandemic decreased caregivers’ worries. However, unlike our study, this study focused on worries in general and did not assess specific areas of caregiver concerns.
In line with other studies—prior to (Harper et al., 2021), as well as during the COVID-19 pandemic (Hindmarch et al., 2021; Mitchell et al., 2021; O’Caoimh et al., 2020; Wammes et al., 2020)—we found that caregivers often judged communication by the AL home as sub-optimal. However, our study is the first to assess the association of specific communication topics related to COVID-19 in AL with caregiver concerns about resident mental health. Being informed about outbreaks among residents or care staff was not associated with caregiver concerns about resident mental health. However, caregivers were 30% more likely to be concerned about the resident’s depressed mood if their resident was tested for COVID-19. This focus on the specific resident experience is supported by the finding that feeling well-informed about and involved in the care of the resident decreased the likelihood of caregiver concerns about residents’ loneliness and anxiety by about 20%. We also found that caregivers’ perception that residents did not have access to counseling services increased the risk of concerns about resident mental health by 40%. Access to mental health services for AL and nursing home residents was poor even before the pandemic and deteriorated further due to the lockdown measures (Flint et al., 2020; Perlman et al., 2019). This is concerning, given the higher prevalence of dementia, depression, and anxiety among older adults living in congregate, compared with community settings (Seitz et al., 2010). In addition to infection prevention, future public health measures must ensure AL and nursing home residents’ continued access to mental health services.
Strengths and Limitations
Research on the impact of COVID-19 on caregivers of AL residents is emerging but limited by the lack of robust, quantitative studies applying advanced statistical modeling approaches. Previous studies often excluded caregivers of assisted living residents (Hindmarch et al., 2021; Mitchell et al., 2021; O’Caoimh et al., 2020; Prins et al., 2021; Wammes et al., 2020; Yeh et al., 2020), only included small samples of assisted living caregivers (Anderson et al., 2021; Parmar et al., 2021), and/or did not report subgroup analyses (Nash et al., 2021). Our study is one of the few to address this important research gap. Other strengths of our study include the use of a validated survey with a large sample of caregivers of assisted living residents in 2 Canadian provinces. The cross-sectional design of our study is a limitation, not allowing temporal precedence of outcomes, which prevents causal conclusions. The generalizability of our results is limited as most participants were White, spoke English as the primary language, and had relatively high household incomes. The nature and amount of caregiver concerns may differ in equity-seeking groups. Our study found that non-White caregivers were more likely to express concerns about residents’ depressed mood and anxiety. However, as our study did not include resident data, we cannot assess whether these differences were due to inequities among residents, cultural differences in caregiver perceptions, or both. Generally, the lack of resident data limits our ability to further contextualize the caregiver perceptions. For example, from our previous studies in AL in Alberta (Strain et al., 2011; Wanless et al., 2011), we know that 71% of the residents were widowed, 8% were divorced and 6% were never married. In that study, 78% of the homes had private rooms only, 31% had spousal suites (range from one to 10 suites per home), and only few of these were used by spouses. This suggests that most assisted living residents live alone and that support from caregivers may be critical as residents’ social contacts within the home are limited. However, due to the pandemic conditions and restrictions, we were not able (and permitted as per our ethics approvals) to obtain resident data that would have helped to investigate these issues.
Conclusion
Caregivers of assisted living residents are at high risk of experiencing moderate to extreme concerns about residents’ depressed mood, loneliness, and anxiety. Caregiver concerns are important indicators of unmet resident care needs, and they put caregivers at risk of poor mental health. The pandemic substantially increased caregivers’ concerns about resident’s mental health. We found that modifiable factors that can be influenced by nurses, including continued resident access to counseling, and keeping caregivers informed about and involved in resident care reduced the risk of caregiver concerns. Facility-level factors (outbreaks among care staff and residents in general, and information about infection control measures and visitor restrictions) were less relevant for caregivers’ concerns than the individual resident’s situation. Public health policies, AL settings, and nurses working in these settings need to ensure continued resident access to mental health services, and caregivers’ continued access to information and involvement in resident care. AL settings and nurses working in these settings need to be aware of the relevance, types and amount, and factors associated with caregiver concerns about residents. This can help prevent or mitigate unmet resident care needs and caregiver mental health issues.
Footnotes
Acknowledgements
We thank the participating caregivers and assisted living homes for taking the time to participate in this research and for providing their valuable insights. We also thank our collaborators, including Caregivers Alberta, Family Caregivers of British Columbia, Alberta Health, Alberta Health Services, Government of British Columbia, and Vancouver Coastal Health for their support of and contributions to our research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an Alberta Innovates National Partnered R&I Initiatives Grant (#202100518), an Establishment Grant and a Professorship in Continuing Care Policy Research, both awarded by the Faculty of Nursing, University of Alberta.