
Abstract
Down syndrome (DS) is the most common genetic cause of intellectual disability worldwide. The purpose of this analysis was to determine the internal consistency reliability of eight language versions of the Family Management Measure (FaMM) and compare family management of DS across cultures. A total of 2,740 parents of individuals with DS from 11 countries completed the FaMM. The analysis provided evidence of internal consistency reliability exceeding .70 for four of six FaMM scales for the entire sample. Across countries, there was a pattern of positive family management. Cross-cultural comparisons revealed parents from Brazil, Spain, and the United States had the most positive family management and respondents from Ireland, Italy, Japan, and Korea had the least positive. The rankings were mixed for the four remaining countries. These findings provide evidence of overall strong internal consistency reliability of the FaMM. More cross-cultural research is needed to understand how social determinants of health influence family management in families of individuals with DS.
Down syndrome (DS) is a chromosomal abnormality associated with chronic health concerns and intellectual disability. Worldwide, the incidence of DS is one in every 1,000 to 1,100 live births, making it the most common genetic cause of intellectual disability. Individuals with DS have an increased risk of mortality and morbidity due to co-occurring conditions such as congenital heart disease, blood disorders, hypothyroidism, celiac disease, behavioral and emotional problems, and sleep disorders (Bull & Committee on Genetics, 2011; Kapoor et al., 2014; Kazemi et al., 2016). While the number and severity of co-occurring conditions can vary greatly from one individual with DS to the next, most individuals with DS have health-related concerns which can pose added care responsibilities for their families.
Background
Regardless of sociocultural context, families of individuals with DS face unique challenges due to the ongoing health and developmental concerns associated with DS. Researchers worldwide have examined adaptation in families of individuals with DS and factors contributing to more optimal adaptation. However, most of these studies were conducted with families of individuals with DS who live in Western countries (H. Choi & Van Riper, 2017) and samples for these studies have typically included families of individuals with DS from a single country. Moreover, in most of these studies, adaptation was assessed at the individual level (i.e., parental and sibling adaptation), with relatively little attention paid to family members’ perceptions of their efforts to address the family challenges they were facing.
For this article, we reviewed reports from over 90 studies conducted during the past 10 years on adaptation in families of individuals with DS. Of these studies, only 31 included an assessment of adaptation at the family level. Usually based on parental report, the family variables most commonly assessed in these studies were family functioning, family well-being, family adaptability and cohesion, family quality of life, family stress and coping, and family management. The 31 studies were conducted in 11 different countries (for some of the studies there were more than one publication): five studies in Australia (Carling-Jenkins et al., 2012; Foley et al., 2014; Leonard et al., 2016; Muggli et al., 2009; Povee et al., 2012), two studies in Canada (Auyeung et al., 2011; King et al., 2009, 2011), one study in Ecuador (Huiracocha et al., 2017), two studies in Korea (E. K. Choi & Yoo, 2015; H. Choi, 2015), one study in Italy (Lanfranchi & Vianello, 2012), two studies in the Netherlands (Marchal et al., 2016; van der Veek et al., 2009), one study in Nigeria (Ajuwon, 2012), one study in Poland (Dabrowska & Pisula, 2010), two studies in Taiwan (Gau et al., 2008; Hsiao, 2014; Hsiao & Van Riper, 2011) two studies in the United Kingdom (Carr, 2008; Griffith et al., 2010), and 12 studies in the United States (Blacher & McIntyre, 2006; Burke & Hodapp, 2014; Corrice & Glidden, 2009; McGrath et al., 2011; Mitchell et al., 2015; Neely-Barnes et al., 2010; Nelson Goff et al., 2016; Phelps et al., 2012; Rieger & McGrail, 2013; Skotko et al., 2016; Stoneman, 2007; Van Riper, 2007).
Findings from the reviewed studies concerning adaptation in families of individuals with DS indicate that although parents usually described the period surrounding their family member’s diagnosis as stressful and emotionally charged, most reported that over time they and their families came to recognize that, despite the challenges, there were many positive aspects to having an individual with DS in the family (Bentley et al., 2015; King et al., 2009; Marshak et al., 2018; Pillay et al., 2012; Povee et al., 2012; Skotko et al., 2011). For example, Pillay and colleagues (2012) reported that the Australian mothers in their study described having a child with DS as an unexpected, but beautiful journey, and Bentley and colleagues (2015) identified different patterns of strength and meaning-making that contributed to adaptation in fathers of children with DS living in the United States. In another study involving fathers, most fathers reported a positive trajectory in terms of their adjustment and many attributed this to realizing that their previously held negative assumptions about people with DS were not accurate (Marshak et al., 2018). Of the 2,044 parents surveyed by Skotko and colleagues (2011), 79% indicated that they felt their outlook on life was more positive because of their son or daughter with DS.
Studies of family system responses to having an individual with DS in the family also have reported positive outcomes. Povee and colleagues (2012) found that the marital adjustment and family functioning of Australian families in which there was a child with DS were comparable to that of families of typically developing children. Pillay and colleagues (2012) reported that mothers believed family relationships had been strengthened because of having a child with DS. In a study conducted with Korean parents of children with DS (E. K. Choi & Yoo, 2015), family functioning was good or average in over 90% of the families. Brown and colleagues (2006) reported high overall satisfaction with family life among Canadian families.
Despite studies reporting that many family members and family systems adapt well to the challenges associated with raising an individual with DS, there also is evidence of considerable variability across families, with some family members and family systems struggling to accommodate to challenges related to the family member’s condition (Canbulat et al., 2014; Durmaz et al., 2011; Huiracocha et al., 2017; Marchal et al., 2016; McGrath et al., 2011; Yildirim & Yildirim, 2010). Given the variability in family response, researchers also have sought to identify factors supporting versus inhibiting optimal family adaptation. Factors that have been investigated include parent and family system variables (e.g., parental health, parental depression, family demands, and family resources), as well as sociocultural variables (e.g., family income, educational level of parents, family–provider relationship, cultural context, and religion) (Ajuwon, 2012; E. K. Choi & Yoo, 2015; Geok et al., 2013; Hsiao, 2014; Hsiao & Van Riper, 2011; Lanfranchi & Vianello, 2012; Van Riper, 1999).
For example, in a sample of 126 Korean parents (E. K. Choi & Yoo, 2015), parental depression, family cohesiveness, and family problem-solving communication were strongly related to family resilience and adaptation. Findings from a study conducted in the United States concerning maternal perceptions of family–provider relationships and well-being in families of children with DS (Van Riper, 1999) revealed that higher levels of parental well-being and family functioning were reported by mothers who had a positive relationship with their child’s primary provider, received family centered care, and were satisfied with the care their child had received. In a study of quality of life among Malaysian mothers of children with DS, Geok and colleagues (2013) found that variation in a mother’s background characteristics in terms of rural–urban locality, household income, marital status, and maternal age were significantly correlated with their quality of life and the lowest quality of life domain score was for the environmental support domain. Ajuwon (2012) studied quality of life in 31 Nigerian families of children with DS and found that of the nine domains of quality of life, parents were least satisfied with the support from services domain; most of the families indicated that access to basic health care services was problematic and for roughly 50% of the families, medical care and prescription drugs were unaffordable. In a study focusing on family adaptation to DS among Taiwanese families (Hsiao, 2014; Hsiao & Van Riper, 2011), families with fewer family demands, greater social support, higher family income, and greater parental education had better family functioning. In a study of parents of children with DS from the United States, three family variables (family demands, family resources, and family problem-solving) were significantly associated with family adaptation (Van Riper, 2007).
The importance of understanding the nature and predictors of adaptation in families of individuals with DS is underscored by the fact that family functioning has been significantly linked to child and parent well-being (Hsiao & Van Riper, 2011; Mitchell et al., 2015; Povee et al., 2012). Although studies such as these provide insights into factors that contribute to better family functioning and adaptation, the diversity of study objectives, conceptual underpinnings, samples, and measures limit our ability to make cross-cultural comparisons and examine more fully how sociocultural differences influence how families respond to the challenges associated with raising an individual with DS. Knowledge of such differences is needed to develop culturally appropriate interventions aimed at supporting family adaptation.
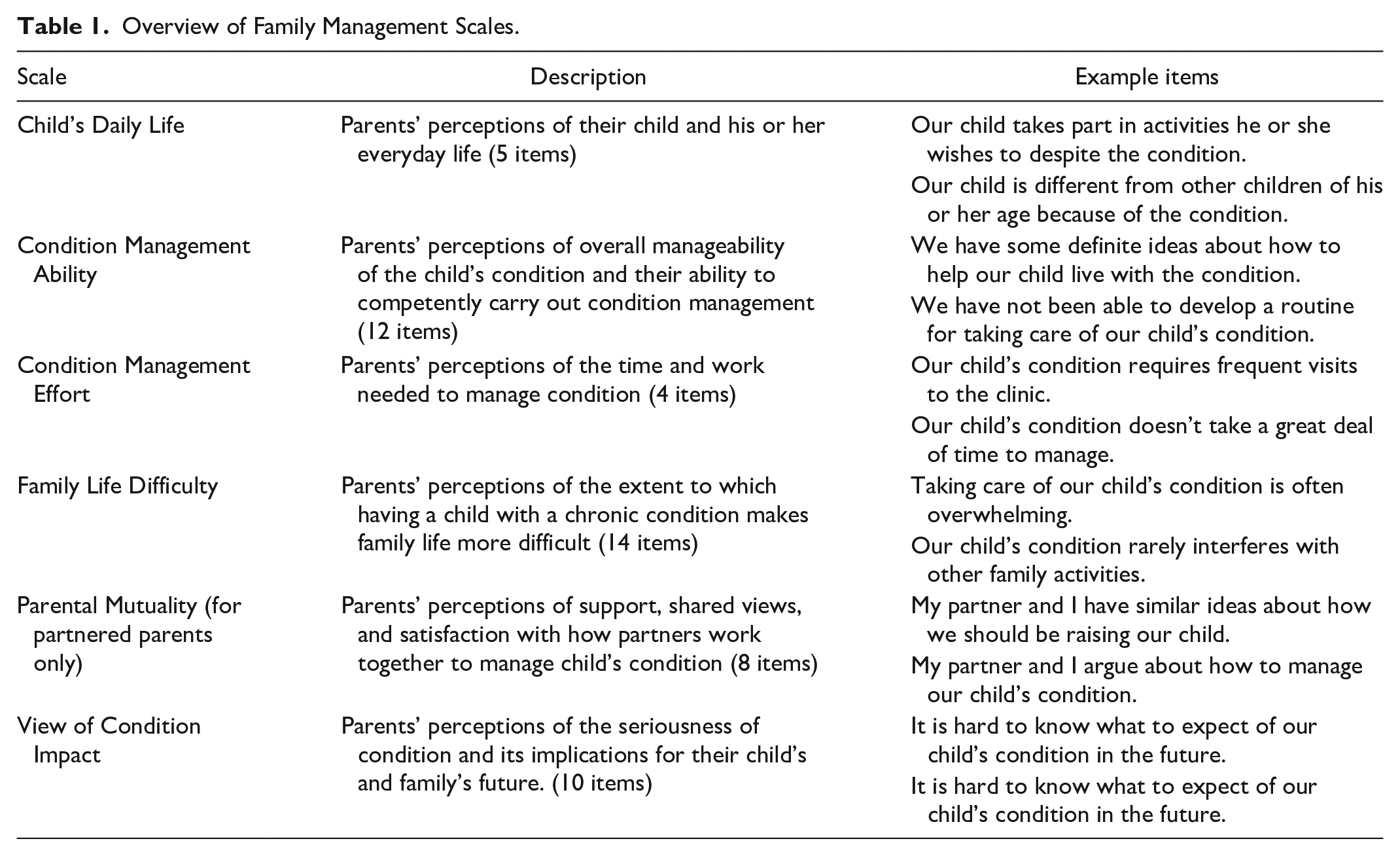
A key aspect of the family’s response to having a family member with DS is how family members incorporate the individual’s unique needs into everyday family life, hereafter referred to as family management. Prior studies assessed parents’ perceptions of family management using the Family Management Measure (FaMM) (see “Method” section and Table 1) and reported a significant relationship between family management and child and family outcomes across a broad array of chronic conditions, but excluding those associated with intellectual disability (Deatrick et al., 2018; Knafl et al., 2011, 2013; Mendes et al., 2016). Recently, our team evaluated the appropriateness of the FaMM for use with families of individuals with DS (Van Riper et al., 2018). Based on the analysis of FaMM data from parents in the United States (539 parents who had a son or daughter with DS and 571 parents who had a son or daughter with a chronic physical condition), we established the reliability of the measure for use with DS samples and its ability to differentiate family management strengths and areas of difficulty in families with a child with DS versus a chronic physical condition. In this article, we report the results of our efforts to assess the appropriateness of the FaMM for use cross culturally in studies of families in which there is an individual with DS.
Overview of Family Management Scales.
Purpose
The purpose of this analysis was to: (a) determine the reliability of the Dutch, Italian, Japanese, Korean, Portuguese, Spanish, and Thai translations of the six FaMM scales; (b) determine the reliability of the English version of the FaMM scales when used with samples from Ireland, the United States, and the United Kingdom and the reliability of the Portuguese version of the FaMM scales when used with samples from Brazil and Portugal; and (c) compare family management across diverse cultural contexts. By measuring modifiable aspects of family management (e.g., parents’ perceptions of their management ability), the FaMM scores provide potentially useful information for developing and testing interventions to improve adaptation in families of children with DS. Our intent in this analysis was to provide further evidence of the extent of the applicability of the FaMM.
Method
Design
This analysis was part of a larger cross-sectional, cross-cultural study examining family factors associated with adaptation in families of individuals with DS lead by the first author (Caples et al., 2018; Van Riper et al., 2018). Data for this analysis come from parents’ responses to the Dutch, English, Italian, Japanese, Korean, Portuguese, Spanish, or Thai versions of the FaMM. The English version of the FaMM was completed by parents from Ireland, the United Kingdom, and the United States; the Portuguese version was completed by parents from Brazil and Portugal; and the Spanish version was completed by parents in Spain and multiple Central and South American countries.
Instruments
The survey for the larger study included a demographic/family information questionnaire, a measure of parental well-being and multiple family measures, including the FaMM (Knafl et al., 2011). The focus of this analysis was results from the demographic/family information questionnaire and the FaMM.
The FaMM
The FaMM (Knafl et al., 2011) is a 53-item parent report instrument based on the Family Management Framework (Knafl & Deatrick, 2003; Knafl et al., 2012). As described in Table 1, it comprises six scales addressing parents’ perceptions of how families incorporate a family member’s chronic condition into everyday family life. Five scales (Condition Management Ability, Child’s Daily Life, Condition Management Effort, Family Life Difficulty, and View of Condition Impact) are completed by all respondents; the Parental Mutuality scale is completed only by respondents who are partnered. The instructions to parents state “Many of these questions use the word ‘family’. This refers to those people living in your household that you think of as family.”
Scales are scored separately and there is no overall summary scale. Investigators using the FaMM can choose to use all or a subset of the six scales. Missing items can be imputed using the average of the items for a scale as long as no more than 30% of a scale’s items are missing, in which case the scale value is missing.
The FaMM instrument development study provided strong evidence of the reliability and validity of the FaMM for families in the United States with a child having a chronic physical condition (Knafl et al., 2011), and a more recent analysis provided evidence of the applicability of the FaMM for studying families of individuals with DS (Van Riper et al., 2018). Translation and cultural adaptation of the FaMM into the seven language versions used in this analysis was done using a multistep process based on existing literature concerning translation and cultural adaptation of research measures (e.g., Beaton et al., 2000; Gjersing et al., 2010). The nine steps were (a) translation of the original instrument by two individuals who are fluent in the target language and have a good understanding of the original language (English), (b) synthesis of translated versions, (c) back-translation by two individuals who are fluent in the original language and have a good understanding of the target language, (d) synthesis of back-translations, (e) revisions by the principal investigator (PI) of the main study, (f) review by expert committee and/or researcher who was the PI for the development of the FaMM, (g) pilot testing of the translated versions of the FaMM, (h) revisions by PI of the main study if needed, and (i) use of translated versions in main study.
Demographic information
The demographic/family information questionnaire, developed by the authors, included questions about the parent completing the questionnaire, their son or daughter with DS, and the family unit. For example, parents were asked to indicate their age, marital status, occupation, educational background, and religion. They were also asked the age of their son or daughter with DS and the number of children in the family.
Participants and Settings
For inclusion in the larger study, the families had to include an individual with DS and one or both parents who were (a) at least 17 years of age, (b) able to read and understand one of eight languages (Dutch, English, Italian, Japanese, Korean, Portuguese, Spanish, and Thai), and (c) willing to complete the self-report questionnaires. The 11 main countries where data were collected were Brazil, Ireland, Italy, Japan, Korea, the Netherlands, Portugal, Spain, Thailand, the United Kingdom, and the United States.
Data collection started in the United States and when the first author who was the primary investigator of the study became a Fulbright Scholar in Ireland, data collection was expanded to include parents from Ireland and the United Kingdom. When the PI started sharing findings from the study at international conferences, such as the International Family Nursing Conference, other family nurse researchers began expressing interest in having the PI expand data collection to include parents from their home countries. This resulted in the formation of an international team of family researchers interested in adaptation and resilience in families of individuals with DS, many of whom participated in the research reported in this article.
Procedures and Data Collection
Prior to the onset of data collection, the study was approved by the Institutional Review Board at the home university of the PI for the larger study. Then, approval was obtained from ethics committees in each of the target countries. Families were recruited through national DS organizations and local DS support groups, as well as by word of mouth. Leaders from the DS organizations and support groups were given information about the study to share with eligible families. In addition, they were given an Invitation to Participate to post on their websites and send out via their listservs. The Invitation to Participate included the PI’s contact information. Parents were given the option of completing an online version of the survey or a hard copy version. If they completed the survey online, the consent form was part of the online survey. Parents were encouraged to contact the PI if they had questions or concerns. Data collection started in the United States in 2012 and other countries in 2013. Data collection ended in 2018. For most countries, the data collection period was approximately 12 to 18 months. Over 90% of the parents completed the survey online.
Statistical Analysis
For each of the six FAMM scales, we computed internal consistency reliability (ICR) scores using Cronbach’s alpha for the whole sample as well as for each language version subsample and tested for differences in scale means across the 11 main countries using one-way analysis of variance F tests. The larger study recruited both parents from families with partnered parents. For this analysis, we used data from all mothers in the larger study as well as data from fathers if they did not have a partner participating in the larger study, thereby making it reasonable to assume independence when computing Cronbach’s alpha and the F test. We also computed descriptive statistics for the whole sample and for children’s age by country. We computed as well F tests for a country effect controlling for covariates, one-at-a-time and altogether, including age of the individual with DS, parent’s age, number of children in the family, mother versus father, and partnered versus not to assess whether covariates affected conclusions about a significant country effect.
Results
Sample
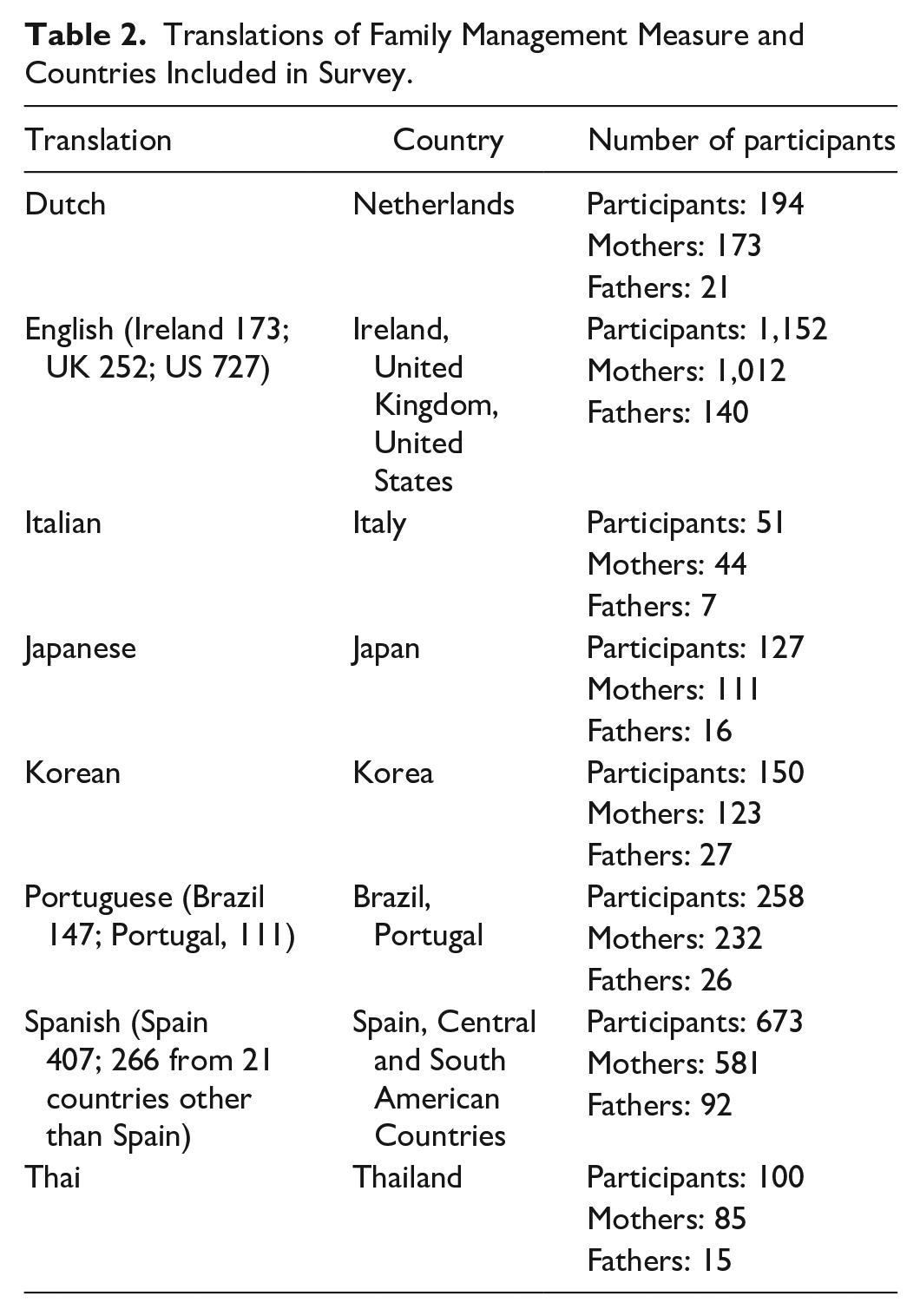
Table 2 provides an overview of sample participants and countries represented in responses to the language versions of the FaMM. Across countries, 2,705 respondents (2,361 mothers, 344 fathers) completed the FaMM, with between 51 and 1,152 parents responding to the various language versions. The largest number of parents (42.6%) completed the English version (respondents from Ireland, the United Kingdom, and the United States) and the fewest number of parents (1.9%) completed the Italian version. Although mothers comprised a substantial majority of respondents (87%), there were father respondents to all FaMM translations, ranging from 10% of those responding to the Portuguese version to 18% of those responding to the Korean version.
Translations of Family Management Measure and Countries Included in Survey.
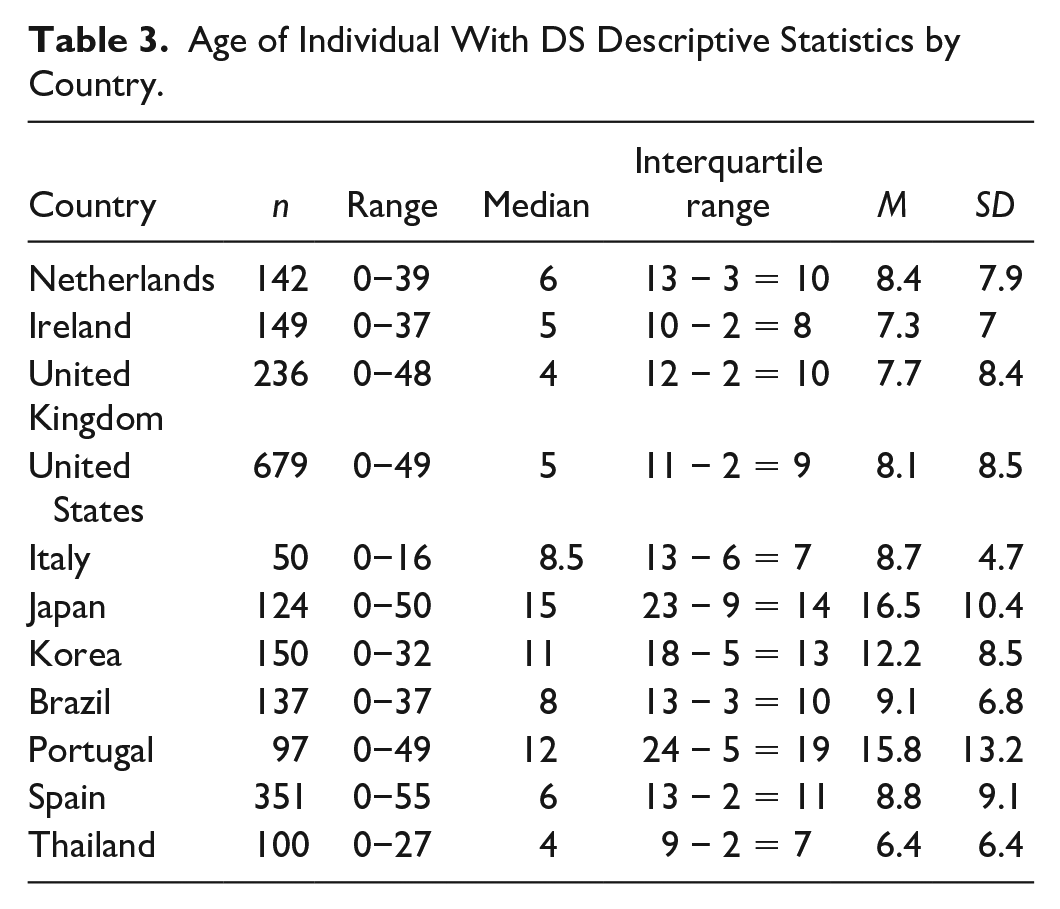
Seventy-four percent of both mothers and fathers were partnered. Mothers’ age ranged from 17 to 85 (n = 1,987) with mean (SD) 42.9 (9.0) years while fathers’ age ranged from 22 to 81 (n = 276) with mean (SD) 44.9 (10.1) years. The number of children in the family ranged from 1 to 23 (n = 2,211) with median (interquartile range) of 2 (3 − 1 = 2). Age of the individual with DS ranged from 0 to 55 (n = 2,450) with median (interquartile range) of 6 (13 − 2 = 11) years. Table 3 contains descriptive statistics for age of the individual with DS broken down by country.
Age of Individual With DS Descriptive Statistics by Country.
ICR
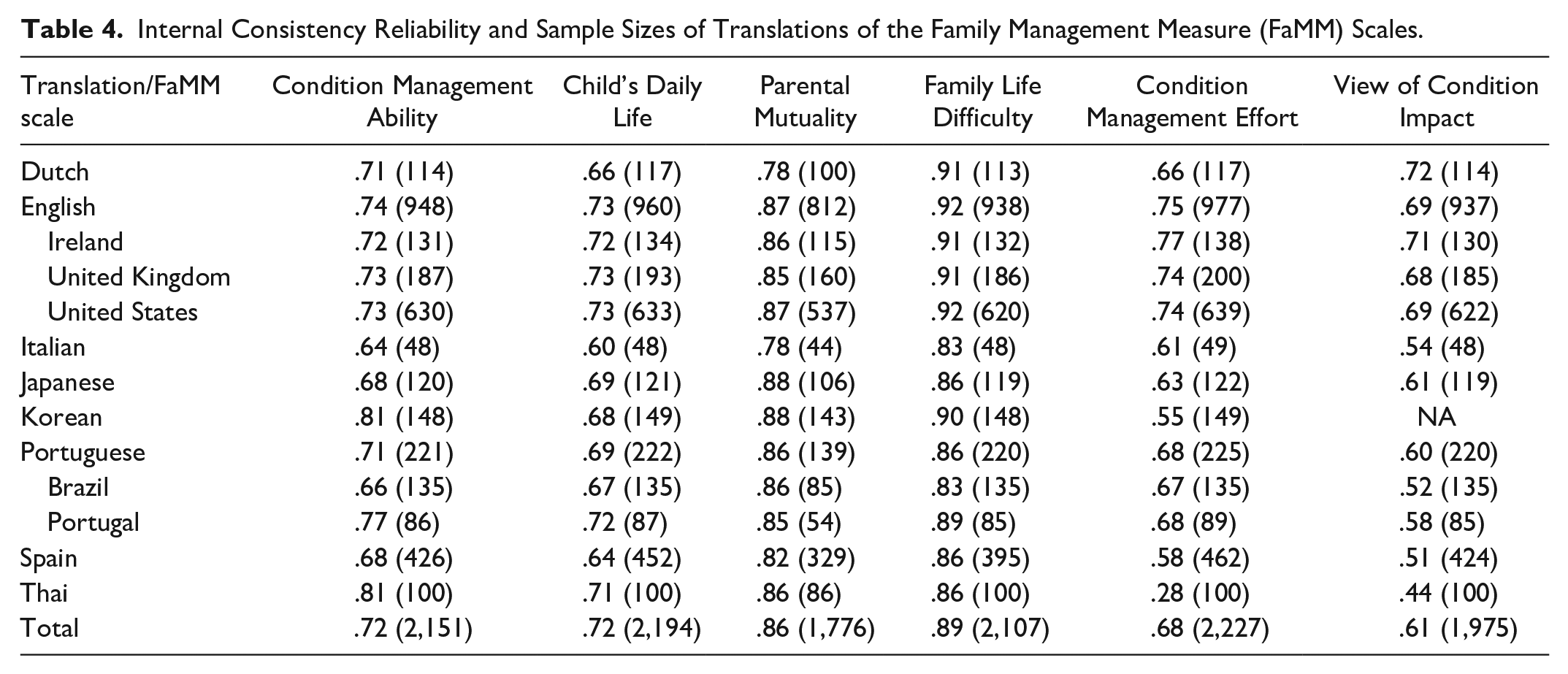
There was evidence of overall strong ICR for the entire sample, with ICR scores ranging from .90 for the Family Life Difficulty scale to .61 for the View of Condition Impact scale. ICR exceeded .70 for four of the FaMM scales (Condition Management Ability, Child’s Daily Life, Family Life Difficulty, and Parental Mutuality) and were .61 and .68 for the remaining two scales (Condition Management Effort and View of Condition Impact).
Across language versions, there was variability in ICR scores of the FaMM scales (Table 4; sample sizes vary across FaMM scales due to missing values). The Family Life Difficulty and Parental Mutuality scales demonstrated excellent ICR across language versions, exceeding the usual .70 cut-off for acceptable reliability, with ICR scores ranging from .83 to .92 for the Family Life Difficulty scale and .78 to .88 for the Parental Mutuality scale. ICR scores for the Condition Management Ability and Child’s Daily Life scales were above .60 across language versions, and for the Dutch, English, Japanese, and Portuguese versions, all FaMM scales had an ICR of .60 or better. On the contrary, ICR scores were below .60 for the Korean, Spanish, and Thai versions of the Condition Management Effort scale and the Italian, Portuguese, and Spanish versions of the View of Condition Impact scale. ICR scores for the English version of the FaMM were roughly comparable for Ireland, the United Kingdom, and the United States, demonstrating strong ICR. However, there were some notable differences in ICR scores between Brazil and Portugal. Scores exceeded .70 on four FaMM scores among respondents from Portugal, but only two scales among respondents from Brazil. For both countries, the Family Life Difficulty and Parental Mutuality Scales had the strongest ICR values and View of Condition Impact had the lowest.
Internal Consistency Reliability and Sample Sizes of Translations of the Family Management Measure (FaMM) Scales.
Cross-Cultural Differences in Family Management
In Table 5, we present a summary of the FaMM mean scale scores across countries. Because of the small number of respondents from different Central and South American countries, only Spain was included in the cross-cultural analysis of the Spanish version of the FaMM. Except for the Condition Management Ability and the View of Condition Impact scales, respondents used the full range of response options (1–5) for all scale items, indicating the scales effectively tap the variability in parents’ perceptions of the family experience of having a family member with DS. For the Condition Management Ability and View of Condition Impact scales, no respondent had the lowest possible ability or the highest possible impact score. Based on the FaMM scale means for the total sample, there was evidence that parents of individuals with DS have positive perceptions of all aspects of family management of DS. Total sample mean scores for the three FaMM scales reflecting areas of strength in family management (i.e., Condition Management Ability, Child’s Daily Life, and Parental Mutuality) were above the midpoint of possible scores, while mean scores for the three FaMM scales reflecting areas of problematic family management (i.e., Family Life Difficulty, Condition Management Effort, and View of Condition Impact) were below the midpoint. Furthermore, in terms of country-specific FaMM scale mean scores, the range of mean scores for the six FaMM scales reflected a pattern of relatively high mean scores for FaMM scales reflecting areas of family strength and relatively low mean scores for FaMM scales reflecting more problematic family management.
Score Range, Scale Means, and Mean Rankings of Family Management Measure Scales Across Countries.
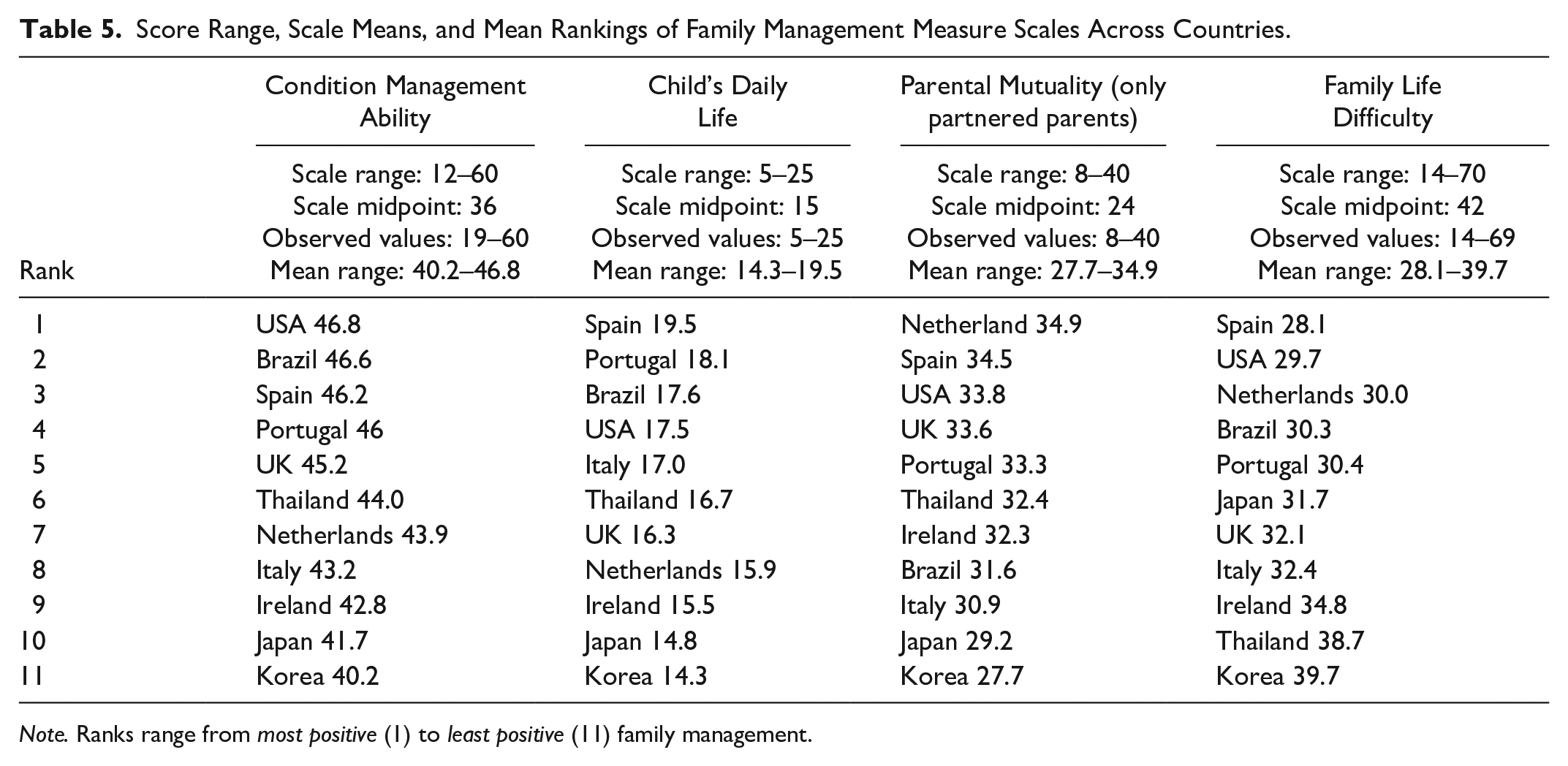
Note. Ranks range from most positive (1) to least positive (11) family management.
Despite this overall pattern of positive family management, there were differences across countries. Analysis of variance revealed an overall significant (p < .001) across-country difference for the means of each of the FaMM scales. This remained significant (p < .001) after controlling for covariates, one-at-a-time or altogether, thereby supporting a cross-cultural country effect. To identify overall patterns of difference across countries, mean scores for each country for the four FaMM subscales with ICR scores exceeding .70 (Condition Management Ability, Child’s Daily Life, Parental Mutuality, and Family Life Difficulty) were ranked from 1 to 11, with a rank of 1 signifying the most positive view of family management and a rank of 11 signifying the least positive view. On average, parents from countries with a scale rank of 1 perceived themselves as being the most competent in the management of their family member’s condition (Condition Management Ability) and, for couples, as having a shared view of their son or daughter and approach to condition management (Parental Mutuality). They had a positive view of their son or daughter and their life (Child’s Daily Life) and reported that condition management did not make everyday family life more challenging (Family Life Difficulty). In contrast, respondents from countries with a scale rank of 11 had the most negative view of their family management.
As reflected in Table 5, respondents from some countries had on average predominantly high FaMM scale rankings (1–4) and some had predominantly low rankings (8–11). Respondents from Brazil, Spain, and the United States ranked between 1 and 4 on at least three out of the four FaMM scales with ICR scores exceeding .70. In contrast, respondents from Ireland, Italy, Japan, and Korea ranked between 8 and 11 on at least three of these four FaMM scales. For the four remaining countries, the rankings were mixed; parents from Portugal and the United Kingdom had a combination of high- and moderate-level rankings, parents from the Thailand had a combination of moderate- and low-level rankings, and parents from the Netherlands had rankings that spanned across all three levels.
Discussion
Our current understanding of how families adapt to having a family member with DS is based primarily on findings from studies conducted with families who live in Western countries. Moreover, the outcomes assessed in these studies have typically been individual outcomes such as parental stress and parental well-being. In this study, existing gaps in the literature were addressed by including families of individuals with DS from both Eastern and Western countries. In addition, the primary focus of this study was a family-level variable, parents’ perception of family management. Family management of the ongoing challenges associated with having a family member with DS was assessed using the FaMM (Knafl et al., 2011).
Findings from this study provide evidence of overall strong ICR of the FaMM when it is used with parents of individuals with DS. For the entire sample, ICR scores for the FaMM ranged from .90 for the Family Life Difficulty scale to .61 for the Family Life Impact scale. Findings from this study also provide evidence of the ICR of the English version of the FaMM, as well as the seven translations of the FaMM. The Family Life Difficulty and Parental Mutuality scales demonstrated excellent ICR across language versions. In addition, ICR scores for two other FaMM scales (i.e., Condition Management Ability and Child’s Daily Life) were above .60 across language versions. The ICR scores for the remaining two FaMM scales (i.e., View of Condition Impact and Condition Management Effort) were below .60 for three language versions; ICR scores were below .60 for the Italian, Portuguese, and Spanish versions of the View of Condition Impact scale and below .60 for the Korean, Spanish, and Thai versions of the Condition Management Effort scale.
While this is the first known study to use eight language versions of the FaMM, there are at least 16 published reports of studies using one or more of the FaMM scales in a language other than English: Chinese (Hsiao & Van Riper, 2011; Sheng et al., 2018; Zhang et al., 2014, 2015; Zhang, Wei, Han, et al., 2013; Zhang, Wei, Zhang, et al., 2013); Dutch (Geense et al., 2018); Korean (H. Choi & Van Riper, 2014; Ima et al., 2019; Kim & Im, 2015; Son et al., 2018); Portuguese (Mendes et al., 2016, 2017; Salvador et al., 2018); and Thai (Chusri et al., 2019; Sananreangsak et al., 2012). Unfortunately, in many of these publications, the researchers did not report the ICR scores for the FaMM scales used in their study.
When researchers who used the FaMM did report the ICR scores for their sample, the ICR scores were fairly similar to those reported in this study. For example, Mendes and colleagues (2016, 2017) reported ICR scores of .79 for the Parental Mutuality scale and .83 for the Family Life Difficulty scale in a study involving Portuguese parents of children with asthma, obesity, epilepsy, and diabetes and ICR scores of .73 for the Child Daily Life scale and .86 for the Family Life Difficulty scale for a study with Portuguese parents of children with epilepsy. In the current study with families of children with DS, ICR scores for the Portuguese version were .85 for the Parental Mutuality scale, .89 for the Family Life Difficulty scale, and .72 for the Child Daily Life scale. In studies with Korean parents of children with DS conducted by H. Choi and Van Riper (2014) and Kim and Im (2015), ICR scores ranged from .63 to .90 and .69 to .90, respectively, while in the current study the ICR scores ranged from .55 to .90 for the Korean translation of the FaMM. In a study concerning parents of children with thalassemia from Thailand conducted by Chusri and colleagues (2019), ICR scores for the FaMM scales ranged from .26 to .82; for this study, the ICR scores for the Thai translation of the FaMM ranged from .28 to .86. The study by Chusri and colleagues stands out in reporting a low ICR score for the Child’s Daily Life scale, which was one of the most robust scales across countries in the current analysis with ICR scores ranging from .60 to .73. Given that some FaMM scales have low ICR scores for one or more language versions, researchers interested in using language versions of the FaMM other than English may want to consider using only the FaMM scales found to have acceptable ICR scores for that language version.
Findings from this study provide evidence of an overall positive pattern of family management among a culturally diverse sample of families of individuals with DS. There was, however, evidence of cross-cultural differences in family management with parents from Brazil, Spain, and the United States reporting the least problematic family management and parents from Ireland, Italy, Japan, and Korea reporting the most problematic family management. It is important to note that these cross-cultural differences remained significant (p < .001) after controlling for covariates (i.e., age of the individual with DS, age of the parent completing the survey, number of children in the family, mother vs. father, and partnered vs. not partnered), thereby supporting a cross-cultural effect.
There is growing evidence that across countries social determinants of health (SDOH), such as access to health care, education of primary caregiver, family income, environmental conditions, psychosocial resources, societal attitudes toward people with disabilities, and social support, have a critical impact on how individuals and families are affected by DS and other chronic conditions such as congenital heart disease which is common in individuals with DS (Geok et al., 2013; Haddad et al., 2018; Jackson et al., 2015; Xiang et al., 2019). Thus, it is likely that the SDOH may have contributed to the cross-cultural differences in family management revealed in this study. For example, looking at the countries reporting the most problematic family management (Ireland, Italy, Japan, and Korea), two of these countries (Ireland and Italy) were experiencing an economic crisis during the time frame data were being collected. As a result of the economic crisis in Ireland, families experienced social service cuts in many areas including health care spending and disability allowances (McGinnity et al., 2014). In addition, many families in Ireland experienced a reduction in family income, an increase in costs for needed items, and the removal of discretionary medical cards (Caples et al., 2018). In Italy, the economic crisis affected families in a similar manner. Moreover, in Italy, public policies for individuals with disabilities and their families are not well developed (Covelli et al., 2018). Because of this, the health, employment, and social needs of many individuals with DS, especially adults with DS, are not being met (Bertoli et al., 2011) and their families may feel overwhelmed.
Three Asian countries (Japan, Korea, and Thailand) were among the countries reporting the most problematic family management. This finding may be due, in part, to the fact that many families in these countries practice Confucianism and certain features of Confucian values, such as strict gender roles and the expectation that the mother is the primary caregiver are likely to impact a mother’s ability to manage the ongoing challenges associated with DS (H. Choi & Van Riper, 2017; Park & Chesla, 2007). According to Confucian values, women are expected to care for family members, especially family members with chronic conditions and disabilities, with limited assistance from male family members. This is likely to result in increased demands being placed on Asian mothers of individuals with DS.
In this study, most of the participants from Japan, Korea, and Thailand were mothers and it is likely that many of them were managing the challenges associated with DS on their own rather than receiving assistance from their spouse or partner. Mean scores on the parental mutuality scale which addresses perceptions of support, shared views, and satisfaction with how partners work together to manage their child’s condition were lowest for parents from Korea and Japan. Korea ranked 11 with a mean score of 27.7, Japan ranked 10 with a mean score of 29.2, and Thailand ranked 6 with a mean score of 32.4. It is important to note that although these mean scores for parental mutuality were lower than those for most of the other countries, they were above the mean suggesting that while the mothers in these countries are the ones primarily responsible for caring for the family member with DS, the mothers may accept this division of labor because it is deemed culturally appropriate.
For this study, as well as much of the existing research concerning adaptation in families of individuals with DS participants were volunteers. However, respondents used the full range of response options (1–5) for all scale items on four of the FaMM scales, suggesting that our sample included parents who report strength in family management as well as parents who reported problematic family management. Ranking of mean scores for FaMM scales provides for ordering countries on the six FaMM dimensions. However, it does not provide an assessment of which countries have means that are the same or different as would be addressed with a post hoc analysis but these generated very complicated results that were difficult to interpret, so they were not included in the results.
Conclusion
Findings from this cross-cultural study provide evidence of overall strong ICR of the FaMM when it is used with parents of individuals with DS. In addition, parental perceptions of family management were generally positive. While there was evidence of cross-cultural differences in family management, it is important to note that in terms of country-specific FaMM scale mean scores, the range of mean scores for the six FaMM scales reflected a pattern of relatively high mean scores for FaMM scales reflecting areas of family strength and relatively low mean scores for FaMM scales reflecting more problematic family management. Moreover, mean scores for the three FaMM scales reflecting areas of strength in family management were close to or above the midpoint of possible scores, while mean scores for the three FaMM scales reflecting areas of problematic family management were close to or below the midpoint of possible scores. Therefore, even though the mean ranking for a country may have been high on the FaMM scales reflecting areas of problematic family management, signifying the least positive view of family management, the mean scores across countries actually reflected relatively positive family management in terms of the range of possible scale scores. At the same time, the broad range of scores across scales and countries provide evidence of considerable variation across families regarding the extent to which they are able to address the management challenges associated with having a child with DS.
More cross-cultural research is needed to fully understand how culture and social determinants influence family management in families of individuals with DS. Moreover, it is important that both within and across-country variation in family management be examined because findings from this study add to the growing evidence that while some families struggle with the challenges associated with raising a family member with DS, others adapt well and some thrive. Gaining a more comprehensive understanding of modifiable factors contributing to better outcomes for individuals with DS, their parents/caregivers and their families will facilitate the identification of individual, family, group, and country-specific challenges facing families of individuals with DS and this will contribute to the development of more precisely tailored interventions.
Footnotes
Acknowledgements
The authors offer their most sincere thanks to the families who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
![]() ) and “Young Italian NEETs (Not in Employment, Education or Training) and the Influence of Their Family Background” in Europe’s Journal of Psychology (2015, with S. Alfieri, E. Sironi, A. Rosina, & D. Marzana. DOI: 10.5964/ejop.v11i2.901).
) and “Young Italian NEETs (Not in Employment, Education or Training) and the Influence of Their Family Background” in Europe’s Journal of Psychology (2015, with S. Alfieri, E. Sironi, A. Rosina, & D. Marzana. DOI: 10.5964/ejop.v11i2.901).