
Abstract
Down syndrome (DS) is a chromosomal disorder associated with intellectual and physical disabilities and has historically been viewed by health care providers through a negative lens when considering the effect the condition has on the individual, family, and community. The purpose of this scoping review was to provide an overview of recent research concerning adaptation in families of individuals with DS with a focus on family adaptation rather than individual or dyadic adaptation. Three literature indexes were searched from 2017 to 2022, with 41 articles included. Foci of the studies included strength/resilience, stress/coping, and negative/challenge. Thirteen studies reported using a family framework. Multiple methodological approaches and family measures were used in the studies and are outlined. Findings from this review show there has been a shift in focus when researching families of individuals with DS from a negative and challenging experience to one of strength and resilience.
Down syndrome (DS) is a chromosomal disorder associated with intellectual and physical disabilities. Individuals with DS have an increased risk of mortality and morbidity due to co-occurring health concerns such as congenital heart disease, thyroid dysfunction, hematological disorders, autoimmune conditions, and obstructive sleep apnea (Antonarakis et al., 2021; Bull et al., 2022). However, improvements in health care for individuals with DS, especially surgical treatment of congenital heart defects, have resulted in impressive changes in life expectancy and quality of life for individuals with DS (Antonarakis et al., 2021; Carr & Collins, 2018; Hughes-McCormack et al., 2020). In some countries, life expectancy for individuals with DS is approaching that of the general population (Lemoine & Schneider, 2022).
Current estimates of the live birth rate for DS range from one in 546 to one in 1350 live births (Alexander et al., 2016; Antonarakis et al., 2021; Caples et al., 2018; de Graaf et al., 2015, 2021; Hughes-McCormack et al., 2020), making it the most common genetic cause of intellectual disability (Antonarakis et al., 2021; Huete-Garcia & Otaola-Barranquero, 2021). Differences in live birth rates for DS from one country to the next are due to factors such as maternal age at conception, availability and accuracy of prenatal testing, access to elective terminations, societal views about DS, parental decision-making when a prenatal diagnosis of DS is made, and quality of health care available to individuals with DS (Antonarakis et al., 2021; de Graaf et al., 2021; Huete-Garcia & Otaola-Barranquero, 2021).
When expectant and new parents first learn that their child might or does have DS, many are concerned about the impact this will have on their family (Crombag et al., 2020; Kammes et al., 2022; Muggli et al., 2009; Skotko, 2005a, 2005b; Van Riper, 2007). There is growing evidence that many health care providers are not prepared to provide accurate, up-to-date information about how families adapt to having a child with DS (Crombag et al., 2020; Gabel & Kotel, 2018; Kammes et al., 2022; Marshall et al., 2019; Muggli et al., 2009; Skotko, 2005a, 2005b; Skotko et al., 2009; Van Riper, 2007; Van Riper & Choi, 2011). Moreover, despite growing evidence that many families adapt successfully to the challenges associated with raising a child with DS, many health care providers continue to believe that the birth of a child with DS will have a negative impact on the child’s family, their community, and society as a whole (Van Riper & Choi, 2011; Van Riper et al., 2021).
The purpose of this scoping review was to provide an overview of recent research concerning adaptation in families of individuals with DS. For this review, we focused on adaptation at the family system level rather than the individual or dyadic level. The following questions were addressed in this review of research concerning family-system-level adaptation in families of individuals with DS: (a) Which family members participated in the studies and what family system variables were examined? (b) What qualitative approaches have been used in qualitative and mixed-methods studies? (c) What family measures have been used in quantitative and mixed-methods studies?
Findings from this scoping review will set the stage for an integrative or systematic review in which results from studies concerning family-system-level adaptation in families of individuals with DS are described and synthesized. A description and synthesis of the findings will give health care providers a more accurate and up-to-date understanding of family life in the context of DS. By understanding both the challenges and joys associated with raising a child with DS, health care providers will be better prepared to advise and support families as they share the DS diagnosis and guide them in accommodating the child’s unique needs.
Background
Early research on families of children with DS focused almost exclusively on the negative consequences associated with having a child with DS (Cuskelly et al., 2009; Ferguson, 2002; Hodapp, 2007). In addition, much of the early research focused on maternal adaptation, rather on paternal adaptation or adaptation at the family level. It was not until the early 1980s that this predominantly negative focus began to change. In 1983, Crnic et al. encouraged researchers to consider using a stress-and-coping perspective, conceptualizing the presence of a child with DS as a stressor that could account for a range of consequences for the family, both negative and positive, and that could be accommodated through effective coping.
Starting in the 1990s, there has been a notable increase in research focusing on strengths and resilience in families of individuals with DS (Cunningham, 1996; Flaherty & Glidden, 2000; Shonkoff et al., 1992; Sloper et al., 1991; Van Riper, 1999, 2000, 2007; Van Riper et al., 1992). However, much of this research has focused on adaptation at the individual level, rather than at the family system level. A review of over 90 studies examining adaptation in families of individuals with DS conducted between 2006 and 2016 (Van Riper et al., 2021) revealed that only a third of the studies included an assessment of adaptation at the family system level (Ajuwon, 2012; Auyeung et al., 2011; Blacher & McIntyre, 2006; Burke & Hodapp, 2014; Carling-Jenkins et al., 2012; Carr, 2008; H. Choi, 2015; E. K. Choi & Yoo, 2015; Corrice & Glidden, 2009; Dabrowska & Pisula, 2010; Foley et al., 2014; Gau et al., 2008; Griffith et al., 2010; Hsiao, 2014; Hsiao & Van Riper, 2011; King et al., 2009, 2011; Lanfranchi & Vianello, 2012; Leonard et al., 2016; Marchal et al., 2016; McGrath et al., 2011; Mitchell et al., 2015; Muggli et al., 2009; Neely-Barnes et al., 2010; Nelson Goff et al., 2016; Phelps et al., 2012; Povee et al., 2012; Rieger & McGrail, 2013; Skotko et al., 2016; Stoneman, 2007; van der Veek et al., 2009; Van Riper, 2007). Another limitation of the current research noted by Van Riper et al. (2021) was that the majority of the studies were conducted with English-speaking families of individuals with DS living in Western countries.
This scoping review extends the earlier review conducted as part of a larger cross-country analysis by Van Riper et al. (2021) concerning studies of family system adaptation in families of individuals with DS published between 2006 and 2017. For this review, the focus is on research published between 2017 and 2022. Key concepts from the Resiliency Model of Family Stress, Adjustment, and Adaptation (McCubbin et al., 1996) were used to categorize the studies in this review. Grounding this review in an established family framework provides a structured conceptual approach for examining how interacting family variables (i.e., family demands, family appraisal, family resources, family problem-solving communication, and family coping) shape processes and outcomes associated with adaptation at the family level in families of individuals with DS.
Method
The methodology for this scoping review was informed by Arksey and O’Malley (2005) and the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols for Scoping Reviews (Arksey & O’Malley, 2005; Tricco et al., 2018). A scoping review approach was selected for this review in order to include a wide range of methodologically diverse studies addressing adaptation in families of individuals with DS. Consistent with scoping review guidelines, we did not complete a formal quality assessment of studies. However, in an effort to safeguard against including studies of lower quality, only peer-reviewed studies were included.
Eligibility Criteria
While the initial search for this scoping review was broad which included research articles on adaptation at the individual, dyadic, and family levels in families of individuals with DS, the focus for this article is on recent studies in which adaptation was assessed at the family level. Inclusion and exclusion criteria are listed below.
Inclusion Criteria
Assessment of family system variables in families of individuals with DS;
English language publication;
Works published between 2017 and 2022.
Exclusion Criteria
Did not address family system adaptation;
Did not differentiate results for families of individuals with DS from the results for families of individuals with other conditions when the sample included families of individuals with other conditions;
Non-research publications;
Unpublished manuscripts.
Search
In collaboration with a research librarian, the search was completed using the online databases PubMed, CINAHL, and PsycInfo, for the years 2017 to 2022. Search terms were adapted to meet the constraints of each database, with the search terms used for CINAHL listed here: Family OR families OR father* OR mother* OR parent OR parents OR parental OR sibling* OR brother* OR sister* OR grandparent* OR grandmother* OR grandfather* OR aunt* OR uncle* OR caregiv* OR “care giver” OR caretaker OR “care taker”) AND (MH “Down Syndrome”) OR “down syndrome” OR “downs syndrome” OR “down’s syndrome” OR “trisomy 21” OR “chromosome 21”) AND (Adapt* OR cope OR coping OR “well-being” OR resilien* OR adjust* OR “quality of life” OR QOL OR impact* OR stress* OR “family function” OR “family functioning”). Data from each database were exported to Covidence for organization of title and abstract screening and full-text review (Veritas Health Solutions, Melbourne, Australia). In addition, reference lists of included articles were hand-checked to identify articles not captured in the database searches.
Selection of Sources of Evidence
Two reviewers, M.V.R. and B.C., independently completed a title and abstract review. If it was unclear whether the article met inclusion criteria based on the abstract, a full-text review was completed. At each level of review, the two authors discussed any conflicts to reach consensus for inclusion.
Charting the Data
Data were extracted and charted by the second author using a structured template that included author (s), publication year, country of study participants, study purpose/aims, conceptual underpinnings, design, sample (size/family member participants/age of participants/ age of persons with DS), and assessment of adaptation at the family level (family system variables assessed/measures used to assess key concepts of the Resiliency Model). The first author then reviewed the extractions for clarity, accuracy, and completeness.
Collating and Summarizing Data
A basic numerical analysis was completed to tally study characteristics. In addition, authors M.V.R. and B.C. independently reviewed the study purpose/aim and background sections of each study to categorize the primary focus of each study as (a) strength and resilience focused, (b) stress and coping focused, or (c) negative/problem focused. Then, conflicts were discussed to reach consensus. Studies that focused on strength and resilience are those that focused on the family system’s ability to adapt, evolve, and thrive in the face of ongoing challenges associated with having a family member with DS. In these studies, there was an effort to look beyond coping with outcomes such as empowerment, strength, and positive gains. Studies that focused on stress and coping are those that recognized the presence of a family member with DS as a stressor that could account for a range of consequences for the family that could be accommodated through effective coping. Negative/problem-focused studies are those that focused on the negative consequences associated with having a family member with DS.
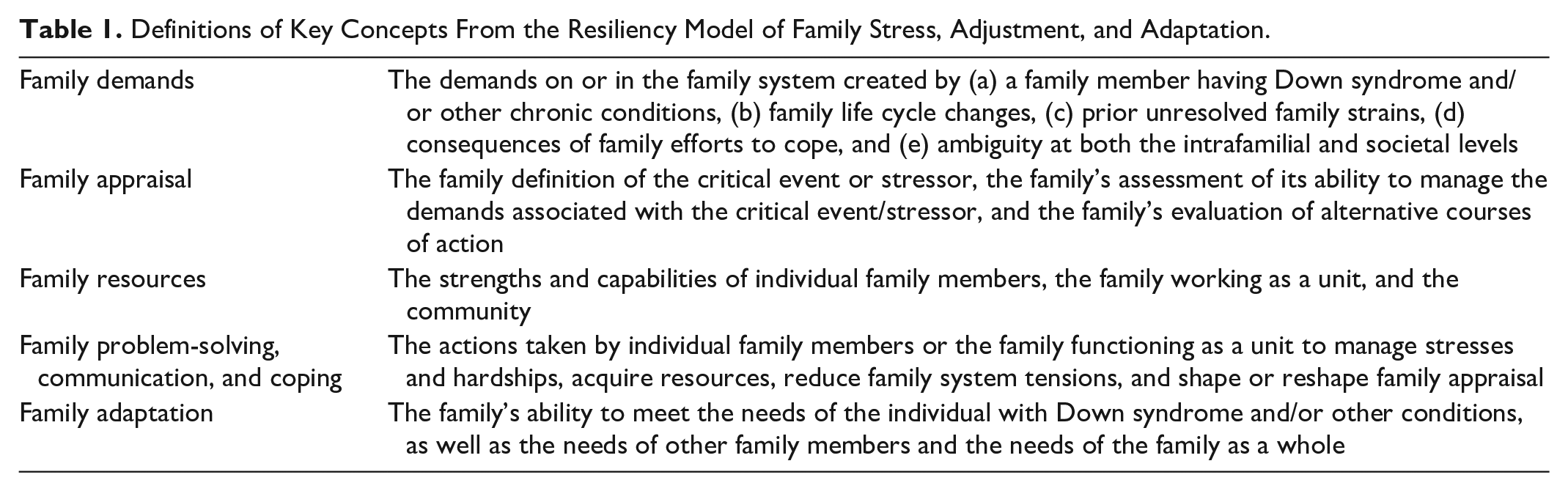
Using the same review processes described above, M.V.R. and B.C. categorized the family system variables addressed in the studies using the key concepts from the Resiliency Model of Family Stress, Adjustment, and Adaptation (McCubbin et al., 1996). See Table 1 for definitions of the key concepts.
Definitions of Key Concepts From the Resiliency Model of Family Stress, Adjustment, and Adaptation.
Results
The search of PubMed, CINAHL, and PsycInfo elicited 473 articles with an additional two articles from other sources after duplicates were removed. Three hundred seventy-six articles were excluded following title and abstract screening, leaving 99 articles to undergo a full-text review. Fifty-eight articles were excluded following the full-text review. Most articles were excluded because data on family system adaptation were not collected. Other exclusion criteria were that the researchers did not differentiate results for families of individuals with DS from the results for families of individuals with other conditions and that it was a non-research publication. The PRISMA diagram is provided in Figure 1.
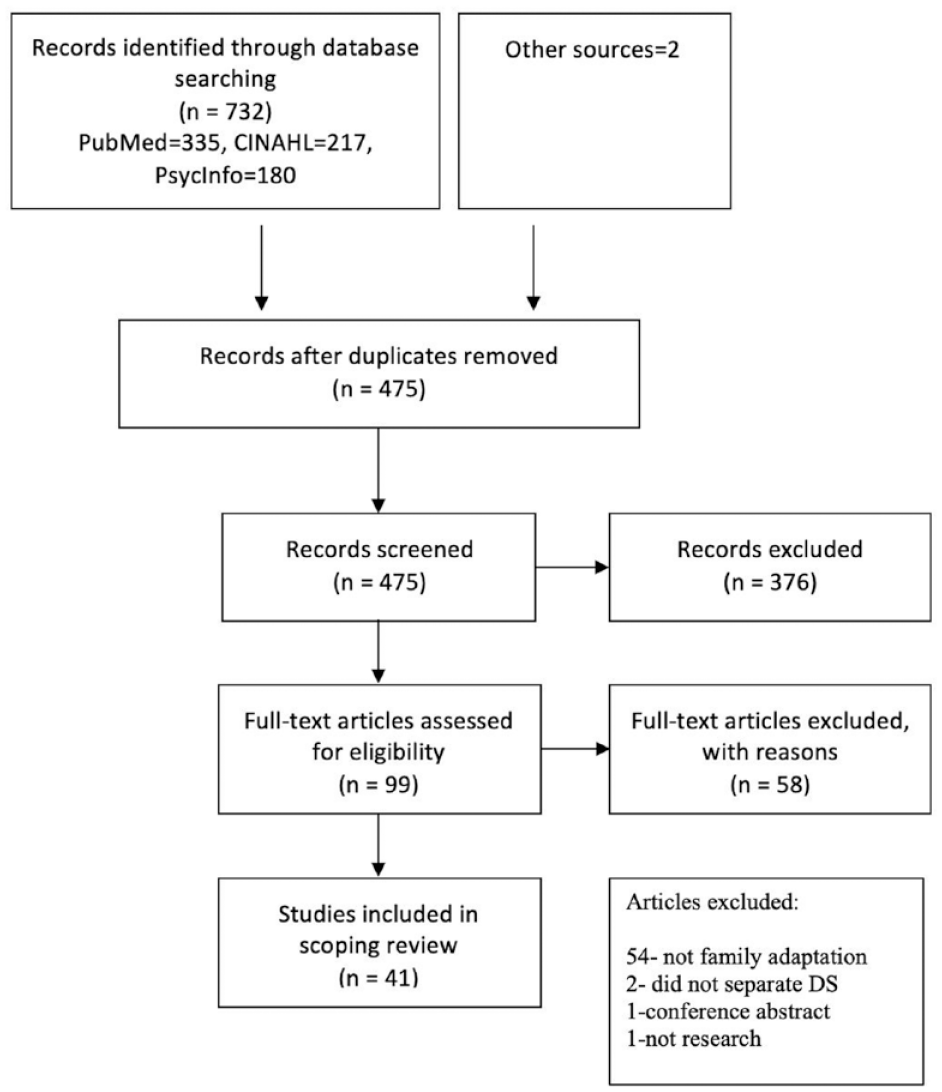
PRISMA Diagram.
Country of Study Participants
Thirty-nine of the 41 studies included participants from a single country (see Table 2). These studies were conducted in the following 20 countries: Belgium (2), Brazil (4), Canada (2), Croatia (1), Denmark (1), Ecuador (1), France (1), India (1), Iran (1), Ireland (2), Israel (1), Italy (1), Japan (1), Korea (1), Poland (2), Saudi Arabia (3), Spain (1), Thailand (2), the United Kingdom (1), and the United States (10). The study conducted by Van Riper et al. (2021) was a cross-cultural investigation that included participants from 11 countries (Brazil, Ireland, Italy, Japan, Korea, Netherlands, Portugal, Spain, Thailand, the United Kingdom, and the United States), and country-specific findings were reported. The study by A. Lee et al. (2020) included participants from 18 countries (Australia, Bosnia and Herzegovina, Canada, Denmark, Germany, India, Ireland, Malta, Mexico, Netherlands, Poland, Slovenia, South Africa, Sweden, Switzerland, Ukraine, the United Kingdom, and the United States), with 77.7% of the participants being from the United States. Country-specific findings were not reported because the number of participants from each of the 18 countries varied greatly. For example, while 164 of the participants were from the United States, there were 16 participants from the United Kingdom and less than 10 participants from the remaining 16 countries.
Studies With Participants From a Single Country.

Purpose/Aims
The purpose/aims of the 41 studies are shown in Table 3. In addition, the studies have been categorized into three groups based on the primary focus of the study: (a) strength and resilience focused, (b) stress and coping focused, and (c) negative/problem focused. Twenty-six of the studies were categorized as strength and resilience focused. In these studies, the focus was on the ability of the family system to adapt, evolve, and thrive in the face of the ongoing challenges associated with having a family member with DS. For example, Clark et al. (2020) developed a grounded theory of rescuing hope through ongoing sense-making. They noted that Rescuing hope does not deny the paradox of disability, that one’s child and one’s family life will be both joyful and tearful, uplifting, and challenging. Rather sense-making to rescue hope encompasses the lived experiences that take time to process, interpret and constitute as family resources for adaptive functioning. (Clark et al., 2020, p. 15)
Study Purpose/Aims as Stated by Authors and Categorization of Overall Approach.
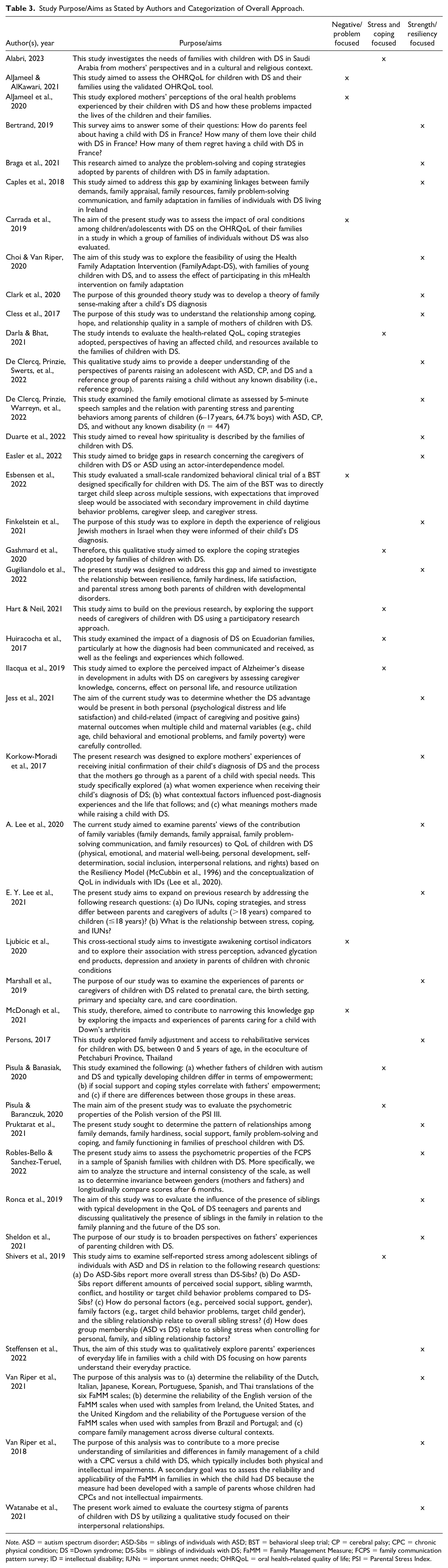
Note. ASD = autism spectrum disorder; ASD-Sibs = siblings of individuals with ASD; BST = behavioral sleep trial; CP = cerebral palsy; CPC = chronic physical condition; DS =Down syndrome; DS-Sibs = siblings of individuals with DS; FaMM = Family Management Measure; FCPS = family communication pattern survey; ID = intellectual disability; IUNs = important unmet needs; OHRQoL = oral health-related quality of life; PSI = Parental Stress Index.
An example of a quantitative study categorized as strength and resilience focused is the study by Gugliandolo et al. (2022). In this study, guided by the Resiliency Model of Family Stress, Adjustment, and Adaptation, they assessed the relationship between resilience, family hardiness, life satisfaction, and parental stress among both parents of children with developmental disabilities. Fifteen of the dyads included parents of children with DS.
Nine studies were categorized as stress and coping focused. An example of a study categorized as stress and coping focused is the study by Gashmard et al. (2020). In this study, the researchers explored the coping strategies adopted by the families of children with DS. Family members from 20 families were interviewed.
Six studies were categorized as negative/problem focused. The study by McDonagh et al. (2021) is an example of a study that is negative/problem focused. Semi-structured interviews were conducted with 10 mothers living in the Republic of Ireland who have a child with DS who also has arthritis. In this study, the primary focus was on negative consequences.
Conceptual Underpinning
Although most authors (N = 28) did not identify the conceptual underpinnings of their study, 13 reported using a family framework, including the Resiliency Model of Family Stress, Adjustment, and Adaptation or earlier versions of the model by McCubbin et al. (1996) (Braga et al., 2021; Caples et al., 2018; J. Choi & Van Riper, 2020; Cless et al., 2017; Duarte et al., 2022; Easler et al., 2022; Gugliandolo et al., 2022; A. Lee et al., 2020; E. Y. Lee et al., 2021; Pruktarat et al., 2021; Knafl et al., 2012; Knafl & Deatrick, 2003), the Family Management Style Framework (Van Riper et al., 2018, 2021), and the combined Ecological CBR and Family Systems Theory by Nihira et al. (1994) (Persons, 2017).
Study Design
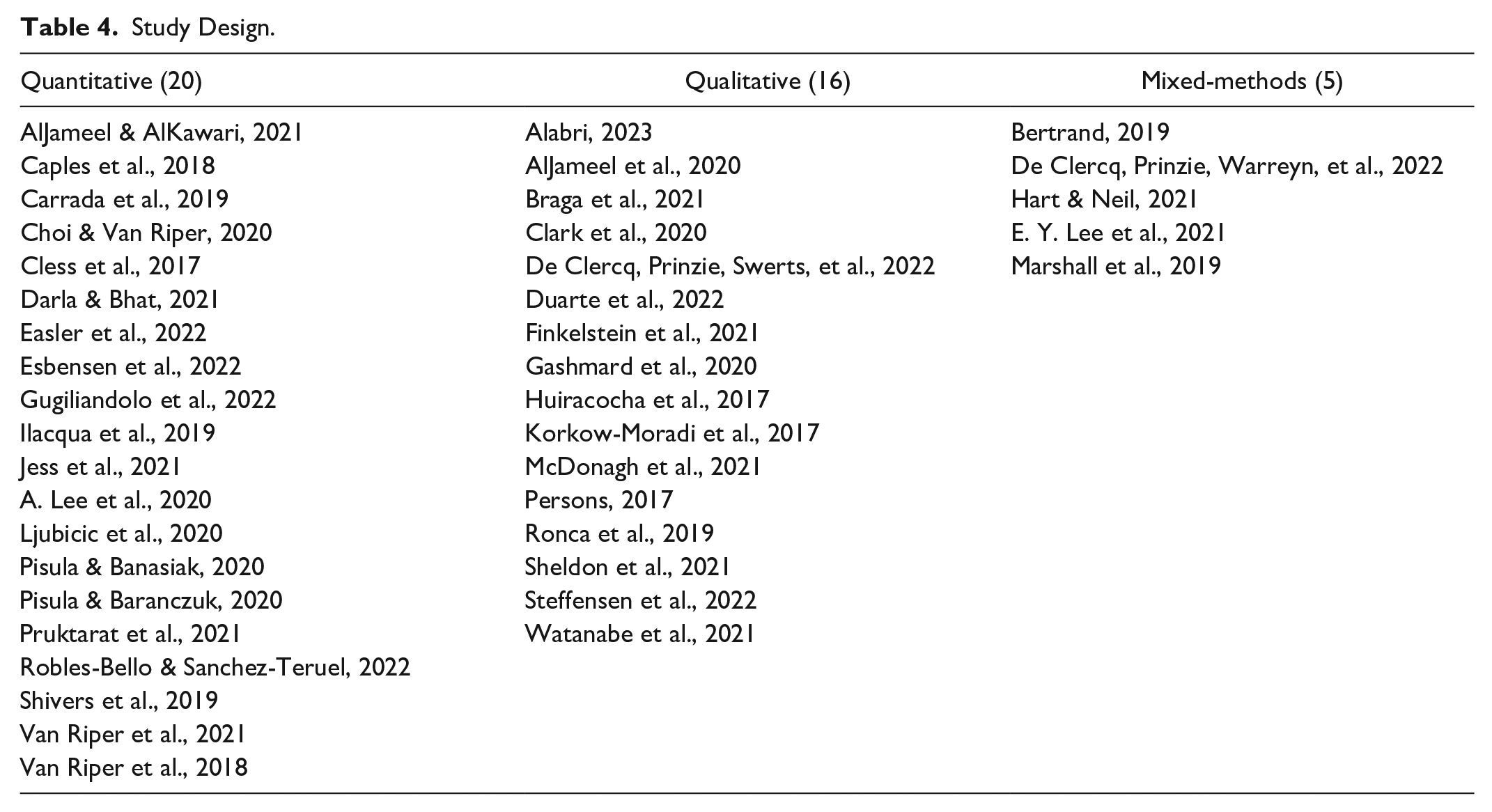
The 41 articles in the final sample included studies with a variety of designs. Twenty of the studies were quantitative, 16 were qualitative, and five were mixed methods (see Table 4). There were only two experimental studies; one had a one-group pre-/post-test design (Choi & Van Riper, 2020), and the other was a randomized control trial (Esbensen et al., 2022). Most of the studies were cross-sectional; there were only two longitudinal studies (Choi & Van Riper, 2020; Robles-Bello & Sanchez-Teruel, 2022). With the exception of two grounded theory studies (Clark et al., 2020; Korkow-Moradi et al., 2017) and two phenomenological studies (Finkelstein et al., 2021; McDonagh et al., 2021), the qualitative studies were descriptive.
Study Design.
Respondents
Across the 41 studies, researchers collected data from 5,989 respondents (Table 5), 4,438 (78%) of whom were the child’s mother, with 9 studies focusing exclusively on mothers (Alabri, 2023; AlJameel & AlKawari, 2021; AlJameel et al., 2020; Cless et al., 2017; Finkelstein et al., 2021; Jess et al., 2021; Korkow-Moradi et al., 2017; McDonagh et al., 2021; Pruktarat et al., 2021). Fathers were included in 29 studies and were the exclusive focus of two studies (Pisula & Banasiak, 2020; Sheldon et al., 2021). Ten studies included multiple care givers from a family, with three studies including only dyads within the sample (Choi & Van Riper, 2020; Darla & Bhat, 2021; Easler et al., 2022; Gugliandolo et al., 2022; Huiracocha et al., 2017; Persons, 2017; Steffensen et al., 2022; Van Riper et al., 2018, 2021; Watanabe et al., 2021). In seven studies, totaling 351 respondents, the authors did not specify who the family member respondent was (Carrada et al., 2019; Darla & Bhat, 2021; Huiracocha et al., 2017; Ilacqua et al., 2019; Ljubicic et al., 2020; Persons, 2017; Steffensen et al., 2022).
Data Related to Participants Across Studies in Review.
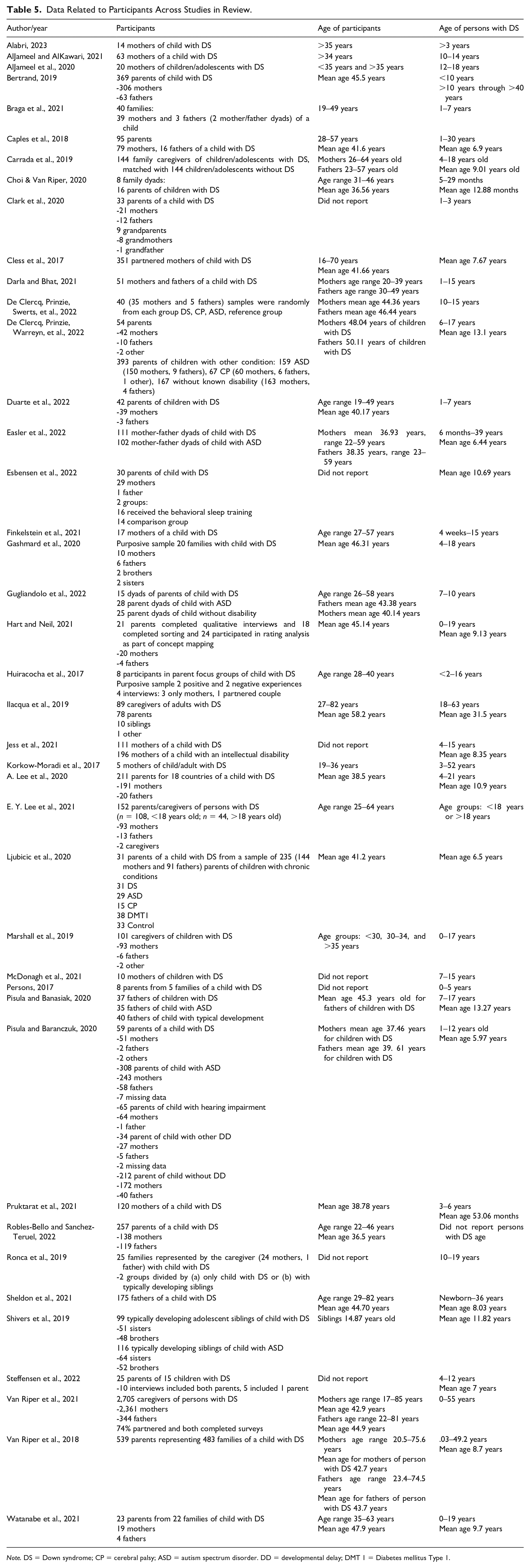
Note. DS = Down syndrome; CP = cerebral palsy; ASD = autism spectrum disorder. DD = developmental delay; DMT 1 = Diabetes mellitus Type 1.
Age of Individuals With DS
Studies varied greatly in reporting the age of the individual with DS (Table 5). Sixteen of the 41 studies included an age range (Al Jameel et al., 2020, AlJameel & AlKawari, 2021; Braga et al., 2021; Clark et al., 2020; Darla & Bhat, 2021; De Clercq, Prinzie, Swerts, et al., 2022; Duarte et al., 2022; Finkelstein et al., 2021; Gashmard et al., 2020; Gugliandolo et al., 2022; Korkow-Moradi et al., 2017; Marshall et al., 2019; McDonagh et al., 2021; Persons, 2017; Ronca et al., 2019; Van Riper et al., 2021), with 16 also including a mean age (Caples et al., 2018; Carrada et al., 2019; Choi & Van Riper, 2020; De Clercq, Prinzie, Warreyn, et al., 2022; Easler et al., 2022; Hart & Neil, 2021; Ilacqua et al., 2019; Jess et al., 2021; A. Lee et al., 2020; Pisula & Banasiak, 2020; Pisula & Baranczuk, 2020; Pruktarat et al., 2021; Sheldon et al., 2021; Steffensen et al., 2022; Van Riper et al., 2018; Watanabe et al., 2021). Only a mean age was reported in four studies (Cless et al., 2017; Esbensen et al., 2022; Ljubicic et al., 2020; Shivers et al., 2019). In addition, four studies listed an open-ended age range such as >3 years old (Alabri, 2023; Bertrand, 2019; Huiracocha et al., 2017; E. Y. Lee et al., 2021). One study did not report the age of the individuals with DS (Robles-Bello & Sanchez-Teruel, 2022). A majority of studies included in the review (24 studies) focused on a younger age range (less than 18 years old), with four studies focusing on persons with DS under the age of 6 years (Choi & Van Riper, 2020; Clark et al., 2020; Persons, 2017; Pruktarat et al., 2021). Twelve studies included adults with DS aged 19 years or older (Bertrand, 2019; Easler et al., 2022; Hart & Neil, 2021; Ilacqua et al., 2019; Korkow-Moradi et al., 2017; A. Lee et al., 2020; E. Y. Lee et al., 2021; Ronca et al., 2019; Sheldon et al., 2021; Van Riper et al., 2018, 2021; Watanabe et al., 2021).
Reporting of age of respondent varied greatly, with most studies reporting an age range (Table 5). Twenty-three studies reported a mean age of respondents, with an overall mean age of 42.31 years; mothers 41.44 years, and fathers 44.05 years (Bertrand, 2019; Caples et al., 2018; Choi & Van Riper, 2020; Cless et al., 2017; De Clercq, Prinzie, Swerts, et al., 2022, De Clercq, Prinzie, Warreyn, et al., 2022; Easler et al., 2022; Gashmard et al., 2020; Gugliandolo et al., 2022; Hart & Neil, 2021; Ilacqua et al., 2019; A. Lee et al., 2020; Ljubicic et al., 2020; Pisula & Banasiak, 2020; Pisula & Baranczuk, 2020; Pruktarat et al., 2021; Robles-Bello & Sanchez-Teruel, 2022; Sheldon et al., 2021; Shivers et al., 2019; Van Riper et al., 2018, 2021; Watanabe et al., 2021). For one study, the respondent was the sibling of the person with DS with a mean age of 14.87 years (Shivers et al., 2019). Seven studies did not report the age of respondents (Clark et al., 2020; Esbensen et al., 2022; Jess et al., 2021; McDonagh et al., 2021; Persons, 2017; Ronca et al., 2019; Steffensen et al., 2022).
Assessment of Adaptation at the Family Level
Key concepts from the Resiliency Model of Family Stress, Adjustment, and Adaptation (McCubbin et al., 1996) were used to categorize the family-system-level variables assessed in the 41 studies (see Table 6). All five of the key concepts were assessed in one of the qualitative studies (Watanabe et al., 2021) and two of the quantitative studies (Caples et al., 2018; Choi & Van Riper, 2020). Four of the key concepts were assessed in four of the qualitative studies (De Clercq, Prinzie, Swerts, et al., 2022, De Clercq, Prinzie, Warreyn, et al., 2022; Duarte et al., 2022; Sheldon et al., 2021) and four of the quantitative studies (A. Lee et al., 2020; E. Y. Lee et al., 2021; Persons, 2017; Pruktarat et al., 2021). In the one qualitative study that included an assessment of all five key concepts, Watanabe et al. (2021) conducted semi-structured interviews to evaluate courtesy stigma and the adaptation process in 23 Japanese families of children with DS. Their interview guide included questions that focused on three themes: (a) negatively perceived interpersonal experiences and coping strategies, (b) information disclosure about a DS diagnosis and others’ responses to the disclosure, and (c) positively perceived interpersonal experiences. The two quantitative studies that included an assessment of all five key concepts were guided by the Resiliency Model of Family Stress, Adjustment, and Adaptation, and they used a variety of family measures developed by McCubbin et al. (1996). Caples et al. (2018) examined how Irish families of children with DS adapt to their child’s diagnosis of DS. Choi and Van Riper (2020) explored the feasibility of using a mHealth Family Adaptation Intervention with Korean families of young children with DS and assessed the effect of participating in this mHealth intervention on family adaptation.
Family System Variables Assessed in the Studies and Categorized According to Key Concepts From the Resilience Model of Family Stress, Adjustment, and Adaptation.
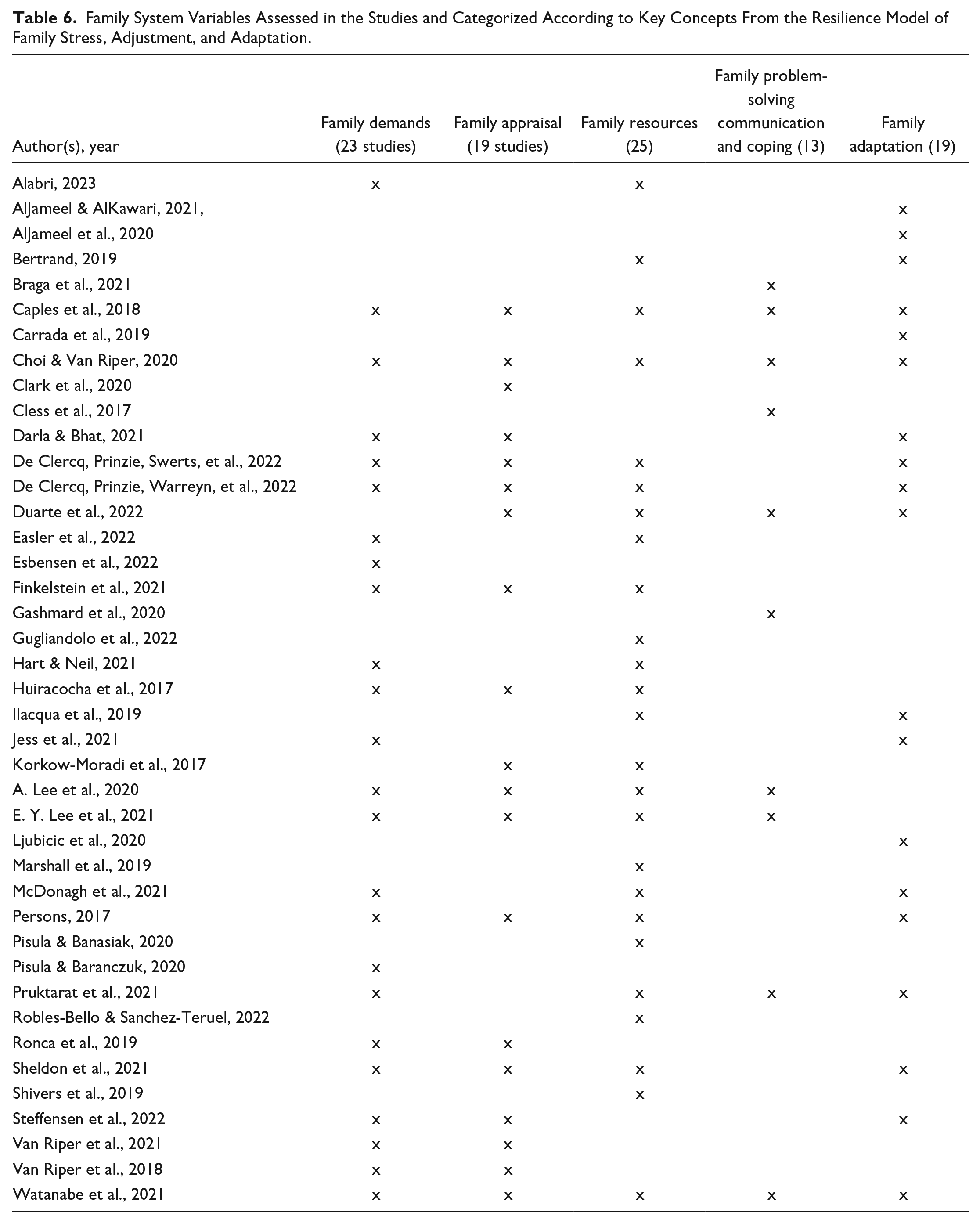
The two family concepts assessed most frequently were family resources and family demands. Twenty-five of the 41 studies included an assessment of family resources. Eleven of these studies were qualitative (Alabri, 2023; De Clercq, Prinzie, Swerts, et al., 2022; De Clercq, Prinzie, Warreyn, et al., 2022; Duarte et al., 2022; Finkelstein et al., 2021; Huiracocha et al., 2017; Korkow-Moradi et al., 2017; McDonagh et al., 2021; Persons, 2017; Sheldon et al., 2021; Watanabe et al., 2021), 10 were quantitative (Caples et al., 2018; Choi & Van Riper, 2019; Easler et al., 2022; Gugliandolo et al., 2022; Ilacqua et al., 2019; A. Lee et al., 2020; Pisula & Banasiak, 2020; Pruktarat et al., 2021; Robles-Bello & Sanchez-Teruel, 2022; Shivers et al., 2019), and four were mixed-methods (Bertrand, 2019; Hart & Neil, 2021; E. Y. Lee et al., 2021; Marshall et al., 2019). Twenty-four studies included an assessment of family demands. Of these, 11 were qualitative (Alabri, 2023; De Clercq, Prinzie, Swerts, et al., 2022; De Clercq, Prinzie, Warreyn, et al., 2022; Finkelstein et al., 2021; Huiracocha et al., 2017; McDonagh et al., 2021; Persons, 2017; Ronca et al., 2019; Sheldon et al., 2021; Steffensen et al., 2022; Watanabe et al., 2021), 11 were quantitative (Caples et al., 2018; Choi & Van Riper, 2020; Darla & Bhat, 2021; Easler et al., 2022; Esbensen et al., 2022; Jess et al., 2021; A. Lee et al., 2020; Pisula & Baranczuk, 2020; Pruktarat et al., 2021; Van Riper et al., 2018, 2021), and two were mixed-methods (Hart & Neil, 2021; E. Y. Lee et al., 2021).
Two of the other family concepts (family appraisal and family adaptation) were assessed in 19 studies. Twelve of the 19 studies that included an assessment of family appraisal were qualitative (Clark et al., 2020; De Clercq, Prinzie, Swerts, et al., 2022; De Clercq, Prinzie, Warreyn, et al., 2022; Duarte et al., 2022; Finkelstein et al., 2021; Huiracocha et al., 2017; Korkow-Moradi et al., 2017; Persons, 2017; Ronca et al., 2019; Sheldon et al., 2021; Steffensen et al., 2022; Watanabe et al., 2021), six were quantitative (Caples et al., 2018; Choi & Van Riper, 2020; Darla & Bhat, 2021; A. Lee et al., 2020; Van Riper et al., 2018, 2021), and one was mixed-methods (E. Y. Lee et al., 2021). Nine of the 19 studies that included an assessment of family adaptation were qualitative (AlJameel et al., 2020; De Clercq, Prinzie, Swerts, et al., 2022; De Clercq, Prinzie, Warreyn, et al., 2022; Duarte et al., 2022; McDonagh et al., 2021; Persons, 2017; Shivers et al., 2019; Steffensen et al., 2022; Watanabe et al., 2021), nine were quantitative (AlJameel & AlKawari, 2021; Caples et al., 2018; Carrada et al., 2019; Choi & Van Riper, 2020; Darla & Bhat, 2021; Ilacqua et al., 2019; Jess et al., 2021; Ljubicic et al., 2020; Pruktarat et al., 2021), and one was mixed-methods (Bertrand, 2019).
Ten of the studies included an assessment of family problem-solving communication and coping. Five of these were quantitative studies (Caples et al., 2018; Choi & Van Riper, 2020; Cless et al., 2017; A. Lee et al., 2020; Pruktarat et al., 2021), four were qualitative (Braga et al., 2021; Duarte et al., 2022; Gashmard et al., 2020; Watanabe et al., 2021), and one was mixed methods (E. Y. Lee et al., 2021).
Examples of How Family System Adaptation Was Assessed Using a Qualitative Approach
In most of the qualitative studies, researchers conducted either unstructured or semi-structured interviews to collect information about adaptation in families of individuals with DS. For example, Clark et al. (2020) conducted in-depth, unstructured interviews with 33 parents of children with DS and nine grandparents of children with DS from the United States in their grounded theory study designed to develop a theory of family sense-making. The initial interview question for this study was, “Starting at the beginning, tell me about how you learned or your child’s (or grandchild’s) condition.” For the study by Braga et al. (2021), semi-structured interviews were conducted with 42 parents from 44 Brazilian families of children with DS between the ages of 1 and 7 years.
Three of the qualitative studies included one or more focus groups. In the study by Huiracocha et al. (2017), a focus group was conducted with eight parents of children with DS to examine the impact of a diagnosis of DS on Ecuadorian families. Then, four interviews were conducted with parents selected on the basis of the distinctly positive attitudes (two interviews) and distinctly negative attitudes (two interviews). Three of these interviews were with the mother alone, and one was with both parents. Eight parents from five families of children with DS living in Thailand held seven self-directed focus group discussions in the study by Persons (2017). In each session, the parents presented genogram drawings about their family. In this study, the researchers were observers, along with a child-development nurse, an occupational nurse, and a special education teacher. Finkelstein et al. (2021) conducted semi-structured interviews, as well as focus groups with 17 Israeli mothers of children with DS.
In the mixed-study by Hart and Neil (2021), concept-mapping methodology was used to obtain caregiver perspectives. Twenty-one parents participated in the telephone interview phase of the study. In addition to answering demographic questions, parents were asked to respond to the following question: “Are parents of individuals with DS supported, why or why not?”
Spontaneous speech samples were collected in two studies with Dutch parents conducted by De Clercq, Prinzie, Swerts, et al. (2022; De Clercq, Prinzie, Warreyn, et al., 2022). The studies are part of a larger, ongoing longitudinal study. In their qualitative study, parent perspectives on raising an adolescent with autism spectrum disorder, cerebral palsy, DS, and no known disability were examined by asking 160 parents (40 per group) to talk spontaneously about what kind of person their child is, how they get along with their child, and their parenting experience. In their mixed-methods study, 5-minute free-speech samples and questionnaire data were gathered from 447 parents of children between the ages of 6 and 17 years who had autism spectrum disorder (N = 159), cerebral palsy (N = 67), DS (N = 54), and without any known disability (N = 167). Parents in this study were asked to speak for five uninterrupted minutes about what kind of person their child is and how they get along together.
Other researchers included open-ended questions in an online survey. For example, in the study by Sheldon et al. (2021), fathers of children with DS living in the United States completed an online survey that included two open-ended questions. The first question was, “What do you find most rewarding about parenting a child with DS?” The second question was, “What do you find most challenging about parenting a child with DS?” In the mixed-methods study by Bertrand (2019), the 369 parents of children with DS living in France who completed an online questionnaire consisting of 25 Likert-type statement were given the option of answering the following two open-ended questions. “What life lessons have you learned from your son or daughter with DS?” “If a couple were expecting to have a child with DS, what would you like to tell them?”
Duarte et al. (2022) conducted a secondary analysis of 42 in-depth, semi-structured interviews from a research project about family and individual adjustment in Brazilian families living with children and adolescents with DS. The aim of this secondary analysis was to explore the spiritual aspects of parenting a child with DS.
Family Measures Used in Quantitative and Mixed-Methods Studies
Table 7 includes a list of the family measures used to assess the concepts of family demands, family appraisal, family resources, family problem-solving and coping, and family adaptation. In addition, Table 7 includes citations for studies that included the measures, as well as how the measure was positioned in the study (e.g., descriptive, correlate, predictor, or outcome).
Measures Used to Assess Key Concepts of the Resilience Model.
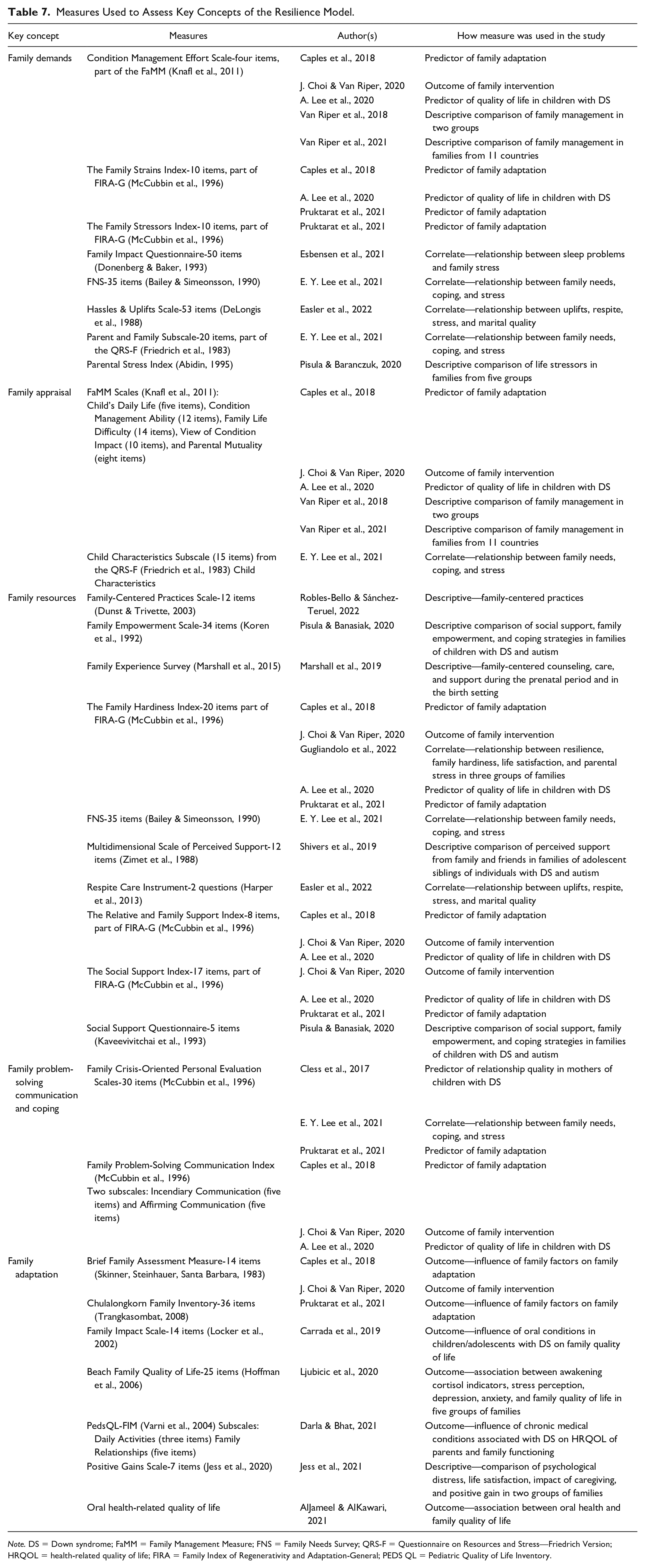
Note. DS = Down syndrome; FaMM = Family Management Measure; FNS = Family Needs Survey; QRS-F = Questionnaire on Resources and Stress—Friedrich Version; HRQOL = health-related quality of life; FIRA = Family Index of Regenerativity and Adaptation-General; PEDS QL = Pediatric Quality of Life Inventory.
Family demands were assessed with a variety of measures including the Condition Management Effort Scale from the Family Management Measure, the Family Strains Index, the Family Stressors Index, the Family Impact Questionnaire, the Family Needs Survey, the Hassles and Uplifts Scale, the Parent and Family Scale of the Questionnaire on Resources and Stress, and the Parental Stress Index. Five scales (Child’s Daily Life, Condition Management Ability, Family Life Difficulty, View of Condition Impact, and Parental Mutuality) from the Family Management Measure were used to assess family appraisal, as well the Child Characteristics Scale from the Questionnaire on Resources and Stress. Three commonly used measures of family resources were the Family Hardiness Index, the Relative and Family Support Index, and the Social Support Index. Other measures used to assess family resources were the Family-Centered Practices Scale, the Family Empowerment Scale, the Family Needs Survey, the Multidimensional Scale of Perceived Support, the Respite Care Instrument, and the Social Support Questionnaire. The Family Problem-Solving Communication Index was used to assess family problem-solving communication. The Family Crisis-Oriented Personal Evaluation Scales was used to assess family coping. Family adaptation was assessed using the Brief Family Assessment Measure, the Chulalongkorn Family Inventory, the Family Impact Scale, the Beach Family Quality of Life Scale, the PedsQL Family Impact Module, the Positive Gains Scale, and the oral health-related quality of life measure.
In terms of how the measures were positioned in the study, in the following four studies (Easler et al., 2022; Esbensen et al., 2022; Gugliandolo et al., 2022; E. Y. Lee et al., 2021), measures were positioned as correlates. There were six studies (Marshall et al., 2019; Pisula & Banasiak, 2020; Robles-Bello & Sánchez-Teruel, 2022; Van Riper et al., 2018, 2021; Shivers et al., 2019) in which measures were used for description or descriptive comparison. In four studies (Caples et al., 2018; Cless et al., 2017; A. Lee et al., 2020; Pruktarat et al., 2021), the measures were positioned as predictors of individual- or family-level adaptation. Seven studies (AlJameel & AlKawari, 2021; Caples et al., 2018; Carrada et al., 2019; Darla & Bhat, 2021; Jess et al., 2021; Ljubicic et al., 2020; Pruktarat et al., 2021) used the measures to assess the impact of other variables on adaptation. The study by J. Choi and Van Riper (2020) is the only study in which measures were used to assess the outcome of a family intervention.
Discussion
This scoping review was conducted to provide an overview of recent research concerning adaptation in families of individuals with DS. One of the strengths of this review is that it was guided by the Resiliency Model of Stress, Adjustment, and Adaptation (McCubbin et al., 1996). As noted earlier, grounding the review in an established family framework provided a structured conceptual approach for examining how interacting family variables shape processes and outcomes associated with family system adaptation in families of individuals with DS. Findings from this review revealed that all five of the key concepts from the Resiliency Model (family demands, family appraisal, family resources, family problem-solving communication, and family adaptation) were assessed in 10 or more of the 41 studies reviewed, with family resources and family demands being the most commonly assessed concepts.
Another strength of this review is that it provides an overview of the wide variety of approaches that have been used to assess family-level adaptation in families of individuals with DS. For example, researchers have conducted unstructured and structured interviews; collected 5-minute free-speech samples; facilitated focus groups; collected both qualitative and quantitative survey data using an online survey; used concept mapping methodology to obtain caregiver perspectives; and conducted a secondary analysis of qualitative data. This review also shows how family measures have been positioned in the studies. That is, was the variable assessed by the family measure considered to be a descriptor, correlate, predictor, or outcome variable? This information can help in the development of future studies concerning adaptation in families of individuals with DS by providing examples of approaches that can be taken and family measures that can be used.
Findings from this review suggest that the shift in focus from negative/problem-focused studies to those focused on strength and resilience has continued. Twenty-six of the 41 studies in this review were categorized as strength and resilience focused. This increased focus on strength and resilience suggests that there is growing recognition among researchers of the need to consider both the positive and negative aspects of having a family member with DS, as well as the need to understand which factors contribute to better outcomes for individuals with DS and their families. Gaining a more accurate understanding of life with DS will help researchers and health care providers develop and implement more effective family-focused interventions. In addition, it can lead to changes in how nursing students and students in other health professions are educated about individuals with DS and their families. For example, rather than focusing solely on the ongoing health and developmental challenges associated with DS listed in their textbooks, students can be given the opportunity to learn directly from individuals with DS and their family members. Having the opportunity to hear an individual with DS or a family member share their story can be enlightening and rewarding.
There has been concerns expressed that by concentrating on adaptation in families of individuals with DS and other conditions associated with an intellectual disability, researchers risk minimizing the socio-political dimensions of this experience (Knight, 2012). Therefore, it is important to note that in addition to examining how families adapt, evolve, and thrive, studies focused on strength and resilience typically include an assessment of family demands and ongoing challenges that increase family stress and/or an assessment of negative outcomes. Also, guiding frameworks for studies focused on strength and resilience usually include an assessment of socio-political dimensions. For example, in the Resiliency Model of Family Stress, Adjustment, and Adaptation (McCubbin et al., 1996), family demands include demands on or in the family system created by socio-political factors such as negative attitudes toward individuals with DS and their families, limited access to support, and poor-quality health care for individuals with DS. The Family Management Style Framework (Knafl et al., 2011, 2021) directs the attention of researchers and health care providers to three primary contextual influences (social network, access to resources, and interchanges with health care and school systems) on family management of chronic conditions.
All studies in this review included some demographic variables. To fully understand family adaptation and factors contributing to better outcomes for individuals with DS and their families, researchers need to gather data on a broad range of demographic variables, as well as data on social determinants of health (SDOH) (i.e., conditions in the environment where people are born, live, learn, work, play, worship, and age that affect a wide variety of health, functioning, and quality) (Kuehnert et al., 2022). While family is not typically identified as an SDOH and no family variables are included in the leading health indicators measuring the outcomes of Healthy People 2030, there is growing recognition that family structures impact and are impacted by SDOHs (Deatrick, 2017; Kuehnert et al., 2022; Russell et al., 2022). Currently there is a need for research addressing how family variables intersect with other SDOH variables to influence adaptation in families of individuals with DS.
Another finding from this review was that there has been an effort to include families of individuals with DS from all over the world, rather than limiting the studies to English-speaking families living in Western countries. Participants for the 41 studies lived in six continents: seven countries in Asia, one country in Africa, 19 countries in Europe, three countries in North America, two countries in South America, and one country in Australia and Oceania. Currently, most of the studies focus on families of individuals with DS from a single country. Country or regional trends were not identified based on sample or methodology. There were only two studies (A. Lee et al., 2020; Van Riper et al., 2021) that included families from more than one country. Moreover, only one of these studies (Van Riper et al., 2021) presented findings for each country, as well as cross-country comparisons of the findings. In the study by Lee et al. (2020), variation in sample size for each country was too large to do cross-country comparisons.
While mothers continue to be the primary respondents in studies of family-level adaptation in families of individuals with DS, there is growing recognition of the importance of including fathers. In the 41 studies included in this review, 77% of the respondents were mothers. However, it is noteworthy that fathers were included in 29 of the studies, and they were the exclusive focus in two of the studies. Unfortunately, in seven of the studies, the researchers did not specify which family member was the respondent. Few studies included multiple family members from the same family.
As with all scoping reviews, there were limitations. This review only included studies published in English language journals. There is also the possibility that we missed relevant publications. However, we minimized this risk by working closely with a research librarian who had expertise in searching electronic databases. This review did not include a quality assessment, but this is consistent with accepted scoping review methods (Arksey & O’Malley, 2005).
Conclusion
This scoping review provides value insights into recent research concerning family-level adaptation in families of individuals with DS. Our results highlight both strengths and gaps in the research. It also offers promising areas for conducting integrative or systematic reviews of study results. In terms of strengths, findings from this review clearly show that there has been a shift from studies that have a negative/problem-based focus to studies with a strength and resilience focus. There has also been greater attention paid to including families from all over the world, rather than just Western countries. In addition, a wide variety of approaches have been used to collect data from families.
In terms of gaps in recent research, there is clearly a need for more longitudinal studies. There is also a need for studies that include not only families from multiple countries but also cross-country comparisons of the findings. In addition, there is a need for researchers to align their family focus and study aims to a conceptual framework. Finally, there is a need for more researchers to expand their sample to include fathers and other family members such as siblings and grandparents, as well consider including multiple family members from the same family.
A promising area for conducting integrative or systematic reviews to build on these findings identifying family system variables would be to examine key findings and outcomes from recent research on family-level adaptation in families of individuals with DS. Another possibility would be to examine the relationship between family variables and quality-of-life outcomes in families of individuals with DS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.