
Abstract
Introduction
Metabolic syndrome (MS) is associated with abnormalities in atrial mechanics, atrial remodeling, and an increased risk of heart rhythm disorders. One of the most commonly used approaches to the prevention of cardiac remodeling in arterial hypertension is the administration of renin–angiotensin system (RAS) inhibitors. Therefore, this study aimed to investigate the effects of RAS inhibitors on atrial mechanics parameters in patients with MS.
Methods and materials
This longitudinal observational study included 55 patients with hypertension and MS, as defined by the ATP III criteria. The patients were evaluated at the start of antihypertensive treatment with an RAS inhibitor. The patients’ clinical characteristics, chosen pharmacological treatment, and transthoracic echocardiography findings were recorded at baseline and 6 months thereafter. A student's dependent sample t-test was used for comparisons between groups. Pearson correlation was used to evaluate the relationships between variables.
Results
Patients with MS had higher peak atrial longitudinal strain (PALS) values at 6 months than at baseline. Meanwhile, systolic strain and peak late strain rates were lower at follow-up than at baseline. The different antihypertensive treatments had comparable effects on the PALS changes during the follow-up period. Higher high-density lipoprotein levels at baseline were correlated with changes in PALS.
Conclusion
The administration of RAS inhibitors improved atrial mechanics parameters in the early stages of antihypertensive management in MS.
Introduction
Metabolic syndrome (MS) captures increased cardiovascular risk and diabetes mellitus, among others. It is often characterized by arterial hypertension, obesity, dyslipidemia, and hyperglycemia.1,2 Recent definitions have noted the significant impact of central obesity on cardiovascular risk. 3
In the last 5–10 years, the risk of developing cardiovascular disease in patients with MS has approximately doubled.1,2 MS is associated with abnormalities in myocardial contractility in patients with coronary disease or cardiac failure. 4 More recently, MS has been associated with abnormal atrial mechanics parameters, including a lower mean strain, strain rate, and early peak strain rate. 5 These changes can lead to atrial remodeling and increased heart rhythm disorder risk. 6
The use of renin–angiotensin system (RAS) inhibitors can help prevent cardiac remodeling and changes in atrial mechanics in patients with arterial hypertension. 7 However, studies that evaluated improvements in these parameters did not include patients with altered atrial mechanics, such as those with MS.8,9 Therefore, this study aimed to investigate the effects of RAS inhibitors on atrial mechanics parameters in MS.
Methods and Materials
Study Design
This longitudinal study included patients with MS and hypertension.
Selection Criteria
Patients were included in this study if they met the following criteria: (1) MS diagnosis based on the ATP III criteria, such as arterial hypertension and at least two of the following characteristics: (i) waist circumference of >103 cm in males or >88 cm in females, (ii) triglyceride levels of ≥150 mg/dL, (iii) high-density lipoprotein (HDL) levels of <40 mg/dL in males and <50 mg/dL in females, and (iv) glucose levels of ≥100 mg/dL 10 ; (2) recent diagnosis with the intended first-line treatment with a RAS inhibitor, either angiotensin II receptor antagonists (ARBs) or angiotensin-converting enzyme inhibitors (iACE); and (3) altered atrial mechanics presenting as: (i) peak atrial longitudinal strain (PALS) of <41%, (ii) early strain rate of <1.6 Seg−1, or (iii) late strain rate of <2.3 Seg−1. 11
Procedures
Patients were evaluated at the start of the antihypertensive treatment. The patients’ clinical characteristics, chosen pharmacological treatment, and transthoracic echocardiography data were recorded, and baseline values were obtained. Subsequent transthoracic echocardiography measurements were performed 6 months later.
Echocardiographic Evaluations
Atrial mechanics parameters were evaluated using the PALS and strain rate curves. Speckle-tracking analysis was performed using Phillips CX50 (Andover, Massachusetts, USA) cardiac ultrasound equipment and a 3.5 MHz transducer with 2-dimensional frozen 2-chamber (2C) and 4-chamber (4C) view images using QLAB-10 software.
Apical 4C and 2C views were recorded using 2-dimensional grayscale. The endocardial border was determined for curve tracing to evaluate the left atrium without considering the mitral annulus, pulmonary veins, or atrial appendages.12–14 The frame rate was set in the range of 60–80 frames per second, as recommended when aiming to achieve temporal resolution with adequate spatial definition and to enhance the feasibility of the frame-to-frame tracking technique. PALS values were the averages of left atrial (LA) segment measurements obtained at the end of the reservoir phase. Curves were drawn to determine strain rates.12–14 The peak systolic strain rate (PSSR), peak early diastolic strain rate (PEDSR), and peak late diastolic strain rate (PLDSR) were measured during ventricular systole, early ventricular diastole, and late ventricular diastole, respectively (Figure 1).

Measurement of PALS from an apical four-chamber view. The software generates curves representing the longitudinal changes in every section, along with a mean curve for all sections, indicative of atrial performance. Meanwhile, during the reservoir stage, the atrium fills up, leading to its expansion. This results in an elevation of the atrial strain, culminating in a positive peak just before the opening of the mitral valve at the conclusion of the filling phase. The dashed curve represents the average atrial longitudinal strain. PSSR is measured during ventricular systole; PEDSR during ventricular early diastole; and PLDSR during ventricular late diastole.
For other echocardiographic evaluations, Simpson's biplane method was used to determine the left ventricular ejection fraction. The Echocardiography European Association of Cardiovascular Imaging criteria were used to assess diastolic dysfunction. 15 Left ventricular and LA volumes were obtained from apical 4C and 2C views. The dimensions were indexed to body surface area according to the recommendations of the American Society of Echocardiography. 15 LA volumes were calculated during the cardiac cycle and indexed to the body surface area using the biplane area-length method at 3 different points: (1) maximum volume before MV opening (LAmax), (2) minimum volume before MV closure (LAmin), and (3) volume before LA contraction at the onset of the P wave (LApreA).12–14
Laboratory
Blood samples were drawn after an overnight fast. Plasma levels of total cholesterol, HDL cholesterol, low-density lipoprotein cholesterol, trigglycerides, and fasting blood glucose were measured using standard laboratory techniques.
Statistical Analysis
Continuous variables are expressed as mean and standard deviation and categorical variables are expressed as frequencies (%). A student's t-test was used to compare dependent samples. Correlation analysis was performed using Pearson's test. Statistical significance was set at p-values of ≤.05. Data analysis was performed with IBM SPSS Statistics software [version 28.0.1.1]. Graphs were generated using GraphPad Prism 9.
Ethical Approval and Consent
This study was approved by the Ethics Research and Biosafety Committee of the University Center of Health Sciences, University of Guadalajara (CI-00922). This study adhered to the principles of the Declaration of Helsinki.
Results
This study included 55 (51% female) patients with a mean age of 58 ± 10 years. Overall, 100%, 89.1%, 36.4%, 85.5%, and 36.4% of the patients had hypertension, elevated waist circumference, hypertriglyceridemia, low HDL levels, and glucose levels of >100 mg/dL, respectively. The prevalence rates of smoking and ethylism in the study population were 32% and 36.4%, respectively.
All patients (100%) were taking antihypertensive drugs, and most (72.7%) used ARBs. The most frequently used drugs were losartan (41.8%), candesartan (10.9%), valsartan (9.1%), and telmisartan (9.1%). In addition, iACEs were used by 27.3% of the patients; enalapril (21.8%) was the most frequently used iACE (Table 1).
Baseline characteristics of patients with metabolic syndrome.
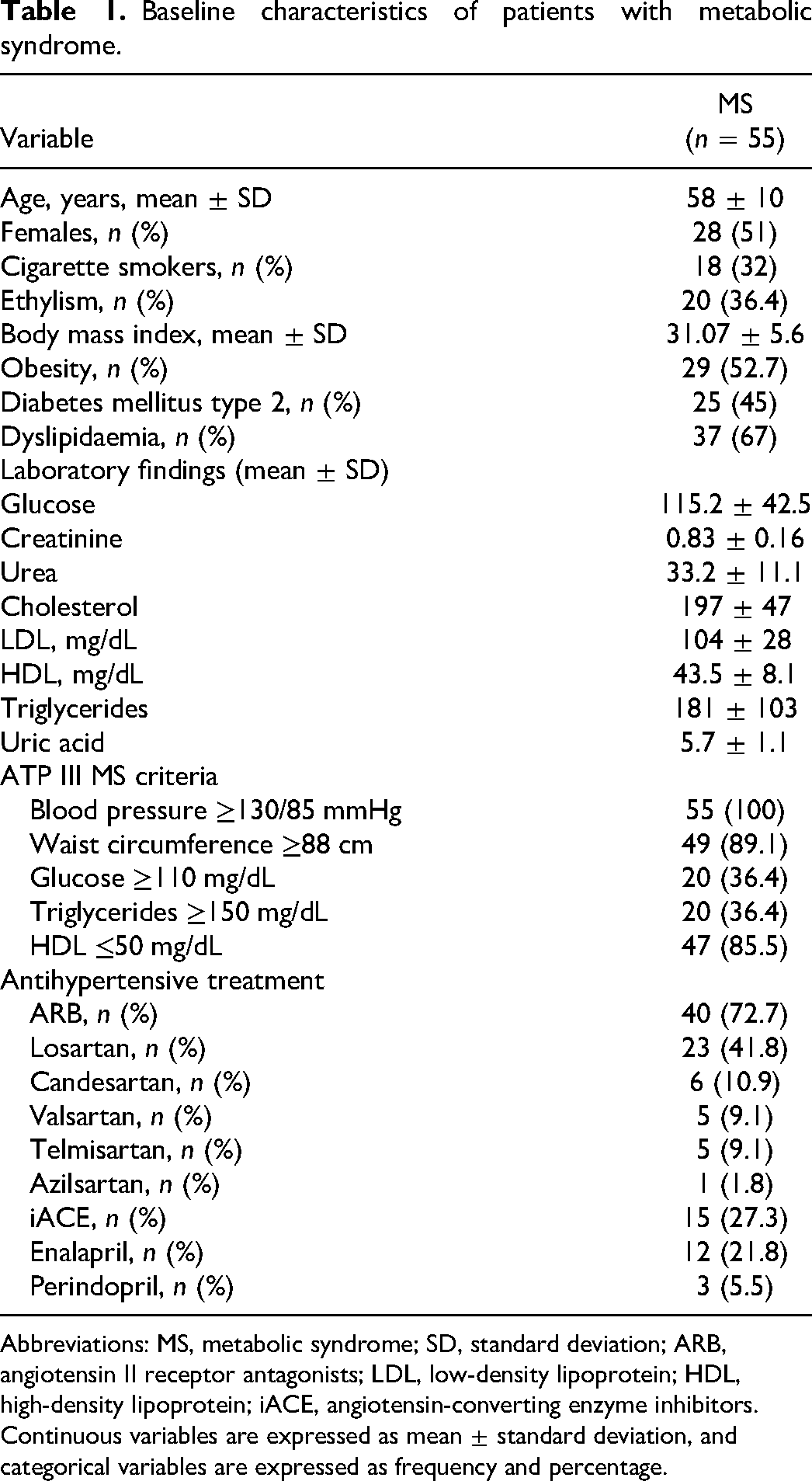
Abbreviations: MS, metabolic syndrome; SD, standard deviation; ARB, angiotensin II receptor antagonists; LDL, low-density lipoprotein; HDL, high-density lipoprotein; iACE, angiotensin-converting enzyme inhibitors.
Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as frequency and percentage.
At baseline, all patients presented abnormal PALS with a mean value of 30.27 ± 6.79, a systolic strain rate of 1.75 ± 0.39, an early strain rate of −1.88 ± 0.74, and a late strain rate of −2.09 ± 0.54. These parameters changed during the follow-up period. The PALS values were higher at the 6-month assessment than at baseline; meanwhile, systolic strain rates were lower. Finally, early and late strain rates remained stable.
Significant improvements were identified in systolic pulmonary arterial pressure (sPAP), LA anteroposterior (AP) diameter, 4C area, 2C area, LA volume indexed, LA volume, LA maximum volume, LA minimum volume, pre-A volume, LA conduction function, LA pump function, and reservoir function (Table 2).
Changes in the echocardiographic characteristics of patients with metabolic syndrome.

Abbreviations: LA, left atrial; sPAP, systolic pulmonary arterial pressure; LA AP, left atrial anteroposterior; LAVI, LA volume indexed to bovine serum albumin (mL/m2); SD, standard deviation.; 4C, 4-chamber; 2C, 2-chamber.
Continuous variables are expressed as the mean and standard deviation and are categorical in frequency and percentage. A student’s t-test was used for comparisons of dependent samples.
Changes in atrial mechanics were observed after 6 months of treatment in patients with MS who commenced therapy with altered PALS (Figure 2). Different antihypertensive treatments were compared, and no differences were identified between the PALS changes during the follow-up period (Figure 3).

Comparison of atrial mechanical parameters in patients with metabolic syndrome. Variables were expressed as mean and standard deviation. The student t-test for dependent samples was used. (a) PALS at baseline was 30.27 ± 6.7 and 6 months at baseline and 31.04 ± 6.6 at 6 months. (b) PSSR 1.75 ± 0.39 at baseline and follow-up (6 months) 1.64 ± 0.37. (c) PEDSR −1.88 ± 0.73 at baseline and follow-up (6 months) −1.86 ± 0.52. (d) PLDSR at baseline and −1.89 ± 0.67 at follow-up (6 months).

Comparison of change in peak atrial longitudinal strain into antihypertensive drugs. Values of change in peak atrial longitudinal strain are presented in medians and ranges. The student t-test for dependent samples was used for comparison between groups.
The correlation analysis showed that the higher the baseline HDL level, the greater the PALS change. No significant differences were observed between PSSR, peak early strain rate, or peak late strain rate values at baseline and changes in the PALS score (Table 3).
Correlation of variables with the value change in PALS.

Abbreviations: PALS, peak atrial longitudinal strain; SD, standard deviation; BMI, body mass index; WHR, waist-to-hip ratio; PSSR, peak systolic strain rate; PEDSR, peak early diastolic strain rate; PLDSR, peak late diastolic strain rate; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Pearson's correlation analysis was performed. Statistical significance was set at p ≤ .05.
Discussion
This study identified modifications in atrial mechanics parameters in patients with MS who received pharmacological treatment with RAS inhibitors. In addition, this study observed that medium-term antihypertensive treatment could generate significant changes in LA strain parameters.
MS comprises several cardiovascular risk factors that affect atrial mechanics. 5 Gomez observed alterations in LA mechanical parameters in patients with MS. This group of patients had a strain reservoir of 23.8 ± 6.7%, strain in the conduction phase of 10 ± 3.8%, and strain in the contraction phase of 10 ± 3.8%. 16 Fang et al 5 evaluated the effect of MS on LA mechanics. In their study, patients with MS had lower average strain levels (19.31 ± 4.78 vs 27.89 ± 5.11, p < .001), and lower systolic strain (1.12 ± 0.030 vs 1.56 ± 0.29, p < .001), and early peak strain (−0.97 ± 0.30 vs −1.6 ± 0.42, p < .001) rates compared to the control group.
PALS during the reservoir phase is a new and important predictor of cardiovascular events that measure the degree of atrial stiffness, which indicates abnormal heart rhythm risk. PALS may be superior to traditional parameters used in LA analysis. 17
Nevertheless, very few studies have evaluated the increase in PALS in patients with new-onset treatment of hypertension. For example, Kokubu et al 9 included 80 patients with hypertension and 50 controls. They performed 2-dimensional color tissue Doppler ultrasound studies to evaluate atrial mechanical parameters. They observed that 46% of the evaluated patients had received drugs that acted on the RAS for at least 2 weeks before the test. This study found that patients with a dilated LA who received antihypertensive treatment with RAS inhibitors had lower peak systolic strain rates than those without a dilated atrium or treatment with renin–angiotensin blockers. 9 This study suggests a significant impact of RAS blockade on atrial mechanical parameters. 9 Dimitroula et al 8 evaluated a sample of patients who had previously received antihypertensive treatment. In the present study, patients commenced therapy with an iACE or ARB and were followed up using Doppler echocardiography. This study observed that patients had a higher peak LA strain (77.8 ± 5.2% vs 63.3 ± 4.1%, p < 0.001) and peak LA strain rate (3.9 ± 0.2 s−1 vs 3.1 ± 0.2 s−1) 9 months after commencing treatment. 8 Although this study shows some evidence of the therapeutic efficacy of drugs acting on the renin–angiotensin pathway in this patient group, the validity of these findings may be limited by the heterogeneity of strain percentage values at baseline (10%–125% of the peak LA strain, n = 40). In contrast, the percentages ranged from 25% to 150% at the 6-month follow-up. 8
This is the first study to evaluate the pharmacological effects of RAS inhibitors in patients with MS and altered PALS. This study only included patients with an altered PALS of <41%, which is the limit of normality established by Sugimoto et al. 11 Importantly, this study compared the outcomes of patients who were administered different RAS inhibitors. The different types of antihypertensive drugs evaluated seemed to have comparable outcomes.
This study has some limitations. First, the follow-up period was short and may have been insufficient to observe changes in atrial mechanics parameters. Second, the sample size was small; larger studies are required to validate these findings.
This is the first study to highlight the impact of antihypertensive treatments with RAS inhibitors in patients with MS and altered longitudinal strain. This study used speckle-tracking ultrasound, which is a reliable method of evaluating myocardial deformation. This technique reduces the influence of observer judgment and observation angle, allowing for a reliable evaluation of preclinical cardiac conditions. 18
Conclusion
MS is associated with early changes in atrial mechanics, which occur even before evidence of atrial remodeling can be observed. In this study, the use of RAS inhibitors improved atrial mechanics parameters already in the early stages of treatment.
Furthermore, this study showed the benefits of RAS inhibitor treatment on atrial mechanics parameters in patients with high cardiovascular risk. These findings can help optimize the management of patients with MS, thereby improving their prognosis and cardiovascular outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Juan A. Peraza-Zaldivar was a recipient of a scholarship from the Consejo Nacional de Ciencia y Tecnología (CONACYT).