
Abstract
Purpose:
Examine patterns of medication use, changes in medication patterns over time, and investigate factors associated with medication patterns among older Australian women with Atrial Fibrillation (AF).
Methods:
It is a retrospective analysis of the 1921-26 birth cohort of the Australian Longitudinal Study on Women’s Health (ALSWH), diagnosed with AF between 2000-2015 (N = 1206). Survey data of these women was linked with national registries for medications and death. Latent Transition Analysis (LTA) identified distinct patterns of medication use and transitions among these patterns for 3 consecutive years following AF diagnosis. LTA with co-variates determined the factors associated with latent status membership.
Results:
One-tenth (9.6%, 11.7%, 11.4%) of the study population did not receive any medication for AF in all 3 years following AF diagnosis and about 60% did not receive any medication for the prevention of thromboembolism. Among those who received medications, almost three-quarters (76.6%, 68.4%, 68.5%) received some kind of combination of medications. LTA indicated at least 6 different patterns of AF medications. These patterns had transition probabilities >85% for most of the latent statuses. All factors but diabetes mellitus among the CHA2DS2-VA scoring scheme were independently associated with latent status membership at the time of AF diagnosis.
Conclusions:
Evaluation of pharmacological treatment indicates that prevention of thromboembolism is inadequate among women with AF. There exists wide variations in medication patterns. However, once in a particular pattern, women are likely to continue the same medications long-term. This underscores the importance of initial assessment of patient profile and stroke risk score in determining the treatment for AF. Failure to assess risk makes women susceptible to devastating AF complications.
Keywords
Introduction
Globally, Atrial Fibrillation (AF) is the most common cardiac arrhythmia. Prevalence of AF is age dependent and increases with advancing age. 1 In people younger than 40, AF prevalence is less than 1%, 1 rising up to 20-25% among those aged 80 years and above. 2 -4 With the changes in population demographics and improved longevity, AF is considered an emerging epidemic and a major public health challenge. 5 Literature suggests that AF is independently associated with a number of health impacts, such as reduced quality of life, 6 increased risk of embolic stroke, 1,7 and premature death. 1,7 -9
Treatment of AF involves careful assessment of risks and other comorbidities and involves two major decisions - rate or rhythm control, and initiation of anticoagulation therapy to prevent stroke. CHA2DS2-VASc (Congestive heart failure, Hypertension, Age 65-74, Diabetes, Stroke or TIA, Vascular disease, Age ≥ 75 years and Sex[female]) score is the most widely used scoring scheme to calculate the risk of stroke among AF patients. 10 It is recommended that a score of one or more for men, and two or more for women indicates high risk of stroke and patients be treated with anticoagulants. However, the 2018 Australian guidelines, 11 recommend the use of the risk-prediction model CHA2DS2-VA (sexless version of CHA2DS2-VASc recommending same threshold for both genders) to guide decisions about anticoagulation treatment. 11 Literature, however, indicates that medication use does not correlate well with the stroke risk. 12 Rather, the use of anticoagulant decreases with increasing stroke risk especially among women and older patients. 13
Women with AF are particularly at increased risk of AF complications such as stroke and death compared to men. 7,9 However, despite improvements in the overall trends of medication uptake, treatment among women is less aggressive and less effective 14 leading to increased complications and consequences related to AF. Sabouret et al. 15 confirms that women < 75 years were 17 times less likely to receive antithrombotic treatment compared to men. This is doubled to 34% in women ≥ 75 years of age. With age associated increased risks, there is a need to understand this potential for under treatment of older women with AF particularly for ones in their 80s and 90s.
To the best of our knowledge, there are no studies to date of the long term use of AF medication among octa- and nonagenarian women in Australia or elsewhere. This study therefore aims to explore the medication use for AF among older women. Specific objectives include understanding the medication use for AF among older Australian women, investigating the distinct patterns of AF medications over time, and examining factors associated with these identified medication patterns.
Methods
Study Population and Datasets
The study is based on the data from the oldest cohort (born 1921-26) of the Australian Longitudinal Study of Women’s Health (ALSWH, www.alswh.org.au). ALSWH is a prospective, longitudinal cohort study examining the socio-demographic and lifestyle factors over the life course which affect the physical and mental health of women and their use of health services. In 1996, this cohort of women participated in the first survey (N = 12432) and were regularly surveyed every 3 years thereafter until 2011, returning self-completed comprehensive paper questionnaires. Since 2011, due to the age of the participants, a shortened survey continues to be sent to participants every 6 months. Further details about the ALWSH are reported elsewhere. 16
AF was determined using linked state-based hospital data from New South Wales (NSW), Queensland (QLD), Western Australia (WA), South Australia (SA) and the Australian Capital Territory (ACT), during the period from 2000 to 2015. Previously, 1827 women from this cohort were identified as having AF based on the hospital records, using ICD-10-AM (I48, I48.0, I48.1, I48.2 and I48.9) codes. 17 Details of the AF identification process is reported in another paper. 2
Eligibility for the Analysis
Among 1827 women previously identified with AF, 1206 women were eligible for the current analysis. Women were included in the analysis if they: i) consented for Pharmaceutical Benefit Scheme (PBS) 18 data linkage, and ii) were alive for at least 30 months after first hospital reported diagnosis of AF to ensure assessment of medication use for at least 3 years post AF diagnosis (Year1 [T1], Year2 [T2], Year3 [T3]). The main reason for exclusion from the current analysis was death within 30 months of first AF diagnosis (n = 620 women), with only 1 woman who did not consent to PBS data linkage.
AF medication data for all eligible women was obtained through PBS data linked with ALSWH participants. The PBS is an administrative dataset initiated to monitor prescription medicines in Australia and is available for ALSWH participants from 2000-2018. Using Anatomical Therapeutic Chemical (ATC) 19 codes, AF medications use was evaluated for each subsequent year following the first reported diagnosis of AF for 3 consecutive years. (Details of the AF medications and corresponding ATC codes are presented in Supplementary Table S1.) Yearly medication use for all identified ATC codes was considered positive if at least one PBS record indicated dispensing of that medication. All medications were initially classified into 6 categories: 1) Rate Control (RC); 2) Rhythm Control (RyC); 3) Vitamin K Inhibitors (VKI); 4) Platelet-aggregation Inhibitors (PAI); 5) Direct Thrombin Inhibitors; and 6) Factor Xa Inhibitors. Categories 5 and 6 were later merged for analysis due to low prevalence of these drugs in the study population and were labeled as Non-Vitamin K Antagonist Oral Anticoagulants (NOACs).
Medication Use and Time Period for Ascertainment
Medication use for each category was defined dichotomously (yes/no), and was calculated for 3 consecutive years. The 3 year time periods were calculated as 12 (T1), 24 (T2) and 36 (T3) months from the date of first reported AF diagnosis in hospital data. Medication use was considered positive for a given category per year if a woman had at least one record of medication in that category during that year.
Statistical Analysis
Descriptive statistics were used to describe study participants under 4 domains: (i) demographics; (ii) health behaviors; (iii) access to health care services; and (iv) self-reported co-morbid conditions. Variables under these domains are described in supplementary Table S2. Data on these variables were obtained from ALSWH Survey 3 conducted in 2002, corresponding to the earliest available linked hospital data for most states. These were considered as baseline characteristics of the study population. Missing data were filled in from Survey 2 (1999), initially, and then from Survey 1 if necessary.
Prevalence of AF medication use
Prevalence of AF medication use was assessed for each year following AF diagnosis based on the drug categories and the total number of drug categories used by AF women simultaneously in a year.
Latent transition analysis (LTA)
Latent Transition analysis (LTA) was applied to identify underlying patterns of AF medication use among older women in Australia and to understand how they change over time for at least 3 years after AF diagnosis. LTA is an extension of Latent Class Analysis (LCA). 20 In addition to identifying mutually exclusive latent statuses, known as latent classes in LCA, LTA also allows the estimation of the incidence of transition among these latent statuses from one time point to the next, conditional on the latent status membership at the previous time point. The analysis was conducted for a range of latent statuses from 2 to 9. The iterative model building process was stopped when the fit indices showed no further improvement. Model selection was based on parsimony, model interpretability, and information criteria (Bayesian Information Criterion (BIC) and Akaike Information Criterion (AIC), for which lower scores represent better fitting models).
Following model selection, 3 sets of parameters were calculated for each latent status: latent status prevalence, gamma (
All statistical analysis were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
Ethical Approval
The ALSWH project has ongoing ethical clearance from both the University of Newcastle (UoN) and University of Queensland’s (UQ) Human Research Ethics Committees (HREC) [HREC UoN no.: H-076-0795 & HREC UQ no. 2004000224]. This project has been approved by the Data Access Committee of ALSWH, registered as Project A685.
Results
Baseline Characteristics
Most women lived either in major cities or regional areas at baseline with only 2% of women living in remote Australia, and 42% were married or partnered at the time of survey with another 56% previously married or partnered (Table 1). More than three quarters of all women reported having excellent access to hospital (87%) and General Practitioners (GPs). A quarter of women reported difficulty managing on their available income. The 3 most common comorbidities included hypertension (HTN, 53%), cancer (52%, includes skin cancers) and arthritis (47%). Less than 5% of women reported being a current smoker, with a similar proportion reporting high risk alcohol consumption. More than half of the women had a BMI which was overweight or obese (54%) with 42% of women reporting a sedentary lifestyle (defined as 0-10 minutes of moderate physical activity per week). At the time of first reported AF diagnosis, all women were aged 75 years or older (range 75-94).
Baseline Characteristics of Older Australian Women (Born 1921-26) Who Were Identified With Atrial Fibrillation Between 2000 to 2015 (N = 1206).

Use of Medication
Despite strong recommendation for initiation of medication for prevention of thromboembolism among women ≥ 75 years with AF (using the CHA2DS2-VA or CHA2DS2-VASc scoring schemes), only 44% of women received any mediation for stroke prevention and a further ∼10% did not receive any medication for AF during the first year post-diagnosis (Table 2).
Prevalence of Atrial Fibrillation Medications Among Older Australian Women (Born 1921-26, N = 1206) for 3 Consecutive Years Following First Diagnosis of Atrial Fibrillation.
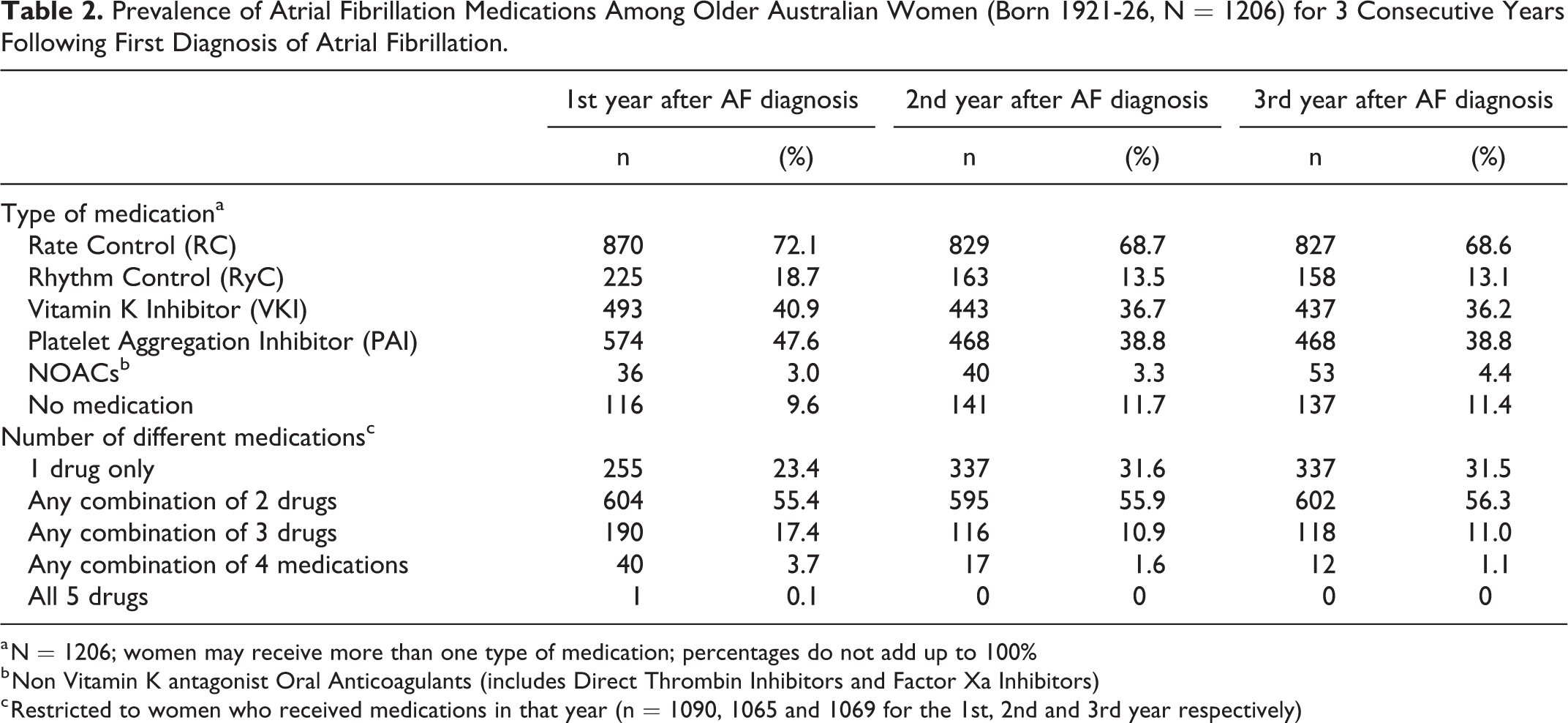
a N = 1206; women may receive more than one type of medication; percentages do not add up to 100%
b Non Vitamin K antagonist Oral Anticoagulants (includes Direct Thrombin Inhibitors and Factor Xa Inhibitors)
c Restricted to women who received medications in that year (n = 1090, 1065 and 1069 for the 1st, 2nd and 3rd year respectively)
Among women who received any type of medication (Table 2), the majority received some combination of medications. The majority of women (55%) received a combination of 2 medications, this prevalence remained stable across all 3 years. The prevalence of women with one type of AF medication increased from 23% to 31% from T2 to T3. In the first year, 17% of women used 3 different types of AF medication although this decreased to 11% for the second and third years. Very few women used 4 types of medications; the prevalence decreased from 4% in the first year to 1% in the third year.
Latent Transition Analysis
Model selection for number of statuses
Latent transition analysis was performed to further understand the medication combinations and change in these medication patterns over time. Latent statuses were identified based on the observed use of AF medications, e.g. RC, RyC, PAI, VKI, and NOACs, in each of the 3 years following AF diagnosis. Based on model selection criteria of parsimony, model interpretability and the information criteria, a model with 6 latent statuses was selected as the optimal model (Supplementary Table S3). It indicates that AIC and BIC both declined through to the 6 status model. At the seventh status, the AIC continued to decline but the BIC rose. Thus, AIC points to a 7 status model and BIC points to a 6 status model. However, the 6 class model was chosen after careful analysis of latent class separation, as it was more parsimonious, while being conceptually interpretable and more clinically relevant.
Latent status prevalence
Following careful review of the item response probabilities (Table 3), labels were assigned to the latent statuses: 1) Low medications; 2) Rate Control only (RC only); 3) Platelet-aggregation Inhibitors only (PAI only); 4) Rate Control with Platelet-aggregation Inhibitors (RC with PAI); 5) Rate Control with Vitamin K inhibitors (RC with VKI); and 6) Rate, Rhythm and Platelet-aggregation Inhibitors (RC, RyC with PAI). For each time period,
Six Latent Status Model of AF Medications Use for 3 Consecutive Years of Older Australian Women Were Identified With Atrial Fibrillation Between 2000 to 2015 (N = 1206).

* Item response probabilities constrained equal across times
Item response probabilities ≥ .5 are in bold to facilitate interpretation
RC = Rate Control, PAI = Platelet Aggregation Inhibitor, VKI = Vitamin K Inhibitor, RyC = Rhythm Control.
Measurement invariance
Hypothesis testing for equality of item response probabilities across time points indicated that differences (either qualitative or quantitative) exist between the latent statuses across times (Supplementary Table S4). Item response probability patterns were visually assessed for all 3 time points and were found to be similar for all latent statuses except for minor difference in latent status 6
Transition probabilities
Table 4 shows transition probability matrix. It indicates that despite some movement between latent statuses, in general a woman’s most likely latent status at T2 was her latent status membership at T1. Women in
Transition Probabilities for 6 Class Model for AF Medication Patterns Among Older Australian Women Who Were Identified With Atrial Fibrillation Between 2000 to 2015 (N = 1206).

RC = Rate Control, PAI = Platelet-aggregation Inhibitor, VKI = Vitamin K Inhibitor, RyC = Rhythm Control.
LTA with covariates
We used individual factors from the CHA2DS2-VA score (Congestive heart failure, Hypertension, Age > 65-74 years, Diabetes mellitus, Stroke or TIA and Vascular disease) as covariates to predict latent status membership at T1. All variables were dichotomous, with the exception of age. Age was taken to be “age at diagnosis,” and was a continuous variable which was standardized. The latent status
Predictors of Membership (Expressed as Odds Ratios) in Time1 Latent Statuses of AF Medication Patterns Among Older Australian Women Who Were Identified With Atrial Fibrillation Between 2000 to 2015 (N = 1206).

RC = Rate Control, PAI = Platelet Aggregation Inhibitor, VKI = Vitamin K Inhibitor, RyC = Rhythm Control.
Odds ratios generated using Latent Transition Analysis including covariates.
Discussion
To the best of our knowledge, this is the first population based study into understanding the medication patterns among older women with AF, both globally and in Australia. Our study indicates there is low use of medications for prevention of thromboembolic events among older AF patients. Only 40% of women in our study population were either on
Our study also indicates that there are wide variations with respect to management of AF. There were 6 distinct patterns of AF medication use ranging from
About two thirds of the women were using a combination of 2 or 3 medications. For instance
Another interesting finding was that a history of diabetes does not play a role in the decision making for the medication prescription for AF among women. All other individual factors from CHA2DS2VA score were associated with latent status membership.
Strengths and weakness
This is the first population-based study to understand the medication pattern for AF among older women. This study did not investigate medication dosage, monitoring of coagulation status or the type of health care provider, reflecting limitations of the provided linked administrative medication data. We acknowledge that our study had a low prevalence of NOACs due to the time frame of the study. NOACs were approved around 2013 for use among AF patients for the prevention of thromboembolism and their uptake took another couple of years. We are unsure if the low prevalence of NOACs in our study is due to the delayed approval of the medication or because of a lack of studies about the efficacy of these medications among older age groups. This study included women who lived for at least 30 months after the first AF diagnosis report in the hospital data. Though this is considered as a selection bias to include women who were relatively less sick but it was performed to evaluate the longitudinal use of AF medication.
Conclusion
Despite the high risk of stroke among older women with AF, less than half are treated for the prevention of thromboembolism. This makes them at high risk of stroke with devastating consequences or disability further affecting their quality of life. More awareness and education for clinicians might further help in reducing this gap.
Supplemental Material
Supplemental Material, Supplementary_Material_for_Patterns_of_AF_Medications - Patterns of Medications for Atrial Fibrillation Among Older Women: Results From the Australian Longitudinal Study on Women’s Health
Supplemental Material, Supplementary_Material_for_Patterns_of_AF_Medications for Patterns of Medications for Atrial Fibrillation Among Older Women: Results From the Australian Longitudinal Study on Women’s Health by Shazia Shehzad Abbas, Tazeen Majeed, Balakrishnan R. Nair, Peta M. Forder, M. Biostatistics, Natasha Weaver and Julie E. Byles in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Authors’ Note
Acknowledgments
The research on which this study is based was conducted as part of the Australian Longitudinal Study on Women’s Health by University of Queensland and the University of Newcastle. We are grateful to the Australian Government Department of Health for funding and to the women who provided the survey data. The authors acknowledge the assistance of the Data Linkage Unit at the Australian Institute of Health and Welfare (AIHW) for undertaking the data linkage to the National Death Index (NDI). The authors also acknowledge the following: Centre for Health Record Linkage (CHeReL), NSW Ministry of Health and ACT Health, for the NSW Admitted Patients Data Collection, and the ACT Admitted Patient Care Data Collection; Queensland Health, including the Statistical Services Branch, for the Qld Hospital Admitted Patient Data Collection; Department of Health Western Australia, including the Data Linkage Branch, for the WA Hospital Morbidity Data Collection; SA NT Datalink, and SA Health for the SA Public Hospital Separations Data Collection. The authors acknowledge the Department of Health and Medicare Australia for providing MBS and PBS data, and the Australian Institute of Health and Welfare (AIHW) as the integrating authority.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.