
Abstract
In recent months, the new coronavirus SARS-CoV-2 has emerged as a worldwide threat with about 4.2 million confirmed cases and almost 300 000 deaths. Its major clinical presentation is characterized by respiratory symptoms ranging from mild cough to serve pneumonia with fever and potentially even death. Until today, there is no known medication to improve clinical symptoms or even prevent or fight the infection. The search for a useful vaccination is ongoing and it will probably not be available before the end of 2020. In this review, we highlight hydroxychloroquine (HCQ) as a potential agent to prevent coronavirus disease 2019 (COVID-19) and reduce as well as shorten clinical symptoms. Moreover, it might serve as a potential post-exposition prophylaxis. Although it has been used in the treatment of rheumatoid arthritis, discoid or systemic lupus erythematosus, and malaria prophylaxis and therapy for decades, knowledge on HCQ as a potential treatment for COVID-19 is limited and multiple clinical trials have just emerged. Especially, rare HCQ side effects which were of minor importance for use in selected indications might gain major relevance with population-wide application. These rare side effects include retinopathy and—even more important—QT prolongation leading to sudden cardiac death by malignant arrhythmias.
Introduction
Coronavirus SARS-CoV-2 is a single-stranded positive-sense RNA virus of the β coronavirus family, which causes infections of the lower respiratory tract with fever, cough, and dyspnea, potentially leading to acute respiratory distress syndrome and death. 1 The recent worldwide outbreak of coronavirus disease 2019 (COVID-19) has led to a vast amount of clinical trials in the search of potential therapeutic strategies to prevent and fight the disease. The most prominent agent is probably hydroxychloroquine (HCQ), which is an approved medication in the treatment of rheumatoid arthritis and discoid or systemic lupus erythematosus as well as a prophylaxis and therapy for malaria infections. Due to its clinical use since 1955, it is largely available and side effects are known. However, previously limited indications in combination with very rare side effects, such as malignant arrhythmias caused by QT prolongation, might potentially underestimate the risk of a general use to fight COVID-19.
Despite promising in vitro data, previous reports on HCQ to reduce viral infection rates as well as first retrospective analyses from COVID-19 patient registries, dosage, and side effects in a scenario of a population-wide application are largely unknown and require further investigation. In this review, we provide an overview about the potential pharmacological mode of action, previous and ongoing studies on treating COVID-19 by HCQ, and for pre- or post-exposition prophylaxis. We will conclude with a critical discussion about potential benefits versus proarrhythmia as a lethal side effect of HCQ treatment.
Hydroxychloroquine Reduces Viral Uptake and Modulates Immune Response
Several investigations in recent years have shown that chloroquine (CQ) and HCQ are capable of reducing cellular infection rates in vitro as broad-spectrum antiviral drugs with implications in prophylactic and therapeutic use. 2 -4 These observations have now been confirmed for COVID-19, and most results initially evaluated for CQ were adapted to HCQ due to better availability as well as lower toxicity. 5 -7 Chloroquine/HCQ enter the cell and accumulate in endosomes, lysosomes, and Golgi vesicles. They increase endosomal pH in a dose-dependent manner, which inhibits spike protein-mediated viral entry and lysosomal activity and decreases autophagosome–lysosome fusion. 8 -11 Alkalization of cell vesicles also modulates the immune response (reduced tumor necrosis factor α and interleukin 6 secretion) and viral replication by impairing protein translation and posttranslational modifications in the Golgi apparatus. 2,12 -14 Hydroxychloroquine alters the glycosylation of surface receptors utilized by Sars-CoV-2 for cellular infection such as the ACE2 receptor. 4,15 Furthermore, HCQ interferes with Toll-like receptor (TLR) signaling by pH-dependent changes in TLR7 and TLR9 processing as well as direct binding to nucleic acids. Similar immunomodulatory effects have been associated with altered ligand binding to cyclic GMP-AMP synthase, both part of signaling pathways which promote transcription of pro-inflammatory cytokines 16 -18 (Figure 1).

Hydroxychloroquine (HCQ)-associated mechanisms to prevent COVID-19. A, Sars-CoV-2 enters type 2 pneumocytes via the ACE2 receptor which is either modified by N-glycosylation in the endoplasmic reticulum or Golgi apparatus. Accumulation of chloroquine (CQ)/HCQ alters glycosylation of the Golgi-modified ACE2 receptor which impacts spike protein S-mediated viral entry. B, Chloroquine/HCQ accumulates in cell vesicles, for example, phagolysosomes, which leads to endosomal alkalization. Increased pH impairs phagosomal–lysosomal fusion and reduces lysosomal enzyme activity. C, Immunoreactive signaling cascades that promote transcription of pro-inflammatory cytokines are mediated by Toll-like receptor (TLR) signaling. Chloroquine/HCQ suppresses this pathway via increasing the endosomal pH and reduced binding of TLR to nucleic acids.
Hydroxychloroquine in First Clinical Trials to Fight COVID-19
Besides a small number of case series, there are 3 controlled trials on HCQ to treat COVID-19 so far: The first trial on HCQ as a therapeutic approach for polymerase chain reaction (PCR)-confirmed COVID-19 was a randomized, open-label study on 30 patients in Shanghai. 19 Hydroxychloroquine was used in a dose of 200 mg twice daily for 5 days versus a control cohort with conventional treatment. Both groups were PCR negative on day 4 and free of fever after the first day. No significant differences were observed among the 2 groups—a fact that is most likely due to limited sample sizes. 19
In a subsequent French study, 36 PCR-positive patients were nonrandomly divided into 3 groups, either treated with HCQ (n = 14), HCQ plus Azithromycin (n = 6), or supportive therapy only (n = 16). Having in mind that the group sizes were very limited again and significant differences in baseline characteristics were observed concerning age and clinical status, the authors detected a significant improvement in the duration of PCR virus detection under HCQ therapy and even more pronounced when HCQ was combined with Azithromycin. 20
A third clinical trial comprised the largest group of patients (n = 62) who were randomized to HCQ 200 mg twice daily for 5 days versus conventional therapy. Hydroxychloroquine shortened the time of fever or cough from 3 to 2 days. A progression to severe illness was only observed in the control group in 4 of 31 cases and did not occur under HCQ therapy. In line with this, CT scans on day 0 compared to day 6 provided evidence for exacerbation in 29% in the control group versus 6.5% under HCQ therapy. Improvement was detected in 54.8% (38.7% moderate; 16.1% significant) under conventional therapy versus 80.6% (19.4% moderate; 61.3% significant) under HCQ treatment. 21 Reported side effects in the abovementioned trials included gastrointestinal symptoms, elevated liver enzymes, rash, and headache. 19 -21
Larger Trials Are Needed for Safety and Efficacy Evaluation
The abovementioned controlled trails include only 128 patients in total and have a very short observation period. This limits any robust conclusion from these studies. Still, HCQ seems to be a promising therapeutic agent to successfully treat COVID-19. Rare side effects as stated above can most likely not be sufficiently detected with these small case numbers. Therefore, a plethora of larger trials for pre- and post-exposition prophylaxis as well as for the treatment of PCR-positive cases are currently running (Figure 2A and B).

Hydroxychloroquine (HCQ) for COVID-19 treatment—a trial overview. A, Depicted are estimated patient numbers for HCQ trials to fight COVID-19. B, Time scale to illustrate the planned study duration for different HCQ trials. Therapy trials are shown in black, pre-exposition (PreEP) trials on mainly health care workers are green, and post-exposition (PEP) trials are red.
In search of an appropriate HCQ treatment regimen, a relatively large variation with respect to duration and dosage can be observed (Figure 3A and B). Physiologically based pharmacokinetic models use mathematical modeling techniques to predict drug concentrations in human tissues. For HCQ in the lung, different dosing regimens were calculated. Interestingly, there was no significant difference between the once- or twice-daily application of the maintenance therapy. The authors suggested to apply the HCQ treatment as follows: 400 mg twice-daily loading dose followed by 200 mg twice-daily maintenance dosing. 7 Therefore, it is not surprising that most running studies applied this recommendation (Figure 3C). Only about half of the described treatment regimens (20/42) use an initial loading dose of 800 mg before switching to the maintenance dose (Figure 3A).
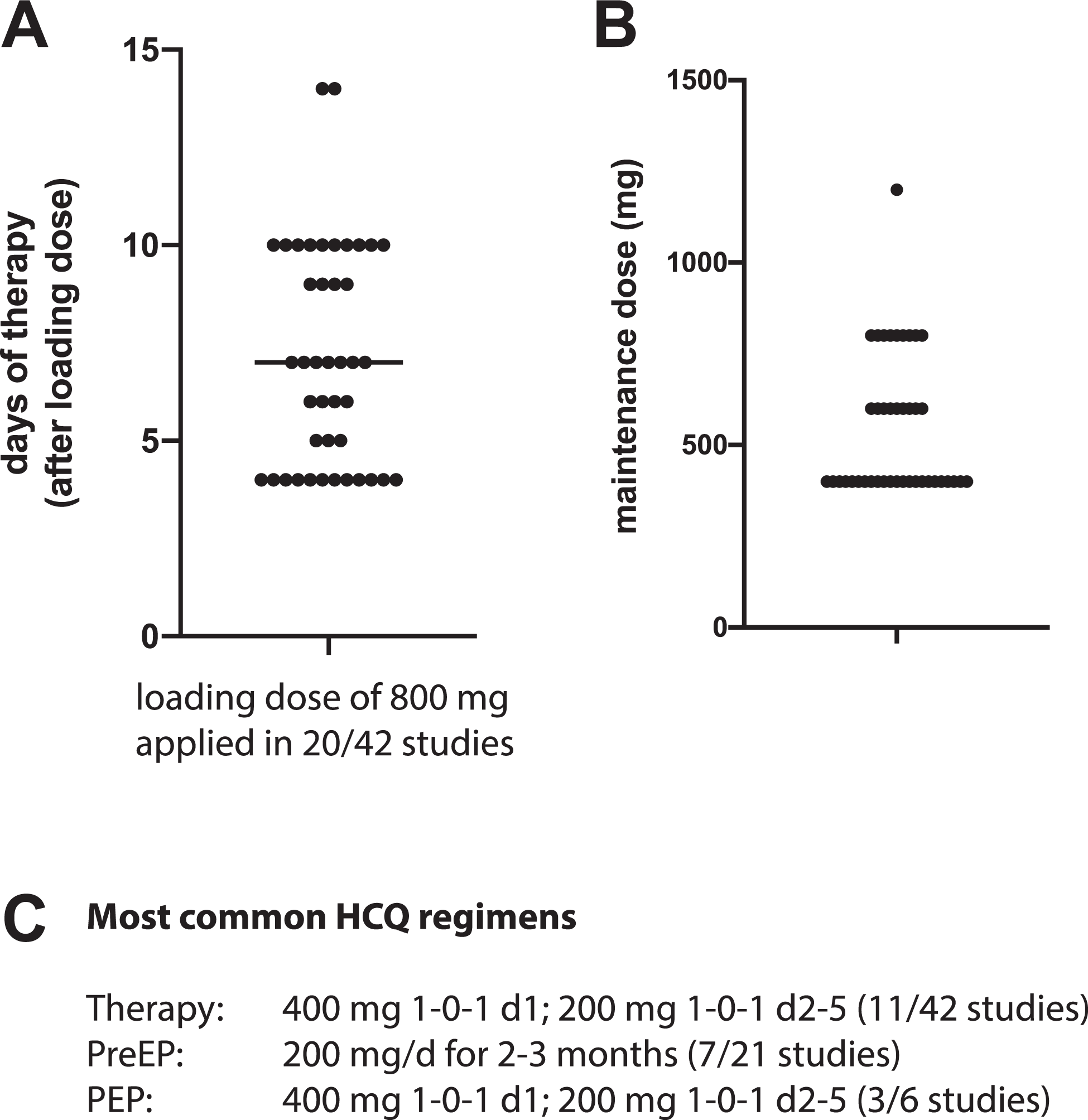
Hydroxychloroquine (HCQ) dosing and treatment duration. A and B, Depicted is the duration of HCQ therapy after loading dose (A) and the maintenance dose used in different trials (B). C, Common HCQ therapy regimens for therapy, pre-exposition (PreEP), and post-exposition prophylaxis (PEP).
Side Effects Under HCQ Therapy
If HCQ was save without any relevant side effects as the first 3 clinical trials in COVID-19 patients suggested, the question arises why not to treat anyone with PCR-proven COVID-19 or even use HCQ as a pharmacological prophylaxis for everyone.
Lessons from HCQ therapies during the last more than 50 years in the context of rheumatoid arthritis, discoid or systemic lupus erythematosus, and malaria prophylaxis and treatment have told us a list of potentially fatal side effects, which will further be discussed in the following section.
Common side effects of HCQ include liver dysfunction, gastrointestinal symptoms, itching, headache, dizziness, peripheral neuropathy, proximal myopathy, and irreversible toxic retinopathy with potential loss of vision. Yet, retinopathy is dependent on the cumulative dosage of HCQ and therefore most likely less relevant in the setting of COVID-19. 22 Most importantly, HCQ is also known to cause severe cardiac arrhythmias. 23 On April 16, 2020, a preprint safety report of a Brazilian study on CQ to fight COVID-19 has been published. The authors report an increased mortality in the high CQ dosage arm of the study (600 mg CQ twice daily for 10 days) and suspect an association with QT prolongation. 24 Focused studies on cardiac side effects under long-term therapy also include conduction disorders and reports of heart failure. 25,26 This is even more threatening since COVID-19 itself was reported to potentially cause myocardial injury and increases the risk of arrhythmias—an observation that is reviewed elsewhere. 27 Most recently, US Food and Drug Administration (FDA) cautions against use of HCQ for COVID-19 outside of hospital setting or a clinical trial due to risk of heart problems. 28
Hydroxychloroquine Prolongs QT Interval and Causes Malignant Arrhythmias
QTc prolongation is defined as >470 milliseconds in males and >480 milliseconds in females or >500 milliseconds as marked QT prolongation for both sexes. 29 This alteration is mediated predominantly by a blockage of KCNH2 potassium channels. Especially patients with different pre-disposures for QTc prolongation summarized as individuals with reduced repolarization reserve including clinically concealed carriers of QT prolonging genetic variants might develop malignant arrhythmias. 29 Familial long QT syndrome is estimated to affect 1 in 2000 individuals. Common genetic variants predisposing to inducible QTc prolongation are even more frequent, 1% to 30% in the general population. 30,31 Current treatment models for COVID-19 affect a very large population of patients who receive HCQ. This leads to an inevitable exposure of predisposed patients with unknown consequences as rare side effects reach relevant absolute numbers. Hydroxychloroquine is eliminated via renal clearance and metabolized in the liver. 16 Its half live is about 50 days due to its very large distribution volume making it comparable to amiodarone. 16,32,33 Therefore, electrocardiography (ECG) monitoring is absolutely essential in the initial phase of HCQ therapy. This can either be done via telemonitoring for critically ill hospitalized patients or, in the outpatient setting, via smartphone-based mobile QTc applications as well as other mobile monitoring devices such as AliveCor (KardiaMobile-6L-device), which has just been approved by the US FDA for this purpose on March 20, 2020. 34
To meet the demands of monitoring a potentially very large cohort of patients under HCQ therapy, the Canadian Heart Rhythm Society has recently released a recommendation to discontinue unnecessary medication which may increase QT interval as well as electrolyte optimization. Additionally, low-risk patients should be identified who do not need intensified ECG monitoring (no history of QT prolongation and normal QTc at therapy initiation, no additional QT-prolonging medication, no unexplained syncope or family history of sudden cardiac death). 35 The Indian Heart Rhythm Society has also raised their concerns for a general public use of HCQ without medical supervision. 34 In line with most cardiac societies, the Mayo Clinic group suggests separating potential individuals under HCQ treatment into 3 risk categories: a low-risk group with no prolonged QTc interval at baseline and less than 60 milliseconds change under therapy; a moderate-risk group with prolonged QTc interval (>470 milliseconds for males; >480 milliseconds for females), but less than 500 milliseconds; and finally, a high-risk group with >500 milliseconds QTc interval at baseline or prolongation of >60 milliseconds under HCQ therapy. According to these risk categories, indications and ECG monitoring intervals should be adapted. 36
In summary, initial studies suggest that HCQ therapy might provide a promising approach in preventive and therapeutic strategies to avoid COVID-19. However, QTc prolongation and subsequent malignant arrhythmias demand high precautions if HCQ was applied population-wide. Therefore, risk category–orientated approaches involving close meshed ECG monitoring are absolutely essential—even in the outpatient setting with potential indications for smartphone-based or comparable technologies. A plethora of running studies will hopefully provide further information of benefits and risks of HCQ therapy and answer the question if protective effects outweigh its proarrhythmic potential.
Footnotes
Author Contributions
C.S. and A.K. conducted literature researach, designed figures and wrote the manuscript. S.M. and S.K. contributed to conception and design and supervised the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.