
Abstract
Background:
Switching between antiarrhythmic drugs is timed to minimize arrhythmia recurrence and adverse reactions. Dronedarone and amiodarone have similar electrophysiological profiles; however, little is known about the optimal timing of switching, given the long half-life of amiodarone.
Methods:
The ARTEMIS atrial fibrillation (AF) Loading and Long-term studies evaluated switching patients with paroxysmal/persistent AF from amiodarone to dronedarone. Patients were randomized based on the timing of the switch: immediate, after a 2-week, or after a 4-week washout of amiodarone. Patients who did not convert to sinus rhythm after amiodarone loading underwent electrical cardioversion. The primary objectives were, for the Loading study, to evaluate recurrence of AF ≤60 days; and for the Long-term study, to profile the pharmacokinetics of dronedarone and its metabolite according to different timings of dronedarone initiation.
Results:
In ARTEMIS AF Loading, 176 were randomized (planned 768) after a 28 ± 2 days load of oral amiodarone. Atrial fibrillation recurrence trended less in the immediate switch versus 4-week washout group (hazard ratio [HR] = 0.65 [97.5% CI: 0.34-1.23]; P = .14) and in the 2-week washout versus the 4-week washout group (HR = 0.75 [97.5% CI: 0.41-1.37]; P = .32). In ARTEMIS AF Long-term, 108 patients were randomized (planned 105). Pharmacokinetic analyses (n = 97) showed no significant differences for dronedarone/SR35021 exposures in the 3 groups.
Conclusion:
The trial was terminated early due to poor recruitment and so our findings are limited by low numbers. However, immediate switching from amiodarone to dronedarone appeared to be well tolerated and safe.
Introduction
In order to optimize antiarrhythmic drug (AAD) therapy for atrial fibrillation (AF), it may be necessary to switch from one AAD to another. 1 For most AADs, the switch is based on stopping the drug for 5 half-lives before starting another. Amiodarone is one of the most frequently prescribed AADs for the treatment of AF in the world, 2 -4 but switching patients from amiodarone to another drug is complicated by the drug’s long half-life of 53 days. 2 Furthermore, little is known about the optimal timing for switching a patient from amiodarone to dronedarone, a noniodinated benzofuran derivative that is advocated for its shorter half-life and sparing of iodine-related side effects. 5
We report here the results from the ARTEMIS AF “Loading” (A
The aim of these 2 studies was to evaluate the efficacy and safety of switching from amiodarone to dronedarone in patients with AF who had either never previously received amiodarone (Loading study) or who had ≥6 months previous exposure to amiodarone (Long-term study). Both studies were intended to provide data to guide optimal AAD use after amiodarone treatment, including drug use in different subcategories of patients with AF.
Methods and Materials
Design, Patients, and Data Collection
Loading and Long-Term Studies
In these 2 international, prospective, multicenter, open-label, randomized, controlled trials, patients with either persistent AF requiring conversion to normal sinus rhythm (Loading study) or paroxysmal or persistent AF (long-term study) were enrolled. Patients aged ≥18 years who had provided written informed consent were eligible for screening. Screening took place ≤12 weeks or ≤10 days prior to randomization in the Loading and the Long-term studies, respectively.
In both studies, key inclusion criteria at screening included the following: a rate corrected QT interval using Bazett’s formula (QTcB) of <500 milliseconds documented on a 12-lead electrocardiogram (ECG) and ≥1 cardiovascular risk factor (age >70 years, hypertension, diabetes, prior transient ischemic attack, or left atrium diameter ≥50 mm). In the loading study, following a change in label recommendations after study start (regarding contraindications to dronedarone in the EU with regard to heart failure after the PALbociclib CoLlaborative Adjuvant Study [PALLAS]), patients with a history of and/or current clinically overt heart failure (congestive heart failure [CHF]), left ventricular systolic dysfunction, or unstable hemodynamic conditions were excluded from the study; however, some patients with CHF or left ventricular ejection fraction <40% were already enrolled prior to this change and were included. Patients in the Loading study must also have had persistent AF >72 hours at screening (documented by an ECG and for which cardioversion, AADs, and anticoagulation were indicated), for which amiodarone had not been administered in the prior 3 months. In the Long-term study, patients were eligible for screening if they had paroxysmal or persistent AF and had been receiving amiodarone for ≥6 months (with at least the last 2 months at a regimen of 200 mg/d). Patients who had been receiving effective anticoagulation treatment or who required a change of amiodarone treatment for any reason (excluding those with major amiodarone-related toxicity, ie, interstitial lung disease, thyroid, or hepatotoxicity) were also eligible for inclusion in the Long-term study.
At randomization, patients must have been in sinus rhythm, receiving effective anticoagulation (according to the American College of Cardiology/American Heart Association/Heart Rhythm Society treatment guidelines for AF), 6 and have a QTcB <500 milliseconds and PR interval <280 milliseconds on a 12-lead ECG. In addition, patients in the Loading study must have been receiving amiodarone for 28 days ± 2 days (at visit 2 of the screening period, patients were given a loading dose of amiodarone consisting of 600 mg daily [one 200 mg tablet 3 times daily] for 1 week, 400 mg daily [one 200 mg tablet twice daily] for 1 week, and 200 mg daily [one 200 mg tablet once daily] for 2 weeks).
The main exclusion criteria were (1) contraindication to oral anticoagulation, (2) documented AF after an acute condition known to cause AF, (3) permanent AF (duration ≥6 months or unknown), (4) bradycardia <50 bpm at rest on 12-lead ECG, (5) CHF, (6) Wolff–Parkinson–White Syndrome, (7) previous history of amiodarone intolerance or toxicity, (8) previous ablation for AF, (9) previous treatment with class I or class III AADs (including sotalol) if taken less than 1 week before screening, and (10) severe hepatic impairment (defined as adverse events [AEs] in the system organ class hepatobiliary disorders and standardized Medical Dictionary of Regulatory Activities query liver-related investigations signs and symptoms). In the Loading study, patients with paroxysmal AF (in whom cardioversion was not indicated) were also excluded. Additional exclusion criteria in the Long-term study included unstable angina pectoris (<7 days), myocardial infarction (<6 weeks), and a history of thyroid dysfunction.
Patients were randomized into 3 parallel groups (A, B, and C) according to the timing of dronedarone initiation after the loading dose or following discontinuation of long-term amiodarone treatment (≥6 months). Group A patients were switched to dronedarone 400 mg twice daily for 8 weeks immediately after randomization, group B patients were switched to dronedarone 400 mg twice daily for 6 weeks following a 2-week amiodarone washout period, and group C patients were switched to dronedarone 400 mg twice daily for 4 weeks following a 4-week amiodarone washout period (Figure 1). Both drugs were supplied by Sanofi for the loading dose study.

Study design. aAmiodarone initiation in Loading study, day - 28 ± 2 days (at visit 2 of the screening period, patients were given a loading dose of amiodarone consisting of 600 mg daily [one 200 mg tablet 3 times daily] for 1 week, 400 mg daily [one 200 mg tablet twice daily] for 1 week, and 200 mg daily [one 200 mg tablet once daily] for 2 weeks). bElectrical cardioversion is allowed (after 7 days of amiodarone in loading study) up to day 1 inclusive. cWith at least the last 2 months at a regimen of 200 mg/d.
The Loading study was conducted from September 2010 to October 2011, while the Long-term study was conducted from October 2010 to April 2012. Unfortunately, due to slow rates of enrollment in the 2 studies, neither study would have been completed within a reasonable and meaningful time frame. Because of the difficulty in recruiting patients to the 2 studies, the study sponsor, in agreement with the Steering Committee, decided to stop the Loading study earlier than planned (on October 20, 2011); no more patients were screened or randomized on or after this date. However, following recalculation of the sample size in the Long-term study, the target number of patients was achieved.
Both studies were approved by the relevant institutional review boards and performed in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki. The ClinicalTrials.gov identifiers are NCT01199081 (Loading study) and NCT01140581 (Long-term study).
Pharmacokinetic Analysis
Plasma samples for quantification of dronedarone and its metabolite SR35021 were collected at baseline (randomization), 3 hours after the first dronedarone dose, and after 1, 2, and 4 weeks of treatment with dronedarone (before the next dronedarone dose). The bioanalytical method used for the analysis of dronedarone and SR35021 was a validated liquid chromatography–tandem mass spectrometry method with a lower limit of quantification (LLOQ) of 0.5 ng/mL for both compounds (Covance). The following exposures were computed for dronedarone and SR35021: (1) the maximum concentration (C max) of the first dronedarone intake on day 1; (2) area under the concentration–time curve (AUC)24 hours in the dosing interval of the first day of dronedarone intake; and (3) AUC336 hours and AUC672 hours, the cumulated AUCs computed over the first 2 and 4 weeks of the repeated dronedarone intake.
Study Objectives
Loading Study
The primary objective of the Loading study was to evaluate the rate of AF recurrence ≤60 days after randomization (defined as an episode of AF lasting ≥10 minutes, as indicated by 2 consecutive 12-lead ECGs or transtelephonic ECG monitoring tracings recorded approximately 10 minutes apart, both showing AF) according to different timings of initiation of dronedarone. Due to a decrease in the sample size of the Loading study as a result of slow recruitment rates, assessment of the primary objective was expanded from 1 month to include the entire study period, that is ≤60 days after randomization. Secondary objectives included (1) assessment of the safety of switching from amiodarone to dronedarone and (2) assessment of the overall safety profile of dronedarone. For the safety analysis, an AE was defined as any untoward medical occurrence in a patient administered a pharmaceutical product that did not necessarily have a causal relationship with this treatment, irrespective of any presumed relationship with the drug.
Long-term study
The primary objective of the Long-term study was to explore the PK profile of dronedarone and its metabolite SR35021 according to different timings of dronedarone initiation. Secondary objectives included (1) evaluation of the rate of AF recurrence ≤60 days after randomization (based on adjudicated ECG data and defined as the time from day 1 [randomization] to the date of ECG where the first AF recurrence was observed), (2) exploration of the potential PK interaction between dronedarone and amiodarone, (3) assessment of the safety of switching from amiodarone to dronedarone, and (4) assessment of the overall safety profile of dronedarone. Recurrence of AF was defined as an episode of AF lasting ≥10 minutes and indicated by 2 consecutive 12-lead ECG tracings recorded approximately 10 minutes apart. Patients who did not experience AF recurrence were censored at day 61 or at the end of the study if this date was prior to day 60; patients who discontinued prematurely were censored at the day of discontinuation. For the safety analysis, AEs were defined as in the Loading study.
Statistical Analysis
Loading study
Based on the original efficacy analysis, and in order to show a reduction of AF recurrence after 1 month by 36.5% in group A (and group B) compared with group C, with an α level of 2.5% (2-sided tests) and 80% power, it was estimated that 256 evaluable patients per treatment group were required. Taking into account an expected screening failure rate of 10%, 860 patients should be screened in order to randomize 768 patients (256 per arm). However, due to the low enrollment rate, only 176 patients were randomized. This figure was significantly smaller than originally estimated.
For the main efficacy analysis, log-rank tests were used to compare group A versus group C and group B versus group C; significance levels for each comparison were set at 0.025 (2-sided), in order to maintain a global α level of .05. A Cox proportional hazard model was used to calculate hazard ratios (HRs), with 2-sided 97.5% CIs. The primary analysis population was the intent-to-treat population, which consisted of all randomized patients.
Long-term study
With an estimated non-evaluability rate of 10% before and 10% after randomization, 165 patients were planned to be screened in order to randomize 147 (49 in each group). However, due to a slow enrollment rate, the protocol was amended (November 8, 2011); following this amendment 147 patients were planned to be screened in order to randomize 105 patients (35 in each group), using an estimated non-evaluability rate of 30% and in order to achieve a maximal imprecision of 20%.
For the main efficacy analysis, a non-stratified log-rank test was used to compare group A with group C and group B with group C; significance levels for each comparison were set at 0.025 (2-sided), in order to maintain a global α level of .05 (2-sided). Cumulative incidence functions were calculated using a nonparametric Kaplan–Meier estimate. A Cox proportional hazard model was used to calculate HR, with 2-sided 97.5% CIs.
Pharmacokinetic analysis
Estimation of dronedarone and SR35021 individual exposure parameters was only possible through a Bayesian process, due to the limited sample size. The Bayesian analysis was performed with the NONMEM computer program (version 7.2) running on a LINUX cluster of multiprocessor computers. 7 A previously developed population pharmacokinetics (PopPK) model was applied to the data set, using its population parameter estimates as prior estimates for the assessment of individual parameters and concentration predictions for the patients from the ARTEMIS AF study. Due to the complexity of the PopPK model (simultaneously fitting dronedarone and SR35021 concentrations), the first-order estimation method was used throughout the whole modeling process. For each patient, individual PK parameter estimates were made from the obtained population parameters.
Dronedarone was given immediately, 2 weeks/336 hours or 4 weeks/672 hours after amiodarone cessation; however, the relative time between the last amiodarone dose and the first dronedarone administration was variable between patients. Due to the limited sample size and to avoid any loss of information, for the purposes of the plots, all dosing times before 48 hours were considered as “immediately,” all times between 48 and 408 hours (17 days) as “2 weeks,” and all times >408 hours as “4 weeks.”
Results
Study Population Loading Study
In total, 403 patients were screened from 49 sites in 16 countries across Europe, Asia-Pacific, and South America (Australia, Austria, Estonia, Finland, France, Germany, Israel, Italy, the Republic of Korea, Mexico, the Netherlands, Portugal, Spain, Switzerland, Taiwan, and the UK). Due to slow enrollment, the study was stopped by the sponsor prior to reaching the planned sample size. Overall, 176 patients were randomized: 58, 59, and 59 into groups A, B, and C, respectively (Figure 1; Appendix Table 1). One hundred and forty-eight patients completed treatment (51, 53, and 44 in groups A, B, and C, respectively). Baseline demographics and cardiovascular parameters are shown in Table 1.
Baseline Demographics and Cardiovascular Parameters in the Loading Study (Randomized Population).

Abbreviations: BMI, body mass index; CHF, congestive heart failure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; WO, washout.
a Following a change in prescription recommendations after study start, patients with a history of and/or current heart failure, left ventricular systolic dysfunction, or unstable hemodynamic conditions were excluded from the study; however, some patients with CHF or LVEF <40% were already enrolled prior to this change.
Study Population Long-Term Study
In total, 154 patients were screened from 29 sites in 7 countries across Europe, North, and South America (Colombia, the Czech Republic, Denmark, France, Germany, Mexico, and Spain). Overall, 108 patients were randomized: 37, 38, and 33 into groups A, B, and C, respectively (Figure 1; Appendix Table 2). Eighty-six patients completed treatment (35, 25, and 26 patients in groups A, B, and C, respectively). Baseline demographics and cardiovascular parameters are shown in Table 2.
Baseline Demographics and Cardiovascular Parameters in the Long-term Study (Randomized Population).

Abbreviations: AF, atrial fibrillation; BMI, body mass index; CHF, congestive heart failure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; WO, washout.
Efficacy
Loading study
There was a non-statistically significant decrease in AF recurrence (≤60 days after randomization) of 35.3% (HR = 0.65 [97.5% CI: 0.341-1.225]; P = .14) in the immediate (group A) compared with the 4-week washout group (group C). For the 2-week washout group (group B), there was a non-statistically significant 24.7% decrease in AF recurrence (HR = 0.753 [97.5% CI: 0.413-1.374]; P = .32) compared with the 4-week washout group (group C; Figure 2A).
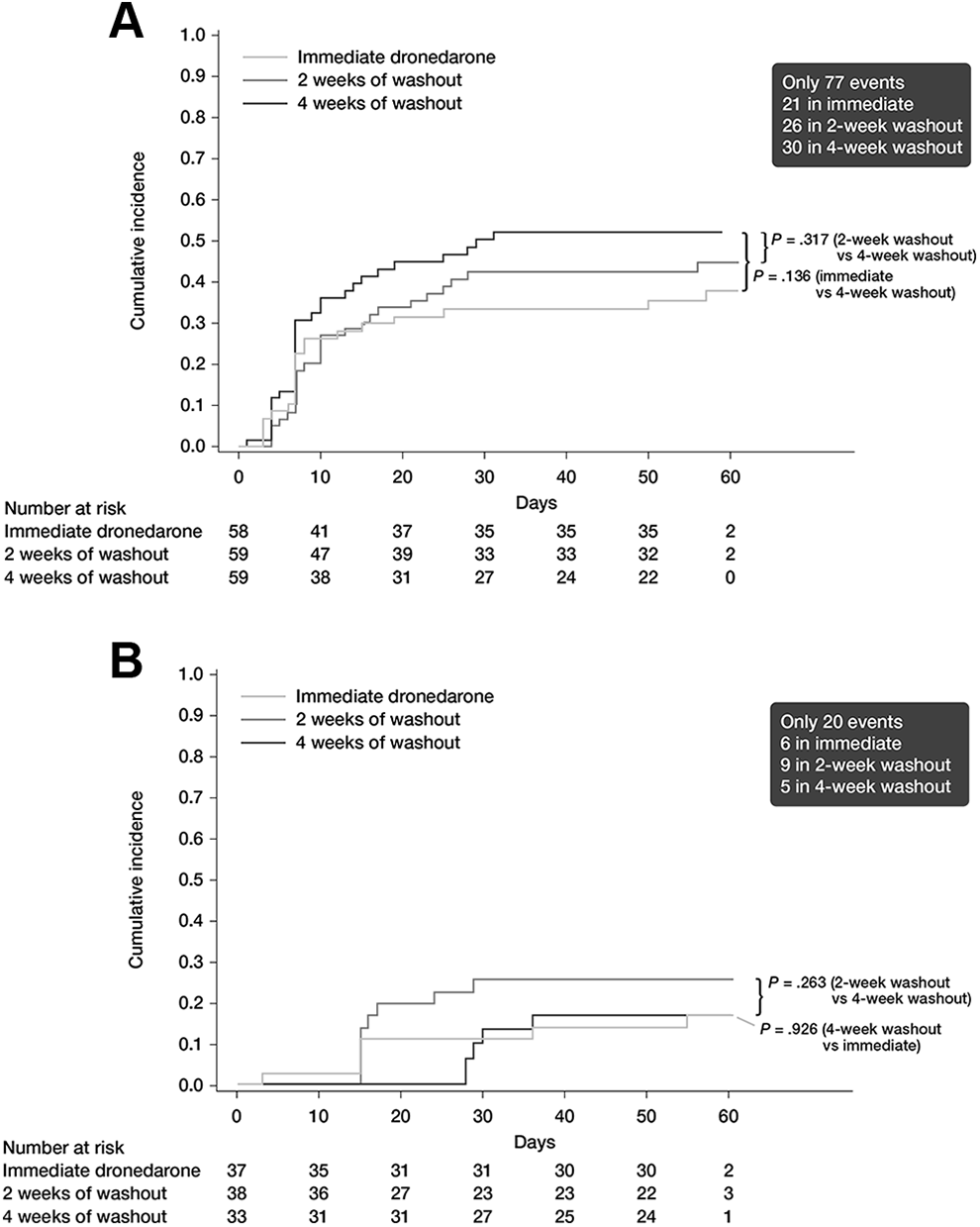
A, First recurrence of AF ≤60 days after randomization in the Loading study (ITT population), and (B) First recurrence of AF ≤60 days after randomization in the Long-term study (ITT population). Cumulative incidence function with Kaplan–Meier estimates, based on adjudicated data. AF indicates atrial fibrillation; ITT, intent-to-treat.
Mean (SD) heart rates remained virtually unchanged between baseline and end of treatment (59.9 [9.7] and 62.0 [11.4], respectively). Overall, changes were similar across the 3 treatment groups. At baseline, rates were 59.8 (10.2) bpm for group A, 60.6 (9.4) bpm for group B, and 59.3 (9.8) bpm for group C. At the end of treatment, rates were 63.4 (13.3) bpm for group A, 61.9 (9.7) bpm for group B, and 60.5 (11.0) bpm for group C.
Long-term study
There were no significant differences in risks of AF recurrence (≤60 days after randomization) among the 3 treatment groups (Figure 2B). Compared with the 4-week washout group (group C), there was a nonsignificant increase in AF recurrence of 6.3% in the immediate group (group A; P = .93). However, there was an 88.5% increased risk of AF recurrence in the 2-week washout group (group B) compared with the 4-week group (group C); again, this difference was not statistically significant (P = .26).
The mean heart rate showed normal variation throughout the treatment period and across the 3 treatment groups, with a total mean (SD) of 63.2 (9.2) bpm at baseline and 62.5 (12.3) bpm at the end of treatment. Overall, changes were similar across the 3 treatment groups. At baseline, rates were 62.3 (8.0) bpm for group A, 63.4 (10.4) bpm for group B, and 64.4 (9.4) bpm for group C. At the end of treatment, rates were 63.0 (13.8) bpm for group A, 60.7 (11.5) bpm for group B, and 63.7 (11.1) bpm for group C.
Pharmacokinetics
Long-term study
The data set comprised the 97 patients who had at least 1 sample of either dronedarone or SR35021 above the LLOQ, for a total of 729 samples (365 for dronedarone and 364 for SR35021). The mean (±SD) age of the Bayesian data set was 67.3 (10.1) years. In total, 48.5% were male and 74.2% were Caucasian.
Dronedarone and SR35021 exposure values (C max) at the first dronedarone intake on day 1 are shown in Figure 3A. The lowest values were observed in this “immediate” group (group A), while the highest values were seen in the 2-week washout group (group B; Table 3). As shown by the AUCs, there was a tendency toward higher values for both dronedarone and SR35021 exposures in the 2-week washout group (group B), while the lowest values were observed in the 4-week washout group (group C; Figure 3B-D). Descriptive statistics on individual exposure values of dronedarone and SR35021 are presented separately for each treatment group in Table 3 (ie, dronedarone given immediately, 2 or 4 weeks after amiodarone cessation).

(A) Dronedarone and SR35021 C max calculated at the first dronedarone intake (Long-term study Bayesian data set), (B) dronedarone and SR35021 AUC24 hours at the first day of dronedarone administration (Long-term study Bayesian data set), (C) dronedarone and SR35021 AUC336 hours calculated over the first 2 weeks of dronedarone intake (Long-term study Bayesian data set), and (D) dronedarone and SR35021 AUC672 hours calculated over the first 4 weeks of dronedarone intake (Long-term study Bayesian data set). White dots represent individual values; black dots and error bars are mean values ± SD. The horizontal error bars quantify the variation in the timing of dronedarone initiation after amiodarone discontinuation in each group. The vertical error bars describe the variation in dronedarone concentrations. AUC indicates area under the curve; C max, maximum concentration.
Mean, CV%, Median, and 5th and 95th Percentiles of Individual Exposure Values of Dronedarone and SR35021 (Long-Term Study Bayesian Data Set).
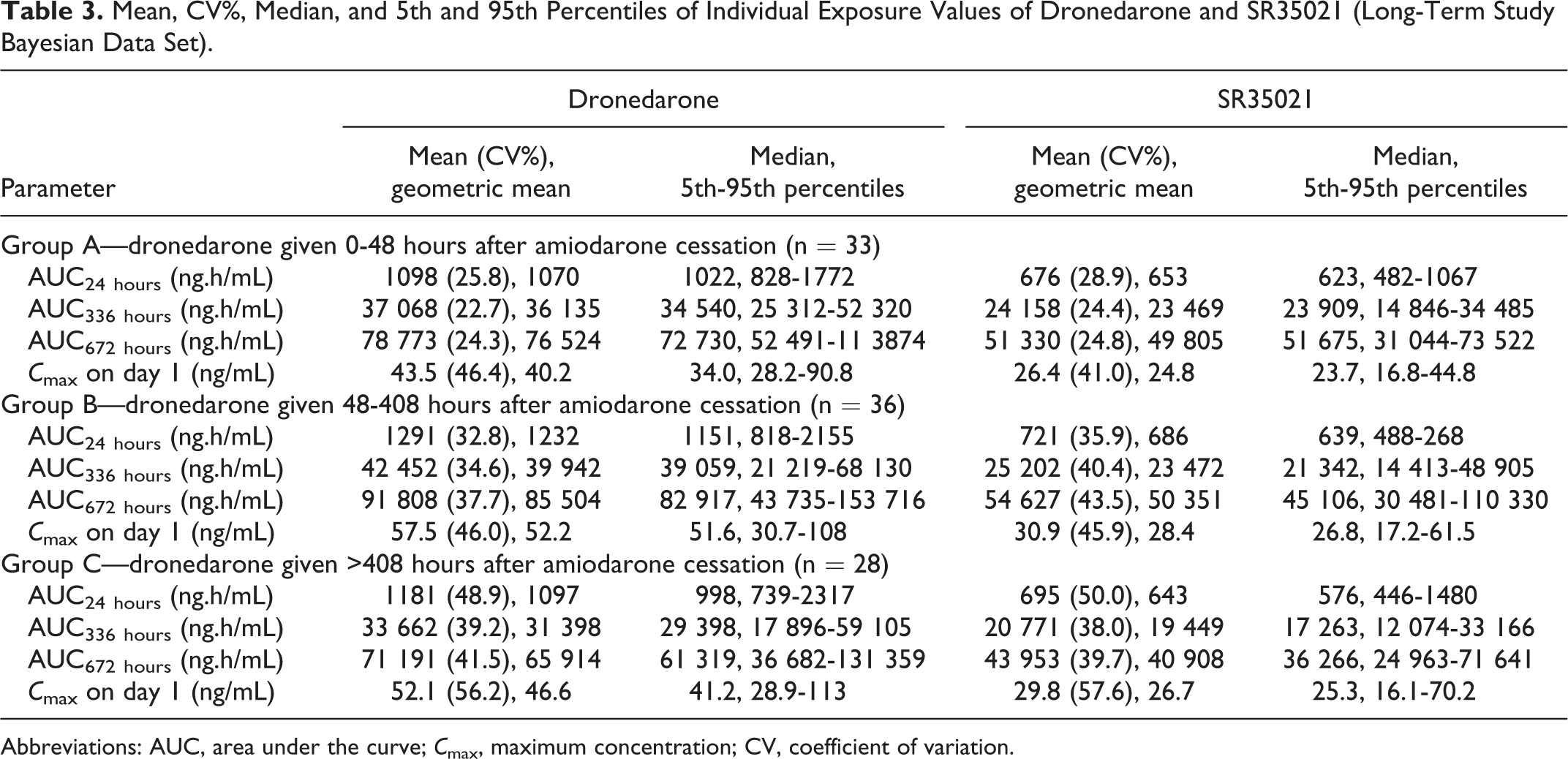
Abbreviations: AUC, area under the curve; C max, maximum concentration; CV, coefficient of variation.
Safety
Loading study
Overall, there were no significant differences among the 3 treatment groups in the risk of bradycardia (defined as a heart rate at rest <50 bpm; group A vs group C, P = .55; group B vs group C, P = .49) or tachycardia (defined as heart rate at rest >90 bpm; group A vs group C, P = .54; group B vs group C, P = .12). In total, 20, 22, and 11 patients (20.1, 27.1, and 25.0 patient-months) experienced an AE in the immediate-switch group (group A), 2-week washout (group B), and 4-week washout group (group C), respectively (Table 4). In total, 53 patients had a treatment-emergent AE (TEAE); 9 of these had a serious TEAE. Across the 3 groups, 4 (1.8 patient-months) patients permanently discontinued dronedarone treatment due to a TEAE (2.0, 1.3, and 2.3 patient-months in the immediate, 2-week, and 4-week washout groups, respectively). Treatment-emergent AEs leading to permanent dronedarone discontinuation included dizziness and tremor in group A, syncope in group B, and chronotropic incompetence in group C.
Safety Overview During the Dronedarone Period in the Loading Study (Randomized and Treated Population).

Abbreviations: TEAE, treatment-emergent adverse event; WO, washout. Patient-months = number of patients with at least 1 TEAE in 100 patient-months.
aAdverse event of special interest (as per the narrow Standardized Medical Dictionary of Regulatory Activity Query, version 14.1).
bIncrease in alanine transaminase.
Overall, there was a similar incidence of potentially clinically significant abnormalities among the 3 treatment groups with the exception of an increased PR interval; an increased PR interval was more frequently reported in the immediate switch group (15.2%) compared with the 2-week washout (4.8%) and 4-week washout (3.4%) groups. While not statistically significant, during the dronedarone period, QTcB ≥500 milliseconds at any visit was greater in the immediate-switch group (group A; 7/58, 12.1%) compared with both the 2-week (group B; 3/57, 5.3%; P = .53) and 4-week washout (group C; 4/48, 8.3%; P = .93) groups, respectively.
Long-term study
Patients in the 2-week washout group (group B) had a significantly higher risk of bradycardia compared with those in the 4-week washout group (group C; HR = 6.15 [97.5% CI: 1.095-34.533]; P = .01). However, there was no significant difference in risk of bradycardia between the immediate dronedarone group (group A) and the 4-week washout group (group C; P = .19) or risk of tachycardia among the 3 treatment groups (group A vs group C, P = .33; group B vs group C, P = .26).
Overall 15, 14, and 9 patients (22.5, 34.3, and 35.0 patient-months) experienced an AE in the immediate-switch group (group A), 2-week washout group (group B), and 4-week washout group (group C), respectively (Table 5). In total, 38 patients reported ≥1 TEAE, 5 of these had ≥1 serious TEAE, and 2 reported a serious TEAE leading to hospitalization (1 patient was hospitalized for pneumonia with symptoms of fever and 1 patient experienced worsening of rectal pain and stool incontinence). Across the 3 groups, 8 (6.0 patient-months) patients permanently discontinued dronedarone treatment due to a TEAE. Although more patients in the 2-week washout group (group B; n = 6 [14.7 patient-months]) had a TEAE leading to permanent discontinuation compared with the immediate-switch (group A) and 4-week washout (group C) groups (n = 2 [3.0 patient-months] and n = 0 [0 patient-months], respectively), there were no other important differences overall in AE profiles among the 3 treatment groups (Table 5). Treatment-emergent AEs leading to permanent dronedarone discontinuation included arrhythmia, cardiac failure, burning sensation, diplopia, vision blurred, and syncope in group A and abdominal pain upper, nausea, tinnitus, pruritus, hypersensitivity, asthenia, and erythema in group B.
Safety Overview During the Dronedarone Period in the Long-term Study (Randomized and Treated Population).a

Abbreviations: TEAE, treatment-emergent adverse event; WO, washout. Patient-months = number of patients with at least 1 TEAE in 100 patient-months.
a Adverse event of special interest (as per the narrow Standardized Medical Dictionary of Regulatory Activity Query, version 14.1)
b Increase in alanine transaminase.
Discussion
Amiodarone is currently the most widely used AAD for the maintenance of sinus rhythm. However, amiodarone has a very long half-life and tissue accumulation, potentially leading to severe organ toxicities and cancer with long-term use in men. Measurable PK and pharmacodynamic effects can be detected several weeks after amiodarone treatment discontinuation. Dronedarone, a benzofuran derivative demonstrating electrophysiological characteristics belonging to all four Vaughan-Williams classes, is devoid of the iodine moiety and has a methane sulfonyl group that reduces its lipophilicity and likelihood of accumulation in tissue. 8 Clinical studies have demonstrated the favorable safety profile of dronedarone in patients with paroxysmal or persistent AF and the lower risk for amiodarone-like organ toxicity. 9 Patients with AF who have already been exposed to amiodarone might be eligible for treatment with dronedarone for safety reasons and, potentially, to target clinical outcome benefits as shown in the ATHENA study. 10
Dronedarone has a low propensity for medical conversion of persistent AF to sinus rhythm, 11 whereas oral amiodarone may convert up to 25% of persistent AF patients after several weeks of loading. 12 In addition, evidence suggests that persistent AF patients treated with amiodarone have a good probability of preserving sinus rhythm following termination of the arrhythmia. 12 As such, amiodarone is commonly used for this purpose. Given that amiodarone is also effective in preventing early AF recurrences post-cardioversion, the clinical approach of loading with amiodarone (to optimize cardioversion outcomes), then switching to dronedarone (for long-term benefits), could become customary in clinical practice. Both drugs have similar multichannel blocking effects and have an extremely low risk of causing torsades de pointes. In the clinical trial program of patients with nonpermanent AF, dronedarone demonstrated a similar risk of ventricular pro-arrhythmia as placebo, 9 -11 and in a real-world analysis of all AF patients in the Swedish Patient registry (2010-2015) dronedarone was the only AAD with lower risk of ventricular pro-arrhythmia than sotalol. 13
However, physicians may be concerned about potential additive safety issues such as bradycardia, QT interval prolongation, and an increase in the PR interval if the 2 drugs are given in combination. Thus, in order to acquire a better knowledge of dronedarone’s behavior following a switch from amiodarone, this phase IV clinical study, ARTEMIS AF, was performed to evaluate the impact of amiodarone on dronedarone.
The ARTEMIS AF Loading study involved administration of dronedarone to patients who had persistent AF requiring conversion at 3 different intervals after administration of a loading dose of amiodarone. Although patients may not have been fully loaded, they all received the same cumulative loading dose of nearly 10 g of drug over 4 weeks. ARTEMIS AF loading was designed to specifically and prospectively evaluate the efficacy and safety of the immediate change from a loading dose of amiodarone to long-term dronedarone treatment in comparison with initiation after a 2-week or a 4-week amiodarone washout period. Unfortunately, due to slow rates of enrollment, the study would not have been completed within a reasonable and meaningful time frame. As such, only 176 patients were randomized out of the original 768 planned. While 148 (84.1%) of randomized patients completed the study, the final sample size was not sufficient to provide robust efficacy data.
In the Loading study, there was a nonsignificant numerical trend for a reduction in AF recurrence in the immediate-treatment group and the 2-week washout group compared with the 4-week washout group. The overall safety profile was similar in all 3 treatment groups, with no increase in AEs seen in the absence of a washout period. Although in this small cohort of patients the tolerability of a rapid switch was acceptable, the decision of when to start dronedarone after the discontinuation of amiodarone should be made on an individual basis, taking into account each patient’s characteristics.
Similarly, in the ARTEMIS AF Long-term study, while the primary objective was to explore dronedarone and SR35021 PK profiles according to different timings of dronedarone initiation, considering the low number of patients available in each study group, it is not possible to confirm whether the differences in dronedarone/SR35021 exposures from 1 treatment group to another are significant. In the Long-term study, the PK data showed that surprisingly, there was a tendency toward higher values for dronedarone and SR35021 exposures in the 2-week washout group, with the lowest values observed in the 4-week washout group. This was mainly visible on cumulative AUCs computed after 2 or 4 weeks of dronedarone intake (Figure 3) and is in accordance with the dronedarone concentrations observed in the ARTEMIS AF study. Similar trends were also observed for amiodarone. Superficially, such observations could suggest a possible drug–drug interaction between dronedarone and amiodarone. However, this possibility can likely be discarded because observed amiodarone concentrations collected before any dronedarone intake (on visit 3) were also higher in the 2-week washout group compared with the immediate dronedarone and 4-week washout groups (median values of 828 vs 605 and 616 ng/mL, respectively).
The higher amiodarone concentrations observed before any dronedarone intake might be due to unbalanced patient randomization regarding a specific patient’s covariates between the different groups, causing higher amiodarone steady-state exposures in the 2-week washout patients. The examination of available covariates (body weight, height, sex, age, race, or creatinine clearance) did not allow for finding any differences between groups. The potentially unbalanced covariate remains unknown but, as amiodarone and dronedarone absorption, distribution, metabolism, and excretion profiles (mainly CYP3A-mediated clearance) are similar, this unknown covariate seems to be also involved in the higher exposures of dronedarone in the 2-week washout patients. The effect of this possible unknown covariate—which could be a pharmacogenomic polymorphism of metabolizing enzymes such as CYP3A5*1/*3 and/or drug transporters—is nevertheless not in accordance with the metabolic ratios, which remained roughly constant whatever the considered exposure, indicating that no metabolic interaction has occurred with dronedarone that could have explained these differences. Of course, the observed differences between the 3 treatment groups might also be due to chance in an underpowered study. While the overall safety profile also appeared to be good in the Long-term study, few AF events were observed, and thus no firm conclusions can be drawn on the optimal time for initiation of dronedarone in patients with more than 6 months of exposure to amiodarone.
A limitation of our findings is that complete enrollment was not achieved in the Loading study due to changes in the dronedarone Committee for Medicinal Products for Human Use labeling required by the European Medical Agency. These changes were made secondary to hepatic issues (external to these studies) and the results of the PALLAS study. However, in spite of this limitation, the results of both studies suggest that immediate switching from amiodarone to dronedarone, after amiodarone loading or long-term treatment with amiodarone, is not associated with an increased rate of arrhythmic recurrences or major AEs, including the necessity of drug discontinuation, QTc interval prolongation, or drug-induced bradycardia. These findings are further supported by Immordino et al, in which a rapid switch from amiodarone to dronedarone within a 2-day time frame was associated with a low overall incidence of AEs and appeared feasible in certain categories of patients with AF. Although this trial demonstrated that a rapid switch from amiodarone to dronedarone appeared safe, there were slightly more bradyarrhythmic and heart failure events.
High-risk patients with heart rates <50 bpm, QTcB >500 milliseconds, or a PR >280 milliseconds were excluded from the trial, similar to previous trials and according to the package insert for dronedarone. Therefore, our findings should not be extrapolated to these high-risk patients. In addition, although heart failure patients were included in the trial, high-risk patients with heart failure were excluded and findings from this study should not be extrapolated to these high-risk patients.
Conclusion
Based on the data presented here, immediate switching from amiodarone to dronedarone, after amiodarone loading or long-term treatment with amiodarone, appears to be well tolerated after both loading dose and long-term amiodarone use. However, due to the low number of patients in the Loading study as a result of the premature study discontinuation, and given that the Long-term study was not powered for efficacy/safety, any conclusions may be limited. As such, any decisions regarding switching between 1 drug and another should be made by the treating physician and taken on a case-by-case basis, considering the individual patients’ characteristics.
Supplemental Material
Supplemental Material, Multaq_ARTEMIS_ms_Appendix_18Mar20 - Evaluation of the Switch From Amiodarone to Dronedarone in Patients With Atrial Fibrillation: Results of the ARTEMIS AF Studies
Supplemental Material, Multaq_ARTEMIS_ms_Appendix_18Mar20 for Evaluation of the Switch From Amiodarone to Dronedarone in Patients With Atrial Fibrillation: Results of the ARTEMIS AF Studies by Gerald V. Naccarelli, Deepak L. Bhatt, A. John Camm, Jean-Yves Le Heuzey, Federico Lombardi, Juan Tamargo, Jean-Marie Martinez, Lisa Naditch-Brûlé and for the ARTEMIS AF Investigators in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Appendix
Authors’ Note
Acknowledgements
The authors acknowledge the assistance of Leigh Prevost and Sola Neunie (employees of PPSI, a PAREXEL company) for the editing of the manuscript. The authors would like to thank Harmonie Goyeau from Sanofi for statistical support and Céline Ollier from Sanofi for the pharmacokinetic analyses. Editorial and administration support was provided by Prime, Knutsford, UK.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. G.V.N. is a consultant for Janssen, Omeicos, Acesion, Milestone, and Sanofi; and has a research grant from Janssen unrelated to this project. D.L.B has participated in advisory boards for Cardax, Cereno Scientific, Elsevier Practice Update Cardiology, Medscape Cardiology, PhaseBio, PLx Pharma, and Regado Biosciences; is a member of the Board of Directors of Boston VA Research Institute, Society of Cardiovascular Patient Care, and TobeSoft; is Chair of the American Heart Association Quality Oversight Committee; is on the data monitoring committees for Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), and Population Health Research Institute; has received honoraria from the American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ![]() ; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), and WebMD (CME steering committees); has other relationships with Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), VA CART Research and Publications Committee (Chair); has received research funding from Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Cardax, Chiesi, CSL Behring, Eisai, Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Idorsia, Ironwood, Ischemix, Lexicon, Lilly, Medtronic, Pfizer, PhaseBio, PLx Pharma, Regeneron, Roche, Sanofi Aventis, Synaptic, and The Medicines Company; has received royalties from Elsevier (Editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart Disease); is a site co-investigator for Biotronik, Boston Scientific, CSI, St. Jude Medical (now Abbott), and Svelte; is a trustee for American College of Cardiology; and has performed unfunded research for FlowCo, Merck, Novo Nordisk, and Takeda. J.-Y.L.H. has worked on advisory boards for Sanofi, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi-Sankyo, GSK, Meda, MSD, Pfizer, and Servier. A.J.C. has worked on advisory boards and/or speaker’s bureaus for Acesion, Actelion, AstraZeneca, Bayer, Biotronik, Boehringer Ingleheim, Boston Scientific, Bristol-Myers Squibb, ChanRX, Daiichi-Sankyo, Gilead, GSK, InfoBionic, Incarda, Johnson & Johnson, Medtronic, Menarini, Merck, Mitsubishi, Novartis, Omeicos, Otsuka, Pfizer, Sanofi, Servier, St. Jude Medical, Takeda, and Xention. F.L. is a consultant for Sanofi and has also worked on speaker’s bureaus for AstraZeneca, Daiichi-Sankyo, and Merck. J.T. is a consultant for and/or has worked on speaker’s bureaus for Menarini and MSD; and has received honoraria from Menarini, BMS, and Pfizer. J.-M.M. and L.N.-B. are both employees of Sanofi and own stock.
; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), and WebMD (CME steering committees); has other relationships with Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), VA CART Research and Publications Committee (Chair); has received research funding from Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Cardax, Chiesi, CSL Behring, Eisai, Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Idorsia, Ironwood, Ischemix, Lexicon, Lilly, Medtronic, Pfizer, PhaseBio, PLx Pharma, Regeneron, Roche, Sanofi Aventis, Synaptic, and The Medicines Company; has received royalties from Elsevier (Editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart Disease); is a site co-investigator for Biotronik, Boston Scientific, CSI, St. Jude Medical (now Abbott), and Svelte; is a trustee for American College of Cardiology; and has performed unfunded research for FlowCo, Merck, Novo Nordisk, and Takeda. J.-Y.L.H. has worked on advisory boards for Sanofi, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi-Sankyo, GSK, Meda, MSD, Pfizer, and Servier. A.J.C. has worked on advisory boards and/or speaker’s bureaus for Acesion, Actelion, AstraZeneca, Bayer, Biotronik, Boehringer Ingleheim, Boston Scientific, Bristol-Myers Squibb, ChanRX, Daiichi-Sankyo, Gilead, GSK, InfoBionic, Incarda, Johnson & Johnson, Medtronic, Menarini, Merck, Mitsubishi, Novartis, Omeicos, Otsuka, Pfizer, Sanofi, Servier, St. Jude Medical, Takeda, and Xention. F.L. is a consultant for Sanofi and has also worked on speaker’s bureaus for AstraZeneca, Daiichi-Sankyo, and Merck. J.T. is a consultant for and/or has worked on speaker’s bureaus for Menarini and MSD; and has received honoraria from Menarini, BMS, and Pfizer. J.-M.M. and L.N.-B. are both employees of Sanofi and own stock.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was sponsored by Sanofi, who provided assistance with data collection. PAREXEL and Prime were funded by the sponsor.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.