
Abstract
Remote ischemic conditioning is the phenomenon whereby brief, nonlethal episodes of ischemia in one organ (such as a limb) protect a remote organ from ischemic necrosis induced by a longer duration of severe ischemia followed by reperfusion. This phenomenon has been reproduced by dozens of experimental laboratories and was shown to reduce the size of myocardial infarction in many but not all clinical studies. In one recent large clinical trial, remote ischemic conditioning induced by repetitive blood pressure cuff inflations on the arm did not reduce infarct size or improve clinical outcomes. This negative result may have been related in part to the overall success of early reperfusion and current adjunctive therapies, such as antiplatelet therapy, antiremodeling therapies, and low-risk patients, that may make it difficult to show any advantage of newer adjunctive therapies on top of existing therapies. One relevant area in which current outcomes are not as positive as in the treatment of heart attack is the treatment of shock, where mortality rates remain high. Recent experimental studies show that remote ischemic conditioning may improve survival and organ function in shock states, especially hemorrhagic shock and septic shock. In this study, we review the preclinical studies that have explored the potential benefit of this therapy for shock states and describe an ongoing clinical study.
Keywords
Remote Conditioning and Acute Myocardial Infarction
Ischemic preconditioning is a therapeutic approach that consistently has been shown to reduce the size of acute myocardial infarction in experimental models. Repetitive episodes of brief ischemia within one vascular bed protect the myocardium from a subsequent prolonged episode of ischemia in that same vascular bed, reducing the amount of ischemia/reperfusion-induced necrosis. 1 There is evidence that this phenomenon occurs in humans as well, including the observation that patients who have preinfarction angina have smaller myocardial infarctions than those who do not experience angina prior to their myocardial infarction. In a study done in collaboration with the TIMI group, preinfarction angina was also associated with less death, cardiogenic shock, and heart failure. 2 The problem with trying to apply ischemic preconditioning to the clinical scenario of acute myocardial infarction as a therapy is that there is no way to know when a myocardial infarction will occur and no way to preemptively and ethically induce brief episodes of ischemia within the vascular bed of the myocardium that is at risk of developing a heart attack.
Another approach is to induce conditioning episodes of ischemia in a remote vascular bed, which could include a limb. Przyklenk et al 3 showed that brief episodes of ischemia in the circumflex bed of the dog protected the left anterior descending vascular bed from a prolonged occlusion, resulting in a significantly smaller infarction than in dogs that did not receive this remote conditioning. Ischemia in the legs prior to coronary artery occlusion reduced infarct size in a rabbit model. 4 In addition, Gho et al 5 found that brief mesenteric artery occlusions and reperfusion could reduce myocardial infarct size. Now many experimental studies have confirmed that brief episodes of ischemia in a limb could protect the heart and reduce the size of the heart attack, as described in recent reviews and meta-analyses. 6,7 In one meta-analysis, the authors reviewed 31 reports including 22 controlled comparisons and data from 280 control animals and 373 animals subjected to remote ischemic preconditioning (RIPC) and found that conditioning could reduce infarct size as a percentage of the ischemic risk zone by an average of 23% compared to untreated controls. The limb ischemia could be induced prior to the coronary artery occlusion (preconditioning) and some investigators found that limb ischemia could protect the heart even when the conditioning regimen was begun after the coronary artery was already occluded (perconditioning) or reperfused (postconditioning). In the meta-analysis of animal studies by Bromage et al, 6 remote ischemic preconditioning or postconditioning reduced infarct size by 22%.
Remote conditioning could become a potential therapy as it could be induced by simply inflating a blood pressure cuff on an arm or leg above systolic pressure for a few minutes, then deflating the cuff, and then repeating the procedure a few times; in addition, it could be started after the patient experienced symptoms in a perconditioning or postconditioning manner. Botker et al 8 performed one of the first large clinical trials testing this therapy in patients with acute myocardial infarction. Patients with ST-elevation myocardial infarction (STEMI) were randomized to remote ischemic perconditioning by inflating and deflating a blood pressure cuff on the arm in the ambulance on the way to the hospital. Patients who received this treatment had an improved salvage index on nuclear cardiology studies. In addition, a long-term follow-up showed that patients who received this conditioning protocol had a lower incidence of major adverse cardiovascular events. 9 There were several other studies that showed a reduction in myocardial infarct size assessed by a variety of techniques with this type of conditioning regimen. Most of these studies included tens to hundreds of patients and were consistent in the positive effect of remote ischemic conditioning on reducing evidence of ischemic necrosis in patients, as reviewed in several recent meta-analyses. 10 -12 However, a very recent large, prospective, single-blind, randomized and controlled multicenter study of 5401 patients who received primary percutaneous coronary intervention for STEMI failed to show any benefit of remote ischemic conditioning on either myocardial infarct size or clinical outcome (cardiac death or hospitalization for heart failure at 1 year; 8.6% in the control group and 9.4% in the conditioning group). 13 This negative study has now raised the question of the usefulness of this therapy in myocardial infarction. Why were these recent results negative when other experimental and clinical trials were positive? One theory is that the smaller trials were subject to type 1 error. Another has to do with the evolving mode of treating myocardial infarction and its risk factors. It was observed in the recent Lancet paper that mortality rates were very low (less than 3% 1-year mortality in the control group). One possibility is that the usual therapies for acute myocardial infarction, including rapid reperfusion by stenting, persistent reperfusion with the addition of potent antiplatelet agents, and continued benefit of anti-adverse remodeling agents as well as other standard adjunctive agents (β-blockers) and statins, might make it difficult for any new adjunctive agent to show additional benefit. Another concern is that the optimal dosing of conditioning regimens is not known. 14 We do not know how many cycles and the duration of the cycles of blood pressure cuff inflation and deflation are required to optimally reduce infarct size. The follow-up time was 12 months. It is possible that this might have been too short a time to observe a benefit of remote conditioning on clinical outcomes. It is also possible that remote conditioning only works in the setting of larger myocardial infarctions. Perhaps, remote conditioning might have a benefit in situations where very early reperfusion with primary percutaneous coronary interventions are not available, such as in countries where only thrombolytic therapy is the mainstay of therapy. Another possibility is that preconditioning in animal models is more protective than the perconditioning that must occur in the clinical trials. At the present time, remote conditioning will not be used in the clinical situation of acute myocardial infarction. Perhaps, remote conditioning needs to be tested in clinical situations where the outcomes are not as good as they currently are with a usual acute myocardial infarction. There other potential applications of this relatively easy to use and potentially cost-effective therapy. There is now an entire literature emerging on the potential of applying remote conditioning to stroke therapy. 15 Another potential therapy is in the area of shock and the paragraphs below will describe what is known about the application of remote conditioning to this devastating condition.
Remote Conditioning in Shock States
There are several forms of shock. These include hemorrhagic shock due to blood loss, cardiogenic shock due to severe heart failure, and septic shock, due to infection. Experimental studies have been exploring the potential application of remote conditioning therapies to shock. The best studied of the effect of conditioning on shock are studies in hemorrhagic shock, followed by septic shock; and, there is a lack of studies regarding cardiogenic shock.
Hemorrhagic Shock
Hemorrhagic shock and blood resuscitation is recognized as a pathophysiologic process of total body global ischemia and reperfusion that causes damage to multiple organs, resulting in organ failure and, in some cases, death. The studies that are available to date that have investigated remote conditioning as a potential therapy have primarily been done in experimental animal models (Table 1). Leung et al used an acute hemorrhagic shock model in mice and reported that RIPC reduced the levels of inflammation and liver injury. They studied 2 levels of injury. In the first study of mild injury, mice were anesthetized with isoflurane and hemorrhagic shock was induced by withdrawing blood over a 15-minute period to lower mean arterial pressure to 30 mm Hg; hypotension was maintained for 1 hour and then mice were resuscitated with saline. In the RIPC group, one cycle of 10 minutes of left femoral artery occlusion was induced, followed by 10 minutes of reperfusion before initiating hemorrhagic shock. In the second study of severe injury, the duration of hypotension was maintained for 2 hours and RIPC was induced by performing 4 cycles of alternating 5 minutes of ischemia, followed by 5 minutes of reperfusion of the right lower extremity using an externally applied tourniquet. In both the mild injury and severe injury studies, RIPC induced lower levels of pro-inflammatory cytokines, reduced transaminase release from hepatocytes, and was associated with less histologic damage to the liver. Remote ischemic preconditioning also mitigated lung inflammation and injury and reduced systemic tumor necrosis factor (TNF)-α levels. 16
Hemorrhagic Shock.

Abbreviation: TNF-α, tumor necrosis factor α.
Hu et al showed that RIPC reduced myocardial and neurologic dysfunction and improved survival in rats after severe hemorrhagic shock and resuscitation. In this study, male rats were anesthetized with pentobarbital. The RIPC protocol consisted of 4 cycles of 5 minutes of limb ischemia, followed by reperfusion for 5 minutes. Hemorrhagic shock was induced by removing approximately 50% of the total blood volume over an hour. Shock was maintained for 30 minutes at a blood pressure of above 45 mm Hg. Shed blood was then returned to the rats over 30 minutes and the rats were observed for 72 hours. Blood pressure rapidly increased to near-baseline values during the resuscitation phase and was significantly greater in the RIPC group. Left ventricular ejection fraction, myocardial performance index, and sublingual microvascular flow index and perfused vessel density were significantly greater in the RIPC group than those in the control group at 2 hours after reperfusion. Survival at 72 hours was better in the RIPC group (7/7) than in the control group (1/7; P < .01). Neurologic testing revealed improved function in the RIPC group versus the control group. The benefits of RIPC were abolished by the KATP channel blocker, glibenclamide. The authors concluded that RIPC mitigated myocardial and neurologic dysfunction and improved survival by activation of the KATP channel. 17
In a recent study, our research group reported that RIPC markedly improved short-term survival benefit, which was maintained long term after resuscitation in a rat fixed pressure hemorrhagic shock model. Sprague-Dawley rats of both genders were anesthetized with intraperitoneal ketamine and xylazine. Prior to hemorrhagic shock, rats were randomized to RIPC or control. Remote ischemic preconditioning was induced by 4 cycles of inflating bilateral pressure cuffs around the femoral arteries to 200 mm Hg for 5 minutes, followed by 5 minutes release of the cuffs. In the control group, the cuffs were inflated to only 30 mm Hg. Hemorrhagic shock was induced by withdrawing blood from the carotid artery to a fixed mean blood pressure of 30 mm Hg and that pressure was maintained for 30 minutes. Heparinized shed blood was then reinfused and rats were allowed to recover for 6 weeks. Remote ischemic preconditioning significantly increased survival at 6 weeks: 5 (19%) of 27 rats survived in the control group, while 13 (50%) of 26 rats survived in the RIPC group (P = .02). Most of the deaths occurred within the first few days of resuscitation. During the first hour of resuscitation, blood pressure was improved in the RIPC group. By echocardiography, the diastolic internal dimension of the left ventricle was significantly larger in the RIPC group at 1 hour after initiation of resuscitation compared to the control group. This result suggests that there was more circulating intravascular blood volume in the RIPC group than the control group. At 48 hours, the liver injury indicated elevations of both aspartate transaminase and alanine transaminase, but there was no significant difference between the groups. Blood urea nitrogen was elevated in the control group, but not in the RIPC group. This study showed that if the rats survived for the first few days after an episode of hemorrhagic shock, they would survive long term. 18
Although, not practical as a therapy, one study by Tamion et al suggested that intestinal preconditioning prevented the inflammatory response associated with experimental hemorrhagic shock. In this study, RIPC was induced by repetitive brief occlusions and reperfusions of the mesenteric artery prior to inducing hemorrhagic shock in a rat model. Compared to sham treatment, remote ischemic intestinal preconditioning reduced fluid requirements, lung edema, lactate production, and levels of TNF-α. A heme oxygenase inhibitor abolished these beneficial effects. This study supports the concept that remote ischemic conditioning, even if performed in the mesenteric system, is protective against hemorrhagic shock and the mechanism may involve one of the known heat shock proteins, namely, heme oxygenase that appears to play a protective role. 19
Not all studies have been positive. Shaylor et al recently investigated the effects of RIPC in pigs that underwent hemorrhagic shock, but without resuscitation. They did not find any differences in mortality between an RIPC and control group. There were some major differences in the experimental approach compared to the previously reported rat studies. In this porcine study, the anesthesia regimen was complex with numerous agents used: diazepam, ketamine, propofol, tramadol, and isoflurane. Hemorrhagic shock was induced by removing 35% of the pig’s calculated blood volume over 30 to 60 minutes at a rate of bleeding to keep the mean arterial pressure from dropping below 30 mm Hg. Unlike the previously reported rat studies, there was no shed blood or other volume replacement given postbleeding. Survival at 7 hours was 50% (4/8 pigs) in both groups. 20 The discrepancy in the effects of RIPC on posthemorrhagic shock survival may have been related to the complex anesthetic regimen, the use of pigs, the use of fixed volume rather than fixed pressure model of shock, and, perhaps most importantly, the lack of postshock volume resuscitation.
The current clinical practice of the treatment of hemorrhagic shock includes early recognition, rapid control of the source of hemorrhage, fluid replacement using oxygen-carrying blood components including red blood cells, platelets, blood substitutes, hypertonic solutions, colloid solutions, and crystalloids. The goal is to limit the depth and duration of the shock state with fluid resuscitation before the level of shock becomes irreversible (meaning that even with volume replacement, the patient dies). The strategy of increasing tissue tolerance to hemorrhagic shock has remained largely unexplored. Animal experiments from our laboratory and other laboratories suggest that RIPC is a promising noninvasive intervention capable of improving survival, blood pressure in the early phase of resuscitation, and improving organ function. Remote ischemic preconditioning could be used in a prophylactic manner. For example, a soldier facing battle could self-protect against hemorrhagic shock, by simply inflating a blood pressure cuff above systolic pressure for 5 minutes, deflating the cuff for 5 minutes, and repeating these steps 3 or 4 times. Remote ischemic preconditioning can be thought of as a “vaccination” against the ischemia/reperfusion injury of hemorrhagic shock/resuscitation. To the best of our knowledge, a clinical study exploring the potential efficacy of RIPC has yet to be carried out.
The underlying mechanism of RIPC remains unknown. Review of these mechanisms remains beyond the scope of this article. However, previous papers have discussed the potential mechanism(s), 21 -24 which may include the production and release of a cardioprotective humoral factor into the blood stream by the organ receiving RIPC, that then protects other organs, certain neurogenic reflexes, the KATP channel, and others. Studies have shown that the transfer of venous or coronary effluent from a preconditioned organ is cardioprotective. Although the exact humoral substance that is released by the limbs that undergo brief cycles of ischemia and reperfusion is still being explored, some of the candidates that have been suggested include adenosine, 25 bradykinin, 26 opioids, 27 and nitrite. 28 A study of preconditioned isolated hearts suggested that the cardioprotective substances were hydrophobic peptides in the 4 to 12 kDa size range and were related to the PKC and KATP pathways. 29 The beneficial effect of humoral transfer from remote-ischemic-conditioned organs to other animals was blocked by inhibiting reperfusion injury salvage kinase or survivor-activating factor enhancement pathway. 23
There are unanswered questions regarding RIPC optimization to protect against hemorrhagic shock. The optimal dose and frequency of RIPC is not known. Would 10 inflations and deflations be superior to a few cycles? The timing of RIPC in relationship to the episode of shock could be an issue. In our experimental studies, the shock followed a few minutes after the last episode of limb ischemia/reperfusion and this was protective. Is it possible that the protection would still occur if RIPC occurred an hour prior to the severe ischemic insult? Is there a loss of protection if the separation between RIPC and the severe insult is greater than a few hours as is seen with standard ischemic conditioning; and is there then a second wave of protection that occurs at about 24 hours after the RIPC? How many times a week is RIPC necessary to protect an individual going out into battle? Are there certain anesthetic agents that interact with RIPC or may mask its benefit (this might have been the case in the porcine studies described above)? Hopefully, future research will answer these important questions.
Septic Shock
Septic shock is the condition whereby sepsis (infection that involves the blood) is associated with hypotension as well as perfusion abnormalities despite volume replacement. Septic shock remains a significant global health problem affecting thousands, if not millions, of individuals. Septic shock is associated with a high mortality, with up to 50% of cases of septic shock ending in death. 30,31 Septic shock is associated with multiple organ failure due to an uncontrolled inflammatory response throughout the body, ischemia/reperfusion events related to transient arterial hypotension, low cardiac output, compromised microcirculation, cellular hypoxia/reoxygenation, and mitochondrial dysfunction. 30,32 Vascular perfusion abnormalities are common with septic shock and may persist despite attempts to bring the blood pressure back toward normal levels with fluids, inotropes, and vasopressors. Septic shock is associated with lactic acidosis, oliguria, and alterations in mental status. Guidelines for the treatment of septic shock include control of the infection, fluid therapy, and vasoactive drugs. As is the case with hemorrhagic shock, there is little in the literature on attempts to better protect the organs themselves from the ischemia/reperfusion injury associated with hypotension, followed by fluid resuscitation (Table 2).
Septic Shock.
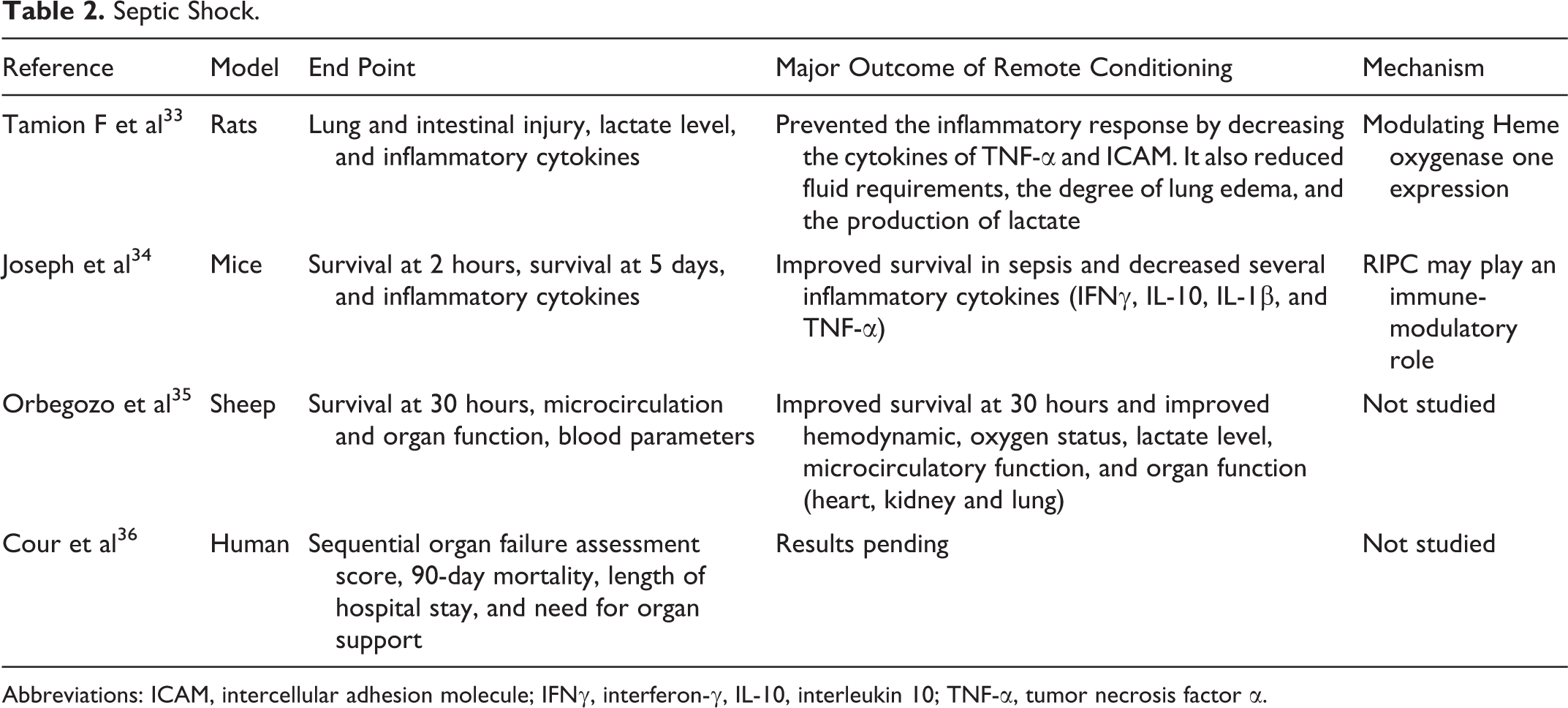
Abbreviations: ICAM, intercellular adhesion molecule; IFNγ, interferon-γ, IL-10, interleukin 10; TNF-α, tumor necrosis factor α.
A study from 2007 showed that intestinal preconditioning could prevent the inflammatory response associated with an endotoxin shock model. In this study performed in rats, preconditioning was induced by 4 cycles of 1 minute of mesenteric artery occlusion separated by 4 minutes of reperfusion. Twenty-four hours later, after preconditioning or sham surgery, endotoxic shock was induced by injecting lipopolysaccharide (derived from Escherichia coli) intravenously. Onset of endotoxic shock was defined as time when mean arterial pressure fell below 65 mm Hg. Fluid resuscitation was given to maintain mean arterial blood pressure and rats were monitored over a total of 6 hours. Preconditioning reduced fluid requirements, the degree of lung edema, production of lactate by the intestine, and histologic assessment of intestinal injury. Preconditioning reduced the expression of TNF-α and intercellular adhesion molecule in the intestine and lung. These benefits were blocked by a heme oxygenase—one inhibitor. 33
There are some experimental studies that suggest that remote ischemic conditioning of a limb may be a promising therapy for septic shock. Joseph et al studied mice with septic shock using a model in which the mice received an intraperitoneal injection of lipopolysaccharide to induce septic shock. Remote ischemic conditioning was induced by six 4-minute cycles of femoral artery clamping at 0, 2, and 6 hours after lipopolysaccharide injection. Survival at 5 days was higher in the remote ischemic conditioning group at 57% compared to a sham-treated group (21%; P = .02). The highest survival rate (70%) was observed in those rats that received remote conditioning at 2 hours after lipopolysaccharide injection, meaning that perconditioning worked. In addition, remote ischemic conditioning was associated with a fall in several inflammatory cytokines (interferon-γ, interleukin-10, interleukin-1β, and TNF-α) after a 2-hour peak. The authors concluded that remote ischemic conditioning improves survival in sepsis and may play an immune-modulatory role. 34
Orbegozo et al examined the effect of RIPC and remote ischemic postconditioning (RIPoC) on septic shock in a sheep model. Sepsis was induced by injecting autologous feces into the abdominal aorta of sheep. The sheep were randomized to ischemic pre- and postconditioning or no conditioning. Both RIPC and RIPoC were achieved by inflating a balloon catheter into the aortic bifurcation for 2 minutes followed by 4 minutes of deflation and the procedure was performed 4 times before sepsis induction (RICP) and 4 hours afterward (RIPoC). The sheep were then followed for up to 30 hours. The investigators monitored hemodynamics, oxygen status, and measures of microcirculatory function. The conditioning group had higher mixed venous oxygen saturation, cardiac index, mean arterial blood pressure, and lower lactate levels compared to the nonconditioned control group. The median proportion of perfused blood vessels was improved and there was less heterogeneity of perfusion in the conditioned group. Death, hypotension, and oliguria occurred later in the conditioned group than in the control group. The authors concluded that RIPC and RIPoC prolonged survival, preserved organ function, and preserved the microcirculation. 35
There is an ongoing clinical trial that will be looking at the issue of whether remote ischemic conditioning has benefits. The clinical trial is called remote ischemic conditioning (RECO). It is a prospective, multicenter, randomized, open-label trial. Eligible patients are adults admitted to an intensive care unit with documented or suspected infection, lactatemia, and treated with norepinephrine for less than 12 hours. Patients are then randomized to remote conditioning or no conditioning. The remote ischemic conditioning protocol consists of 4 cycles of blood pressure cuff inflation to 200 mm Hg for 5 minutes, followed by deflation for 5 minutes. The conditioning protocol is performed on enrollment and then at 12 and 24 hours later. The primary end point is the Sequential Organ Failure Assessment score; secondary end points are 90-day mortality, length of hospital stay, and need for organ support. This will be an important trial as it may answer for the first time whether remote conditioning can play a role in improving outcomes in patients who are experiencing septic shock; a disease that is very difficult to treat. 36
Cardiogenic Shock
Cardiogenic shock is a severe life-threatening condition of acute heart failure and hypotension associated with complex physiologic alterations. Mortality remains very high at 25% to 50%. 37 -39 Since cardiogenic shock is characterized by a low cardiac output state of circulatory failure that results in end-organ ischemia and hypoxia, one could speculate that remote ischemic conditioning may have the potential to be organ protective.
However, there is a lack of data on the issue of whether remote conditioning can reduce cardiogenic shock. If remote conditioning truly reduces infarct size, then theoretically it should be able to reduce cardiogenic shock. However, as described above, the recent large multicenter trial failed to show that RIPC had any benefit on infarct size or clinical outcome. The control group in this study had a very low mortality rate at 1 year; so it may be that if the patients were at higher risk, with larger infarcts in the controls, with a higher baseline mortality rate, that remote conditioning might be beneficial. Until a group of patients with higher risk, larger infarcts in the control group, access perhaps to only thrombolytic therapy but not primary percutaneous coronary intervention, are studied; it is unlikely that remote conditioning will be studied in a population of patients with cardiogenic shock with STEMI.
Conclusions
A recent large multicenter study has dampened the enthusiasm for the treatment of acute myocardial infarction with remote conditioning. Current accepted therapies including early reperfusion have been so successful that it may be difficult to show that any new adjunctive therapy, including remote conditioning, further improves outcome of acute myocardial infarction. Outcomes for shock states, however, remain poor. There are now several preclinical studies suggesting that remote ischemic conditioning (either pre, per, or post) may improve survival and organ function associated with shock states, such as hemorrhagic shock or septic shock. There has yet to be an analysis of the role of remote conditioning in the treatment of cardiogenic shock. An ongoing clinical trial is examining the potential efficacy of remote ischemic perconditioning on the clinical outcomes of septic shock. There are not yet clinical trials studying the effect of remote conditioning for hemorrhagic shock. In that situation, RIPC could be applied prophylactically to the soldier who was heading into battle.
Footnotes
Author Contribution
All coauthors contributed to the writing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Peer Reviewed Medical Research Program under Award No.W81XWH-16-1-0606.