
Abstract
Remote ischemic conditioning (RIC) is at a pivotal point in its evolution, both in terms of its adoption as a therapy and its viability commercially. The most usual way of inducing RIC, with a standard blood pressure cuff and a stopwatch, is time-consuming and potentially inaccurate and unsafe. Development of automated devices have facilitated large-scale randomized trials and will make clinical deployment of the technique more straightforward. Both the medical and commercial future of RIC will depend on the results of upcoming phase 3 pivotal trials.
Introduction
The ultimate goal of biomedical research must be to translate discovery into patient care. This inevitably requires that significant hurdles be overcome. Fundamentally, all practice change in health care must be driven by strong mechanistic science followed by translation from bench to bedside via phased clinical trials, culminating in large multicenter trials designed to prove a measurable benefit of the innovative treatment on hard clinical end points. Although these are necessary steps, they represent only 1 component of the path of a new therapy becoming accepted into clinical care. Equally important steps on this path, albeit less predictable, are the need for spreading clinical awareness, adoption, and commercialization. These are rarely at the forefront of the minds of either the scientist or clinician, but in today’s complex and fiscally driven health-care environment, the need for successful navigation of the regulatory and commercial landscape cannot be overemphasized. In this review, we will discuss some of the opportunities and challenges as they relate to remote ischemic conditioning (RIC), a therapy that is in the early stages of adoption and commercialization.
Possible Areas of Clinical Application
The phenomenon of ischemic preconditioning was first described in the heart, 1 and cardioprotection has been the main thrust of many of the seminal developments in the field. 2 The benefits of ischemic conditioning are not restricted to the myocardium; however, as virtually all tissues possess protective pathways that can be induced by local or remote conditioning stimuli. For example, RIC induced by transient limb ischemia 3 has been shown to provide protection in animal models of brain injury, 4,5 renal injury, 6 liver injury, 7 soft tissue and skeletal muscle injury, 8 and even more nebulous insults such as sepsis. 9 Furthermore, proof of principal clinical data exists or being gathered in many of these areas: there are 178 ongoing or completed studies in almost 38 000 patients registered on ClinicalTrials.Gov investigating the potential efficacy of RIC in a wide range of clinical scenarios. Despite this broad promise, the cardiovascular arena remains the most advanced in imminent clinical relevance. Unsurprisingly, given their direct correlation with the consistently demonstrable benefits of RIC in acute ischemia reperfusion injury models in animals, 3 the clinical data supporting the use of RIC in elective coronary angioplasty 10 –13 and percutaneous coronary intervention (PCI) for evolving myocardial infarction 14 –20 are the most robust. The data are less strong, but equally intriguing, for acute neuroprotection in embolic stroke 21 and, perhaps unexpectedly, acute renal protection against contrast-induced nephropathy. 22,23 Beyond these acute effects, there are emerging data supporting the use of repeated RIC to reduce remodeling and heart failure 24 –26 in the aftermath or myocardial infarction and as a therapeutic adjunct to recovery after stroke. 27,28 The current state of the science for many of these indications is discussed elsewhere in this issue, but it is fair to say that clinical adoption, even where the available data are overwhelmingly positive, has been slow. What then, are the barriers to, and opportunities for, RIC to becoming a standard of care treatment?
Adoption of RIC in the Clinic
The Rogers bell-shaped adoption curve for new innovations 29 is well known to many and has been shown to be remarkably consistent across different medical therapies and procedures. Even when readily available, new therapies typically build early adoption more slowly in the first months or years and then grow as the early majority begin to use the intervention, achieving widespread use when joined by the late majority (Figure 1).
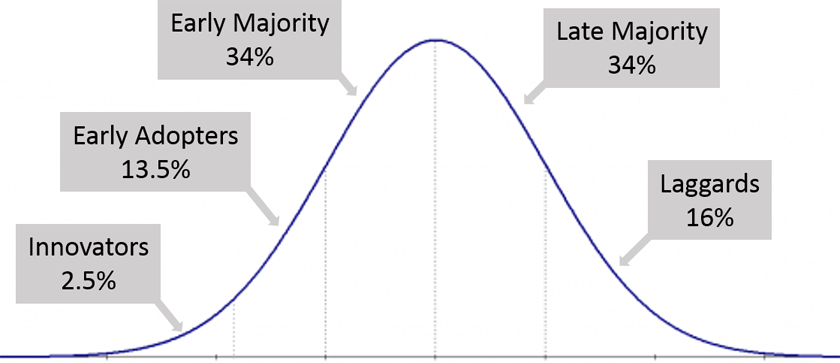
The Rogers adoption curve for innovative procedures (modified and redrawn from original 29 ).
The interplay of factors driving adoption is complex, and a detailed analysis is beyond the scope of this article. Today, RIC remains toward the left-hand side of the adoption curve even in areas where most, if not all, of the clinical trial data are positive—such as for RIC therapy as an adjunct to PCI in evolving myocardial infarction. For RIC to move into practice beyond the early adopters, there needs to be a device, specifically designed to deliver RIC, clinical data of sufficient impact on outcomes and health-care economics to warrant inclusion of RIC into standard practice, and regulatory clearance to facilitate commercial availability.
Although the process of RIC is simple, safe, and straightforward, delivering it using a blood pressure (BP) cuff and stopwatch—as has been done in many research trials—is burdensome and expensive. Consequently, many of the contemporary large-scale trials being performed are using an automated device. The “standard” RIC protocol, in use in most trials, consists of 4 cycles of 5 minutes of limb ischemia (cuff inflation to 200 mm Hg) followed by 5 minutes of reperfusion. Consequently, in the absence of an automated device, 40 to 45 minutes of a practitioner’s time is required to prepare and deliver the therapy. In a busy cardiac catheterization laboratory, or emergency department for example, this might require an additional full-time equivalent to deliver the stimulus to every patient prior to their procedure. Furthermore, concerns regarding accuracy and safety (eg, leaving the cuff inflated in an anesthetized or obtunded patient) add logistic barriers to routine use of a manual BP monitor for RIC. Aside from patient safety, this raises concerns regarding litigation around the use of a device in an off-label manner. The availability of an automated, approved device for RIC will largely overcome these issues. The only automated device widely available to deliver RIC (the autoRIC device, CellAegis Devices, Toronto, Canada) essentially reproduces the manual method but automates cuff inflations (to 200 mm Hg), cycle number, and duration. To date, it has been restricted to research use (a “sham” inflation protocol device is available); nevertheless, its availability has facilitated large scale multicenter randomized controlled trials 30,31 that otherwise would have been financially nonviable if RIC had to be delivered by a cadre of research nurses. Similarly, one can anticipate clinical adoption being facilitated once such specifically designed devices become available for the widespread use.
Beyond the availability of an automated RIC device, the rightward shift of the adoption curve will occur when a persuasive body of evidence allays the skepticism of the majority. Some data already exist, such as improved survival at 5 years in RIC-treated patients with evolving myocardial infarction 15 and reduced overall health-care costs, 32 but it is fair to say that the field awaits the results of adequately powered multicenter randomized trials and regulatory clearance or approvals. As mentioned above, these are on the way, and 2 large multicenter trials (enrolling over 4300 patients) are being performed in Europe, examining a composite end point of cardiac death and hospitalization for heart failure at 12 months after PCI for evolving myocardial infarction. 30,31 In the interim, skeptics cite the 2 recent large scale in cardiac surgery 33,34 as fundamentally undermining the clinical utility of conditioning strategies as a whole. The fact that they were neutral, despite a large body of proof-of-principle trials showing promise, clearly cannot be ignored. The veracity of these trials, and their implications for the use of RIC in cardiac surgical patients is discussed elsewhere, but the collateral impact upon the entire field of cardioprotection has not been negligible. Irrespective of one’s opinion regarding the potential use of remote conditioning in cardiac surgery, the fundamental differences between organ dysfunction as a result of cardiopulmonary bypass versus the discrete injury associated with other ischemia reperfusion syndromes (such as evolving myocardial infarction and stroke) are sometimes ignored in this argument.
Even against the background of neutral results in cardiac surgery, positive clinical outcomes in the large evolving myocardial infarction trials can reasonably be expected to result in integration of RIC into clinical protocols, as well as inclusion in national and international guidelines, both of which would result in new technique becoming established as a standard of care. Although RIC’s benefit in cardiac surgery may remain controversial for some time, from a commercialization viewpoint, cardiac surgery represents less than 10% of the potential acute market for RIC and so is relatively inconsequential in terms of the viability of an emerging product.
Commercial availability of an automated RIC device and positive data from large multicenter trials will therefore potentially shift the adoption curve rightward. But these are not the only requirements for commercialization and adoption of health-care innovation: unsaid so far and mostly not in the minds of clinicians, significant amounts of capital are required to develop the equipment, conduct clinical trials, achieve regulatory clearance, and commercialize innovative medical devices. In order to raise capital, companies must usually convince venture capitalists or other investors that their product is clinically beneficial and commercially viable, well before multicenter trials have been completed. Still further, commercial viability requires country-specific regulatory approvals, 35 demonstration of intellectual property protection, and supply chain of product to enable investment worthy margins. In the United States, average cost to bring a low-to-moderate risk 510(k) product from concept to market is US$31 million with more than 77% of that, US$24 million, spent on Food and Drug Administration–dependent or –related activities. 36 This can be prohibitive for small start-up companies, and it is well known that many viable treatments fail to enter clinical use, because of the cost-to-market issues, rather than clinical viability. Demonstration of product cost-effectiveness is therefore not only important to facilitate clinical uptake but also to secure the capital investment required to bring that product to market. Remote ischemic conditioning treatment has already shown cost savings of approximately 20% (€2900 per ST segment elevation myocardial infarction patient) in the Danish health-care system, 32 which reduces the business risk for investors, increases the likelihood of bringing the product to market, and also provides the business reason for health-care systems to adopt a clinically effective therapy. The cost savings in the US health-care market are likely to be much larger.
In summary, RIC is at a critical point in its evolution both in terms of its clinical impact and its commercial viability. Each is dependent on the other, large-scale clinical trials will be difficult to perform without RIC delivery devices, and those devices will only be commercially viable if meaningful clinical benefit can be demonstrated. The next 2 or 3 years will be pivotal and will define whether RIC is confined to the history of exciting experimental innovation that fails to translate into clinical practice, or whether that excitement will prove to be warranted as the technique becomes an important adjunct to our armamentarium for the acute and chronic treatment of ischemia–reperfusion syndromes.
Footnotes
Authors’ Contribution
Andrew Redington, Vera Belaoussoff, and Rocky Ganske contributed to writing and review of this article and are responsible for its content equally.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Andrew Redington, Vera Belaoussoff, and Rocky Ganske are all significant shareholders in CellAegis, a company developing an automated preconditioning device.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.