
Abstract
Purpose:
There is a lack of knowledge on the effects of nitrates alone in heart failure (HF). We aimed to assess the impact of nitrates use in the occurrence of ischemic events in patients with ischemic HF attending an HF clinic.
Methods:
We performed a retrospective analysis of a cohort of 632 patients managed in an HF clinic between January 2000 and December 2011. Patients with ischemic etiology were selected (n = 290). Patients were classified according to chronic nitrates use (n = 83 nitrates users vs n = 194) and followed up for 5 years for the occurrence of fatal or nonfatal myocardial infarction or stroke.
Results:
Nitrates users had more frequently diabetes, dyslipidemia, and higher body mass index but were less frequently treated with statins. Thirty adverse events were recorded (n = 16 in nitrates group). Variables significantly associated with the occurrence of the end point in univariate analysis were arterial hypertension, diabetes, and nitrates use. Male gender, beta-blockers, statin, and clopidogrel use had a protective effect on the occurrence of the end point. In multivariate analysis, nitrates use remained an independent predictor of adverse outcome when adjusted for each of the variables: arterial hypertension, gender, diabetes, beta-blocker, and clopidogrel use; however, when adjusted for statin use, nitrates were no longer associated with the outcome.
Conclusion:
Long-term nitrates use in patients with ischemic HF was associated with higher occurrence of ischemic events, defined as fatal or nonfatal myocardial infarction or stroke. Our results, although from a retrospective analysis, do not support a role for chronic nitrate use in HF.
Introduction
Nitrates are one of the classical drugs that have been widely used for cardiovascular diseases. They act via nitric oxide signaling pathways and exert endothelium-independent vasodilation, leading to an increase in coronary perfusion and reduction in cardiac pre- and postload. 1 Nitrates acutely improve cardiac conditions such as angina attacks and acute heart failure (HF); nevertheless, its long-term effects have been controversial. 1,2 Data from the Grace registry on acute coronary syndrome suggested that long-term therapy with nitrates is beneficial in this setting. 3 On the other hand, multivariate analysis data from large nonrandomized studies suggested that long-term nitrate use in ischemic heart disease may increase acute coronary syndromes, thus worsening prognosis. 4,5 Recently, a multicenter study by the Japanese Coronary Spasm Association demonstrated that chronic nitrate therapy did not improve the prognosis of patients with vasospastic angina and could rather be correlated with poor outcome. 6 The chronic exposure to nitrates seems to result in a rapid development of tolerance, blunting their anti-ischemic and hemodynamic efficacy. 1 –7 Furthermore, they can cause potential harm to cardiovascular patients by the generation of reactive oxygen species with resultant endothelial dysfunction; sympathetic nerve activation and increase in sensitivity to vasoconstrictors have also been suggested. 8 –16 Previous studies documented benefits of combining nitrate therapy with hydralazine in chronic HF (CHF) 12 –15,17,18 ; however, this combined therapy is underused for several reasons. 14 Also, some authors suggest that angiotensin-converting enzyme (ACE) inhibitors, as vasodilators and as holders of antioxidant properties, prevent nitrate tolerance and may facilitate nitrate use in CHF. 14,15 The paucity and conflicting results of data on nitrates use in HF is in contrast to its widespread use in clinical practice. 19 Therefore, more information is needed in order to clarify the role of isolate nitrate therapy in HF, particularly in the vulnerable group of patients with ischemic HF.
The aim of this study was to assess the impact of nitrates use in the occurrence of ischemic events in patients with ischemic HF attending an HF clinic.
Methods
Study Population
We performed a retrospective analysis of a cohort of 632 adult patients followed in an HF clinic at a public academic tertiary care hospital in Portugal. We screened files of patients consecutively referred to the clinic from January of 2000 to December 2011.
Patients with ischemic HF (n = 290; 45.9% of the whole sample of patients) were selected for analysis. Ischemic etiology was defined as previous myocardial infarction, angiographic stenotic lesions >70%, or moderate and severe perfusion defect on myocardial perfusion scintigraphy.
Medical Treatments
Patients with ischemic HF were classified according to chronic nitrates use, defined as isosorbide mononitrate or dinitrate or nitroglycerin being prescribed in the first 2 visits (n = 83, 29%).
End Points
Patients were followed up for 5 years for the occurrence of fatal or nonfatal myocardial infarction or stroke.
Statistical Analysis
Data storage and statistic analysis were made using SPSS statistics 22 software. Continuous variables are presented as medians and interquartile ranges (IQRs). Patients were divided in 2 groups according to nitrates use. Demographic data, medical comorbidities, medication use, clinical, and echocardiographic characteristics were compared using the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables. Survival analysis was performed using Cox regression and Kaplan-Meier curves. A p value < .05 was considered to be statistically significant.
Results
Among the 632 patients managed in the HF clinic during January 1, 2000, and December 31, 2011, 342 had nonischemic etiology and were excluded from further analysis. Of the remaining 290 with ischemic HF, 83 (29%) used nitrates chronically according to the study definition; all had intermittent administration; 23 patients were under nitroglycerin (transdermal route), 52 were under isosorbide mononitrate (oral route) and 8 under isosorbide dinitrate (oral route).
The demographic characteristics, New York Heart Association class (NYHA), grade of ventricular systolic dysfunction, and medical treatments of our sample are presented on Table 1. Nitrates users group had higher prevalence of diabetes and dyslipidemia and higher body mass index (BMI), but they were less frequently on statin therapy.
Patients Demographics, HF Data, and Comorbidities According to Nitrates Use Group.

Abbreviation: BMI, body mass index; NYHA class: New York Heart Association functional classification; ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; IQR, interquartile range.
ap < .05.
Thirty adverse events were recorded (16 in nitrates group [11 nonfatal myocardial infarctions, 4 strokes, 1 death—fatal myocardial infarction] and 14 in the other group [10 nonfatal myocardial infarctions, 2 strokes, 2 deaths—1 fatal myocardial infarction and 1 fatal stroke]; p = .002).
Ten patients died of other causes: 2 in the nitrates group (1 during aortic valve replacement surgery and 1 of septic shock) and 8 in the other group (1 of sudden death, 1 of pump failure, and 6 of septic shock).
A survival analysis using Kaplan-Meier curves was performed, showing significantly worse outcome in patients who were taking nitrates (Figure 1). Table 2 shows the univariate Cox regression analysis. The variables significantly associated with the occurrence of the end point in univariate Cox regression analysis were arterial hypertension, diabetes mellitus, and nitrates use. Male gender, beta-blockers, statin, and clopidogrel use had a protective effect on the occurrence of the end point. Age was not associated with the occurrence of the end point (hazard ratio [HR] 1.01; 95% confidence interval [CI]: 0.98-10.04; p = 1.01). When adjusted for each of those variables with prognostic significance in the univariate analysis, nitrates use remained an independent predictor of occurrence of adverse events (HR = 2.58 [CI: 1.26-5.29]; p = .01) when adjusted for arterial hypertension (HR = 2.41 [CI: 1.16-4.98]; p = .018), when adjusted for gender (HR 2.72 [CI: 1.33-5.58] p = .006), when adjusted for diabetes mellitus (HR = 2.23 [CI: 1.07-4.64]; p = .032), when adjusted for beta-blocker use (HR = 2.48 [CI: 1.2-5.08], p = .013), and when adjusted for clopidogrel use. However, when adjusted for statin use, nitrates were no longer independently associated with the outcome.
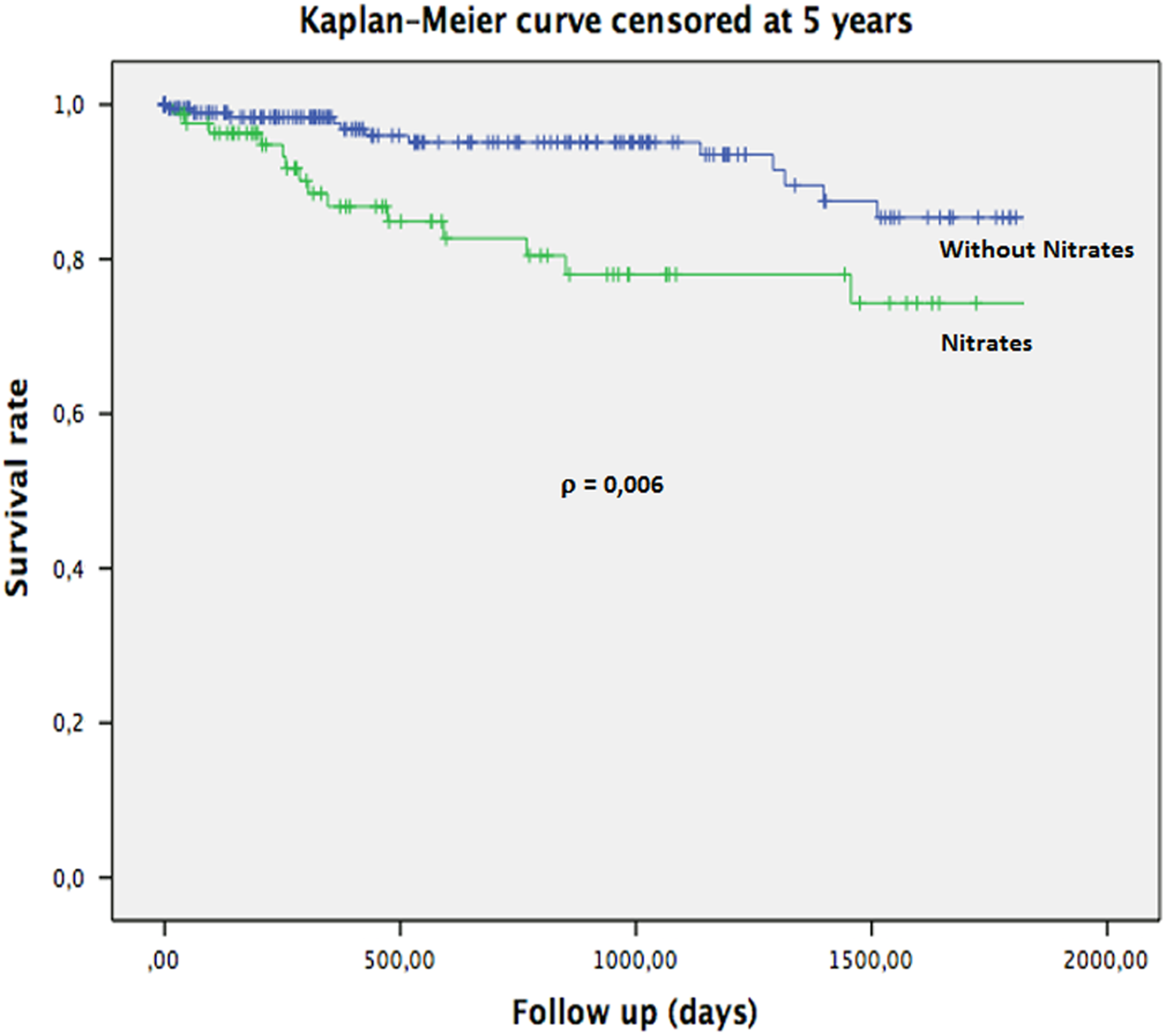
Kaplan-Meier curve showing event-free survival according to nitrates use group.
Univariate Analysis Identifying Predictors of Adverse Events.

Abbreviation: BMI, body mass index; ACE inhibitor, angiotensin-converting enzyme inhibitor.
ap < .05.
Discussion
The findings of the present study suggest that chronic nitrate therapy is associated with the occurrence of adverse vascular events (fatal or nonfatal myocardial infarction and stroke). These results, although obtained in a retrospective analysis, question the frequent use of nitrates alone in ischemic HF.
Although data on the effects of isolate nitrates use in HF is scarce, the negative impact of chronic nitrate therapy on prognosis demonstrated in this study is in accordance with previous reports. 2,5,6 In one of these studies, Nakamura et al showed that chronic nitrates therapy was associated with all-cause mortality in 2821 postmyocardial infarction patients. Farag et al conducted a systematic review of randomized trials. 19 There were 19 studies with a total of 589 patients, evaluating nitrates alone in CHF; 10 of those studies compared nitrates to placebo. Most patients were men and had moderate to severe CHF, as in our patient sample, and etiology was ischemic heart disease in about 77% of patients. The meta-analysis of the studies that reported mortality and compared nitrates to placebo showed no significant effect of nitrates on all-cause mortality. However, there were few events in these studies and the trend was toward harm. 19
Several reasons can be evoked to explain the worse prognosis in patients on chronic nitrates therapy. The mechanisms include the rapid development of tolerance 1 and the induction of endothelial dysfunction and cardiac autonomic dysfunction. 7 –10 These mechanisms could have been implicated in the occurrence of more ischemic heart and cerebral events in our patients using nitrates chronically.
Another possible reason for the worse prognosis of nitrates users could be the presence of a more severe degree of coronary/cerebral atherosclerotic disease, as they had increased prevalence of some coronary risk factors (diabetes mellitus, dyslipidemia and higher BMI); although this hypothesis was not analyzed in this study, as we had no data on coronary angiography or carotid ultrasound, nitrate use was associated with the occurrence of ischemic events, independently of the presence of diabetes or dyslipidemia. Besides, a nitrates prescription might be related to persistence of angina symptoms, thereby reflecting more severe coronary artery disease which would have a negative prognostic impact related to the severity of the disease by itself.
Ambrosio et al conducted a subanalysis of Study of the Effects of Nebivolol Intervention on Outcomes and Hospitalisation in Seniors with Heart Failure (SENIORS) and demonstrated that treatment with nebivolol can provide additional benefits besides its effects on HF, by reducing cardiac ischemic events in patients with ischemic HF. 20 In our cohort, there were no statistically significant differences in beta-blocker prescription between nitrates group and the other group. On univariate analysis, beta-blocker use was identified as predictor of favorable outcome (Table 2). When multivariate analysis was performed, nitrates use remained an independent predictor of occurrence of adverse events, when adjusted for beta-blocker use.
The negative impact of nitrates on the prognosis is lost when adjusted to statins. A possible explanation to this finding is that patients in the nitrates group, in spite of being more frequently dyslipidemic (78.3% vs 61.4%, p = .006), had less statin prescribed (65% vs 76.3%, p = .036). Statins use in patients with HF has been challenged by the results of 2 large randomized controlled trials ([The Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico - HF trial (GISSI-HF) 21 and the Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA) 22 ]), which demonstrated that rosuvastatin had neutral effects on long-term outcomes in patients with systolic HF with or without coronary artery disease. These studies might have influenced the prescription of statins in our cohort. It seems that in our sample of patients with ischemic HF, the use of statins might have had a protective effect in the occurrence of a ischemic event. In fact, in the CORONA study, patients in the rosuvastatin group had a trend to less ischemic events (myocardial infarction and stroke).
Study Limitations
Several limitations should be mentioned for our study. First, its observational and retrospective nature. Second, the management decision wether to prescribe nitrates was left to the discretion of each individual physician. Although patients prescribed long-term nitrate therapy were likely a group of patients with more angina symptoms, more severe coronary artery disease, not accessible percutaneous or surgically, this data was not collected. Third, nitrates use was defined as nitrates being prescribed in the first 2 clinic visits, and compliance or therapeutic changes during follow-up were not evaluated. Fourth, as in the other studies, the number of events was limited.
Conclusion
Long-term nitrates use in patients with ischemic HF was associated with higher occurrence of ischemic events, defined as fatal or nonfatal myocardial infarction or stroke, questioning the role of chronic nitrate alone use in HF.
Although the retrospective design of the study precludes the establishment of a firm causal relationship, our results provide a rationale and background for a randomized trial to validate our observations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joana Pimenta receives consultancy payments and payments for lectures from Bayer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.