
Abstract
Myocardial infarction results from a blockage of a major coronary artery that shuts the delivery of oxygen and nutrients to a region of the myocardium, leading to massive cardiomyocytes death and regression of microvasculature. Growth factor and cell delivery methods have been attempted to revascularize the ischemic myocardium and prevent further cell death. Implantable cardiac tissue patches were engineered to directly revascularize as well as remuscularize the affected muscle. However, inadequate vascularization in vitro and in vivo limits the efficacy of these new treatment options. Breakthroughs in cardiac tissue vascularization will profoundly impact ischemic heart therapies. In this review, we discuss the full spectrum of vascularization approaches ranging from biological angiogenesis to microfluidic blood vessels as related to cardiac tissue engineering.
Introduction
Vascularization is one of the greatest challenges in tissue engineering, especially in cardiac tissue engineering. The high-metabolic rate of cardiomyocytes (CMs) is reflected by the capillary density in the heart; almost every CM neighbors a capillary to facilitate efficient mass transfer. 1 Initial vascularization solutions stemmed from biological methods (ie, growth factor [GF] delivery, gene therapy, cell therapy, etc). These methods attempt to stimulate endogenous blood vessels to grow into the infarcted myocardium, reducing the expansion of the infarct and improving heart function 2 -5 but with limited efficacy.
Engineered cardiac patches have been applied to the ischemic rat heart. The improved function through simultaneous remuscularization and protective paracrine signaling provided by cardiac patches was encouraging. However, further progress toward clinical translation requires achieving adequate vascularization, vascular integration, and tissue engraftment. Vascularization is crucial in 2 respects: (1) without a functional and mature prevascular network in vitro, thick (∼1 cm) physiologically relevant 3-dimensional (3D) cardiac tissue cannot be cultivated and (2) successful integration with the host will depend on rapid initial vascular anastomosis and long-term integration with the host vasculature.
Engineering-based solutions have begun to solve these limitations. Initially, through controlling vascular signaling pathways or cellular interactions to promote angiogenesis, blood vessels were allowed to innately self-assemble. However, as modern microfabrication techniques and biomaterial science advance, direct assembly of engineered blood vessels from single cells is beginning to show intriguing promise. Boundaries between biological and engineering strategies have begun to converge as recent approaches partially utilize microfabrication methods to help guide the natural assembly of blood vessels. For a comprehensive review of clinical trials focused on cardiac cell therapy, GFs, and biomaterial delivery, please focus on the following reviews. 6 -9 In this review, therapeutic cardiac vascularization strategies ranging from biological aspects of angiogenesis to recent engineered designs for growing microvasculature are highlighted, with a focus on cardiac tissue engineering (Figure 1).

Strategies for revascularization of damaged myocardium and vascularizing engineered cardiac tissues based on biological and engineering approaches. Depiction of current methods used to both directly vascularize native damaged myocardium (growth factor/gene therapy/microRNA, cell therapy, and bioactive scaffold) and to vascularize engineered cardiac tissue constructs (prevascularization, modular tissue assembly, guided tubulogenesis, and microfluidic blood vessels). Vascularization methods are listed in order of increasing applied engineered guidance. The dark arrows in the flow diagrams indicate the sequential steps involved in each strategy as well as the physical and biological effect generated with each strategy. The text box at the right end of the figure indicates the final step, which is also the final objective of each method.
Growth Factor and Gene Therapies
Growth Factor, Gene, and RNA Therapy
Numerous clinical studies have been initiated based on GF delivery, gene therapy, and cell-based therapy to promote myocardial angiogenesis and post-myocardial infarction (MI) healing. However, there is still no general consensus from clinical trials whether GF delivery or gene therapy trials are beneficial for treating ischemic myocardium. It is well established that the delivery of angiogenic GFs can promote the vascularity of ischemic myocardium. However, there are several limiting factors to this approach. For example, the delivery of an angiogenic GF such as vascular endothelial GF (VEGF) can result in vasculature that is highly disorganized and leaky. 10 Furthermore, localization, complex pharmacokinetics, and the high cost to maintain GF levels further limit the approach. It seems unlikely that the process of endogenous endothelial repair alone could regenerate a major infarct like myocardial scar tissue. 11
Consequently, several gene therapy approaches (plasmid DNA, adenovirus, adenoassociated virus) attempted to deliver VEGF-coding DNA to the myocardium using endogenous cells. 12 These approaches had low in vivo transfection rate, short-term expression levels, and uncertain efficacy of the expressed protein. 13 To overcome these limitations and gain benefits from paracrine factors secreted by progenitor cells, Melly et al developed a novel high-throughput fluorescence-activated cell sorting method for selecting transduced myoblast progenitors with well-defined VEGF expression levels. 14 Intramyocardial injection of transduced and sorted adipose tissue-derived stem cells into an ischemic heart promoted controlled angiogenesis and improved heart function. 14 Using a similar approach, Marsano et al found that ischemic heart contractility improved when 1-mm thick elastomeric patches, seeded with sorted VEGF-transduced myoblasts, were applied. The intrinsic vascularization potential of the transduced myoblasts improved engraftment by inducing normal angiogenesis in the myocardium and within the construct. 15
A relatively new branch of research focuses on manipulating endogenous noncoding RNAs (∼22 nucleotides) known as microRNAs to direct myocardial angiogenesis. 16 Zangi et al synthesized a modified RNA (modRNA) that encoded human VEGF-A. 17 Intramyocardial injection of the modRNA into infarcted rat hearts (time = 0) produced an optimal “pulse” of VEGF. After 1 week, nonleaky vasculature in the peri-infarct region was primarily attributed to the improved heart function and by the enhanced paracrine signaling. Additionally, epicardium-derived cells migrated into the myocardium and differentiated into endothelial cells (ECs). However, the low occurrence rate of this latter scenario likely precluded it from significantly contributing to the improved state of the myocardium. RNA therapy appears to be an attractive approach due to several reasons: (1) no genetic manipulation is required, (2) a localized region can be targeted, (3) the influence on gene regulation can be timed, and (4) high transfection rates can be achieved. 17
Bioactive Scaffolds and Hydrogels
Porous collagen scaffolds 18 and decellularized porcine myocardial matrix 19 can induce angiogenesis when placed on the myocardium. Hao et al used alginate to differentially release VEGF and platelet-derived growth factor BB to promote the growth of mature vessels and improved systolic function. 20 The nanofibrous microenvironments created by the self-assembling peptide AcN-RARADADARARADADA-CNH2 promoted the recruitment of vascular cells (VCs) and promoted CM survival. 21 A heparin-binding domain sequence (LRKKLGKA) was later added to the self-assembling peptide and used to sustainably deliver VEGF for up to 1 month resulting in improved angiogenesis and heart function. 22 Zhang et al engineered a VEGF protein that incorporated a collagen-binding domain (CBD). 23 When CBD-VEGF was either intramyocardially injected (where it was retained within the cardiac extracellular matrix) 23 or loaded in a collagen patch and applied to the myocardium, 24 there was a decrease in the scar size and an increase in the vascular density compared to the native VEGF group. Ruvinov et al developed an injectable alginate sulfate in situ forming hydrogel capable of controlling hepatocyte GF (HGF) delivery via affinity binding. 25 The alginate hydrogel was shown to extend the half-life of the bound HGF and improve CM cell culture survival. Delivery of the HGF loaded hydrogel post-MI resulted in significantly improved angiogenesis. They then used differential affinity-binding kinetics to deliver both HGF and insulin-like GF (IGF) to produce release profiles. 26 An injection into rat post-MI improved vascularization, decreased cell apoptosis, and increased GATA-4 expression, resulting in a thicker scar with less fibrosis.
We developed a collagen–chitosan hydrogel for the controlled release of the angiogenic and cardioprotective thymosin β4 (Tβ4). 27 The Tβ4 encapsulated gel induced the recruitment and differentiation of both ECs and smooth muscle cells (SMCs) in epicardial capillary outgrowths in vitro and augmented angiogenesis in a subcutaneous injection in vivo. 27 Subsequently, we administered intramyocardial injections of this hydrogel to infarcted rat hearts in order to achieve sustained Tβ4 release and lower the applied doses. 28 We found a significant reduction in viable tissue loss and maintenance of wall thickness in the group that was treated with collagen–chitosan hydrogel containing Tβ4. These improvements were positively correlated with the blood vessel density. In a study combining human embryonic stem cells (hESCs), vascular-like cells, Tβ4, and a biomimetic polyethylene glycol matrix metalloproteinase-sensitive scaffold, angiogenesis and improved ejection fraction 6 weeks post-MI were induced by paracrine signaling. 29
The biological activity of GFs can be augmented by covalently immobilizing them onto a biomaterial. 30 We showed that implanted collagen scaffolds with covalently immobilized VEGF and angiopoietin 1 can improve H5V EC proliferation in vitro, increase EC infiltration in the chorioallantoic membrane assay, 31 and promote tube formation of primary rat aortic ECs. 32 We next attempted to repair an intramyocardial defect using a collagen patch with immobilized VEGF165 and seeded with bone marrow cells. 33 After 28 days, improved angiogenesis and patch thickness was observed. We have also coimmobilized VEGF and basic fibroblast GF (FGF) onto porous collagen scaffolds and showed that “old” mesenchymal stromal cells (MSCs) can be rejuvenated to a “young” phenotype by the presence of covalently immobilized GFs. 34 The proangiogenic factors altered the aging-related p16 gene expression to promote increased cell proliferation, which led to improved in vivo angiogenesis and cardiac function 28 days after surgical ventricular restoration. This is a new platform for cultivation of tissue constructs that could be used for treating aged patients with heart failure using their own bone marrow cells.
Cell Therapy
Despite showing some improvements in attenuating adverse cardiac remodeling, cell injection therapies have long been plagued by excessive cell death after delivery 35 -38 and minimal functional host integration. 39 -41 Reports on MSC therapies have largely concluded that the improvements in function of the ischemic myocardium are due to secreted paracrine factors that increase vascular density and reduce apoptosis. 42 -44 Mesenchymal stromal cells are advantageous for clinical trials due to their relative safety, immunity privilege, relative ease of isolation in high cell numbers, and no genetic modification. 13 Additional issues with injection-based approaches include myocardial tissue damage, inflammatory issues, and disruption of electrical signal propagation. 13,45
Circulating endothelial progenitor cells (EPCs) can home to ischemic sites and be mobilized as part of a natural response to tissue trauma. 46,47 Endothelial progenitor cells can directly contribute to the revascularization of tissue through vasculogenesis by differentiating into ECs. 48,49 Endothelial progenitor cells also express a host of paracrine factors that are prosurvival and encourage endogenous ECs to migrate and proliferate. 50 However, EPC-based clinical trials have shown mild benefits for patients. The low availability of EPCs is a limiting factor; it could take 6 to 12 L of a patient’s blood to collect enough EPCs for a systemic delivery therapy. 50 Furthermore, patients at a higher probability of requiring cardiovascular therapy (eg, aging, diabetes, hypertension, hypercholesterolemia, and smoking) often have lower EPC counts initially. 51
Understanding the natural healing response in myocardial infarcts could lead to better therapies. Monocytes/macrophages are key cells involved in healing response. A balanced inflammatory response is crucial in the infarct healing process. Monocytes/macrophages are initially required to clear necrotic tissue and induce angiogenesis. However, extended duration of an inflammatory state can lead to impaired extracellular matrix deposition and stress on ECs and myofibroblasts. 52 Nahrendorf et al described a hypothetical parabolic relationship between MI monocyte numbers and MI healing. 52 Future studies should investigate how current and future cardiovascular drugs modulate the presence and state of monocytes/macrophages in the infarct.
To improve efficacy, several cell types (EPCs, bone marrow cells, bone marrow-derived MSCs, skeletal myoblasts) were applied as patches to the myocardium which improved cell engraftment and cardiac function. 53 It has been determined that the MSCs in the myocardium mostly gave rise to SMCs, myofibroblasts, and rarely immature CMs. 53 Seeding preconditioned human mesenchymal progenitor cells (MPCs) with transforming GF-β onto decellularized human myocardium provided a unique niche for improved MPC angiogenic paracrine signaling and MPC migration into the infarct. 54 However, the MPCs were not observed to differentiate into CMs or directly integrate with coronary vasculature.
Cell Sheet and Assembly
Cardiac Cell Sheets
Rather than building vasculature from the bottom-up, cell sheet technology has been incorporated with surgical techniques to vascularize thick tissues. 55,56 By manipulating the ratio of ECs present in the cardiac sheets, the degree of subcutaneous neovascularization could be regulated. 57 Cardiac sheets placed onto an infarcted myocardium containing ECs resulted in increased capillary density compared to no ECs and showed that donor ECs connected to the host vasculature. 58 Cardiac cells from neonatal rats were cultured to 80 μm in thickness as a cell sheet before implantation to vascularize in vivo for 1 to 3 days. Vascularized tissues were then restacked and stacked together to form a ∼1-mm thick tissue. 59 By transplanting the cell sheet to host artery and veins (AVs), points of anastomosis can be established which makes the final tissue connection ready. However, this approach might be impractical for clinical applications due to the extensive surgical intervention involved. In an attempt to improve in vitro methods for producing mature blood vessels, Sekine et al generated 3D vascularized cardiac sheets cultured on a bed of resected rat femoral muscle with a media-perusable AV. 60 Including ECs and the angiogenic FGF-2 greatly augmented blood vessel formation. Up to 12 layers of coendothelialized cardiac sheets could be sequentially cultivated on a media-perfused femoral AV bed, 4 times the thickness achievable with no in vitro blood supply. Direct anastomosis of the AV bed and rat neck vasculature provided an immediate blood supply to the 3D tissue in vivo, which resulted in significantly improved cell survival after 2 weeks.
To avoid teratoma formation in vivo in a clinically relevant large animal model, cell sheets were generated from adipose-derived stromal cells (to provide paracrine signaling) and stage-specific embryonic antigen 1 (SSEA-1)+ cardiac progenitors derived from Rhesus monkey autologous ESCs. 61 The constructs were implanted in the monkeys 2 weeks after transient coronary artery ligation. Due to experimental limitations, the functional benefit could not be assessed, but thorough histological analysis revealed that the SSEA-1 population only gave rise to CMs and no teratomas. Interestingly, it was found that in control sheets containing no CMs, there was a loss in neovascularization and function suggesting an important role for paracrine signaling from CMs as well. 62
Modular Tissue Assembly
The lack of control over induced unmediated angiogenesis opens the opportunities for a more engineering-based approach. Instead of solely relying on GFs or biomolecules to induce angiogenesis, engineering methods were introduced to guide the assembly of blood vessels. One of the most prominent engineering approaches is modular assembly where microtissues coated with ECs were packed into a macrotissue with endothelialized void interstitial space for media perfusion. This approach allowed a premature working vascular network to be assembled quickly for blood perfusion. 63 The ECs coated around the tissue modules acted as an antithrombogenic surface that mitigate clotting. 64,65 However, the initial vasculature was physically unstable. For instance, the extensive remodeling of the parenchymal cells within the tissue could undermine the physical integrity of the endothelial monolayer coating in vitro. 66 Animal studies indicated the presence of ECs alone led to significant vessel regression due to the immune response of the animal to the implants. 67 However, the addition of MSCs significantly enhanced blood vessel maturation possibly through two mechanisms. 68,69 First, MSCs were shown to migrate around the ECs and became smooth muscle actin-positive (SMA+) playing the role of pericytes in stabilizing vessel structure. 68 In addition, the presence of MSCs also mitigated macrophage infiltration into implanted tissue. 68
Although vascular integration with the host tissue was demonstrated, the randomized vascular network provided with this method can take up to 20 days to connect to the host vasculature and lacks components that can enable immediate vascular anastomosis. 70 The successful engraftment of modular tissue heavily depends on the extensive tissue remodeling and vascular maturation process, which must take place in vivo. The modular tissue approach is easily scalable but is not necessary universal to all tissue types. The module arrangement physically isolates each tissue module due to the endothelial coating. The isolation may be problematic for connective muscular tissues. For example, functional cardiac tissue relies on intercellular junctions to establish synchronous macroscopic contraction. However, some successes have been demonstrated on other tissue types using the modular approach. For instance, cotransplanting islet cells within endothelialized tissue modules showed a trend toward improved cell viability but not a significant additional benefit to islet function. 70 Nonetheless, the modular tissue approach is one of the first engineering concepts that moved away from random cell assembly toward a more controlled structural assembly.
Prevascularization Strategies
Prevascularization
Significant effort has been dedicated to growing tissue-engineered myocardium for direct remuscularization of the infarcted heart. Comprehensive reviews of engineered cardiac tissue patch approaches are covered by Iyer et al 71 and Ye et al. 72 A requirement not sufficiently met has been the rate of vascularization from the coronary vasculature into these constructs. Even 30 minutes may be long to induce apoptosis in CMs. 72 In seminal work by Zimmermann et al, transplanted engineered heart tissue (EHT) derived from neonatal CMs appeared vascularized, innervated, and the contractile function was maintained after 2 weeks. 73 However, these thick EHTs (∼1 mm) did not have homogenous CM cell density.
In an attempt to create a cardiac patch with more mature prevascularized networks, patches were placed on the omentum for 1 week prior to inducing an MI. 74 To facilitate initial vessel ingrowth and patch viability, prosurvival and proangiogenic factors were incorporated by affinity binding to the porous alginate scaffold. The omental explants showed improved structural and electrical integration with the myocardium and thicker scar tissue. Disadvantages to this approach include the need for 2 additional surgeries on the omentum (implantation and removal) and the temporary cessation of blood flow to the explant prior to implantation.
To improve EHT condition, Narmoneva et al included ECs and observed that cross talk between ECs and CMs improved CM survival and spatial organization in vitro. 75 Kelm et al demonstrated that coating myocardial microtissues with human umbilical vein ECs (HUVECs) enhanced the integration of host capillaries when implanted onto the heart of a chicken embryo or onto the rat pericardium. 76 Caspi et al created an in vitro prevascularized human engineered cardiac patch by seeding hESC-CMs and hESC-ECs or HUVECs and embryonic fibroblasts onto a highly porous poly(L-lactic acid)/poly(lactide coglycolide; PLG) acid sponge. 77 The inclusion of embryonic fibroblasts improved EC organization, density, and survival. Staining revealed that many SMA+ cells were present and also adjacent to von Willebrand factor positive cells acting as pericytes. The ECs promoted CM proliferation and upregulation of both early and late CM markers of differentiation and maturation. Scaffold-free, hESC-CM-only patches implanted onto skeletal muscle did not survive due to ischemic injury. 78 To mitigate cell death, HUVECs were included but necrotic CD31+cells formed in the core of the patch while CMs remained viable on the periphery. In a third attempt, the addition of mouse embryonic fibroblasts produced a 20-fold increase in CD31+ EC vascular networks. Implantation of this tricellular patch containing hESC-CMs, HUVECS, and embryonic fibroblasts improved the in vivo survival by 10-fold. When applied to the myocardium, anastomosis and blood delivery to the graft were observed.
Lesman et al demonstrated functional vascular integration with the host coronary vasculature in patches containing hESC-CMs, HUVECS, and embryonic fibroblasts. 79 The major limitation of this study was that the patches were placed on nonischemic rat hearts, which would affect the patch survival outcomes. However, several important observations were made. Both donor (human) and rat (host) blood vessels were found within the patch, the donor vessels were functionally integrated with the host coronary vasculature, and there was a significant increase in capillary density within the tricultured patches compared to hESC-CMs only patches. When Tulloch et al added ECs to human induced pluripotent stem cell-derived CM cardiac tissue in vitro, increases in CM proliferation were observed. 80 The inclusion of stromal cells promoted a much denser vascular network in vitro, which became perfused when implanted onto rat hearts. Despite the similarities between Tulloch’s and Caspi’s reported effect of stromal cells, Tulloch reported a decrease in EC proliferation, not an increase. There are several differences in the experimental design that could have led to this discrepancy including the cell seeding conditions, cell source variations, and differences in the methods used to quantify proliferation.
The generation of alternatives to HUVECs is an important step toward translation as they have poor vessel stability and survival in vivo and carry immune compatibility issues. 81 Xiong et al found that a fibrin patch comprised of hESC-VCs (ECs and SMCs) improved cardiac functionality compared to intramyocardial injections. 82,83 The improvements in myocardial function were due to paracrine factors that were antiapoptotic for CMs, recruited endogenous c-kit+ progenitors, and enhanced angiogenesis. Similar results were recently reported using human-induced pluripotent cell (hiPSC)-VCs. 84 Recently, Kusuma et al differentiated hiPSCs in a synthetic matrix into early VCs which then gave rise to a bicellular population of ECs and pericytes. 85 A self-organized microvascular network spontaneously formed. The microvasculature was able to survive, integrate, and carry blood flow in vivo. The cell source, differentiation protocol, and well-defined synthetic matrix used make this a clinically relevant approach for regenerative medicine. Combining ECs and supporting pericytes-like cells with the metabolic CMs appears to be beneficial.
Guided Tubulogenesis
An interesting study by Koffler et al concluded that improved organization of EC-based vascular networks within engineered skeletal tissue resulted in faster anastomosis, increased perfusion, and improved maturation. 86 They also suggested that once the implanted vasculature has anastomosed and perfusion has begun, the host remodeled and replaced the donor vasculature as required. To further control the assembly of a blood vessel network in vitro prior to implantation, microfabrication techniques have been utilized to construct physical topographical cues to guide the assembly of blood vessels. For instance, ECs embedded within the collagen matrix can be seeded within patterned microgrooves (100 μm width and 50-100 μm in height) where the ECs can self-organize into tubular structures within 2 days. 87 Initial tubules did not have completely open lumens and pericytic support. Established vessel structures could be encased within a 3D hydrogel embedded with parenchymal cells for further implantation. The patterned grooves determined the initial pattern of the vessel network. Therefore, highly organized vessel patterns could be achieved. Upon implantation, the patterned vessel network anastomosed with host vasculature within 3 days. The vessels progressively matured by developing perfusable lumens as well as recruiting pericytes after 28 days. 88 Cotransplantation of patterned vessels with hepatocytes showed improved hepatocyte function compared to that of randomized vessels.
The concept of topographical guidance can not only help the assembly of ECs into tubular structures but could also help guide the natural sprouting of blood vessels. Our laboratory used a similar microgrooves pattern to direct capillary sprouting between an explanted artery and a vein. 89 The process could also be accelerated with the addition of thymosin β4, VEGF, and HGF. Sprouting capillaries could connect the AV in just 14 days. Cardiac cells can be cultured on top of the capillary bed to form a vascularized beating cell sheet. The presence of the microgrooves not only provided physical guidance to the sprouting capillaries but also established increased paracrine GF concentrations, which induced cell aggregation and assembly within the grooves.
To scale-up to a 3D construct, Madden et al demonstrated that 3D scaffolds with built-in microstructures can provide structural guidance to the formation of cardiac fibers and induce angiogenesis. 90 The CMs could form fibers mimicking native cardiac bundles within the parallel circular microchannels built into the scaffolds. Small pores were distributed around the parallel channels to guide the penetration of the blood vessel in vivo. This engineered scaffold is a significant step forward from the conventional scaffold where seeded cells are often arranged randomly and provide no topographical cues. However, CMs and ECs cannot be seeded within the scaffold in a spatially defined manner; hence prevascularization cannot be achieved. Without in vitro prevascularization, vascularization in vivo is still limited.
Topographical guidance can also be incorporated into scaffold-free approaches using microfibers to facilitate the scaling of 3D constructs. The ECs embedded within a collagen fiber encapsulated within an alginate shell were fabricated through fiber extrusion. 91 The ECs were able to remodel and form tubular structures within the protective alginate shell, which created environmental conditions similar to the micropatterned grooves. In addition, individual microfibers can be assembled through weaving and reeling into a 3D tissue construct. 91 By combining ECs with other parenchymal cells, preformed endothelial vessels can be embedded directly within the tissue construct. 92 Using a similar technique, adipose tissue and hepatic tissue have been constructed. 92 However, the construction of a vascularized, dense, and aligned cardiac muscle tissue is yet to be demonstrated. Further animal studies are also required to examine these vascularized tissue implants to see whether spontaneous vascular anastomosis with the host is sufficient to support a thick and dense tissue construct.
It appears that the generation of an organized and mature vasculature embedded in parenchymal cells could be beneficial for the maintenance of function of parenchymal cells. Disorganized vasculature can give rise to disturbed flow patterns that loosen EC–EC junctions, increase in the presence of cell adhesion molecules that can attract circulating leukocytes that can be proinflammatory, increase recirculation of leukocytes within tortuous lumens that could lead to their adhesion, and expose basement membrane that can activate platelets leading to thrombi and occlusion. 93 Mechanical stimulation and fluid flow within ECs could promote a more mature vascular network formation. 81
Microfluidic Blood Vessels
Rather than guiding the growth or assembly of a blood vessel network, one specific area of work has focused on directly constructing branched perfusable blood vessel networks by pushing the limits of modern microfabrication techniques. This field originated through the interplay between microfluidic technology and tissue engineering. General fabrication techniques traditionally used in making microfluidic devices began to be applied to scaffold fabrication and tissue building. Microfluidic approaches to tissue vascularization were introduced in early 2000s. 94 Microfabrication techniques provide precise control over the spatial arrangement of the vascular network (eg, tree-like vascular structure). Points of anastomosis can be easily included allowing immediate vascular integration with the host vasculature upon implantation. However, the advancement of this strategy also depends heavily on the development of a suitable biomaterial. Figure 2 highlights the progression of microfluidic tissue vascularization approaches using biodegradable polymers and hydrogel materials. Borenstein et al first fabricated vascular network templates by silicon etching. 95 Then, polydimethylsiloxane (PDMS) molding was used to form closed vascular network seeded with ECs mimicking the natural vasculature for oxygen, nutrient delivery, and waste removal. 96 However, materials such as PDMS are nonbiodegradable and thus limit their use in vivo. Since then the field has shifted to the use of biocompatible and biodegradable materials such as PLG and poly(glycerol sebacate; PGS). The mechanical strength and the biodegradable properties of PGS allow it to be molded into a vascular network using standard soft lithography techniques. Fidkowski et al demonstrated this approach with an endothelialized PGS network. 97 In addition, they argued that PGS is a superior material compared to PLG because PLG swells significantly in vivo and induces chronic inflammation. In addition, PLG is more rigid and loses its mechanical integrity rapidly through bulk degradation. On the other hand, PGS degrades gradually through surface erosion. 98
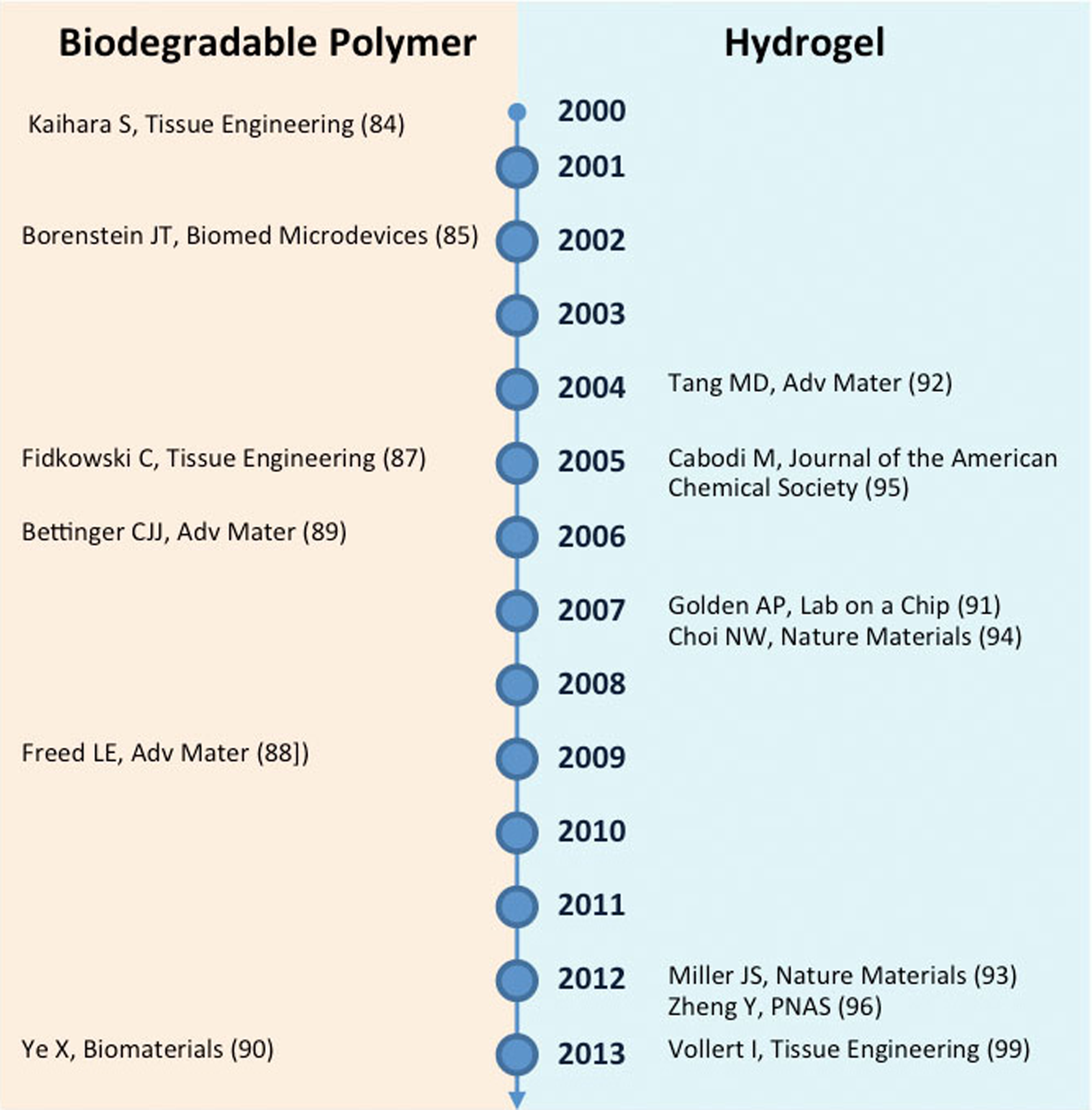
Progression of microfluidic approach to tissue vascularization based on biodegradable polymer and hydrogel.
Vasculature alone is clearly insufficient to resemble actual tissue. Parenchymal cells and VCs must be cocultured in a spatially defined manner. Bettinger et al 99 tried to tackle this issue by engineering a multilayer scaffold with defined network patterns on each layer where ECs and hepatocytes were cultured within alternating layers. Despite the intimate contact of each layer, little interaction was observed between the 2 cell populations. The polymer material was only permeable to gas but not to biomolecules. In addition, the system is geometrically constrained due to the low porosity and lack of interconnectivity between layers. For a highly contractile cardiac tissue, intercellular connectivity is essential for establishing gap junction and electrical signal propagation through the entire tissue construct. Artificial physical barrier prevents the formation of cardiac myofibers and bundles. For the microfluidic blood vessel approach to be successful, scaffold interconnectivity would need to be improved. Despite these limitations, in vivo implantation of a PGS scaffold with a built-in network was achieved. 100 Biodegradation of the scaffold was observed as well as the infiltration of host blood cells into the microvessels. However, direct surgical anastomosis of the scaffold, which is a major conceptual strength of this type of microfluidic approach, was not demonstrated. Highly metabolic cardiac tissue would specifically benefit from direct anastomosis by ensuring the rapid delivery of oxygen through the engineered tissue construct immediately after implantation.
Similar fabrication techniques were also extended to a hydrogel material. By switching to hydrogel, several obstacles related to the use of biodegradable polymers were immediately overcome. First, both large biomolecule and gas exchange are possible within hydrogels. Second, cell interactions in 3D are no longer constrained by physical boundaries. However, the use of a hydrogel also fetches many challenges in fabrication and cell remodeling which become more prominent as the field advances. In this area, there are two major approaches. One approach pioneered by Golden et al used a subtractive method where a sacrificial vascular network was first created from gelatin 101,102 and embedded within a cellularized hydrogel. The gelatin structures were subsequently removed by increasing the temperature of the construct to physiological conditions, thus, leaving behind open channels for endothelialization. Recently, the use of mechanically stable carbohydrate glass, which can be printed with a 3D printer, greatly facilitated the scaling of this subtractive method in 3D. 103 Another major method pioneered by Dr. Strook’s lab used traditional fabrication technique by molding microchannels into cell-embedded hydrogel and then closing the channels by compressing it against another flat hydrogel sheet. 104,105 Although this technique lacks the ability to be scaled to a multilayer network, it is the one of the first methods to demonstrate the interaction between pericytes and ECs in 3D and has proven valuable in the study of angiogenesis and thrombosis. 106
One major shortcoming in hydrogel-based methods is its inability to simultaneously reach physiological cell density within the gel while preserving the engineered vasculature. To create a compact tissue at a physiological cell density (108 cells/cm3), gel remodeling must take place to allow the seeded cells to organize into a compacted tissue. 107,108 This is especially necessary for engineered cardiac muscle, which requires physical cell–cell junctions to establish synchronized macroscopic contraction. This compaction process tends to collapse the open channel networks that lack mechanical support. In the native cardiac tissue, the presence of pericytes and SMCs, as well as the extracellular matrix in the larger vessels, provides the structural support to the blood vessels. However, localized seeding of SMCs and ECs is yet to be demonstrated in an engineered vascular network. Even if this is achieved, it is still unclear how such organized cell seeding would yield a stabilized vessel networks in vitro. It is also hypothesized that constant medium perfusion could maintain an open vascular network during the tissue remodeling process. However, achieving constant perfusion as the tissue remodels is technically challenging. Nonetheless, this technique was achieved by Vollert et al. 109 Compacted cardiac tissue was perfused with an internal hollow vessel created from degraded alginate fibers for up to 3 weeks without vessel collapsing. This work shows promising signs that fabricated open vessel networks could potentially be constructed and maintained within condensed cardiac tissue. It was shown that perfusion helped to increase dystrophin-positive CMs as well as increase overall cell size. However, the work also reveals many technical difficulties in this method. For instance, the degradation of initial sacrificial fibers could be detrimental to surrounding cells due to the increase in osmotic pressure. In addition, cardiac tissue is very sensitive to pressure generated through medium perfusion. Finally, this work is limited to just a single vessel and would need to be scaled-up to a complex 3D network in the future.
Future Perspectives
The next major breakthrough will be the generation of a robust, mature, perfusable, organized vascular network capable of supporting contractile cardiac tissue with physiological CM density. A 3D continuously perfused vascular network will allow the generation of a functional cardiac patch with clinically relevant thickness. In addition, direct vascular anastomosis should be achieved to ensure the survival of highly metabolic cardiac tissue construct upon implantation and to accelerate the tissue engraftment. It appears perhaps the solution lies somewhere in between: engineering methods could be used to guide the assembly of early vasculature and controlled biological signaling could be applied to accelerate vascular integration and maturation in vivo. A sequential treatment that primes the myocardial infarct prior to patch transplantation could also potentially produce better engraftment.
Concluding Remarks
In this review, we have discussed a range of cardiac vascularization strategies from biological-oriented approaches, such as GFs, gene, and microRNAs therapy, to engineering approaches, such as microfluidic blood vessels. Biological methods have shown significant progress in improving heart function by directly revascularizing damaged myocardium but have limited potential in recovering late-stage heart failure. Novel engineering approaches focusing on microfluidic scaffolds have made significant progress in vascularization in recent years but are yet to create a truly functional vascularized cardiac patch due to the tremendous challenges in microfabrication methods. Transplantation of engineered cardiac patches could provide a means of directly remuscularizing the heart. Before these approaches can progress toward the clinic, improved engraftment and increased tissue thickness must be achieved with organized and mature prevasculature.
Footnotes
Authors’ Note
Miles Montgomery and Boyang Zhang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: ORF-GL2 grant, NSERC-CIHR Collaborative Health Research Grant (CHRPJ 385981-10), NSERC Discovery Grant (RGPIN 326982-10) Discovery Accelerator Supplement (RGPAS 396125-10) and McLean Award to MR. Ontario Graduate Scholarship and NSERC CGS M to MM and The Heart & Stroke/Richard Lewar Centre of Excellence Studentship, NSERC CREATE in Microfluidic Applications and Training in Cardiovascular Health (MATCH), NSERC CREATE in Manufacturing, Materials and Mimetics (M3) to BZ.