
Abstract
Objective:
Cardiovascular complications represent a major cause of morbidity and mortality in patients undergoing vascular surgery. This was a prospective randomized, open-label study to investigate the effect of lipid-lowering treatment by statin monotherapy or intensified by combining statin with ezetimibe on a 12-month prognosis after vascular surgery.
Methods:
Patients were randomly assigned to receive rosuvastatin (RSV) 10 mg/d or rosuvastatin 10 mg/d plus ezetemibe (RSV/EZT) 10 mg/d, starting prior to scheduled surgical procedure. The primary end point was the first major cardiovascular event, including death from cardiac causes, nonfatal myocardial infarction, ischemic stroke, and unstable angina.
Results:
A total of 136 patients assigned to RSV and 126 to RSV/EZT completed the study protocol. As many as 6.6% of patients in the RSV group experience a major cardiovascular event within 30 days after surgery versus 5.6% in the RSV/EZT group (P = .72). From month 1 to 12 of the follow-up period, primary end point was observed (9 taking RSV vs 2 in the RSV/EZT group [P = .04]). Intensified lipid-lowering therapy with RSV/EZT was associated with a greater decrease in low-density lipoprotein cholesterol levels compared with RSV (75.87 ± 31.64 vs 87.19 ± 31.7, P = .004), while no differential effect on triglyceride, high-density lipoprotein cholesterol or high-sensitivity C-reactive protein levels was noted between groups.
Conclusion:
Our findings indicate that statin therapy intensified by ezetimibe may reduce the incidence of cardiovascular events within the first 12 months after vascular surgery. Nonetheless, whether the use of ezetimibe as an add-on therapy to reduce cardiovascular risk in these patients needs to be tested in larger future studies.
Introduction
Cardiovascular complications represent a major cause of morbidity and mortality in patients undergoing vascular surgery that adversely affect both short- and long-term prognosis. In Europe, the cardiovascular death rate in such patients is estimated 1 to be approximately 2%. The prevalence of symptomatic or asymptomatic perioperative myocardial damage as assessed by serum concentration of troponin ranges from 14% to 47%, reflecting the high likelihood of underlying significant coronary artery disease in patients undergoing these operations. 2 Indeed, Hertzer et al found after performing coronary angiography in 1000 patients scheduled for vascular surgery, only 8% of them had a normal coronary artery tree. 3
Several trials involving patients undergoing vascular surgical procedures have demonstrated a beneficial role of long-term statin therapy for the prevention of cardiovascular complications. 4 –7 These protective effects related to the use of statins are based on the reduction of low-density lipoprotein (LDL) cholesterol levels as well as other pleiotropic benefits, including reduction of inflammation and plaque stabilization. 8 However, the optimal use of statin and the target level of LDL cholesterol prior and after the procedure remain controversial. The guidelines of the American College of Cardiology/American Heart Association on the management of patients with peripheral artery disease recommend statin treatment in all patients with peripheral artery disease to achieve a target LDL level of <100 mg/dL. 9 Additionally, higher doses of statin and lower LDL cholesterol levels proved to be both independently associated with improved outcome in patients with peripheral arterial disease. 10 The addition of ezetimibe, a selective cholesterol absorption inhibitor, is known to potentiate the lipid-lowering effect of the statins. However, the favorable effect on cardiovascular outcomes with statin plus ezetimibe combination has been shown only recently in patients with chronic kidney disease. 11
There is a lack of evidence regarding the effect of aggressive lipid-lowering therapy in the reduction of cardiovascular events following vascular surgery. This was a prospective randomized, open-label study to investigate the effect of lipid-lowering treatment by statin monotherapy or intensified by combining statin with ezetimibe on the occurrence of cardiovascular events 12 months after vascular surgery.
Participants and Methods
Patients who underwent elective vascular surgery from January 2007 to June 2009 were included in the trial. Patients were excluded if they had any contraindication to the use of statins; emergency surgery; a reoperation within 30 days after a previous procedure; liver disease; a history of a cardiovascular event within the previous 6 months prior to randomization (myocardial infarction [MI] or stroke).
After giving written informed consent, eligible patients were randomly assigned to receive either rosuvastatin (RSV) 10 mg/d or a combination of rosuvastatin 10 mg/d plus ezetimibe 10 mg/d (RSV/EZT), starting 2 weeks prior to the procedure. All regimens were prescribed by our institution and were continued by the patients during the follow-up period. Because of the commercial unavailability of a single drug combining the 2 substances (RSV and EZT), the patients of the RSV/EZT group were given 2 different regimens. A computer algorithm was used in the randomization. In patients already on statin, there was an 8-week washout period between different drug treatments. Initiation of lipid therapy before surgery was decided to enhance compliance afterward. The RSV was selected due to its anticipated significant absolute LDL cholesterol reduction and the favorable safety profile with the starting dose of 10 mg/d.
12
The addition of ezetimibe to the statin was decided because it is well documented that this combination reduces LDL cholesterol by the equivalent of around 3 doublings of the statin dose.
13
All patients were preoperatively screened in accordance with the recommendations proposed by the American Heart Association/American College of Cardiology Task Force. 14 Patients’ risk factors for cardiovascular events were noted and recorded on admission.
All patients were under antiplatelet therapy for at least 3 weeks prior to the procedure. Preoperative medications were continued immediately after surgery. Patients who were enrolled and were already receiving β-blocker therapy continued their medication. For patients not already on a β-blocker, bisoprolol (2.5 mg once daily) was initiated at the screening visit. Anesthetic management and surgical technique were at the discretion of the same surgical and anesthesiologic team, who were unaware of patient group assignment.
Baseline lipid levels were measured at the screening visit for the statin-naive patients and after the 8-week washout period for the patients already on a statin. During the in-hospital phase of the study, electrocardiograms and measurements of lipid profile, hepatic transaminase concentrations, and creatine kinase (CK) concentration were obtained before surgery and at the first postoperative day.
The analysis of serum lipid parameters was carried out on an Olympus AU2700 analyzer (Olympus Diagnostica, Hamburg, Germany). Total cholesterol and triglycerides were determined enzymatically and high-density lipoprotein (HDL) cholesterol by a direct assay (Olympus Diagnostica). The LDL-C was calculated by the Friedewald formula and non-HDL-C was calculated as total HDL-C. Serum apolipoproteins B (apoB) and A1 (apoA1) and lipoprotein (a) were measured on a BN ProSpec System (Siemens). Outpatient follow-up was performed at the 1st, 6th, and 12th month after surgery.
The primary study end point was a composite of death from cardiac causes, nonfatal acute MI, ischemic stroke, and unstable angina. Death was considered due to cardiac causes if the patient died of MI, cardiac arrhythmia, or congestive heart failure caused primarily by a cardiac condition. The diagnosis of MI required elevated troponin concentration with at least one of two 12-lead electrocardiographic changes, including development of new Q waves or new persistent ST-T segment or T-wave changes. Unstable angina was defined as severe chest pain lasting for at least 30 minutes, unresponsive to standard therapeutic intervention and associated with transient ST-segment deviation of 0.05 mV or greater, new or T wave inversion of 0.3 mV or greater without development of Q waves, or CKMB elevation. The diagnosis of ischemic stroke was made if signs or symptoms of ischemic stroke were confirmed with imaging studies.
The secondary outcome was defined as the effect of therapy on serum biomarkers, including lipids and high-sensitivity C-reactive protein (hs-CRP). These markers were measured preoperatively, postoperatively, and at the 1st, 6th, and 12th month after the procedure. In the analysis of the end points, the events were further divided into those occurring during the first month (early) after the procedure and those occurred after the first month and during the first year (late).
Safety outcome diagnostic measures included serum CK and aspartate transaminase (AST) levels as well as clinical evaluation of any adverse event. The patient was withdrawn from the study if AST levels were more than 3 times the upper limit, if CK was more than 10 times the upper limit, or the patient had any clinical sign of myopathy or rhabdomyolysis.
Statistical Analysis
Data were expressed as mean ± standard deviation or mean ± standard error of mean as appropriate. Comparisons of continuous variables were performed by Student t test for normally distributed variables and Mann-Whitney U test for nonnormally distributed variables, while chi-square test was used for categorical variables. Differences between the groups in the rate of occurrence of primary end points were evaluated with the Fisher exact test. Event rates were further examined with the Kaplan-Meier method, while Kaplan-Meier survival curves were compared using the log-rank test. Univariate and multivariate Cox proportional hazard regression analyses were used to evaluate the effect of each therapy. All analyses were performed according to the intention to treat principle. All statistical tests were 2-sided and a P value of <.05 was considered to indicate statistical significance.
All analyses were carried out with SPSS 15.0 statistical package for Windows (SPSS Inc, Chicago, Illinois) and Stata 10.0 (Stata Corp LP, College Station, Texas).
Results
Of the 334 consecutive patients assessed for trial eligibility, 72 were excluded: 39 of these patients did not meet the inclusion criteria, 4 had hepatic disease, 6 had a malignancy, 12 had a recent cardiovascular event, 8 underwent reoperation, while 9 patients had an acute coronary syndrome. Thirty-three patients refused to participate in this trial. Of the 262 patients enrolled, 136 were assigned to RSV and 126 to RSV/EZT. The demographic and clinical characteristics of the study population are described in Table 1. The median age was 71 years (range 41-89), and 89.7% of the patients were male.
Demographic and Clinical Characteristics of the Study Population (N = 262)

Abbreviations: RSV, rosuvastatin; EZT, ezetimibe; ACE, angiotensin-converting enzyme; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease.
A total of 142 patients included in the study had aneurysm disease (54.2%) and 69 (26.3%) had carotid artery disease, while 51 (19.5%) patients had critical limb ischemia. In all, 184 (70.2%) patients underwent endovascular procedure, while the remaining 78 (29.8%) had open repair.
Eight patients did not attend their follow-up visit but were reached via telephone. One patient receiving RSV died of cancer 10 months after the procedure. Six patients did not receive the intended study regimen: 2 patients who had been assigned to RSV/EZT did not take the ezetimibe and 4 patients (2 in each group) discontinued their study drugs because of side effects (1.5%).
During the whole follow-up period of 1 year, 18 (13.2%) of the 136 patients in the RSV group had a major cardiovascular event when compared with 9 (7.1%) of the 126 patients in the RSV/EZT group (P = .11). Sixteen patients (6.1%) in the whole cohort had a major adverse cardiovascular event within 30 days of surgery resulting in 2 deaths. Specifically, a total of 9 (6.6%) of the 136 patients in the RSV group had a major adverse cardiovascular event within 30 days after surgery when compared with 7 (5.6%) of the 126 patients in the RSV/EZT group (P = .72).
During 1 to 12 months of follow-up period, a primary end point was recorded in 11 (4.2%) of the remaining 260 patients: 9 patients in the RSV group and 2 patients in the RSV/EZT group. In the RSV group, 5 patients died of a cardiac-related cause (3 patients sustained a fatal acute MI, 1 patient had severe heart failure, and 1 patient ventricular fibrillation) on month 7, 6, 8, 10, 10 following surgery respectively; 1 patient had a nonfatal acute MI; 1 patient sustained an ischemic stroke, while in 2 patients, unstable angina and worsening of their cardiac failure was developed during the follow-up period. In the RSV/EZT group, 1 patient experienced an ischemic stroke and 1 patient developed unstable angina. There was no relation between the type of pathology or the type of operation (open or endovascular) with the occurrence of the primary end point during and after the first month.
The clinical characteristics of the population according to the study group are presented in Table 1. The risk of event occurrence was further compared between the groups with the Kaplan-Meier method, as event-free survival after surgery. The event rate, including the events occurring during the first month after the procedure, was 12.5% in patients on RSV and 7.1% in patients taking RSV/EZT (P = .106). When studying the events occurring after the first month, patients in the RSV/EZT group exhibited a significant decrease in the rate of cardiovascular event compared with the rate in the RSV group (P = .04; Figure 1).

Subset analysis expressed with a Kaplan-Meier curve for event-free survival within 1 year after surgery for the events occurring after the first month. P values are derived using the log-rank test.
In the multivariate model taking into account lipid therapy, age, gender, type of operation, and clinical characteristics, intensive lipid-lowering therapy were associated with a significant reduction in the rate of cardiovascular events after the first month of a vascular operation (P = .05). Achieved LDL levels could predict the occurrence of a late cardiovascular event (B = 0.001, P = .003) and that effect remained even when the type of pathology and surgery were forced in the regression model. Cardiac-related deaths that occurred in the RSV group were not significantly correlated with any other cofactor. No other pharmacologic intervention was retained as an independent predictor of the cardiovascular event rate in the multivariate model. Furthermore, an extensive array of subgroup analyses showed no statistically significant differences between any subgroup of interest (P > .05 for all comparisons).
Baseline lipid levels were similar in the 2 groups (Table 2): RSV group had a baseline LDL cholesterol level of 143 ± 54.1 in comparison with 148.24 ± 58.1 in the RSV/EZT group (P = .451). Both groups showed a decrease in total cholesterol and LDL cholesterol levels. General linear model analysis for all measurements depicted a significant decrease in total cholesterol and LDL cholesterol levels, while triglycerides and HDL cholesterol levels did not alter significantly during the follow-up period (Table 2; Figure 2). Specifically, when comparing these 2 groups at the first year of follow-up, the latter group showed a significant decrease in mean LDL levels (75.87 ± 31.64 vs 87.19 ± 31.7 mg/dL, P = .004), while there was no significant change noted in triglycerides and HDL cholesterol levels between the study groups in the same time frame (median TG 144 vs 155 mg/dL, P = .502 and mean HDL 44.7 ± 9.45 vs 44.67 ± 10.23 mg/dL, P = .983, respectively; Table 2).

Plot of linear model analysis for repeated measures of total cholesterol, LDL cholesterol, HDL cholesterol, and TG levels. P value refers to comparison between groups. TG indicates triglyceride; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Lipids, Lipoprotein, and High-Sensitivity C-Reactive Protein Levels at Baseline and 1 Year After Surgery According to Treatment Arms
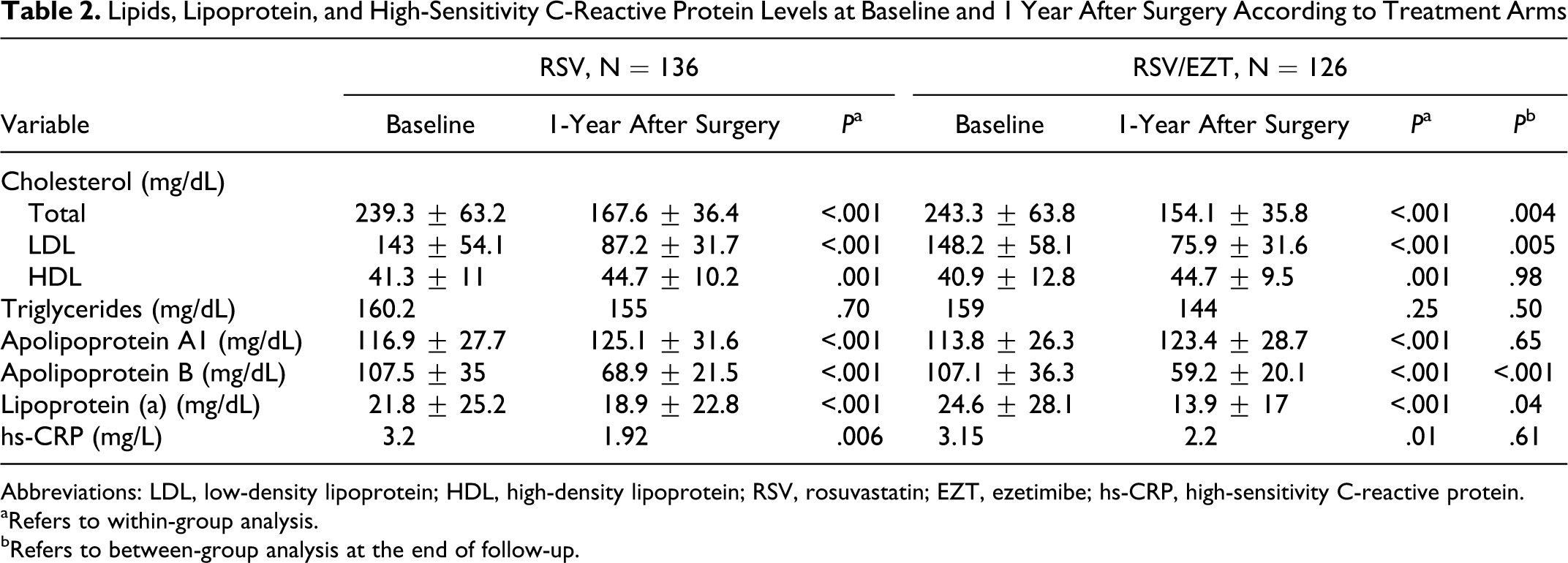
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; RSV, rosuvastatin; EZT, ezetimibe; hs-CRP, high-sensitivity C-reactive protein.
aRefers to within-group analysis.
bRefers to between-group analysis at the end of follow-up.
Baseline lipoprotein levels were similar between the 2 groups. There was a significant difference in lipoprotein levels within both groups (Table 2). However, at the first year of follow-up, the RSV/EZT group showed a significant decrease in ApoB and Lp(a) levels, when compared with RSV group (Table 2). Levels of ApoA1 were not significantly different between the 2 groups at the end of the follow-up.
The median baseline hs-CRP level was 3.2 mg/L in the RSV group and 3.15 mg/L in the RSV/EZT group (Table 2). At the conclusion of the 12-month follow-up, the median decrease in the hs-CRP levels from the baseline was 0.73 mg/L (21.88%) in the RSV group compared with 0.84 mg/L (24.33%) decrease in the RSV/EZT group (P = .09).
The median CK level was 87 (range 21-236) U/L in the RSV group and 93 (range 14-236) U/L in the other group (P > .05). The median level of alanine aminotransferase was 20.5 (range 10-173) U/L in the RSV group and 20 (range 10-237) U/L in the other group (P > .05). Four patients (1.5%) had an adverse reaction to rosuvastatin, that is, clinical sign of myopathy with no elevated levels of aminotransferase, and the statin was withdrawn.
Discussion
Since several trials have elucidated even better clinical outcomes with early and intensive statin therapy in acute coronary syndrome, 15,16 it is very important to define which is the optimal lipid-lowering strategy after a vascular operation. The present study shows a strong protective effect of intensified lipid-lowering therapy (statin plus ezetimibe) against the incidence of a late cardiovascular event during the first year of follow-up in patients undergoing vascular surgery.
In the vascular surgery setting, several trials have evaluated the relation between statin use and perioperative mortality. In the first prospective study, 100 patients undergoing aortic aneurysm, lower extremity bypass, or carotid endarterectomy procedures were randomly assigned to atorvastatin or placebo and followed for at least 6 months. 4 The incidence of cardiac events was more than 3 times higher with placebo (26%) compared with atorvastatin. In the Statins for Risk Reduction in Surgery study, the cardiovascular complications rate was significantly lower in patients on statin (9.9% vs 16.5%) than in those not receiving statins, yielding a protective effect of 0.52 among statin users (P < .001). 5 Moreover, McNally et al reported a decreased rate of postoperative complications and mortality in the open aortic repair group receiving statin, while there was also a trend toward the same result for the EVAR group on statin. 6 These reports have been affirmed by level I evidence in a randomized prospective clinical trial recently published. 7 In this study, 497 patients who underwent major open vascular surgery were randomly assigned to receive fluvastatin or placebo. In patients assigned to statin, there was a significant low incidence of MI and cardiovascular death.
In the present study, a total of 16 (6.1%) of the 262 patients had evidence of a cardiovascular event within 30 days after surgery. This rate is certainly lower than recently reported. 7 Indeed, Schouten et al depicted a rate of 10.8% for patients on statin, although only one fourth of this cohort underwent endovascular procedure. In the last decade, the incorporation of endovascular procedures into the standard operative armamentarium has changed the composition of the vascular surgical population, leading to a trend in favor of endovascular methods. Our cohort mainly consisted of patients treated with an endovascular technique (70.2%), representing the current and perhaps the future surgical practice.
Rosuvastatin is the most potent currently available statin and appears to be relatively safe and well tolerated, 17 with evidence of reducing the burden of atherosclerosis. 18 The cholesterol-lowering effects of statins can be further augmented by adding ezetimibe, a selective cholesterol transport inhibitor with proven efficacy and safety. 19 Robinson in a recent pooled analysis of 13 282 patients aged 18 to 93 years in 16 published trials of ezetimibe monotherapy or combined with a statin demonstrated lipid efficacy and safety of administration across all age groups (<65, 65-74, >75). 20 Our study agrees that in patients undergoing vascular surgery, rosuvastatin treatment in combination with ezetimibe is safe and well tolerated.
In the vascular surgical setting, no randomized trials have yet been conducted in order to assess the potential benefit of intensified lipid-lowering therapy. Nevertheless, there are some reports concerning that intensified lipid-lowering therapy may be effective in maintaining graft patency. 21 Our findings support the importance of achieving low-target LDL cholesterol levels in patients undergoing vascular surgery.
Statins confer their postulated beneficial effects by lowering cholesterol levels, reducing inflammation, by stabilization of the soft lipid-rich atherosclerotic plaque and, possibly improvement of endothelial function. 4 Schouten et al recently reported a significant decrease in hs-CRP levels in patients after vascular surgery that were under statin therapy compared with those under placebo. 7 On the other hand, conflicting results have been provided by the few studies that have investigated the anti-inflammatory effect of ezetimibe. Krysiak et al recently reported a strongest lymphocyte-suppressing effect, accompanied by a decrease in plasma levels of hs-CRP and ICAM-1, in patients receiving both simvastatin and ezetimibe. 22 In our study, there was no difference in the reduction of hs-CRP levels and therefore the difference in clinical outcomes could not be attributed to a greater anti-inflammatory effect by intensified treatment.
The effects of ezetimibe monotherapy on cardiovascular disease remain to be sufficiently established in comparison to other lipid-lowering agents. Ezetimibe in monotherapy seems to produce mainly quantitative rather than qualitative changes in LDL. 23 Although ezetimibe was shown to have some kind of pleiotropic effects including the amelioration of inflammation, insulin resistance, and fatty liver, neither the underlying mechanism nor the atherosclerotic effect of ezetimibe monotherapy are yet fully clarified. 24
Beyond the lipid-lowering effect, Bulut et al found that a combination of atorvastatin 10 mg/d and ezetimibe 10 mg/d was more effective in improving endothelial function than 40 mg of atorvastatin alone in patients with metabolic syndrome. 25 Although Gounari et al and Landmesser et al disputed this observation, as they reported that lipid-lowering treatment achieved by ezetimibe alone is unable to affect endothelial function in patients with heart failure. 26,27 Additionally, Berneis et al found that treatment with ezetimibe alone or in combination with a statin increased the proportions of small dense LDL subfraction profile, thus resulting in a more proatherogenic LDL subfraction profile. 28
The clinical benefit by adding ezetimibe to a statin has been disputed in patients with familial hypercholesterolemia (no additional favorable effect on the carotid intima–media thickness) 29 and in patients with aortic stenosis. 30 However, in the recently published Study of Heart And Renal Protection (SHARP) trial involving about 9500 patients with chronic kidney disease, treatment starting with the combination of ezetimibe plus simvastatin resulted in an approximate 25% reduction in cardiovascular events. 11 Our study reaffirms that starting with statin plus ezetimibe combination may confer clinical benefit over that achieved with statin alone. Moreover, although the overall randomized comparison for the 2 dyslipidemic strategies was neutral for the primary end point, we found that after the first month of surgery, the combination therapy had a protective role. This finding certainly raises questions concerning the optimal time frame for the initiation of lipid-lowering therapy in order to anticipate clinical benefit. On the other hand, we should keep in mind that the surgery-related stress is diminished after 1 month and what remains is the preexisting cardiovascular burden disease.
The results of our study should be interpreted in the light of certain limitations. This was a study of open-label design, which may introduce bias in ascertaining subjective end points, as for example unstable angina. The diagnosis of CAD was based on history and medical records and was evaluated as presence or absence in the analysis due to lack of detailed information. The sample size and the subsequent small number of cardiovascular events and mortality observed should be acknowledged. Despite statistical significance, our results need to be tested in larger studies. Another arm assessing a dose-dependent effect of statin monotherapy would also be of value in deciding optimal treatment. However, the design of a study that includes a control group of vascular patients not on statins may raise ethical issues for approval.
In conclusion, our findings indicate that intensified lipid-lowering therapy with RSV/EZT reduces the incidence of late cardiovascular events within the first 12 months after vascular surgery. Although this study does not avail to endorse the broad use of ezetimibe to reduce cardiovascular risk in patients undergoing vascular surgery, our data provide a stimulus toward future investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.