
Abstract
Background:
Curcumin, the active ingredient of turmeric (Curcuma longa), is known to have anti-inflammatory and antioxidative properties. The present study was aimed to determine the effect of curcumin in regional myocardial ischemia/reperfusion (I/R) injury and its underlying mechanisms involving the role of prosurvival kinases and apoptotic kinases.
Methods:
Sprague-Dawley rats (n = 109) subjected to a 30-minute left anterior descending coronary artery (LAD) occlusion followed by reperfusion were assigned to receive saline (control), curcumin (100 mg/kg), wortmannin (inhibitor of phosphatidylinositol-3-OH kinase [PI3K]-Akt), wortmannin + curcumin, U0126 (inhibitor of extracellular signal-regulated kinase [ERK1/2]), U0126 + curcumin, SB216763 (inhibitor of glycogen synthase kinase [GSK-3β]), and SB216763 + curcumin 20 minutes before LAD occlusion. Infarct size was measured after 2 hours of reperfusion by triphenyl tetrazolium chloride staining. The phosphorylation of Akt, ERK1/2, GSK-3β, p38, and c-Jun N-terminal kinases (JNK) was determined by immunoblotting after 10 minutes of reperfusion.
Results:
Curcumin significantly reduced the infarct size compared with the control (33.1% ± 6.2% vs 50.1% ± 3.9%; P < .05). Wortmannin or U0126 alone did not affect the infarct size but abolished the curcumin-induced cardioprotective effect. Curcumin significantly enhanced the phosphorylation of Akt, ERK1/2, and GSK-3β, while it reduced that of p38 and JNK. Wortmannin or U0126 abolished enhanced phosphorylation of GSK-3β induced by curcumin. SB216763 alone or combined with curcumin reduced the infarct size and enhanced phosphorylation of GSK-3β compared with the control.
Conclusions:
Preconditioning by curcumin effectively protects against regional myocardial I/R injury through the activation of prosurvival kinases involving PI3K-Akt, ERK1/2, and GSK-3β, and attenuation of p38 and JNK.
Introduction
The rapid restoration of blood flow following an acute coronary artery occlusion is a prerequisite for myocardial salvage. However, it has been demonstrated that myocardial ischemia/reperfusion (I/R) activates the 2 “stress-response” mitogen-activated protein kinase (MAPK) subfamilies, namely, c-Jun N-terminal kinases (JNK) and p38 mitogen-activated protein kinases (p38-MAPKs; so-called death pathway) resulting in apoptosis. 1 At the same time, antiapoptotic cascades involving prosurvival kinases (reperfusion injury salvage kinase [RISK] pathway) such as phosphatidylinositol-3-OH kinase (PI3K)-Akt and extracellular signal-regulated kinase (ERK1/2) may also be activated to confer tissue protection. 2,3 Therefore, these pathways may comprise important molecular mechanisms responsible for I/R-induced tissue injury, in which the relative activity of proapoptotic and antiapoptotic kinases determine cell survival or death.
Curcumin (diferuloylmethane), a yellow pigment from Curcuma longa, is a major component of turmeric (also called curry powder) and is commonly used as a spice and food-coloring agent. It has been known to mitigate I/R or cytotoxic injury in various tissues including the heart, 4 –6 through its anti-inflammatory 7,8 and antioxidative properties. 9 –12 Curcumin has also been shown to reduce the phosphorylation of JNK, p38-MAPKs, signal transducer and activator of transcription 3 (STAT-3), and subsequent downstream signals in human endothelial cells in vitro. 13 Nevertheless, the activity of the antiapoptotic kinases and its balance with proapoptotic proteins under curcumin have not been determined. Therefore, the present study was aimed to determine the effect of curcumin in regional myocardial I/R injury and, if any, its underlying mechanisms involving the role of prosurvival kinases such as PI3K-Akt, extracellular signal-regulated kinase (ERK1/2) and subsequent downstream signaling pathway glycogen synthase kinase (GSK-3β), and apoptotic kinases such as p38 and JNK.
Materials and Methods
The study was approved by the Institutional Animal Care and Use Committee at Chonnam National University Medical School and performed in accordance with the guidelines of the Committee.
General Preparation
Male Sprague-Dawley rats (250-300 g) were anesthetized with intraperitoneal (IP) pentobarbital (60 mg/kg). They were intubated and ventilated using a Harvard rodent respirator (model 683; Harvard Apparatus, South Natick, Massachusetts) with oxygen-enriched air. The tidal volume and ventilation rate were adjusted to 10 mL/kg and 45 to 55 strokes/min, respectively. Electrocardiograms were recorded using 3 lead limb electrodes. The right internal carotid artery was cannulated with a saline-filled polyethylene catheter (PE 50), and connected to a pressure transducer (Deltran; Utah Medical Products, Midvale, Utah). The right jugular vein was cannulated to administer drugs. Body temperature was continuously monitored with a rectal temperature probe and maintained at 37.5°C to 38.5°C using a heating lamp and a heating pad. Additional pentobarbital was given as needed to maintain stable anesthesia.
A left thoracotomy at the fourth intercostal space was performed, and a 6-0 silk ligature was passed below the main branch of the left anterior descending coronary artery (LAD). The ends of the ligature were passed through a short segment of soft vinyl tube to form a snare. A stabilization period of at least 20 minutes was allowed to elapse before induction of ischemia. Successful coronary artery occlusion was verified by ST segment changes in the electrocardiogram and the presence of epicardial cyanosis.
Experimental Protocols
Rats were subjected to a 30-minute LAD occlusion followed by 120 minutes of reperfusion. They were divided into 8 groups: (1) control group without any drugs; (2) curcumin group received curcumin 100 mg/kg; (3) Wor group received wortmannin (inhibitor of PI3K) 0.6 mg/kg; (4) Wor + curcumin group received wortmannin plus curcumin; (5) U0 group received U0126 (inhibitor of ERK1/2) 1 mg/kg; (6) U0 + curcumin group received U0126 plus curcumin; (7) SB group received SB216763 (inhibitor of GSK-3β) 1.2 mg/kg; and (8) SB + curcumin group received SB216763 plus curcumin. All study drugs or vehicle were administered 20 minutes before LAD occlusion. The dosage of curcumin (Sigma, St Louis, Missouri; 100 mg/kg) was adopted, since it was shown to attenuate myocardial I/R in the rat, and the time point of its administration was adopted, since it reaches its peak plasma level within 15 minutes after IP administration. 14,15 Curcumin was dissolved in dimethyl sulfoxide (DMSO) and administered IP. Wortmannin (Tocris Cookson Ltd, Bristol, UK), U0126 (Tocris), and SB216763 (Tocris) were also dissolved in DMSO and administered over 2 minutes as an intravenous (IV) bolus. It has been demonstrated in a previous study that DMSO does not affect myocardial infarct size in an identical rat model. 16
Assessment of Infarct Size
Myocardial infarct size was measured as previously described.16 Briefly, on completion of the above protocols, the rats were sacrificed with a ketamine–xylazine overdose under heparinization (200 units IV). Hearts were rapidly excised and mounted on a modified Langendorff apparatus for perfusion with normal saline via the aortic root at a perfusion pressure of 40 cm H2O to wash out intraventricular blood. After 10 minutes of perfusion, the coronary artery was reoccluded and fluorescent polymer microspheres (Duke Scientific, Palo Alto, California) suspended in saline were infused into the aorta to negatively mark areas at risk (AARs). After the atria were removed, hearts were weighed and frozen at −20°C for 2 hours and subsequently sliced into 2 mm cross-sectional pieces. The slices were incubated at 37°C for 10 minutes in 1% 2,3,5-triphenyl tetrazolium chloride (Sigma, St Louis, Missouri) in sodium phosphate buffer with pH adjusted to 7.4 to visualize infarcts. The slices were fixed overnight in 7.5% formaldehyde to enhance the contrast between stained (viable) and unstained (necrotic) tissue. The slices were photographed under ultraviolet light to visualize the AAR (non-luminous) and the surrounding normal areas and also under room light to visualize the infarcted and noninfarcted myocardium. The infarcted area, AAR, and surrounding normal areas were determined by Image Tool (UTHSCSA Image Tool Software 3.0, San Antonio, Texas). This processing was performed by 2 persons in a blind manner, and the mean values were used. The volumes of the infarcted area and AAR were calculated by multiplying the size with the thickness of the slice. Myocardial infarct size was expressed as a percentage of the AAR.
Immunoblotting
Rats were subjected to a 30-minute LAD occlusion followed by reperfusion in all groups except sham. The hearts were excised 10 minutes after reperfusion, and the risk area in the left ventricular tissue was quickly separated and frozen in liquid nitrogen. On the experimental day, the tissue samples were thawed, homogenized in ice-cold Pro-Prep TM Protein Extraction Solution (Intron Biotechnology, Seoul, Korea), and centrifuged at 14 000 rpm for 15 minutes at 4°C. The supernatant was used for electrophoresis. The protein concentration was assayed with the BCA protein assay kit (Pierce, Rockford, Illinois). Equivalent amounts of proteins were loaded and run on a 10% Tris-HCl sodium dodecyl sulfate (SDS) polyacrylamide gel. Proteins were transferred to a nitrocellulose membrane and then blocked with 5% nonfat dry milk, 20 mmol/L Tris-buffered saline (TBS), with 0.1% Tween 20. The membrane was then incubated overnight at 4°C with rat polyclonal-specific primary antibodies against Akt (No. 9275), ERK1/2 (No. 9101), GSK-3β (No. 9336), p38 (No. 9211), and JNK (No. 9251; Cell Signaling Technology, Danvers, Massachusetts), diluted 1/1000 in 5% bovine serum albumin (BSA) in TBS-Tween. It was subsequently incubated with anti-rabbit immunoglobulin horseradish peroxidase (HRP)-linked secondary antibody (Cell Signaling Technology, No. 7074) at a dilution of 1/2000 in TBS-Tween. After washing 3 times, immunereactive bands were visualized using luminol reagent (Santa Cruz, California). The membrane was stripped with Restore TM Western Blot Stripping Buffer (Pierce), and reprobed with antibodies specific for Akt (No. 9272), ERK1/2 (No. 9102), GSK-3β (No. 9315), p38 (No. 9212), and JNK (No. 9258; Cell Signaling Technology). Densitometry was performed with Multi Gauge Program version 3.0 (Fuji, Tokyo, Japan). The images were quantified using luminescent image analyzer (LAS-3000, Fuji) to determine the ratio of phosphorylated/total kinases.
Statistical Analysis
Results were expressed as means ± standard deviation (SD). Differences in the hemodynamic parameters were analyzed by 2-way repeated measures analysis of variance (ANOVA). Differences in infarct size and immunoblot data between groups were tested by 1-way ANOVA. A Scheffé test was used for multiple pairwise comparisons when a significant difference was found with ANOVA. A P < .05 was considered to be statistically significant. Statistical analysis was performed with SPSS 16.0 (Lead Technologies, Chicago, Illinois).
Results
A total of 109 rats were used; 12 were excluded because of failure to determine the infarct or risk area after incubation in triphenyl tetrazolium chloride (1 in the control group, 1 in the curcumin group, 2 in the wortmannin group, 2 in curcumin + wortmannin group, 1 in the U0126 group, 2 in the U0126 + curcumin group, 2 in the SB216763, and 1 in curcumin + SB216763 group).
The hemodynamic data are summarized in Table 1. There were no significant differences in heart rate and arterial blood pressure among the groups throughout the experiment. Heart weight, area of left ventricle, and AAR did not differ among the groups (Table 2). As shown in Figure 1, curcumin significantly reduced infarct size compared with controls (33.1% ± 6.2% vs 50.1% ± 3.9%; P < .05). The protective effect of curcumin was blocked by wortmannin or U0126, while these drugs alone did not affect the infarct size. SB216763 alone or combined with curcumin significantly reduced the infarct size.

Effects of curcumin on the infarct size. The infarct size is expressed as a percentage of area at risk. Values are means ± standard deviation (SD). *P < .05 versus control group.
Hemodynamic Dataa
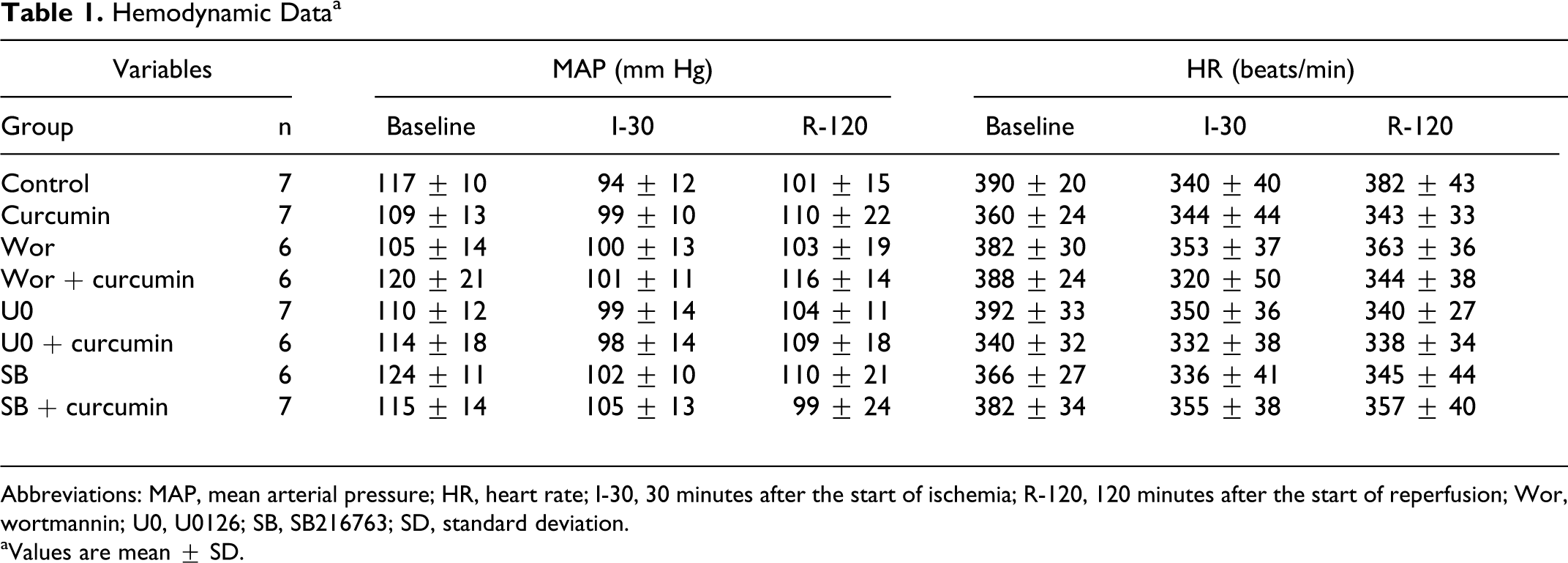
Abbreviations: MAP, mean arterial pressure; HR, heart rate; I-30, 30 minutes after the start of ischemia; R-120, 120 minutes after the start of reperfusion; Wor, wortmannin; U0, U0126; SB, SB216763; SD, standard deviation.
aValues are mean ± SD.
Infarct Size Following a 30-Minute Regional Ischemia and 120-Minute Reperfusiona

Abbreviations: LV, left ventricle; AAR/LV, area at risk as a percentage of left ventricle; Wor, wortmannin; U0, U0126; SB, SB216763; SD, standard deviation.
aValues are mean ± SD.
b P < .05 versus control group.
Curcumin significantly enhanced the phosphorylation of Akt, ERK1/2, and GSK-3β induced by I/R (P < .05; Figures 2 -4). In contrast, it reduced the phosphorylation of p38 and JNK induced by I/R (P < .05; Figure 5A and B). Wortmannin and U0126 alone did not affect the phosphorylation of Akt and ERK1/2 but abolished the effects of curcumin. SB216763 alone or combined with curcumin significantly enhanced the phosphorylation of GSK-3β compared with controls (Figures 2 -4).
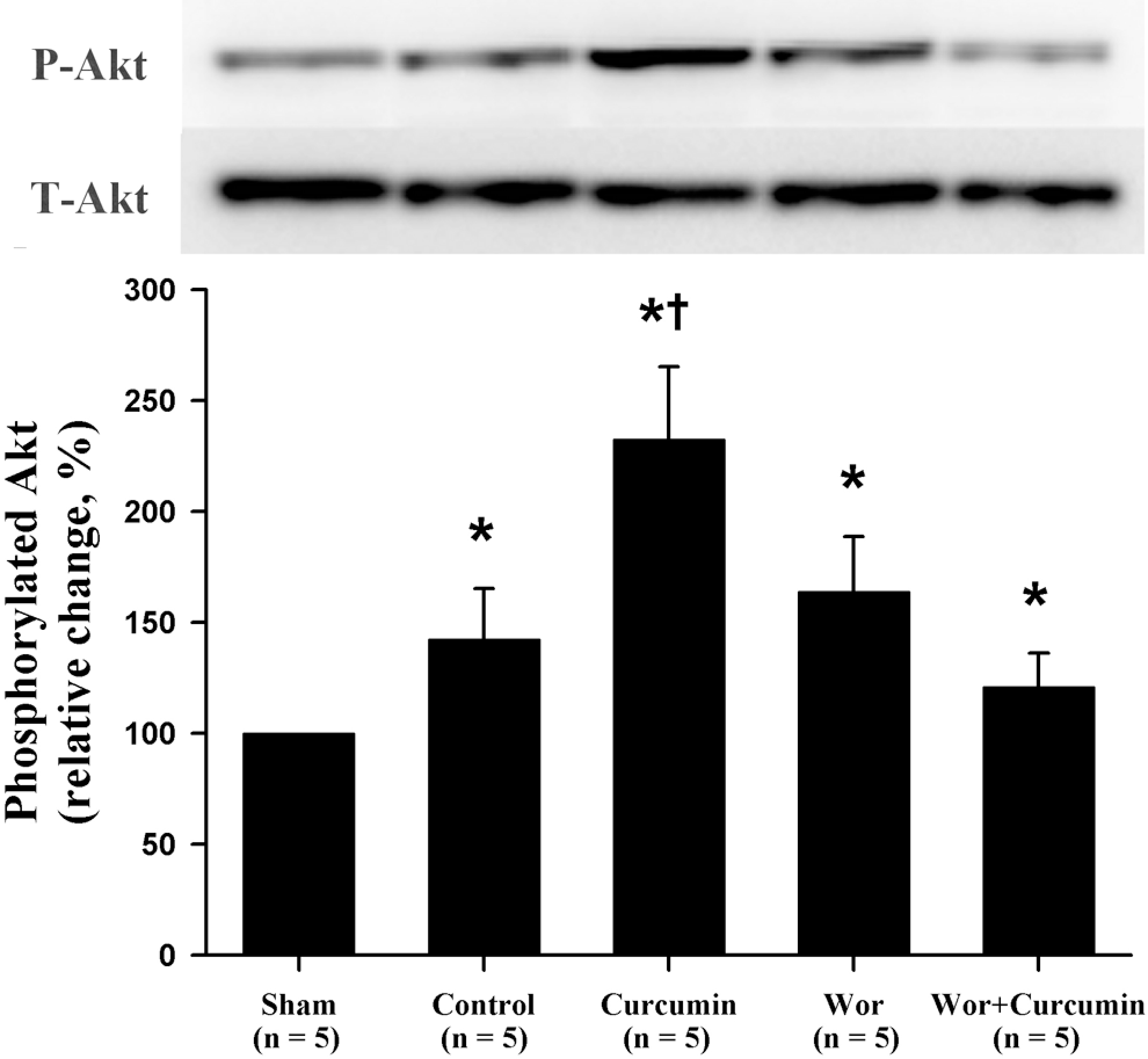
Effects of curcumin on the expression of total and phosphorylated Akt. The sham group was not subjected to ischemia/reperfusion. The upper panels show representative immunoblots, and the lower panels show densitometric data. Values are means ± standard deviation (SD). *P < .05 versus sham group. † P < .05 versus control group.

Effects of curcumin on the expression of total and phosphorylated ERK1/2. The sham group was not subjected to ischemia/reperfusion. The upper panels show representative immunoblots, and the lower panels show densitometric data. Values are means ± SD. *P < .05 versus sham group. † P < .05 versus control group. ERK1/2 indicates extracellular signal-regulated kinase; SD, standard deviation.

Effects of curcumin on the expression of total and phosphorylated GSK-3β. The sham group was not subjected to ischemia/reperfusion. The upper panels show representative immunoblots, and the lower panels show densitometric data. Values are means ± SD. *P < .05 versus sham group. † P < .05 versus control group. GSK-3β indicates glycogen synthase kinase; SD, standard deviation.

Effects of curcumin on the expression of total and phosphorylated p38 (A) and JNK (B). The sham group was not subjected to ischemia/reperfusion. The upper panels show representative immunoblots, and the lower panels show densitometric data. Values are means ± SD. *P < .05 versus sham group. † P < .05 versus control group. JNK indicates c-Jun N-terminal kinases; SD, standard deviation.
Discussion
The present study demonstrated that curcumin significantly reduced infarct size, implying its role in protecting I/R injury in the rat heart. The RISK pathway including PI3K-Akt and ERK1/2 has been reported as a critical signaling pathway for cardioprotection, which can be recruited at the time of myocardial reperfusion by a diverse variety of both ischemic/pharmacological pre- and postconditioning. 2,17 Chiari et al 18 reported in an in vivo rabbit model that isoflurane administered during early reperfusion enhances activation of PI3K-Akt which was causally related and tightly linked to cytoprotection. In the present study, the blockade of PI3K-Akt with wortmannin or that of ERK1/2 with U0126 abolished the protective effect of curcumin. The protection was associated with enhanced phosphorylation of prosurvival kinases such as Akt and ERK1/2. Taken together, it is likely that curcumin given before LAD occlusion (preconditioning) protects against focal myocardial I/R at least in part through activating PI3K-Akt and ERK1/2.
The MAPKs such as p38 and JNK exert a detrimental effect when activated at the time of myocardial reperfusion either through a proapoptotic mechanism, enhancing the expression of adhesion molecules 1 and production of cytokines 19 or by downregulating components of the prosurvival pathway. The activation of p38 MAPK and JNK may surpass that of the prosurvival kinases PI3K-Akt and ERK1/2 during I/R, resulting in myocardial apoptosis and necrosis. In the present study, curcumin reduced the phosphorylation of p38 and JNK, while it enhanced the phosphorylation of Akt and ERK1/2. The greater activity of prosurvival kinases may favor cell survival following I/R insult.
It was also shown that curcumin given before LAD occlusion increased phosphorylation of GSK-3β. Moreover, this increase was blocked by wortmannin or U0126. These results indicate that curcumin phosphorylates GSK-3β through Akt- and ERK-dependent pathways, consistent with those reported previously. 20 The GSK-3β, a downstream target of the RISK pathway, is an important key regulator of apoptosis which inhibits the opening of the mitochondrial permeability transition pore (mPTP) when phosphorylated. 21 The disturbance of ion homeostasis resulting from ATP depletion following the opening of the mPTP can lead to necrotic and apoptotic cell death. 22 The RISK pathways involving PI3K-Akt and ERK1/2 have been shown to prevent cellular damage by converging on the mPTP through GSK-3β, which in turn inhibits its opening. 23,24 Therefore, the curcumin-induced myocardial protection is likely to be mediated through the activation of PI3K-Akt and ERK signaling and, at least in part, subsequent inhibition of GSK-3β, which in turn inhibits the opening of mPTP (Figure 6). Further studies defining the role of mPTP and its interaction with GSK-3β at the time of reperfusion in curcumin-induced myocardial protection may be needed.
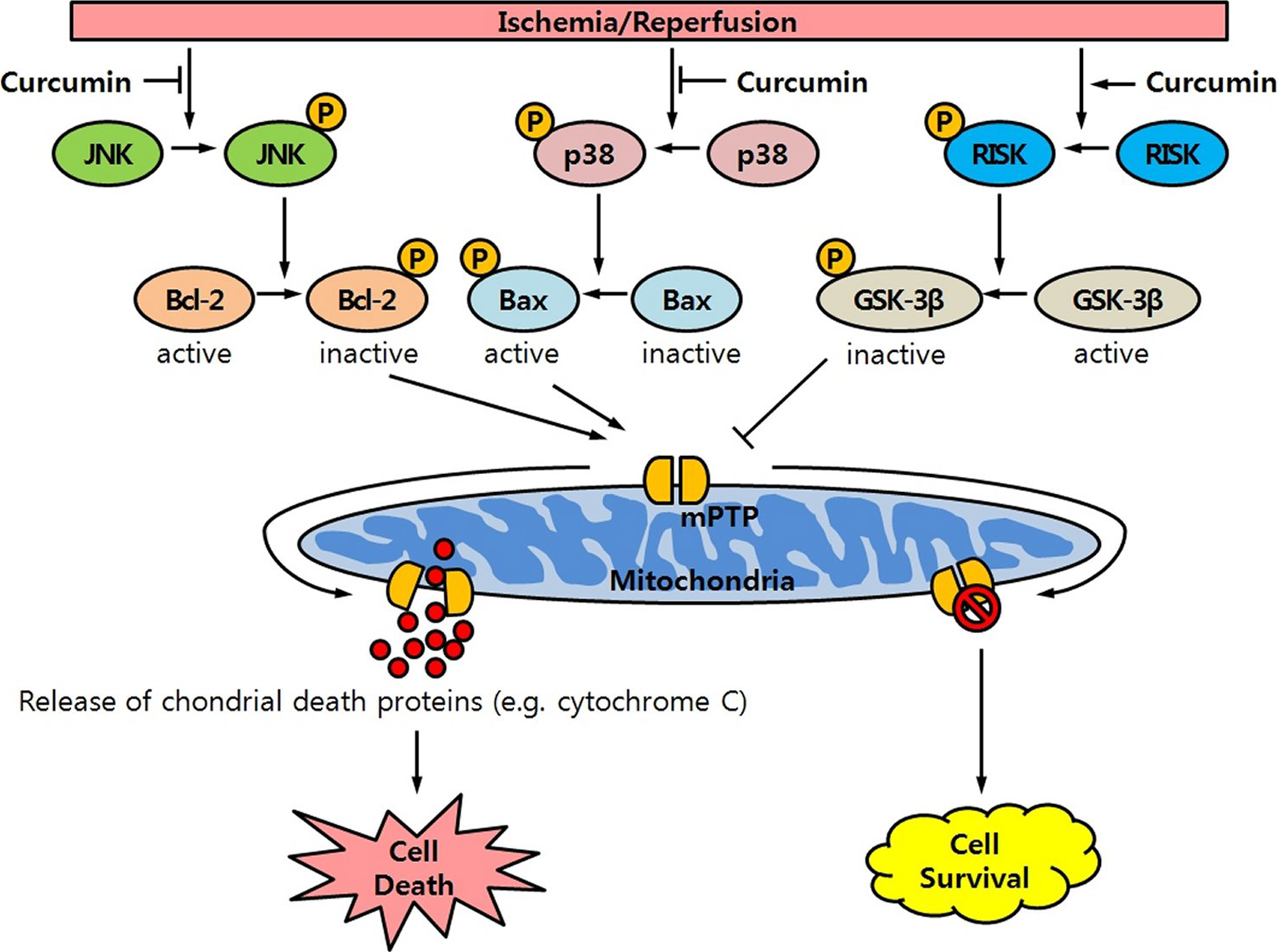
Potential signaling pathway leading to the cardioprotection of curcumin given before induction of ischemia against ischemia/reperfusion (I/R) injury in the rat heart. I/R injury will activate the stress kinase signaling pathway (JNK and p38, so-called death pathway), which is blocked by curcumin. Without curcumin, activated (phosphorylated) JNK (or p38) phosphorylates Bcl-2 (or Bax), thereby shifting the equilibrium toward a more proapoptotic state. And then, the opening of mitochondrial permeability transition pore (mPTP) will lead to the release of chondrial death proteins (ie, cytochrome c, procaspases, and apoptosis-inducing factor) and cell death. Simultaneously, I/R injury will activate the survival signaling pathway (ERK and Akt, so-called RISK pathway), which is enhanced by curcumin. Activated (phosphorylated) RISK phosphorylates GSK-3β, shifting the equilibrium toward a more antiapoptotic state. And then, the inhibition of the opening of mPTP will attenuate release of chondrial death proteins, resulting in an improved cell survival. JNK indicates c-Jun N-terminal kinases; ERK1/2, extracellular signal-regulated kinase; RISK, reperfusion injury salvage kinase; GSK-3β, glycogen synthase kinase.
The present study has a few limitations. First, there were no significant differences in any hemodynamic parameters among the groups, suggesting that the effect of curcumin cannot be attributed to hemodynamic effects. Nevertheless, the results should be qualified because coronary venous oxygen tension was not measured nor was myocardial oxygen consumption calculated. Second, additional PI3K-Akt or ERK1/2 targets besides GSK-3β may contribute to the observed cardioprotection by curcumin. In fact, Tsang et al 25 showed that pharmacologic inhibition of endothelial nitric oxide synthases, another PI3K-Akt signaling downstream target, prevented infarct size limitation in ischemic postconditioning. Nonetheless, GSK-3β is a known major regulator of mPTP activity. Third, the present results implicating a role for PI3K-Akt, ERK1/2, and GSK-3β in curcumin-induced cardioprotection were obtained in barbiturate-anesthetized rats. Whether similar effects may occur in other animal species or humans are unknown.
Conclusion
This study demonstrates that preconditioning by curcumin effectively protects the heart from regional I/R injury by reducing the infarct size in the rat in vivo. The protective effect may be related to the activation of prosurvival kinases such as PI3K-Akt and ERK1/2, and their downstream targets GSK-3β, and attenuation of apoptotic kinases such as p38 and JNK. Curcumin may have cardioprotective effects in patients undergoing surgeries prone to myocardial I/R injury. Additional research will be required to identify the role of other signaling elements previously documented to be involved in preconditioning, including PKC, ATP-sensitive K+ channel, and reactive oxygen species, and to determine whether postischemic administration of curcumin activates the RISK pathway and decreases myocardial damage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chonnam National University Hospital Research Institute of Clinical Medicine (grant no. CRI10013-1).