
Abstract
Circulating tumor DNA (ctDNA) has emerged as a clinically actionable biomarker for the management of colorectal cancer (CRC). Improvements in analytical accuracy and sequencing depth have expanded the role of ctDNA from early cancer detection to include molecular profiling of advanced disease, postoperative risk stratification, and real-time evaluation of therapeutic response and resistance. In screening and early detection settings, ctDNA-based assays integrating mutation analysis, methylation profiling, and fragmentomic features have demonstrated high specificity for CRC and multi-cancer early detection (MCED). Prospective studies suggest that ctDNA can identify CRC before clinical diagnosis; however, its sensitivity for advanced premalignant lesions remains limited, supporting its use as a complementary approach for individuals who do not participate in established screening rather than as a replacement for stool-based tests or colonoscopy. Postoperatively, ctDNA-based detection of minimal residual disease (MRD) is a strong independent predictor of recurrence and survival, often preceding radiographic evidence of relapse. Randomized trials have demonstrated that ctDNA-guided adjuvant strategies have the potential to reduce overtreatment and identify candidates for treatment escalation, although the impact on long-term outcomes remains under prospective validation. In metastatic disease, serial ctDNA monitoring enables early treatment–response assessment, detection of resistance mechanisms, and optimization of targeted therapy, including rechallenge strategies. The emerging concept of NeoRAS further illustrates the dynamic nature of tumor genomics and its therapeutic implications. Collectively, these advances have positioned ctDNA as a central tool in precision medicine. This narrative review summarizes recent clinical evidence supporting ctDNA-guided strategies for CRC and discusses their implications for the broader field of precision oncology.
Plain Language Summary
What is this review about? Colorectal cancer is a common cancer, and many people still die from it despite advances in treatment. Doctors need better ways to detect cancer early, decide who needs treatment after surgery, and monitor how well treatments are working. This review explains how a blood test called circulating tumor DNA (ctDNA) may help improve these decisions. What is circulating tumor DNA (ctDNA)? ctDNA consists of very small pieces of DNA released into the bloodstream by cancer cells. It can be detected using a simple blood sample. Because blood tests are less invasive than tissue biopsies, ctDNA can be measured repeatedly over time. How can ctDNA be used in colorectal cancer care? This review summarizes evidence showing that ctDNA can be useful at several stages of care. Before diagnosis, ctDNA blood tests can detect colorectal cancer with high accuracy, but they are not very good at finding precancerous polyps. Therefore, they should not replace standard screening methods such as stool tests or colonoscopy, but may help people who do not participate in existing screening programs. After surgery, ctDNA can detect tiny amounts of remaining cancer cells earlier than scans or standard blood markers. This can help doctors decide who truly needs additional chemotherapy and who may safely avoid it. In advanced cancer, repeated ctDNA testing can show whether treatments are working, identify early drug resistance, and help guide personalized treatment choices. Why is this important? Using ctDNA may reduce unnecessary treatments, detect cancer recurrence earlier, and support more personalized care. However, challenges remain, including cost, access, and the need for clear guidelines on when and how to use these tests. What comes next? More clinical studies are needed before ctDNA testing becomes routine in everyday colorectal cancer care.
Keywords
Introduction
Approximately 1.93 million new cases of colorectal cancer (CRC) are diagnosed worldwide each year, accounting for nearly 930,000 cancer-related deaths, ranking third in incidence and second in mortality globally. 1 Although survival has improved — most notably in high-income countries — owing to the widespread adoption of screening programs and advancements in therapeutic modalities, the prognosis of patients with advanced or recurrent disease remains poor, and further refinement of therapeutic strategies is urgently required. A considerable proportion of patients present with stage IV disease at diagnosis, and postoperative recurrence occurs in up to 60% of patients with stage II or III. 2
The introduction of molecular targeted therapies and immune checkpoint inhibitors (ICIs) has fundamentally reshaped the therapeutic landscape, and the incorporation of precision medicine based on molecular profiling has significantly increased survival rates compared to conventional chemotherapy alone.3,4 The therapeutic efficacy of anti-epidermal growth factor receptor (EGFR) monoclonal antibodies is determined by KRAS/NRAS gene mutations, with clinical responses confined to patients harboring wild-type tumors. 5 Furthermore, the BRAF V600E mutation has been identified as a poor prognostic factor and a target for rational combination therapy with molecularly targeted agents. 6 Conversely, microsatellite instability-high (MSI-H) tumors exhibit high sensitivity to ICIs, with response rates exceeding 40–71% in advanced CRC.7,8 As precision oncology has rapidly evolved, the need for accurate genomic characterization has become urgent. Conventional genomic profiling depends on tissue sampling, which has inherent limitations, including tumor heterogeneity and procedural invasiveness. 9
These limitations have led to the emergence of liquid biopsy, which enables the analysis of circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA) from body fluids10,11 and owing to its low invasiveness, it allows for serial assessments throughout the disease course. ctDNA has genetic alterations concordant with those of the tumor tissue and offers a complementary approach for tissue analysis.
12
By enabling real-time, non-invasive tracking of tumor genomic dynamics, ctDNA is a highly promising biomarker for early detection,
13
prognosis assessment,
14
treatment response monitoring,
15
and identification of resistant mutation. Its potential clinical applications now span the CRC disease continuum — from screening and early detection, through postoperative minimal residual disease (MRD) assessment, to molecular profiling and dynamic monitoring in metastatic disease (Figure 1). In this narrative review, we summarize recent advances in the clinical application of ctDNA in CRC, discuss its current limitations, and highlight future challenges. Clinical applications of circulating tumor DNA (ctDNA) across the colorectal cancer disease continuum. Schematic representation of ctDNA dynamics (y-axis: ctDNA level in plasma; x-axis: time) throughout the course of colorectal cancer (CRC) care. The dashed horizontal line indicates the analytical limit of detection of the ctDNA assay; ctDNA levels below this line are not detectable. Black arrows indicate key clinical events and decision points. Four main clinical applications of ctDNA are shown along the top of the Figure 1 Early detection: rising ctDNA signal in the pre-diagnostic period, supporting the use of ctDNA-based screening assays. (2) Assessment of minimal residual disease (MRD): following curative-intent surgery, ctDNA levels fall; postoperative ctDNA positivity (or persistence) identifies patients at high risk of recurrence and may guide the use or omission of adjuvant chemotherapy. (3) Early detection of recurrence: a secondary rise in ctDNA during surveillance typically precedes radiographic recurrence, enabling earlier intervention. (4) Treatment response and resistance: during systemic therapy for advanced or recurrent disease, serial ctDNA measurements reflect treatment response (declining ctDNA) or emerging resistance, supporting dynamic adjustment of systemic therapy
Methods
This article is a narrative review in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA). 16
Databases and search period
We searched PubMed, the Cochrane Library for English-language publications from January 1, 2005, to April 1, 2026. ClinicalTrials.gov was additionally queried to identify ongoing and recently completed trials. Proceedings of major international oncology meetings — the American Society of Clinical Oncology (ASCO) Annual Meeting, ASCO Gastrointestinal Cancers Symposium, European Society for Medical Oncology (ESMO) Congress, ESMO Gastrointestinal Congress — were searched for conference abstracts published between January 1, 2015 and April 1, 2026.
Search terms
The following key terms were combined: “circulating tumor DNA” OR “ctDNA” OR “liquid biopsy” AND “colorectal cancer” OR “colon cancer”. Additional searches were performed using the names of major clinical trials and commercial ctDNA platforms to ensure comprehensive coverage.
Selection criteria
Priority was given to: (i) randomized controlled trials; (ii) large prospective cohort studies; (iii) systematic reviews and meta-analyses; (iv) landmark translational studies defining assay performance or mechanisms of resistance. Case reports, non-peer-reviewed preprints, and studies not available in English were excluded.
Evidence synthesis
Because this is a narrative rather than a systematic review, no formal risk-of-bias assessment or quantitative pooling was performed. Instead, the authors — all of whom are practicing medical oncologists with expertise in gastrointestinal oncology — critically appraised each selected study and integrated the findings around the clinically meaningful stages of the CRC disease continuum: early detection, post-operative MRD assessment, metastatic disease monitoring, molecular profiling for anti-EGFR therapy, and the NeoRAS phenomenon. The evidence level of each cited finding is made explicit wherever this distinction is clinically relevant.
Cutting-Edge Technologies in ctDNA Analysis
Biological Basis of cfDNA and ctDNA
Cell-free DNA (cfDNA) in human blood was first reported by Mandel and Métais in 1948, 17 and in 1977, it was demonstrated that cfDNA concentrations are higher in patients with cancer than in healthy individuals. 18 ctDNA consists of tumor-derived fragments within cfDNA. One contributor to elevated cfDNA levels in patients with cancer is the presence and increased concentration of ctDNA. The half-life of ctDNA is short, typically 1–2 hours. Compared to protein markers such as carcinoembryonic antigen (CEA) (half-life ranges several days to weeks), ctDNA provides a more immediate reflection of changes in tumor burden and treatment response.19-21 Furthermore, ctDNA is minimally invasive and has a short turnaround time (TAT), potentially enabling shorter screening intervals. 22
Detection Rates and Clinical Context
The detectability of ctDNA varies depending on the primary site, metastatic pattern, tumor burden, clinical stage, and histology.15,23-25 ctDNA can be detected in more than 75% of patients with several advanced malignancies, including metastatic CRC, whereas detection rates fall below 50% in primary brain tumors, renal cell carcinoma, prostate cancer, and thyroid cancer. In localized CRC, ctDNA is detectable in approximately 73%, 26 with detection rates varying markedly by stage: approximately 40% in stage I, rising to over 90% in stages II and III. 15 In stage IV CRC specifically, pretreatment ctDNA is detectable in 80–90% of patients. 27 The detection rate drops markedly in the postoperative setting, where assays specifically designed for MRD detection are required (discussed in detail in the section on MRD). Nakamura et al. reported that ctDNA-based comprehensive genomic profiling (CGP) improved screening success rates and reduced time to test completion compared with tissue-based testing, leading to an approximately twofold increase in clinical trial enrollment. 22 Collectively, these characteristics make ctDNA a rapid and practical tool for biomarker identification in advanced CRC, with broad applications in precision oncology and clinical research.
Analytical Approaches
In these sections, we outline two frequently employed analytical approaches: polymerase chain reaction (PCR)-based and next-generation sequencing (NGS)-based assays.
PCR-Based Platforms
PCR-based analysis is widely used in clinical practice, enabling rapid and low-cost quantification of known driver mutations in ctDNA. 28 Conventional quantitative PCR (qPCR) permits relative quantification of targeted mutations, with a limit of detection (LoD) typically approximately 1% variant allele frequency (VAF). 29 Droplet Digital PCR (ddPCR) is a quantitative PCR method capable of ultra-high-sensitivity absolute quantification, enabling the detection of mutations at substantially lower allele fractions — generally around 0.1% VAF, and in optimized assays as low as 0.01% VAF.30,31 However, because ddPCR-based methods require prior knowledge of the specific mutation, they are not suitable for evaluating intratumoral heterogeneity or identifying novel resistance mutations, or performing comprehensive genomic analysis. 32 The OncoBEAM RAS CRC Kit (Sysmex, Japan), based on the highly sensitive BEAMing digital PCR technology, requires a relatively high minimum input DNA concentration. 33
NGS-Based Platforms
NGS-based assays enable simultaneous evaluation of numerous genetic alterations through broad multiplexed analysis, and they are generally classified into targeted and non-targeted approaches. 34
Tumor-Informed and Tumor-Naïve Frameworks
ctDNA assays can be categorized as tumor-informed or tumor-naïve (also referred to as tumor-agnostic or tumor-uninformed). This distinction has profound implications for analytical sensitivity, TAT and clinical use case.
In general, tumor-informed approaches are preferred for postoperative MRD assessment, 37 where high sensitivity is essential and a delay for tumor profiling is acceptable, whereas tumor-naïve approaches are preferred for molecular profiling of advanced disease and for serial monitoring of acquired resistance, where detection of newly emergent variants is paramount. These two frameworks should therefore be regarded as complementary rather than competing.
Analytical Noise and Mitigation Strategies
ctDNA analysis is impeded by germline variants and clonal hematopoiesis of indeterminate potential (CHIP).40,41 To mitigate these sources of noise, analyses are often conducted using tumor-informed approaches. Erve et al. demonstrated that ultra-deep targeted sequencing of cfDNA, which simultaneously analyzes leukocyte DNA, allows accurate identification of ctDNA in a tissue-independent manner while excluding CHIP-associated mutations. 4 42 In addition, by interrogating both tumor and normal samples, paired WGS enables comprehensive detection of somatic alterations, positioning this approach as a promising strategy to overcome these limitations. 43
Integration With Artificial Intelligence and Digital Pathology
Loeffler et al. reported that the combination of artificial intelligence (AI)-based pathological assessment and ctDNA profiling (the HIBRID approach) improved recurrence-risk prediction. 44 Negoi et al. demonstrated the feasibility of personalized surveillance schedules integrating AI and ctDNA, suggesting that monitoring intervals could be individualized rather than fixed. 45 These integrated frameworks have the potential to extend recurrence-risk assessment beyond existing clinicopathological and molecular criteria. If their clinical utility is confirmed in prospective studies, AI-integrated ctDNA analysis may emerge as a key determinant of treatment decision-making in CRC. At present, however, formal economic evaluations of AI-guided strategies remain limited, and cost-effectiveness assessment will be a critical hurdle for clinical implementation.
Major Analysis Platforms
Overview of Representative Circulating Tumor DNA (ctDNA) Analysis Platforms Organized by Technology Category
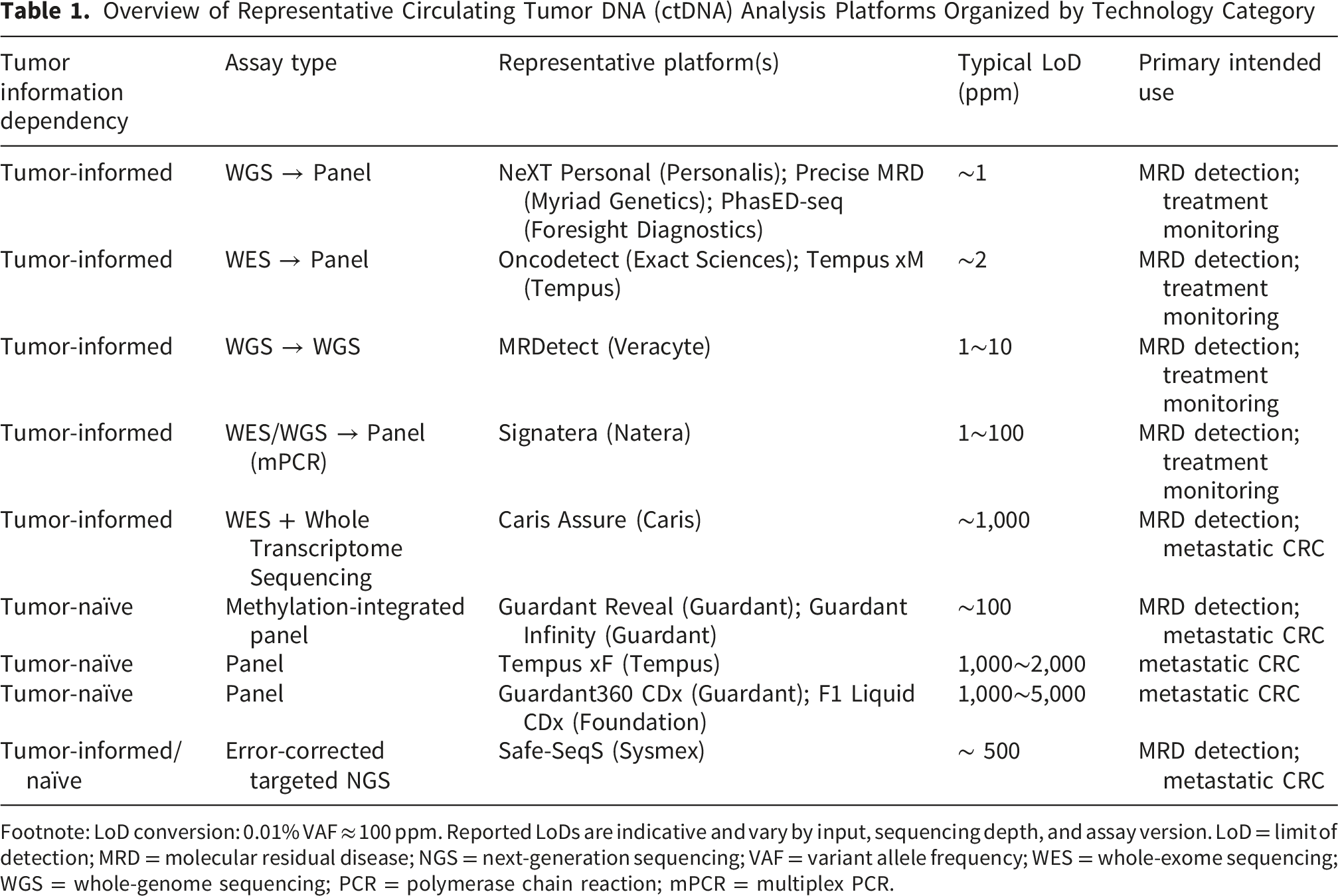
Footnote: LoD conversion: 0.01% VAF ≈ 100 ppm. Reported LoDs are indicative and vary by input, sequencing depth, and assay version. LoD = limit of detection; MRD = molecular residual disease; NGS = next-generation sequencing; VAF = variant allele frequency; WES = whole-exome sequencing; WGS = whole-genome sequencing; PCR = polymerase chain reaction; mPCR = multiplex PCR.
Tumor-informed WGS-based platforms rely on WGS that analyzes tumor-specific mutations. This strategy achieves LoD in the ppm range (∼10-6), which is the sensitivity required for reliable MRD assessment. 37 PhasED-seq (Foresight Diagnostics) combines duplex sequencing with haplotype phasing and achieves detection of VAF below 10-6. Caris Assure (Caris Life Sciences) is a blood-based cfDNA monitoring system integrated with the comprehensive molecular analysis platform called Caris Molecular Intelligence. This approach employs a tumor-informed, individualized panel design while maintaining broad genomic coverage comparable to that of WES. It enables recurrence risk stratification and longitudinal post-treatment MRD assessment and has gained increasing adoption in clinical practice, particularly in the United States. The remaining platforms are listed in Table 1.
Role of ctDNA in Early Detection
ctDNA testing is minimally invasive and generally well accepted by patients. Two strategies have been developed: CRC-specific assays and multi-cancer early detection (MCED) tests. In the HUNT study, methylated CRC-associated ctDNA could be detected in plasma up to 2 years before clinical diagnosis, 46 supporting the biological rationale for blood-based screening. To improve sensitivity and specificity, integrating additional technologies, such as fragmentomics and mutation signature analysis, is required.
Prospective Evidence in CRC-specific Screening
In the PREEMPT CRC study, among an evaluable cohort of 27,010 participants, blood tests showed 79.2% sensitivity for CRC and 91.5% specificity for advanced colorectal neoplasia, with colonoscopy as the reference standard. 47 The pivotal ECLIPSE trial demonstrated a sensitivity of 83.1% for CRC and a specificity of 89.6%; however, sensitivity for advanced precancerous lesions (APCL) was only 13.2%. 48 It is essential to recognize that these performance metrics derive from prospective screening cohorts, whereas the projected reductions in CRC incidence (∼40%) and mortality (∼52%) attributed to cfDNA-based screening are derived from modeling studies, not from prospective randomized trials, and were lower than the corresponding model-based projections for fecal immunochemical testing (FIT), colonoscopy, or multi-target stool DNA testing. Moreover, the associated costs with cfDNA- and ctDNA-based approaches were higher than those of the aforementioned approaches. 49 In a comparative analysis using the BLITZ study cohort, FIT achieved significantly higher sensitivity than cfDNA testing for APCL (31.5% vs 13.2%, P < 0.001) and approximately one-third lower false-positive rates. 50
Evidence in Multi-Cancer Early Detection
CancerSEEK, which detects eight cancer types by evaluating cfDNA mutations and circulating proteins, demonstrated a median positivity rate of 70% across all eight cancer types. Among five cancers for which no population-level screening tests were available (ovarian, liver, gastric, pancreatic, and esophageal cancers), sensitivity ranged from 69% to 98%, and specificity exceeded 99%. 51 The PATHFINDER trial enrolled 6,621 asymptomatic individuals aged ≥50 years and reported a specificity of 99.1%, a positive predictive value (PPV) of 38%, and a tumor-of-origin (TOO) accuracy of 87%. 52 The SYMPLIFY observational study within the UK National Health Service reported a sensitivity of 66%, specificity of 98%, and TOO accuracy of 85%. 53 The K-DETEK trial enrolled 9,057 asymptomatic individuals aged ≥40 years and reported sensitivity of 70%, specificity of 99%, and TOO accuracy of 52%. 54 These studies consistently demonstrate high specificity but limited sensitivity for early-stage and pre-malignant lesions. Importantly, because MCED assays are not optimized for any single cancer type, their sensitivity and specificity for CRC detection are inherently inferior to those of CRC-specific screening modalities.
Clinical Positioning
It is estimated that 75–92% of the mortality reduction achieved by colonoscopy is attributable to polyp resection rather than early cancer detection. 55 Modeling and observational data have shown that switching individuals from colonoscopy or stool-based testing to cfDNA-only screening is projected to increase CRC mortality.56,57 Conversely, offering blood-based screening to adults who would otherwise decline established methods has been shown to increase overall screening uptake by 17.5% (30.5% vs 13.0%). 58 Taken together, the current evidence supports ctDNA-based blood testing as a complement to — rather than a replacement for — colonoscopy and stool-based screening, with its primary value lying in improving uptake among those who currently refuse established modalities. Prospective randomized evaluations through the U.S. National Cancer Institute’s Cancer Screening Research Network (including the ACCESS program) 59 and ongoing Japanese initiatives (MONSTAR-SCREEN Group and Tohoku Medical Megabank Organization) will help define the role of ctDNA-based screening in the years ahead.
Frontiers in MRD Detection
In the MRD setting, the detection of post-surgical residual disease is critical for guiding adjuvant treatment and surveillance. 60 Conventional monitoring with imaging and biomarkers such as CEA lacks sufficient sensitivity to detect MRD.61-63 ctDNA reflects tumor dynamics in near real time and consistently enables MRD detection well before radiographic relapse,15,64,65 with reported median lead time of 7.3 months (interquartile range (IQR), 3.3–12.5) 66 . Optimal plasma sampling for MRD detection should be performed at least 2 weeks after curative surgery and before initiation of adjuvant chemotherapy (ACT). 67 Immediately after surgery, cfDNA elevation dilutes ctDNA, while ACT can rapidly suppress ctDNA levels. 68
As outlined earlier in this review, two analytical frameworks dominate ctDNA-based MRD assessment:
WGS/WES can simultaneously track hundreds to thousands of patient-specific targets and detect low VAF through integrated analysis. Plasma-only WES-based MRD detection has demonstrated higher sensitivity than conventional approaches and has provided insights into the mechanisms of recurrence, including immune escape. 39 WGS-based assays target the entire genome by integrating multilayered information, including single nucleotide variants, indels, copy-number changes, structural variants, fragmentomic and methylation features, with both theoretical and empirical data supporting LoDs in the parts-per-million range. 37 Tumor-informed WES/WGS approaches provide the highest specificity and resolution, making them particularly well suited for MRD detection. Tumor-naïve methylation-integrated platforms have recently narrowed the performance gap; the Caris Assure ABCDai-M&M model achieved a negative predictive value of 98% and a specificity of 76% in an independent pan-cancer validation cohort, with recurrence detected on average 261 days earlier than imaging. 69
Summary of Clinical Evidence for ctDNA-Based MRD
Multiple meta-analyses have shown that postoperative or post-adjuvant ctDNA positivity is an independent predictor of recurrence and shorter recurrence-free survival (RFS).70-73 In the prospective CIRCULATE-Japan GALAXY cohort of 2,240 patients with stage II–III colon or stage IV CRC, MRD-window ctDNA positivity significantly associated with poorer disease-free survival (DFS) (hazard ratio (HR) 11.99, 95% Confidence interval (CI): 10.02-14.35) and OS (HR: 9.68, 95% CI: 6.33-14.82). Moreover, longitudinal ctDNA dynamics in MRD-positive patients receiving ACT stratified outcomes markedly: 24-month DFS was 89.0% in patients with sustained ctDNA clearance versus only 3.3% in those with transient clearance (HR: 19.72, 95% CI: 8.61–45.17). 74 Henriksen et al. classified the rate of ctDNA increase during ACT into two categories — “fast” (143% increase/month) and “slow” (25% increase/month) — in a cohort of 168 patients with stage III CRC. When the fast-growth subgroup (n = 8) was compared with non-relapsing patients from the same cohort (n = 89), overall survival (OS) was markedly reduced (HR: 42, 95% CI: 8–221, P < 0.001), whereas the slow-growth subgroup had OS comparable to that of non-relapsing patients (P = 0.18). 75 In locally advanced rectal cancer, a meta-analysis demonstrated that ctDNA positivity at post-neoadjuvant chemoradiotherapy (CRT) or at post-surgery was strongly associated with worse RFS (post-neoadjuvant CRT: HR: 9.16, 95% CI: 5.48-15.32, post-surgery: HR: 14.94, 95% CI: 7.48-29.83) whereas baseline ctDNA levels showed only a limited correlation with long-term survival outcomes or pathological complete response. 76
Clinical Trials of ctDNA-Guided ACT
Ongoing Circulating Tumor DNA (ctDNA)-Guided Adjuvant Therapy Trials in Colorectal Cancer

Footnote: ctDNA = circulating tumor DNA; DFS = disease-free survival; XELOX = capecitabine plus oxaliplatin; FOLFOX = folinic acid, fluorouracil, and oxaliplatin; FOLFIRINOX = folinic acid, fluorouracil, irinotecan, and oxaliplatin; FOLFOXIRI = folinic acid, fluorouracil, oxaliplatin, and irinotecan; LARC = locally advanced rectal cancer.
Role of ctDNA in Metastatic Colorectal Cancer
ctDNA is increasingly integral to the management of metastatic CRC (mCRC), where it serves four distinct but complementary roles: (i) prognostic assessment and dynamic response monitoring; (ii) molecular profiling and initial treatment selection; (iii) detection of acquired resistance and rechallenge strategies; and (iv) interrogation of clonal dynamics, as exemplified by the NeoRAS phenomenon. We discuss each in turn, emphasizing how ctDNA complements rather than replaces tissue-based genomic profiling and imaging-based response assessment.
Prognostic Assessment and Treatment Response Monitoring
The clinical significance of ctDNA has been increasingly recognized for both prognostic assessment and guiding therapeutic selection and monitoring for mCRC. High baseline ctDNA levels and VAF are consistently associated with shorter OS and progression-free survival (PFS), while early on-treatment declines in ctDNA correlate with favorable outcomes. These observations are supported by prospective studies, secondary analyses of randomized trials, and multiple meta-analyses.27,98-102
In the AGEO prospective study, Bachet et al. demonstrated that baseline ctDNA was an independent prognostic factor for OS in mCRC, and that combining ctDNA mutant allele fraction (MAF) with CEA distinguished three prognostic groups with median OS (mOS) of 14.2, 21.1, and 46.4 months. 103 In a retrospective, exploratory analysis of the RECC Trial, Ohta et al. found that patients with high cfDNA concentration (median or above) before regorafenib administration had significantly shorter mOS than that of patients with low concentration. 104 Hamfjord et al. showed that high pre-treatment ctDNA allelic frequency in RAS/BRAF-mutant mCRC predicted poor prognosis independently of CEA and CA19-9 (HR: 2.38, 95% CI: 1.74-3.26, P < 0.001). 105
Early On-Treatment ctDNA Dynamics
Early on-treatment dynamics have emerged as a particularly informative biomarker. Osumi et al. demonstrated that patients whose ctDNA levels 8 weeks after initiation of second-line chemotherapy decreased to ≤50% of baseline experienced significantly longer PFS and OS than those with smaller declines. 106 Ghidini et al. reported that ctDNA normalization (≥99% reduction) at one month after treatment initiation was associated with markedly improved OS (45.6 vs 22.6 months, P = 0.01) and PFS (13.9 vs 10.7 months, P = 0.036) than those of the non-normalized patients. 107 Lim et al. analyzed ctDNA in patients with KRAS/NRAS wild-type mCRC receiving cetuximab-containing regimens and observed significant correlations between changes in ctDNA VAF and tumor size at first response assessment. At the time of disease progression, 54 new emergent mutations, including KRAS and MAP2K1, were identified. 108 Kim et al. reported that ctDNA disappearance during first-line therapy predicted prolonged PFS independently of radiographic response, and meta-analyses have confirmed that early, maximal ctDNA reduction correlates with longer PFS and OS. 98 Notably, ctDNA progression preceded radiographic progressive disease (PD) in 58.1% of patients, with a median lead time of 3.3 months. 109 In immunotherapy, a secondary analysis of SAMCO-PRODIGE54 trial demonstrated that baseline ctDNA levels were not predictive of outcomes; however, early ctDNA changes at one month were significantly associated with PFS and OS, particularly in the avelumab arm. 110 Grancher et al. showed that early ctDNA reduction predicted improved survival regardless of doublet versus triplet chemotherapy. 111 In late-line settings, elevated ctDNA levels prior to or during FTD/TPI or regorafenib therapy have been associated with reduced survival.104,112,113
Concordance and Discordance With Tissue
The overall concordance between primary tumor and plasma ctDNA genomic profiles is approximately 86.4%, but this varies markedly depending on the tumor burden and by metastatic site. 33 High concordance rates are particularly observed in liver metastases, reflecting their high ctDNA shedding, whereas it is lower in lung and peritoneal metastases, resulting in reduced mutation detection rates and lower plasma concordance.66,114 Therefore, hybrid surveillance integrating imaging, CEA, and ctDNA may be recommended in mCRC patients with lung and peritoneal metastases. 76 In mCRC, plasma tumor mutation burden (TMB) ≥28 mutations/Mb predicted response to durvalumab plus tremelimumab, whereas tissue TMB did not, suggesting that plasma-derived metrics may capture clinically relevant biology not reflected in single-site tissue sampling. 115
Molecular Profiling and Initial Treatment Selection
ctDNA-based genomic profiling enables minimally invasive identification of biomarkers for first-line treatment selection.
The PRESSING study identified genomic alterations responsible for primary resistance to anti-EGFR monoclonal antibodies (mAbs) in RAS/BRAF wild-type mCRC, including HER2/MET amplification, ALK/ROS1/NTRK1-3/RET fusions, and PIK3CA mutations, and proposed a “negative hyper-selection” strategy that refines patient selection beyond conventional RAS/BRAF wild-type status. 116 Comprehensive plasma analysis of ctDNA has demonstrated that resistance-associated alterations frequently coexist as subclones within the same patient. This subclonal coexistence often cannot be fully captured by tissues alone. 117
Exploratory analyses of the phase III PARADIGM trial demonstrated that the absence of known resistance mechanisms in plasma ctDNA (RAS, NRAS, PTEN, and EGFR extracellular domain (ECD) mutations; HER2 and MET amplifications; and ALK, RET, and NTRK1 fusions) strongly predicted benefit from anti-EGFR mAb therapy, irrespective of primary tumor sidedness. 118 The CAPRI-2 GOIM trial reported that patients with negative results in both tissue and liquid CGP achieved significantly superior objective response rate (ORR) and PFS, supporting the complementarity of the two approaches. 119 In the FIRE-4 trial, ctDNA detected RAS mutations in some cases that were initially classified as wild-type by tissue biopsy, suggesting that ctDNA may offer higher sensitivity for detecting RAS mutations than that of tissue-based methods and may improve eligibility assessment for anti-EGFR therapy. 120
Resistance Detection and anti-EGFR Rechallenge
During anti-EGFR therapy, resistance mutations in RAS, BRAF, and EGFR emerge and contribute to acquired resistance.121,122 However, these resistant clones often decline during anti-EGFR-free intervals, restoring sensitivity and providing a biological rationale for ctDNA-guided rechallenge (Figure 2).
123
Conceptual model of acquired resistance and NeoRAS conversion during systemic therapy for metastatic colorectal cancer. Each circle represents a tumor-cell population; white cells denote anti-epidermal growth factor receptor (EGFR)-sensitive clones, whereas blue cells denote anti-EGFR-resistant clones. The intensity of blue shading reflects the relative abundance of resistant subclones within the tumor. 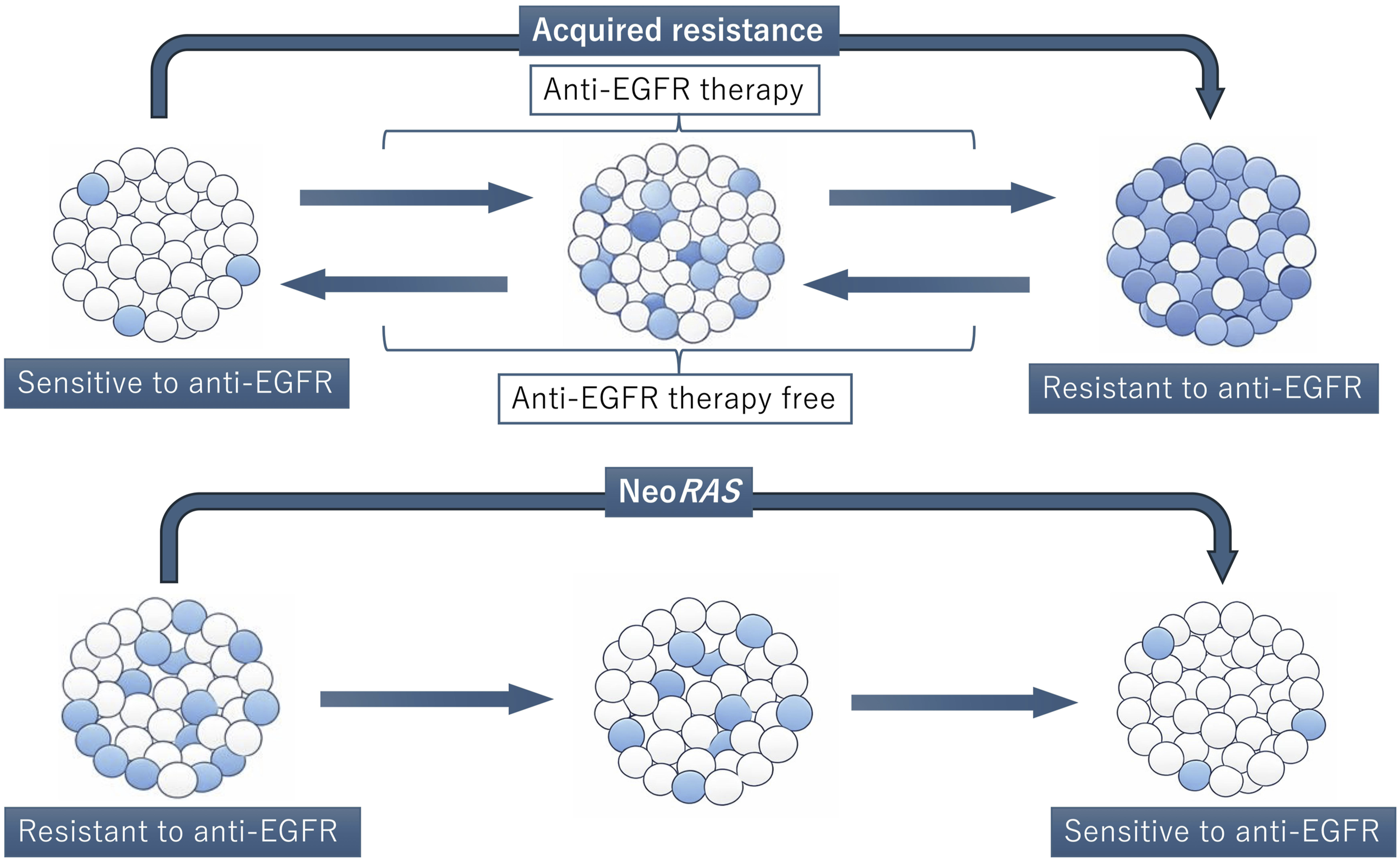
The efficacy of readministering anti-EGFR mAb was prospectively demonstrated in the CRICKET trial, 124 and similar findings were confirmed in the E-Rechallenge 125 and the JACCRO CC-08/09 trials. 126 In the CHRONOS trial, patients were screened using ctDNA to exclude resistance alterations, including RAS, BRAF, and EGFR-ECD mutations, before receiving a panitumumab rechallenge. Among patients without resistant mutation to anti-EGFR therapy, the ORR was 30% and the disease control rate (DCR) was 63%, both exceeding outcomes typically observed with standard third-line therapies. 127 The REMARRY/PURSUIT trial administered irinotecan plus panitumumab to patients who did not harbor RAS mutation and had previously responded to anti-EGFR mAb but subsequently developed resistance, resulting in a median PFS (mPFS) of 3.6 months and a mOS of 12 months. Patients in whom plasma RAS mutations re-emerged during therapy did not respond, exhibiting significantly shorter PFS and OS. 128 In the RASINTRO trial, patients with RAS/BRAF wild-type ctDNA at the time of treatment reinitiation demonstrated significantly longer PFS and OS than those with mutant ctDNA. Furthermore, patients exhibiting an early ctDNA reduction of ≥50% experienced significantly prolonged PFS and OS. 129 The CITRIC trial reported that patients confirmed to be RAS/BRAF/EGFR-ECD wild-type by ctDNA analysis, showed significantly higher response rates and DCR from cetuximab rechallenge than from investigator’s choice. 130 The FIRE-4 trial demonstrated that readministration of FOLFIRI plus cetuximab resulted in a higher ORR, although no significant difference was observed in PFS or OS compared to the investigator’s choice. 131 The PARERE trial evaluated the optimal sequencing of regorafenib and panitumumab in patients who previously benefited from anti-EGFR mAbs, received at least one intervening EGFR-free regimen, and were confirmed to be RAS/BRAF wild-type by ctDNA prior to readministration. Although OS did not differ between treatment sequences, panitumumab produced favorable ORR, DFS, and PFS regardless of the sequence. 132
Circulating Tumor DNA (ctDNA)-Guided Anti-epidermal Growth Factor Receptor (EGFR) Monoclonal Antibodies (mAbs) Rechallenge Trials in Metastatic Colorectal Cancer

Footnote: ctDNA = circulating tumor DNA; EGFR = epidermal growth factor receptor; mAbs = monoclonal antibodies; PCR = polymerase chain reaction; ddPCR = droplet digital PCR; qPCR = quantitative PCR; NGS = next-generation sequencing; NA = not available; ORR = overall response rate; PFS = progression-free survival; OS = overall survival; FOLFIRI = folinic acid, fluorouracil, and irinotecan.
NeoRAS Wild-type Metastatic Colorectal Cancer
NeoRAS refers to the apparent conversion from a RAS mutant-type to a RAS wild-type status during systemic therapy, raising the possibility that initially ineligible patients may become candidates for anti-EGFR therapy (Figure 2).138,139 The reported incidence of NeoRAS conversion varies widely across studies, reflecting heterogeneity in assay sensitivity and patient selection. Moati et al. re-analyzed RAS-mutant mCRC patients from the PLACOL cohort and required orthogonal markers of ctDNA shedding — additional somatic mutations or methylation signatures (WIF1, NPY) — to confirm the detection of ctDNA at the time of RAS assessment, in order to exclude false negative cases. With this method, only 5.5% of patients were classified as NeoRAS wild-type. 140 In contrast, Klein-Scory et al. defined conversion by a drop in plasma RAS MAF below the ddPCR detection threshold, without requiring orthogonal confirmation. They reported NeoRAS conversion in 91% of patients with stable disease (SD) or partial response (PR) on first-line therapy. 141 This difference highlights how strongly the apparent NeoRAS rate depends on whether the assay incorporates markers that distinguish true biological RAS clearance from low ctDNA shedding.
Nicolazzo et al. identified bevacizumab as the only independent factor associated with the NeoRAS phenomenon and proposed that bevacizumab-induced hypoxia enhances the sensitivity of RAS-mutant cells to reactive-oxygen-species-mediated cell death. 142 Osumi et al. evaluated 107 patients with chemotherapy-refractory mCRC and observed NeoRAS conversion in 21.5%; the absence of liver metastases, smaller tumor size, and mutations outside KRAS exon 2 were significantly associated with the conversion. 143 In a sub-analysis of 478 RAS-mutant cases from the GOZILA study, the absence of liver or lymph node metastases and tissue RAS mutations other than KRAS exon 2 mutations significantly correlated with NeoRAS conversion. Although treatment outcomes were limited, anti-EGFR mAb therapy was effective in some NeoRAS wild-type cases, with one PR and two SDs lasting 6 months or longer. 144
Ongoing Trials Assessing NeoRAS in Metastatic Colorectal Cancer

Footnote: rtPCR = real-time PCR; ORR = overall response rate; PFS = progression-free survival; FOLFIRI = folinic acid, fluorouracil, and irinotecan.
Limitations and Future Perspectives
Despite the remarkable progress summarized above, several important limitations must be acknowledged when considering clinical implementation.
Analytical heterogeneity and lack of standardization
Currently available platforms differ substantially in analytical design, LoD, input requirements, TAT, and cost, and there is no internationally harmonized reference standard for ctDNA quantification. Reported sensitivities are often not directly comparable across assays. Cross-platform standardization and external quality assessment programs are needed to support meaningful comparison and routine clinical integration.
Clonal hematopoiesis of indeterminate potential (CHIP)
CHIP-derived mutations can be detected in plasma cfDNA and may be misattributed to tumor-derived ctDNA, particularly in tumor-naïve assays operating at low allele fractions. This is a clinically meaningful source of false-positive calls in the MRD and early-detection settings. Paired sequencing of cfDNA with matched leukocyte DNA is currently the most robust mitigation strategy and should be regarded as a methodological standard.
Reduced sensitivity in lung and peritoneal metastases
ctDNA shedding is substantially lower in lung and peritoneal metastatic disease than in liver metastases. In these subgroups, false-negative plasma results are clinically meaningful, and ctDNA-negative surveillance should not be interpreted as evidence of remission. Hybrid surveillance combining imaging, CEA, and ctDNA is recommended in these patients, and these limitations should be explicitly communicated.
Cost, access, and health-economic evidence
High-sensitivity ctDNA assays remain costly, and access varies substantially across countries and health-care settings. This unevenness risks exacerbating existing inequities in access to precision oncology. Rigorous health-economic evaluations are still limited and are urgently needed to define the patient populations and clinical scenarios in which ctDNA-based strategies provide the greatest clinical and economic value.
Lack of harmonized clinical cutoffs
Although positive/negative calls and longitudinal dynamics are widely used to guide treatment decisions in clinical trials, no universally accepted quantitative cutoffs exist for clinically actionable ctDNA positivity, clearance, or conversion. The definition of “sustained clearance,” the optimal sampling intervals, and the timing at which ctDNA should trigger a treatment change remain areas of active investigation. Until prospective validation defines these parameters, ctDNA results should be interpreted within the context of imaging, established biomarkers, and the individual patient’s clinical trajectory.
Implications for future research
These limitations define a clear agenda for the next generation of ctDNA studies in CRC: platform harmonization and external quality assurance; the development of composite biomarkers that combine ctDNA with imaging, CEA, and AI-based pathology to overcome the sensitivity gap, especially in non-liver metastatic disease; rigorous health-economic evaluation to inform equitable access; and the prospective definition of standardized clinical cutoffs through well-designed randomized trials. Addressing these gaps will be essential to realize the full promise of ctDNA as a central tool in the precision management of CRC.
Conclusion
ctDNA has become a prognostic and monitoring biomarker for early cancer detection and postoperative assessment of MRD, whereas its role in modifying treatment decisions — including escalation and de-escalation of ACT — is supported by promising early data but remains under prospective validation. In the context of early diagnosis, ctDNA-based assays offer high specificity and patient acceptability; however, their limited sensitivity to precancerous lesions supports their use as a complement, rather than a replacement, for stool-based testing and colonoscopy. For postoperative and distant metastasis cases, dynamic ctDNA measurements at multiple time points, rather than a single assessment, are essential for accurate prognosis prediction and optimal treatment decisions. In metastatic disease, dynamic, multi-time-point ctDNA assessment enables prognostic stratification, response monitoring, resistance detection, and rational rechallenge with anti-EGFR therapy. Realizing the full clinical potential of ctDNA will require overcoming the limitations outlined above and integrating ctDNA into existing diagnostic, imaging, and therapeutic frameworks rather than replacing them. Addressed thoughtfully, these challenges position ctDNA as a central pillar of precision oncology in colorectal cancer.
Footnotes
Acknowledgments
Ethical Considerations
This article is a narrative review of previously published literature and does not involve any new studies of human participants or animals performed by any of the authors.
Author Contributions
Keito Suzuki: Conceptualization, Literature search, Writing – original draft, Writing – review & editing. Akira Ooki, Eiji Shinozaki, Eiichiro Toyokawa, Kaoru Yoshikawa, Manabu Shiozawa, Shin Maeda, Kensei Yamaguchi: Writing – review & editing. Hiroki Osumi: Conceptualization, Writing – review & editing, Supervision. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new data were generated or analyzed in support of this review. All data discussed are available in the cited published sources.