
Abstract
Introduction
Poor diet and excess weight have been linked to increased risk for at least 13 types of cancer. Culinary medicine utilizes experiential cooking skill development to improve individuals’ capacity for healthy eating. Digital communication strategies offer pathways for scalable culinary medicine interventions, but little research has explored how online cooking tools could be leveraged for cancer prevention messaging. We conducted a cross-sectional survey study exploring online cooking information-seeking habits and content preferences among participants in four cancer prevention and control cohorts to inform future digital culinary medicine interventions.
Methods
A cross-sectional survey study was conducted with a convenience sample of participants from four existing cohort studies being undertaken at the University of Texas MD Anderson Cancer Center. Survey items examined current cooking practices, online cooking information-seeking behavior, digital intervention content preferences, and evaluation of three online cooking videos. Descriptive statistics were used to summarize findings, and open text comments were examined using rapid thematic analysis to add further context.
Results
Most of the 102 respondents were women (99%), with a mean age of 58 years old. Many (78.4%) reported preparing meals at home ≥4 days per week. Search engines were the most common way recipes were identified online and the majority of respondents reported cooking from online videos some or all of the time. Participants gave the highest overall ratings to the 2-4 minute cooking video and highlighted the host personality and video production as important aspects of online cooking video content.
Conclusions
The findings of this study offer insight to inform the development of digital culinary medicine tools for MD Anderson’s cancer prevention and control cohorts.
Introduction
Diet quality and weight management are important modifiable risk factors for over 13 types of cancer. 1 Home cooking frequency has been associated with lower rates of obesity, better diet quality, as well as lower food costs,2,3 highlighting the potential for culinary medicine programs in the context of cancer prevention and control.4,5 Aligned with the broader Food is Medicine movement, culinary medicine uses cooking skill development to promote healthy eating by teaching strategies for increasing cooking frequency and improving the nutritional quality of home-cooked meals (e.g., teaching how to substitute red meat with lean meats or deep frying with baking). 4 Although various intervention programs that promote healthier cooking skills have been implemented, most rely on in-person classes taught in teaching kitchens.6-8 One analysis of the cost of building and launching an academic teaching kitchen ($755 per participant in 2020) highlights the investment in infrastructure, staffing, and maintenance required for these programs. Cost issues may limit scalability of culinary medicine programs to broader audiences. 7
Digital platforms may provide a salient and scalable way to communicate culinary medicine content that takes advantage of increasing consumer interest in online cooking information. 9 The internet is an important resource for cooking information, mainly in the form of online recipes and instructional videos.10-12 Additionally, over one-third of respondents in a nationally representative survey study reported learning to cook from online resources such as blogs and instructional videos. 13 Digital culinary medicine interventions may be able to leverage the popularity of food media by identifying the key characteristics of online content that consumers find appealing and motivating. The objective of this study was to examine cooking information-seeking habits and preferences related to online culinary medicine content across four diverse cancer prevention and control cohorts. The goal of this work is to inform the development of digital culinary medicine interventions for cancer prevention.
Methods
Participants and Recruitment
This cross-sectional study aimed to examine online cooking information-seeking habits and preferences to inform future digital culinary medicine intervention content. This report conforms to the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) reporting guidelines. Participants were recruited from four existing cohort studies housed at the University of Texas MD Anderson Cancer Center over approximately four months: Project CHURCH (African American church members; n=2,500), 14 the Mexican American Cohort (first and second generation immigrants of Mexican origin; n=26,600), 15 the High Risk Breast Cancer Cohort (women at increased risk of breast cancer; n=2,000), and the MERIT Cohort (women aged 25-80 who receive annual mammograms; n=6,000). A convenience sample of 25 individuals per cohort were targeted for this study. Given the descriptive and hypothesis-generating nature of this study, no formal sample size calculation was conducted. Cohort participants were contacted via email and/or through existing participant communication channels used to communicate with each cohort (such as newsletters), alerting them to the opportunity to participate by completing an online survey. Active recruitment for each cohort was suspended after 25 participants completed the survey, although additional participants from recruitment efforts were able to participate and were included in the analysis. Participants were compensated $10 for their time and participation. This study was approved by the MD Anderson Institutional Review Board, PA19-0145. Written informed consent was obtained from all participants.
Survey
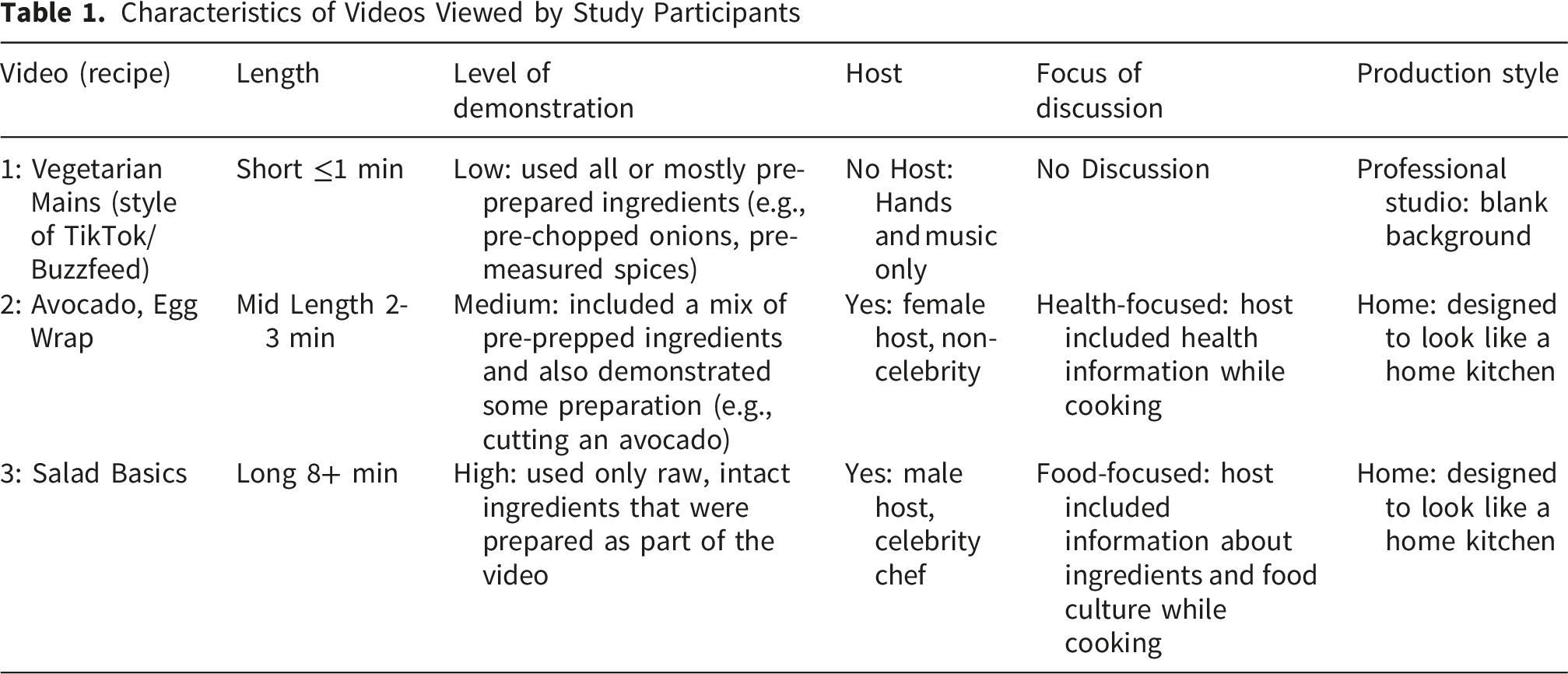
Characteristics of Videos Viewed by Study Participants
Participants also completed the Healthy Cooking Questionnaire II (HCQ2), 16 a 20-item self-assessment of cooking quality that yields a summative Healthy Cooking Index (HCI) score. 4 Described elsewhere, 16 the HCQ2 examines cooking practices that have the potential to impact the nutritional value of home prepared foods. Points are awarded for positive behaviors such as cooking with fresh herbs and spices (+1 point) and negative behaviors such as deep frying (-1) for a possible summative HCI score from (-9 to +10). Previous studies have demonstrated that HCI scores are associated with higher nutritional quality of home prepared meals and favorable dietary behaviors.4,17
Analysis
Sociodemographic and closed-ended cooking information seeking items were assessed using descriptive statistics, including frequencies and means/standard deviations as appropriate. Open-ended comments were analyzed using rapid qualitative analysis, driven by the main research aim of identifying actionable recommendations and considerations for the development of online cooking materials. HCQ2 responses were coded using established guidelines. 4 All items were then summed to create a total HCI score.
Statement of Declarations
Ethical Statement
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by MD Anderson Institutional Review Board, PA19-0145. Written informed consent was obtained from all subjects/patients.
Authors’ Contribution
MR analyzed the data and wrote the original draft of the manuscript. SF coordinated the study and analyzed data. MR, LS, CDM, LM, and KBE formulated the research question and designed the study. MV supported the manuscript development, editing, and proofing. All authors have significantly contributed to this manuscript, approved the final copy, agree on the content, and accept full responsibility for all aspects of the work.
Funding
Funding was supported by the Duncan Family Institute for Cancer Prevention and Risk Assessment. Additionally, this project was supported by the MD Anderson Center for Energy Balance in Cancer Prevention and Survivorship, and the National Institutes of Health (NIH) National Cancer Institute (NCI) under award number P30 CA016672.
Results
Participant Characteristics and Cooking Behaviors (Table 2)
A total of 107 individuals participated in the survey study, n=102 were included in the analysis (English only, Spanish responses n=5 (4.4%) were excluded). The mean age of the sample was 57.9 years (SD= 12.3) and all but one were female. Most, 70.6% of respondents reported having a Bachelor’s degree or above. The mean HCI score for the sample was 4.9 (SD=2.1), out of a possible range of -9 to +10. Individual HCI behaviors were averaged across the sample to show the most common cooking behaviors reported on the HCQ2 (Figure 1). Reported cooking behaviors based on the Healthy Cooking Questionnaire II. Red background indicated negative or less healthy cooking behaviors, green background indicated positive or more health promoting cooking behaviors Characteristics of Survey Respondents (N=102) a) option was select all that apply b) n=100 (n=2 missing data).

Cooking Information-Seeking Behaviors (Figure 2)
Search engines were the most common way respondents identified recipe videos online, followed by social media and specific websites. Other sources included friends and two individuals wrote in “Pinterest” as a specific source. When asked how often they cooked from online videos, 73.3% of respondents noted cooking from online videos sometimes or all the time. Respondents indicated that online recipe sites were looked at often, with 34.7% reporting looking at content one or more times per week, while 13.5% and 14.2% reported looking at cooking TV shows or printed cookbooks one or more times per week, while 9.2% of respondents noted never looking at online recipe sites. In addition, 38 individuals responded to an optional, open-ended question that gave respondents an opportunity to share their favorite cooking resources; 6 individuals mentioned Pinterest or Facebook as preferred sources, and 6 mentioned cooking tv shows. Online cooking information seeking and usage. (A) Bar graph depicting where respondents find recipes online, (B) bar graph depicting how often respondents report cooking from online recipes, (C) stacked bar graph depicting how often respondents look at online, TV, and print cooking resources
Feedback on Cooking Videos
Overall response to embedded cooking videos (Table 1) is shown in Figure 3. Video 1 (Vegetarian Mains) received the least positive feedback, with 41.3% of the sample giving the video an A+, A, or A-rating. This video also received the most negative feedback, with 13.8% of the respondents giving this video a D+, D, D- or F rating. Participants were asked to write positive comments about the video (in response to the question: What did you like about Video #?) and negative comments about the video (in response to the question: What did you dislike about Video #?). Written comments about Video 1 included 92 positive comments on the video and 88 negative comments on the video. Positive comments mentioned the clear instructions (I like step-by-step action with each ingredient shown as needed) and production quality (Colorful, fast paced, made food look easy to make). Other positive comments highlighted the multiple options given in the video (Variety of recipes that are quick and simple to make) and the likelihood that they would try them at home (Excellent recipes! My family would love any of these; Different from what I normally eat but looks good.) Negative comments included the video pace (It was way too fast for me to absorb the information), and lack of host (I would prefer a host that narrates). Other negatives centered on the practicality of the video structure (Not a real recipe, I could not cook using this video; Would have to start and stop to get all the ingredients down). Stacked bar graph depicting response to cooking videos by consolidated grade ranking
Video 2 (Avocado and Egg Wrap) received an A+/A/A-level rating from 65.1% of all participants. Video 2 received 92 positive comments and 60 negative comments. Positive comments noted the length (Short and to the point.), the information given during the video (Tips on why certain ingredients are good for you), the production quality (I liked the visuals of the ingredients), and the clarity of the demonstration (Easy to follow, looked yummy and I loved all the ingredients). Other comments noted some less positive response to the host personality (Host is a little too perky sometimes). Several negative comments were specific to recipe ingredients, including potential issues with access (I am not a fan of avocado, so it did not pertain to me; Avocado is expensive in some areas so I would encourage a substitute for it if the target audience are communities of color with not much access to healthy food).
Video 3 (Salad Basics) received similar responses to Video 2, with 65.1% of all respondents giving the video an A+/A/A-level rating. Participants wrote in 96 responses to what they liked about Video 3, and 61 responses to what they did not like about the video. Positive comments noted the level of demonstration and perceived flexibility (He gave us a starting place, and we could add whatever we want to make it better), the information given during the demonstration (He really threw in a lot of good advice on what makes the salad work), the production style (Looked like he was in a home kitchen), as well as the host’s personality ([host name redacted] knows what he is doing, gave good advice and was funny). Negative aspects commented on included the length of the video (Too long to sit through a salad video). Several participants also commented on the host’s behavior as distracting.
Discussion
This cross-sectional study examined current cooking information seeking behaviors and preferences for digital content. This study revealed high utilization of online recipes and high frequency of preparing meals at home among participants in four diverse cohort study populations. While our findings indicated high cooking quality overall, the HCQII revealed some areas for improvement that could be addressed through digital culinary medicine content, including low use of olive/canola oil and whole grains, as well as high use of processed foods and animal fat. Participants noted reliance on search engines, social media and specific websites for content, and responded positively to mid-length and longer cooking videos that included health information and cooking tips, as well as personable hosts.
This study offers novel insight into the potential for communicating health information through cooking resources. Existing interventions that have utilized technology for delivering culinary medicine content offer context to our findings. A small number of mobile cooking applications have been piloted, and findings indicate that recipe collection features are more popular than nutritional advice features,11,18 emphasizing the appeal of cooking content as a potential method for communicating health information.11,12 Our findings indicated frequent engagement with recipe sites, and approximately 2 out of 3 respondents noted cooking from online videos sometimes or all the time.
Instructional cooking videos have been used for virtual cooking education.19,20 Adam et al delivered a video-based integrated nutrition and cooking course to the general public through an online platform. Over 7,000 people completed the course, with childbearing-aged women aged 20 to 49 making up the majority of participants. 20 Our population was also predominately female but older (mean age = 57.9), and our findings of high frequency of preparing meals at home and high utilization of online cooking content suggests digital recipe and instructional video content may be feasible and acceptable for older women as well. Additional phenomenological research with men that explores cooking behaviors and interaction with online cooking media may be needed to support health education materials and interventions for that population.
In addition, written-in comments on cooking videos in the survey noted how cooking videos with various structures offered easy to follow instructions, interesting and engaging information, and attractive visuals. Many positive comments centered on the attractiveness of the visuals, and the information provided regarding health or food culture facts. Negative comments often centered on the host, the ease of using the video to cook, or objections to specific foods. These findings may support the development of health education videos that utilize cooking graphics to communicate healthy eating information.
Culinary medicine content is relevant to cancer prevention through the impact of home cooking practices on the nutrient content of prepared foods, bioavailability of micronutrients, and the production of and exposure to human carcinogens. 21 Our group and others have successfully piloted in-person culinary medicine interventions targeting cancer populations.22-25 Digital resources may offer avenues to more scalable interventions for participants at high risk for cancer that may lack access to hospital or community-based programs. Some recipe and cooking focused websites targeting cancer populations have emerged,26,27 but little research has explored the efficacy of these resources in promoting cancer preventive dietary behaviors. The current study adds to the early literature regarding cooking information seeking online.
There are several limitations to this study including the use of an online survey, which limits in-depth understanding of participant behavior. Our study population, though diverse with regard to race/ethnicity, was relatively small and education level was relatively high, which may limit our conclusions. The small sample size hindered our ability to examine differences by race/ethnicity, sex or age. Health literacy was not measured, which may impact how participants respond to the videos. In addition, a small number of videos were evaluated and were not selected based on specific theoretical frameworks of health behavior. Additionally, assessment of the videos were not completed using validated tools, thus limiting the conclusions we can draw regarding participant preferences. The removal of the Spanish language responses is a limitation in terms of cultural and linguistic generalizability. The participants in cohort studies may represent a population that is more interested in health, adding a potential bias to our recruitment and limiting generalizability to the broader population. However, the information generated by this study will inform the development of educational resources to be distributed through the participating cohorts.
Conclusions
Digital communication strategies may be an acceptable way to promote healthy eating among adults participating in 4 cancer prevention and control cohort studies. The next step of this project is to develop and pilot test cooking videos embedded with cancer prevention information. These informative healthy cooking videos will serve as educational tools to promote cancer preventive dietary behaviors. Pilot testing these videos and other culinary medicine resources will inform the development of a larger digital culinary medicine intervention for cancer prevention and control. Further research is needed to understand how digital culinary medicine content impacts home cooking behavior and downstream correlates of health relevant to cancer risk.
Footnotes
Ethical Considerations
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by MD Anderson’s Institutional Review Board, PA19-0145.
Consent to Participate
Written informed consent was obtained from all subjects/patients.
Author Contributions
Margaret Raber analyzed the data and wrote the original draft of the manuscript. Sara Fares coordinated the study and analyzed data. Larking Strong, Carrie Daniel-Macdougall, Lorna McNeill, and Karen Basen-Engquist formulated the research question and designed the study. All authors have significantly contributed to this manuscript, approved the final copy, agree on the content, and accept full responsibility for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was supported by the Duncan Family Institute for Cancer Prevention and Risk Assessment. Additionally, this project was supported the University of Texas MD Anderson Cancer Center for Energy Balance in Cancer Prevention and Survivorship, and the National Institutes of Health (NIH) National Cancer Institute (NCI) under award number P30 CA016672.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.