
Abstract
Introduction
Breast cancer (BC) is a leading cause of death and has become an emerging issue for global public health. We aimed to explore and identify the modifiable factors associated with delayed diagnosis among patients with BC in Pakistan.
Methods
An epidemiological analytical cross-sectional study was conducted on patients with BC undergoing chemotherapy at a specialized cancer hospital in Punjab, Pakistan. Data on demographic characteristics and factors associated with delayed diagnosis were collected directly from patients using a self-structured questionnaire. Simultaneously, tumor-related information was obtained from their medical records. Chi-square test and forward stepwise binary logistic regression were applied to find out association and statistical significance.
Results
Of the 490 BC patients analyzed, 68.6% experienced diagnostic delays. Multivariable logistic regression identified several significant predictors of delay: high diagnostic costs (AOR = 0.627; 95% CI: 0.403-0.976; P = 0.039), consultation with traditional healers (AOR = 0.317; 95% CI: 0.196-0.512; P < 0.001), and negligence toward the disease (AOR = 2.35; 95% CI: 1.30-4.28; P = 0.005). Financial problems showed a borderline association (AOR = 0.634; 95% CI: 0.398-1.009; P = 0.055).
Conclusion
Delayed BC diagnosis was significantly associated with high diagnostic costs, consultation with traditional healers before diagnosis, and patient negligence.
Introduction
Breast cancer (BC) is the most common cancer among females, accounting for 11.7% of the 19.3 million newly diagnosed cancer cases in 2020. BC is a leading cause of death and has become an emerging issue for global public health. About 2.3 million females have been newly diagnosed with BC, whereas 0.685 million mortalities are being reported worldwide. 1 According to an estimate, new cases of BC could be increased by over 3 million, whereas about 1 million deaths are predicted per year by 2040. 2
An increasing trend regarding incidence of BC has been shown in low- and middle-income countries (LMICs). 2 The incidence of BC in LMICs is lower than that of high-income countries (HICs), but higher mortality rate compared to HICs. 3 Evidence shows that late-stage diagnosis of BC is common, with less than 50% of cases detected at early stages in LMICs, whereas approximately 70% of stages I and II BC cases has been diagnosed in HICs. 4 Diagnosis is important at an early stage and timely treatment are proposed for a better prognosis, to overcome the severity of the disease, and improve the survival of BC patients. BC patients who experience a delay of 12 to 26 weeks from the onset of symptoms to consultation have lower survival rates compared to those with delays of less than 12 weeks. 5 Delay diagnosis of disease is a common practice in Pakistan that leads to BC related high mortalities. 6 Late-stage diagnosis of BC is 1 of the leading cause of mortality among Pakistani females. 7
Various studies have investigated potential factors affecting the diagnosis of BC. These factors include fear related to a BC diagnosis, 8 and consulting traditional healers about BC before seeking diagnostic tests, 9 ignorance, geographical location, socio-cultural characteristics, and poverty. 10 Limited data is available in Pakistan, therefore, we planned to focus on modifiable factors contributing to the delayed diagnosis of BC, to promote early detection and reduce late-stage BC in Pakistan. The objective of the current study was to explore and identify the modifiable factors associated with delayed diagnosis among patients with BC in Pakistan.
Methods
Study Design and Setting
The current study was an epidemiological analytical cross-sectional study that followed STROBE guideline for the reporting. 11 This study was carried out on the patients with BC who were visiting the Institute of Nuclear Medicine and Oncology Lahore (INMOL) Cancer Hospital, Lahore, Punjab, Pakistan. INMOL is a tertiary cancer hospital that was established by the Pakistan Atomic Energy Commission (PAEC) in 1984 and is situated in Lahore, capital of Punjab, Pakistan.
Sample Size Estimation and Sampling
An appropriate sample size was estimated using the Cochran formula.12,13
Study Population and Study Duration
All registered patients with BC between January 2017-November 2024 were invited to participate in the study. Patients receiving chemotherapy or follow-up consultations with confirmed BC histopathological reports were included in the study. Data were collected from patients between August to November 2024. Patients without histopathological confirmation of invasive BC were excluded, as histopathology is considered the gold standard for ensuring diagnostic accuracy and the validity of results. Patients with amnesia or psychiatric disorders, those exhibiting uncooperative behavior, and individuals unwilling to provide written informed consent were excluded. Moreover, lactating women were excluded to avoid potential confounding factors related to breast physiology during lactation. The selection criteria for participants are summarized in Figure 1. Flow diagram for patients with BC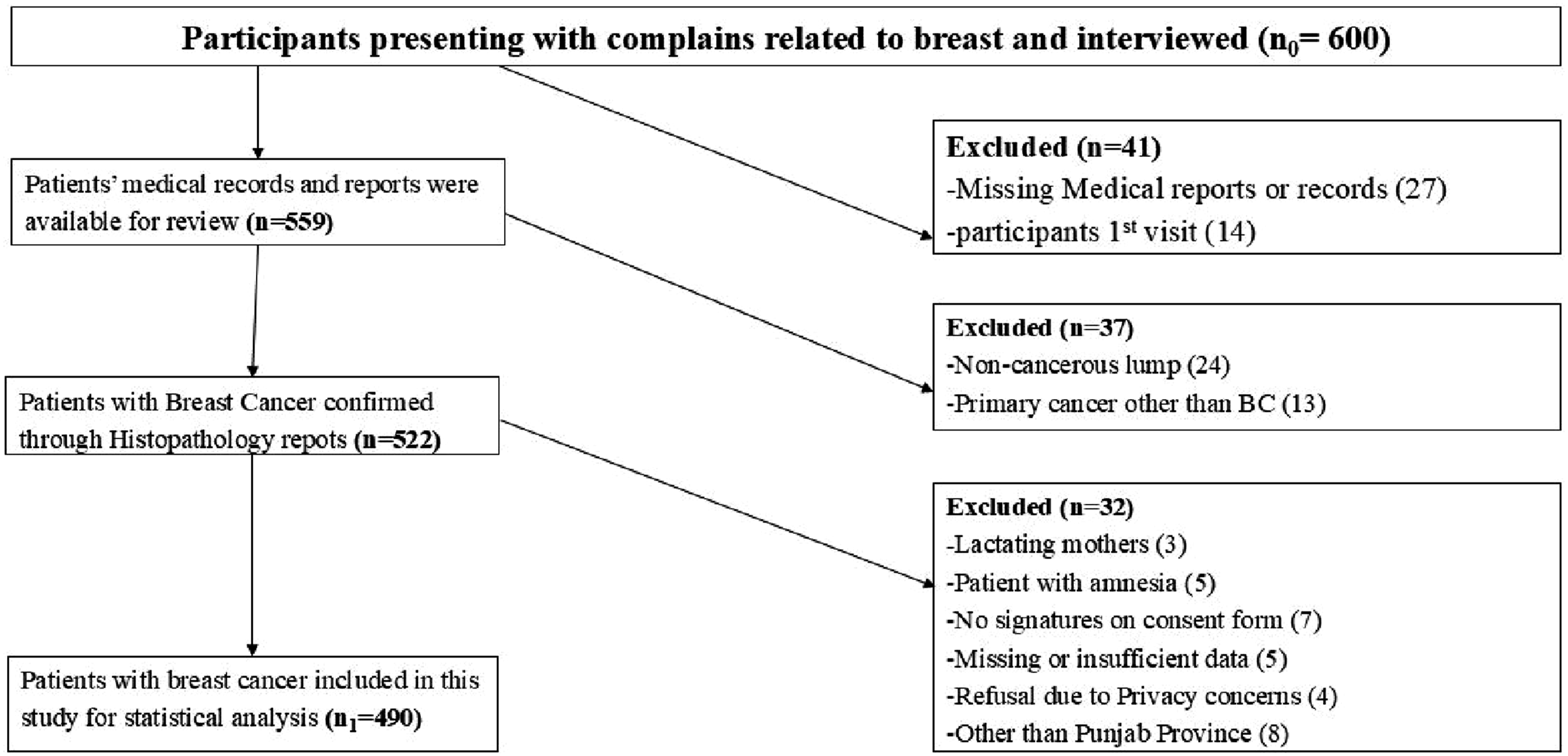
Ethics Statement
This study was conducted in accordance with the ethical standards of the institute and the national research committee, as well as the Declaration of Helsinki and its subsequent amendments. Approval was granted by the Research Ethics Committee (Reference No. UOH/DASR/2024/2246) of The University of Haripur, Khyber Pakhtunkhwa, Pakistan. Written informed consent was obtained from all individual participants included in the study before data collection, and participants were informed about the study objectives, procedures, confidentiality, and their right to withdraw at any stage.
Data Collection Tool and Procedure
Data were collected in local languages, including Punjabi and Urdu. Duration between date of enrollment in the hospital and histopathology report >3 months is considered a delayed diagnosis.
15
A self-structured questionnaire was used as a data collection tool that was developed with the help of a systematic review.
16
Facial and content validation of the data collection tool was completed by five experts, including an Epidemiologist, two Oncologists, and two Public Health experts. Demographic and socioeconomic information of the patients including age (years), gender (female or male), marital status (single or married), side involved (right, left, or both), socioeconomic status (upper class [>3,000,000 PKR], middle class [150,000-3,000,000 PKR], and lower class [<150,000 PKR] based on annual family income),
17
and menopausal status (not applicable, perimenopausal, or postmenopausal) were collected directly from patients. Tumor characteristics, including tumor size (≤2 cm, >2 cm, or undefined), lymph node involvement (yes, no, or undefined), metastasis (Mx, M0, or M1), grade (not determined, I, II, or III), and stage (I, II, III, IV, or unknown), were obtained from histopathology reports whereas, through the questionnaire, information was gathered related to factors that were associated with the delayed diagnosis as shown in Figure 2. A delayed diagnosis was defined as a duration of more than 3 months between the patient’s first visit to a healthcare provider and the histopathology confirmation of breast cancer.15,18,19 Patient-related modifiable factors contributing to delayed presentation and delayed diagnosis of breast cancer
For piloting, data was collected from thirty-six BC patients to test the statistical validity and reliability of the questionnaire; these data were not included in the final analysis. Cronbach’s alpha was used to assess internal consistency. Initially, 17 items related to delayed diagnosis were tested; two items were excluded to improve reliability. The final 15-item questionnaire demonstrated a Cronbach’s alpha of 0.767, while the Intraclass Correlation Coefficient (ICC) was 0.704.The Kuder–Richardson 20 (KR-20) formula was also applied to test the reliability of dichotomous questions, 20 yielding a value of 0.733.
Statistical Analysis
Data was analyzed through SPSS software version 27 (IBM Corporation, Armonk, NY, USA). For descriptive analysis, numerical and continuous data were presented in mean and standard deviation. Whereas, categorical data were displayed in frequencies and percentages. The Chi-square test was applied to compare frequencies and percentages of demographic and tumor-related characteristics of patients with BC between delayed (>3 months) and not delayed (≤3 months) or early diagnosis. The Fisher’s Exact test also applied for a 2 × 2 contingency table when the expected frequency was less than five. The Shapiro-Wilk test was applied to assess normality of the data. The Mann-Whitney U test was used to compare the median time of delayed and non-delayed diagnosed patients. An independent sample t-test was used to compare the mean age of both groups. For the identification of potential modifiable factors associated with delayed diagnosis of BC, logistic regression analysis was performed in two steps. First, univariate binary logistic regression was conducted, and factors with a P < 0.20 were included in the multivariate analysis. Subsequently, a multivariate forward stepwise binary logistic regression model using the Wald criterion was applied to identify independent predictors of delayed diagnosis after adjusting for potential confounders. This technique was allowed to include factors that were statistically significant and most relevant and optimizing the simplicity of the model, and adjusted odds ratios (AORs) were estimated to account for simultaneous effects of potential modifiable factors of delayed diagnosis. Values of pseudo-R2 (Nagelkerke R2 and Cox & Snell R2) and −2 Log Likelihood were calculated for the model to assess the goodness of fit. Performance and discriminative ability of the final multivariate model were evaluated using the Receiver Operating Characteristic (ROC) curve and the Area Under the Curve (AUC), which represent the model’s capacity to accurately distinguish between delayed and non-delayed diagnosis cases. The entire data was analyzed at a 95% confidence interval, and a P < 0.05 was considered as statistically significant value.
Results
Demographic Characteristics and Delayed Diagnosis of Breast Cancer
Demographic Characteristics of BC Patients With and Without Delayed Diagnosis

“*” statistical significance with P-value <0.05, Q = quartile.
aChi-square test.
bFisher’s Exact Test.
cMann-Whitney U test.
dIndependent sample t-test.
Tumor Characteristics and Factors Related to the Delayed Diagnosis of Breast Cancer
Tumor Characteristics of BC Patients With and Without Delayed Diagnosis

Chi-square test was applied.
Logistic Model and Potentially Modifiable Factors Associated with Delayed Diagnosis of BC
The model’s performance was assessed through the ROC curve (Figure 3). The overall discriminative ability of the multivariate logistic regression model was acceptable with AUC = 0.72 (95% CI: 0.67-0.77), calculated using the Hanley–McNeil method A receiver operating characteristic (ROC) Curve to evaluate the performance of the model Univariate Analysis of Modifiable Factors Associated With Delayed Diagnosis of Breast Cancer “*” statistical significance with P-value <0.05, COD- Cruds Odds Ratio, CI – Confidence Interval, BC- Breast Cancer. aFactors meeting the inclusion criterion (P-value <0.20) for multivariate analysis. Multivariate Analysis of Potential Modifiable Factors of Delayed Diagnosis Among Patients With BC Model Fit statistics: −2 Log likelihood = 564.921, Cox & Snell R Square = 0.088, Nagelkerke R Square = 0.124.


Table 3 presents the proposed modifiable factors contributing to delayed diagnosis of breast cancer. High cost of diagnostic tests, financial constraints, consultation with traditional healers before diagnosis, far from health facility, lack of BC symptom awareness, negligence, and rural residence were found to be statistically significant (P < 0.05). In contrast, dependent on family members for healthcare decision-making, lack of lump awareness, limited availability or accessibility of healthcare facilities, and misdiagnosis by professionals were not statistically significant but met the inclusion criteria for multivariate analysis. All variables with P < 0.20 were included in the multivariate analysis. Among these, only the potential modifiable factors significantly associated with delayed diagnosis are presented in Table 4.
Multivariate regression model revealed that the highly cost of diagnostic investigations was associated with delayed diagnosis (β = −0.467, P = 0.039; AOR = 0.627, 95% CI: 0.403-0.976). Similarly, seeking consultation from traditional healers before diagnosis was also negatively associated with delayed diagnosis (β = −1.150, P < 0.001; AOR = 0.317, 95% CI: 0.196-0.512). Negligence toward BC was also significantly associated with delayed diagnosis (
Discussion
The present study highlights multiple challenges that BC patients face related to the timely diagnosis of the disease. Several modifiable factors influence delayed diagnosis, contribute to disease progression and reduce BC survival. This study is unique as it focuses on potentially modifiable factors leading to delayed diagnosis of breast cancer rather than non-modifiable demographic or tumor-related variables. In the current study, 68.57% of patients with BC experienced delayed diagnosis. This proportion was higher than that reported in studies from Lahore (65%) 21 and Karachi (44.6%), 22 but lower than another Pakistani study, which documented 88.8% delayed diagnosis. 15 At the international level, lower rates of delayed diagnosis have been reported, including 36.7% in Sri Lanka, 23 34% in Iran24, and 50.5% in North East Ethiopia. 25 In the current study, the median time from recognition of the first symptom to histopathological confirmation was 6 months, which was longer than the 4 months reported in an Ethiopian study. 25 The observed delay in diagnosis may reflect, in part, the influence of local cultural and social norms, limited health awareness, and restricted access to female healthcare providers.
In the current study, a tumor size greater than 2 cm was observed in 97.6% of patients with delayed diagnosis (>3 months) compared to 91.6% among those diagnosed earlier (≤3 months), representing a notable difference. A Brazilian study similarly reported that 87.1% of patients with BC presented with tumors larger than 2 cm. 26 Lymph node involvement was also more frequent among patients with delayed diagnosis (75.9%) compared to those without delay (62.3%), with the difference being statistically significant. In comparison, an Iraqi study documented lymph node involvement in 53.8% of cases. 27 Furthermore, delayed diagnosis was more common in patients presenting with stage III (39.6%) and stage IV (18.5%) disease, compared to 26.6% and 9.1%, respectively, in the early diagnosis group. A study conducted in Karachi, Pakistan, also demonstrated a significant association between delayed diagnosis (>3 months) and late-stage tumors. 28 Similarly, prior evidence suggests that more than 50% of BC cases in LMICs are diagnosed at stage III or IV. 4 These findings point toward weaknesses in early detection and referral systems, emphasizing the need for improved screening infrastructure and timely diagnostic pathways within the health system.
Lack of awareness of BC symptoms was reported in 80% of patients with delayed diagnosis, which was lower than the 95% reported in a study conducted among Egyptian women. 29 In the present study, the significance of a breast lump was recognized in 78% of patients diagnosed with a delay. Financial constraints contributed to delayed diagnosis in 72% of cases, compared to 52% in an Iraqi study 30 and 23.5% in another Pakistani study. 22 Although financial problems were included in the regression model, they did not reach statistical significance. Furthermore, more than half (54%) of patients with delayed diagnosis in the current study were from rural areas, which was comparable to the 59.2% reported in a previous study. 25 This proportion was higher than the 27.7% reported in another Pakistani study, where rural residence showed a statistically significant association with delayed diagnosis. 21
Additional factors contributing to the delayed diagnosis of BC included fear of being diagnosed with cancer, transportation difficulties, misdiagnosis by healthcare professionals, and inadequate diagnostic facilities. Fear of receiving a BC diagnosis was expressed by 10.7% of participants, while delays due to long travel distances were noted in 23.5% of cases, consistent with previous findings from Pakistan. 22 International evidence also indicates that residing more than five kilometers from a healthcare facility is directly associated with advanced-stage BC. 31 In this study, consultation with traditional healers before diagnosis was more frequent than reported in an Egyptian study, 29 yet lower compared to findings from Ethiopia. 31 Furthermore, misdiagnosis by healthcare professionals at the first visit was reported in 79.4% of patients with delayed diagnosis, highlighting a critical healthcare system factor. 31 Delays in diagnosis among women from rural and low-income areas are likely caused by financial problems, transportation difficulties, and a lack of awareness.
The regression model highlighted important predictors significantly associated with the delayed diagnosis of BC. The cost burden of diagnostic investigations was found to be significantly associated with delay. Patients who were perceived diagnostic tests as expensive had 37.3% lower chances of being diagnosed early (≤3 months). A similar finding was reported in an Egyptian study, where financial constraints were observed as a barrier to the timely diagnosis of BC patients. 32 In the present study, however, 62.7% of patients perceived financial barriers related to diagnostic investigations as a major factor. This considerable difference may be attributed to greater financial instability and limited availability of healthcare resources within the local health system.
Seeking consultation from traditional healers such as hakeems, quacks, or spiritual healers before histopathological confirmation were also strongly associated with delayed diagnosis. Patients who consulted traditional healers had 68.3% lower chances of early diagnosis. This is in line with a study on Ethiopian females, which reported that women who avoided visiting traditional healers had a 62% lower likelihood of experiencing diagnostic delay. 26 Another study further showed that the use of alternative medicine increased the risk of delay by more than eleven times. 33 The lack of accessible and available medical services often forces people to seek help from traditional healers, which can result in delays in diagnosis and treatment.
Patients showing negligence or lack of concern regarding BC symptoms had more than twice the risk of delayed diagnosis compared to those who took their symptoms seriously. A study conducted in Iran similarly reported a statistically significant association between negligence and delayed diagnosis. 34 Financial problems were also included in the model as an important contextual factor. This trend has also been observed in previous literature, where financial difficulties contributed to diagnostic delay, even if not always statistically significant. 22 Limited education and awareness about BC symptoms may lead women to ignore warning signs and delay seeking medical help, resulting in late diagnosis and treatment.
There were certain limitations of the study. First, the data were collected entirely based on patients’ perceptions, which may have introduced subjective bias in reporting factors associated with delayed diagnosis. Second, as this was a single-center study, the findings may not be fully generalizable to other regions or healthcare settings. Third, potential confounders were not fully controlled, which could have influenced the observed associations. In addition, retrospective information was obtained from patients regarding the duration between the first appearance of symptoms and the histopathology confirmation, which may have led to recall bias.
Despite these limitations, studying also has important strengths. The relatively large sample size increases the reliability of results. Moreover, the data collection was conducted by a well-trained team with medical and allied health backgrounds, including medical imaging professionals, which minimized interviewer bias. To enhance participant comfort and data accuracy, female data collectors obtained demographic information and patients’ perceptions about modifiable factors contributing to diagnostic delay.
Conclusion
About two-thirds of BC patients experienced a delayed diagnosis. The median time from recognition of the first symptom to diagnosis, confirmed by histopathology assessment, was 6 months. Tumor characteristics, including larger tumor size, lymph node involvement, and advanced-stage cancer (Stage III and IV), were significantly more prevalent among patients with delayed diagnosis. Costly diagnostic tests, consultancy with traditional healers before diagnosis, and negligence towards patients were significant modifiable determinants of delayed diagnosis.
These findings emphasize the urgent need to reduce delays in BC diagnosis. Public awareness campaigns should focus on educating women about the early symptoms of BC and the importance of seeking timely medical consultation. The government should ensure the availability of accessible and affordable screening and diagnostic services, particularly in rural areas. Additionally, training healthcare professionals to recognize the early signs of BC can facilitate timely diagnosis and improve treatment outcomes.
Footnotes
Acknowledgment
We sincerely thank all study participants, patients, supporting staff, oncologists, doctors, nurses, and the authorities of INMOL Cancer Hospital, as well as everyone who assisted at any stage of this study. We are thankful to the Deanshipship of Scientific Research, King Faisal University for the support.
Ethical Considerations
Approval was granted by the Research Ethics Committee (Reference No. UOH/DASR/2024/2246) of The University of Haripur, Khyber Pakhtunkhwa, Pakistan. This study was conducted in accordance with the ethical standards of the institute and the national research committee, as well as the Declaration of Helsinki and its subsequent amendments.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
Asim Raza designed the study, collected data, analyzed data and wrote first draft of manuscript, Shahbaz Ahmad Zakki designed the study, reviewed manuscript and approved final version. Ijaz ul Haq interpreted data and critically reviewed manuscript. Nasrull Islam collected and analyzed data.
Funding
This study was supported by Deanshipship of Scientific Research, King Faisal University (KFU254816)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets will be available from the corresponding author on request.