
Abstract
Background
Early diagnosis of breast cancer is a key factor affecting patient survival, so screening can reduce the burden of this disease. The present study aimed to investigate the effect of education based on the theory of planned behavior (TPB) on breast cancer screening in rural women.
Methods
In this quasi-experimental study, 480 women referring to the health care centers in the cities of Fasa and Shiraz were divided into two groups, intervention (n = 240) and control (n = 240), using cluster random sampling method, in 2021-2022. We randomly selected two health care centers in Shiraz and Fasa and invited them to participate in the study. The demographic information questionnaire and a researcher-made questionnaire based on the TPB were used to collect the data. The intervention included 50-minute sessions on topics such as breast cancer basics, screening methods, barriers to mammography, and the role of peer groups. Data were collected before and 4 months after the intervention.
Results
The results showed no difference between the two groups in awareness, attitude, perceived behavioral control, subjective norms, behavioral intention, and breast cancer screening performance before the intervention. Four months after the intervention, a significant increase was found in the intervention group in awareness (7.46 ± 1.50 to 18.54 ± 1.20), attitude (28.55 ± 4.62 to 58.69 ± 4.35), perceived behavioral control (22.52 ± 3.32 to 40.88 ± 3.84), and subjective norms (20.37 ± 3.34 to 21.99 ± 3.38). Instead, no significant difference in the mentioned constructs (P < 0.05) was observed in the control group.
Conclusion
This study demonstrated that TPB-based education enhanced awareness, attitude, perceived behavioral control, subjective norms, and behavioral intention towards breast cancer screening. The TPB empowers women in rural communities to prioritize their health and seek timely breast cancer screening. Continued efforts and improved access to screening services are crucial for improved outcomes.
Introduction
Breast cancer is a malignant breast tumor with the highest incidence and mortality rate in women around the world. It has a high prevalence of drug resistance, recurrence, and metastasis. 1 Cancer is a leading cause of death in the world. Malignant diseases recorded 10 million deaths in 2023, with a significant estimated increase by 2030. 2 Breast cancer is the most prevalent and leading cause of death among women.3,4 According to the WHO, cancer was the first cause of death in countries such as the US, France, and Germany, and the second cause of death in countries such as Russia, Iran, and Brazil before the age of 70 in 2019. 5 According to the report of the National Cancer Registration Organization in Iran, breast cancer is one of the most common and deadliest types of cancer in women, with the highest prevalence among women aged 40-50 years. 6 The south of Fars, Iran, recorded 780 cases of cancer between 2011 and 2016, with breast cancer accounting for 22.3% of all cancers in this city. 7
Despite decades of laboratory, epidemiological, and clinical research, breast cancer incidence is still increasing. Breast cancer is the main disease burden for women. One woman out of every 20 in the world, and one woman out of 8 in high-income countries, suffers from breast cancer. 8 According to the published studies, the incidence rate of breast cancer varies among different races and ethnicities and is higher in developed countries. 9 The results of the previous studies showed that the breast cancer mortality rate is higher in less-developed areas. The study also revealed that various demographic, reproductive, harmonic, and genetic risk factors, along with issues related to the breasts and lifestyle, contribute to the incidence of breast cancer. 3 Early diagnosis, treatment monitoring, and prognosis assessment of breast cancer are the key factors affecting patients’ survival. However, breast cancer is still a major factor affecting women’s quality of life and physical and mental health due to a lack of specific biomarkers. 1
Screening can help to reduce the burden of breast cancer. Classification of women based on risk factors can be effective in improving breast screening programs without the risk of side effects, overdiagnosis, and increased costs. 10 The results of controlled random trials in many countries indicate that breast cancer screening programs are effective in reducing breast cancer deaths. 11 It is necessary to design effective educational interventions that are consistent with society’s culture to increase women’s awareness and understanding of breast cancer screening and promote screening behaviors in women. 12 As a result, health care staff providing information about breast cancer to women can be an effective strategy to prevent it. 13 Moreover, educational interventions can promote breast cancer screening in women. 14 The rate of breast self-examination in women with high awareness and self-efficiency is three times higher than that in women with low awareness and self-efficiency. 15 The theories and models of behavior change play a crucial role in identifying the primary effective factors in behaviors, thanks to their ability to pinpoint these factors. The Theory of Planned Behavior (TPB) helps identify the factors affecting behavior. The constructs of behavioral intention, attitude toward behavior, subjective norms, and perceived behavioral control comprise TPB. 16 The constructs of TPB predict women’s behavioral intentions for breast cancer screening. 17 Many studies used this theory for promoting breast cancer screening test in different regions of the world.18-21
Despite advancements in health care infrastructure, late diagnosis of breast cancer remains a significant concern, contributing to increased morbidity and mortality rates among women. The magnitude of late diagnosis in Iran is staggering, with a substantial portion of breast cancer cases being detected at advanced stages, significantly limiting treatment options and reducing survival rates among affected women. Breast cancer is a significant health concern in Fars province, Iran, where it accounts for a substantial proportion of cancer cases among women. Between 2011 and 2016, the southern region of Fars recorded 780 cases, with breast cancer constituting 22.3% of all cancers. The incidence of breast cancer has been rising, particularly among women aged 40-50 years. The demographics in this region show that the highest prevalence is among women aged 40-50 years, emphasizing the urgent need for targeted interventions. 22
The TPB has undergone thorough validation in the field of health-related behaviors, making it a strong and reliable option for developing treatments targeted at modifying behavior. 23 Multiple studies have shown that it is helpful in predicting and changing health behaviors, such as cancer screening practices. 24 Furthermore, TPB’s constructions specifically target the various factors that influence an individual’s choice to participate in health-related actions. TPB is highly effective in identifying and targeting the unique barriers and facilitators associated with issues like breast cancer screening. 24 Furthermore, this theory may be adjusted to suit various cultural circumstances, which is crucial in a diverse and complex country such as rural Iran. Lastly, the organized structure of TPB enables the development of instructional interventions that methodically target each of its components.
Previous investigations which utilized this theory in breast cancer screening mostly focused on evaluating the screening behaviors, rather than using this theory in designing an educational program. 16 Sun et al 24 conducted a study in rural China to predict women’s breast cancer screening intentions using a PLS-SEM approach based on TPB. The study highlighted that attitude, subjective norms, and perceived behavioral control significantly influenced women’s intentions to undergo screening. Wang et al investigated the application of TPB and the Health Belief Model (HBM) in predicting women’s intentions to participate in breast cancer screening. The study found that both models were effective in explaining the variance in screening behaviors, with TPB showing a significant predictive power. 25
All in all, considering the high incidence of breast cancer in Iran and globally, as well as the role of TPB-based training on breast cancer screening and inadequate facilities for rural women to access breast cancer screening services, the present study aimed to investigate the effect of TPB-based educational intervention on breast cancer screening in rural women. By fostering a proactive approach to breast cancer prevention and early detection, our study endeavors to empower Iranian women to take control of their health, reduce the incidence of late-stage diagnoses, and improve the prognosis and quality of life for those affected by this pervasive disease. Through collaborative efforts between health care providers, policymakers, and communities, we envision a future where breast cancer no longer exacts a disproportionate toll on the women of Iran.
Methods
Research Design
This quasi-experimental study was conducted on 480 women referring to rural health care centers in the cities of Fasa and Shiraz (240 rural women from the village of Shiraz city and 240 rural women from the villages of Fasa city) in 2021-2022. Using cluster random sampling method, we randomly selected two health care centers, one from Shiraz and the other from Fasa. We selected the individuals based on their family files and invited them to participate in the study. The announcement of the program was provided in the in health information groups and at the health centers of Fasa and Shiraz Universities of Medical Sciences.
Inclusion Criteria
Women aged 35 and older who had no history of mammography, no breast cancer, no breast biopsy procedures, and a willingness to participate in the study.
Exclusion Criteria
Women who were absent from the classes for more than two sessions, not filling any of the questionnaires, and changing the place of residence during the study.
Sample Size and Sampling Process
Considering the results of Ghaffari et al.,
26
the significance level of 95%, and the test power of 80%, we determined the sample size to be 480 people (240 in the intervention group and 240 in the control group). Figure 1 presents the study flow chart (Figure 1). Presents the study flow diagram.

n: Sample size
Z1: Z-Score of the normal distribution
α: Type I error rate
β: type II error rate
r: The expected correlation coefficient
Data Collection Tools
The collection data tools in this study was a researcher-made questionnaire which was used in the study of Khani Jeihooni et al., 27 The content validity of the tool was verified through expert review, ensuring the items accurately reflected the constructs of the TPB. Reliability was established using Cronbach’s alpha, with the overall reliability of the questionnaire scoring 0.88. Specific constructs also demonstrated high reliability: awareness (0.89), attitudes (0.80), subjective norms (0.82), perceived behavioral control (0.80), and behavioral intention (0.82). These high reliability scores shows consistent and dependable measurement of the variables. 27
We used the questionnaire for rural women due to the importance of the subject matter. The first part of the demographic information consisted of age, ethnicity, number of children, age at first pregnancy, history of breastfeeding, employment status, education, marital status, insurance status, menopause status, income, and family history of breast cancer. The second part featured items from TPB. In this part, the questionnaire included items related to awareness in three areas of symptoms and signs, breast cancer risk factors, and mammography screening, which included twenty-five 3-option items (correct, incorrect, or no idea). We awarded one score for each “correct” answer and zero for “incorrect” and “no idea” answers. The scores of awareness ranged between zero and 25.
We measured the variables of awareness, attitude, subjective norms, and perceived behavioral control using a 5-point Likert scale, ranging from 1 = strongly disagree to 5 = strongly agree. We used 15 items (with a minimum score of 15 and a maximum score of 75) to assess the variable of attitude, such as “the person can live his or her normal life if breast cancer is timely diagnosed and treated.” We used 10 items, each with a minimum score of 10 and a maximum score of 50, for measurement. Subjective norms, for example, health care staff consider mammography necessary for women. We used 10 items, each with a minimum score of 10 and a maximum score of 50, to measure perceived behavioral control, such as “I don’t have enough time for mammography.” The behavioral intention variable included one yes-or-no question about performing mammography. One yes-or-no question about performing mammography also measured behavior. Both the intervention and control groups completed the questionnaire before and 4 months after the intervention.
Procedure
Considering the results of the cross-sectional study, 16 the intervention, which was based on the TPB, involved a comprehensive educational program conducted over nine 50-min sessions. The intervention was led by a Ph.D. expert in health education and promotion, with collaboration from a gynecologist, an oncologist, and six midwives. These professionals brought expertise in health education, medical knowledge, and patient care, ensuring a multidisciplinary approach to the intervention.
The intervention took place in rural health care centers, chosen randomly from the cities of Fasa and Shiraz. Sessions were conducted once a week, with each session lasting 50 min. This frequency allowed for sustained engagement and reinforcement of key messages over time.
The sessions utilized various interactive and participatory methods to engage participants, including lectures, group discussions, question and answer sessions, educational films, and visual aids such as pictures and presentations. These methods catered to different learning styles and ensured active participation.
The content of the intervention covered several key areas related to breast cancer screening and mammography. Topics included:
Basics of breast cancer: Providing foundational knowledge about breast cancer, its prevalence, risk factors, and importance of early detection.
Necessity of screening behaviors: Emphasizing the significance of regular screening, particularly mammography, in detecting breast cancer at early stages when treatment is most effective.
Methods for screening: Educating participants about the process of mammography screening, including its procedure, benefits, and limitations.
Barriers to mammography: Identifying common barriers that rural women may face in accessing mammography services, such as time constraints, financial issues, and lack of awareness, and strategies to overcome these barriers.
Role of peer groups and subjective norms: Highlighting the influence of social networks, health care providers, and family members in promoting positive screening behaviors and creating a supportive environment for mammography uptake.
Role of Health care Staff and Peer Groups: Health care staff, including physicians and midwives, actively participated in the sessions to reinforce positive subjective norms and provide expert guidance. Additionally, peer groups were emphasized to foster a sense of community support and encourage shared experiences among participants.
Follow-up Sessions: Two follow-up sessions were held at one and two months after the intervention to review the content, address any questions or concerns, and provide additional support and reinforcement.
In these sessions, awareness and attitude towards behavior were instructed using lectures, educational films, and visual aids. Subjective norms were discussed using group discussions, role-playing, and peer group involvement. For perceived behavioral control, question and answer sessions, educational films, and strategies to overcome barriers were utilized, and the behavioral intention were a result of previous instructions especially group discussions, peer group involvement, and follow-up sessions.
Participants received educational pamphlets at the end of the sessions, which served as supplementary materials to reinforce key messages and provide reference information. The book contained information regarding introduction to breast cancer screening, understanding mammography, preparing for mammography, overcoming barriers to screening, empowering Participants, resources and support, and frequently asked questions (FAQs). Lastly, arrangements were made with health care centers to facilitate mammography services for participants, including providing visiting cards for mammography appointments and recording screening outcomes. This program was designed to address the cognitive, emotional, and practical factors influencing breast cancer screening behavior among rural women, with the goal of promoting early detection and improving health outcomes.
In the intervention, the involvement of a diverse team of experts ensured high-quality, accurate, and comprehensive content delivery. The presence of health care professionals reinforced the credibility of the information and provided participants with access to expert advice. The use of various interactive methods (group discussions, role-playing, visual aids) ensured that participants were actively engaged and could relate the information to their own experiences.
Moreover, the content was tailored to the needs and challenges of rural women, addressing specific barriers they might face in accessing mammography services. The follow-up sessions provided ongoing support and reinforcement, and by facilitating access to mammography services, the intervention not only provided knowledge but also practical means to apply this knowledge, by bridging the gap between education and action.
Ethical Considerations
The Ethics Committee of Fasa University of Medical Sciences (ethics code: IR. FUMS.REC.1399.134) approved this study. The reporting of this study conforms to STROBE guidelines. 28 The participants signed an informed consent form. We explained the purpose, importance, and necessity of the study to the participants and assured them of the confidentiality of the information. For illiterate participants, a trained researcher or staff member verbally explained the study details, risks, benefits, and procedures to them. After ensuring that the participant understood the objectives of the study, they verbally expressed their consent to the researcher, who also signed the consent form to confirm that the process was conducted appropriately.
All of the participants in both groups participated in the study from beginning to end, and no one left. Measures were also taken to ensure that information about the intervention did not leak to the control group through health care staff or other means, in order to control contamination.
Statistical Analyses
The data were analyzed using SPSS 22, and mean and standard deviation were used as quantative variables. Statistical tests such as independent t test (to compare the results between the experimental and control groups), chi-squared test (for comparing demographic information between the two groups), paired t test (for assessing each variable in each group of the study either before or after the intervention), and McNamara’s test (to analyze mammography screening behavior before and after the study). The significance level was considered to be 0.05.
Results
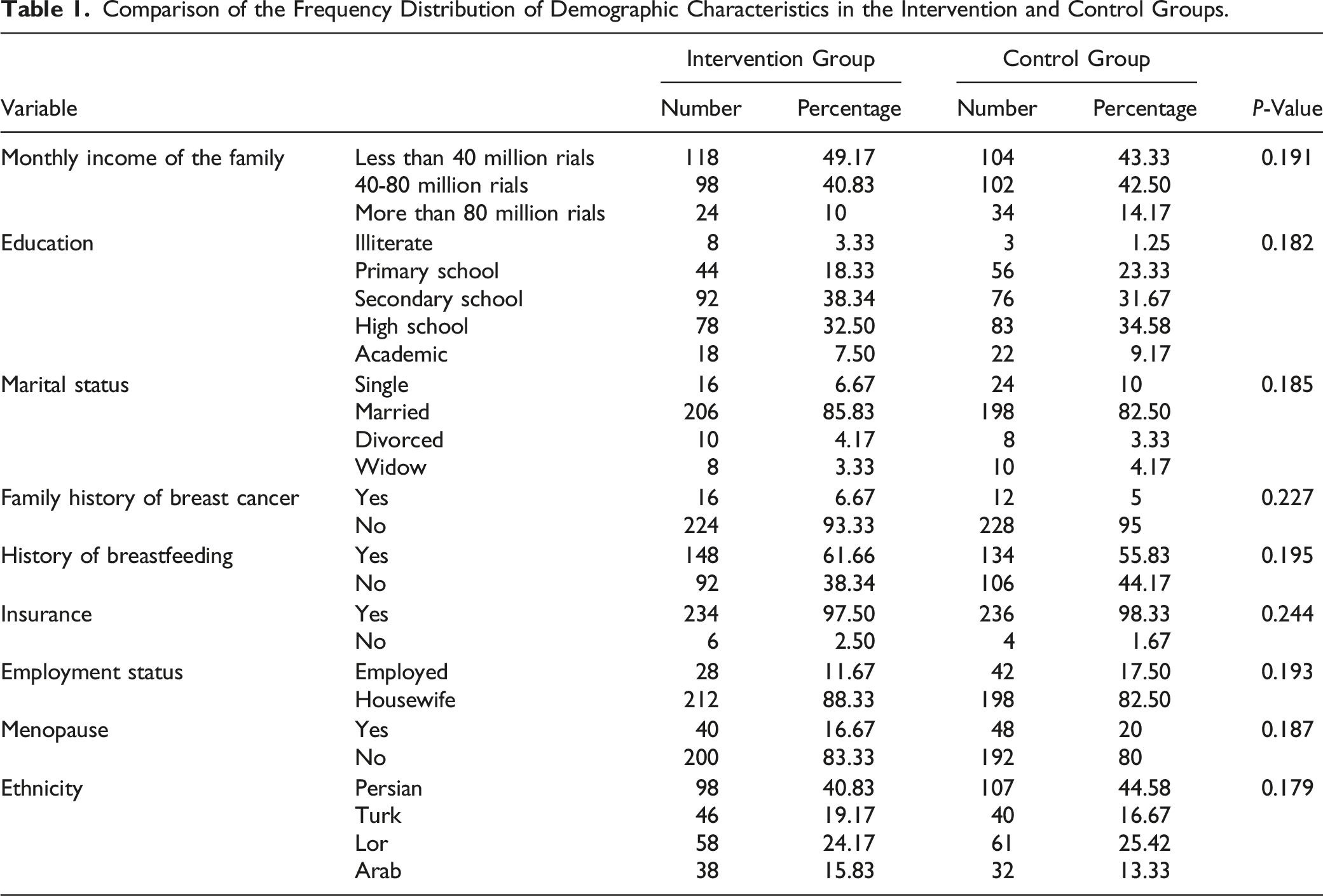
The study involved 480 rural women (240 in the intervention group and 240 in the control group) who referred to the rural health care centers of Shiraz and Fasa. The mean age of the participants in the intervention group and control group was 43.12 ± 5.26 and 42.82 ± 6.60, respectively (P = 0.185). The mean age of the first pregnancy was 20.87 ± 4.22 in the intervention group and 21.19 ± 4.20 in the control group (P = 0.192). The average number of children in the intervention group was 3.35 ± 1.21 children and 3.41 ± 1.15 children in the control group (P = 0.170). The independent t test showed no significant difference between the two groups.
Comparison of the Frequency Distribution of Demographic Characteristics in the Intervention and Control Groups.
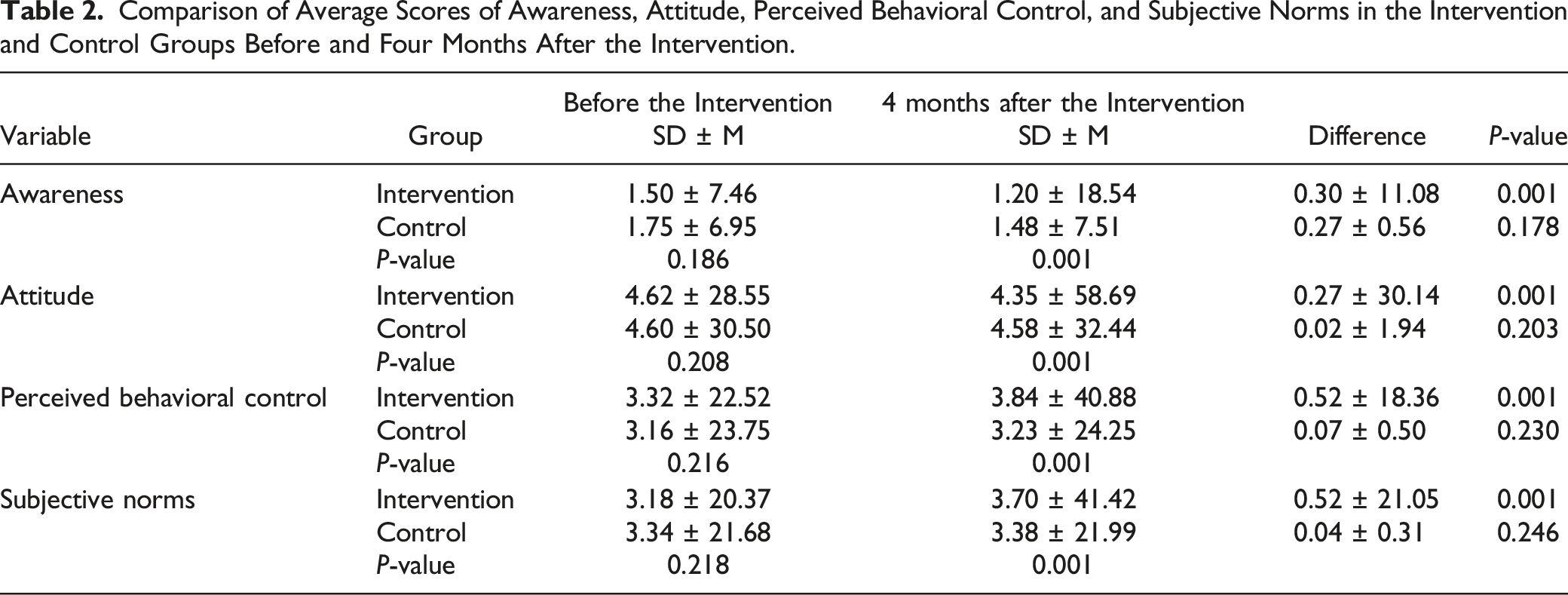
Prior to the intervention, there was no substantial disparity in awareness levels between the intervention group (7.46 ± 1.50) and the control group (6.95 ± 1.75; P = 0.186). After a period of 4 months following the intervention, the group that received the intervention had a noteworthy rise in awareness (18.54 ± 1.20; P = 0.001), while the control group did not exhibit a significant alteration (7.51 ± 1.48; P = 0.178).
At the beginning, there was no notable disparity in attitude scores between the intervention group (28.55 ± 4.62) and the control group (30.50 ± 4.60; P = 0.208). After 4 months of the intervention, the attitude scores in the intervention group showed a substantial increase (58.69 ± 4.35; P = 0.001), while there was no significant change in the control group (32.44 ± 4.58; P = 0.203). There was no statistically significant difference in perceived behavioral control between the intervention group (22.52 ± 3.32) and the control group (23.75 ± 3.16; P = 0.216) prior to the intervention. After a duration of 4 months, the intervention group demonstrated a noteworthy enhancement (40.88 ± 3.84; P = 0.001), while the control group did not exhibit a meaningful alteration (24.25 ± 3.23; P = 0.230).
Comparison of Average Scores of Awareness, Attitude, Perceived Behavioral Control, and Subjective Norms in the Intervention and Control Groups Before and Four Months After the Intervention.
After a four-month intervention, 182 women (75.83%) in the intervention group expressed their intention to get mammography, while 137 women (57.8%) actually underwent mammography. Conversely, the control group had a far lower percentage of women who wanted to have mammography, with just 44 individuals (18.33%) expressing such intention. Furthermore, a mere 18 women (7.5%) actually followed through with the procedure. The disparities between the intervention and control groups were statistically significant (P < 0.05).
Discussion
The present study aimed to investigate the effect of TPB-based educational interventions on breast cancer screening in rural women. The results showed a significant increase in awareness, attitude, subjective norms, and perceived behavioral control in the intervention group, leading to a higher intention to undergo breast cancer screening compared to the control group. This finding highlights the effectiveness of education based on the TPB in improving breast cancer screening behaviors.
The study’s results indicated the intervention’s effectiveness in increasing the construct of awareness in the intervention group. This underscores the importance of educational initiatives in enhancing awareness about breast cancer and screening methods. This finding is consistent with previous research by Khani Jeihooni et al, Taymoori et al, Khazir et al, and Asare et al.,27,29-31 which demonstrated the efficacy of TPB-based educational interventions in increasing awareness in various populations. In the study by Khani Jeihooni et al, TPB-based interventions were shown to significantly boost awareness of breast self-examination among Iranian women. 21 The educational sessions in our study covered content about breast cancer, the necessity of screening behaviors, methods for screening, potential barriers to mammography, and strategies to overcome these barriers, all of which seemed effective in enhancing awareness in the intervention group.
The study’s findings revealed an increase in the construct of attitude in the intervention group as well. These resultd matched what Sheykhan et al found when they looked at how the TPB-based intervention attitudes in relation to breast cancer screening. They found that the intervention worked to improve attitude. 32 Min et al used TPB to understand the intention and behavior of physical activity in Korean women with breast cancer and indicated the intervention’s effect on increasing attitude construct. 33 In the present study, the discussions were led by the leader to indirectly create positive motivation in women to perform diagnostic measures, especially mammography, and provide the grounds to create new attitudes or correct negative attitudes towards the belief that the diseases were uncontrollable. We discussed the incorrect and common beliefs about mammography with the aim of reducing or correcting them. This seemed effective in increasing the construct of attitude in the intervention group.
The present study’s results indicated an increase in the construct of subjective norms in the intervention group. Consistently, Sabouri et al 34 investigated the TPB-based intervention in empowering women of reproductive age to perform self-care behaviors and showed that education increases the construct of subjective norms. Rezaei et al also conducted a study to investigate the effect of TPB-based intervention on prostate cancer screening behaviors and indicated that the intervention promotes subjective norms. 35 In this study, by highlighting the importance of peer and social support, our intervention encouraged participants to prioritize breast cancer screening. In other words, the present study’s educational sessions emphasized the role of peer and friend groups in breast screening behavior, has lead to an increased construct of subjective norms in the intervention group.
The study’s findings indicated an increase in the construct of perceived behavioral control in the intervention group. These findings align with the findings of Heidari Sarvestani et al and Dsouza et al.,36-38 demonstrating the impact of TPB-based educational interventions on this construct within the intervention group. In the current study, the participants attended the intervention through face-to-face education, group discussions, educational pamphlets, visual learning, role-playing, and practice. Watched a mammography video. Additionally, the intervention group received strategies that emphasized the patients’ control and self-confidence in performing mammography, thereby increasing their perceived behavioral control. Through education, group discussions, and practical strategies, we empowered participants to feel more capable of engaging in mammography.
According to the results, there was a significant difference between the two groups in the mean scores of behavioral intention and screening practice. Our results were in line with the results of Dhakal et al, Saei Ghare Naz et al, and Adler et al.,19,20,39 Various studies have indicated the effect of the TPB-based intervention on the performance of breast screening.19-21 The present intervention increased the constructs of awareness, attitude, subjective norms, and perceived behavioral control in the intervention group, leading to increased behavioral intention and breast screening performance.
While our findings are consistent with a body of literature supporting the effectiveness of TPB-based interventions, there are studies that present contradictory results. 19 These discrepancies may be attributed to variations in intervention content, delivery methods, or participant characteristics.
Strengths and Limitations
By employing a strong quasi-experimental approach, our study successfully collected substantial data about the effects of TPB-based educational interventions on different psychological factors and actual screening behaviors. Moreover, the intervention’s all-encompassing strategy, including lectures, group discussions, educational films, and visual aids, offered a diverse and captivating learning experience for the participants, potentially leading to the favorable results reported in the intervention group.
An inherent shortcoming of the study is its dependence on self-reported data, which has the potential to induce response biases and compromise the precision of the findings. The study did not account for all potential demographic characteristics, such as socioeconomic status or previous health practices, that could impact the results. This may restrict the applicability of the findings. In addition, the sample was obtained from a particular geographic region (Fasa and Shiraz), which may restrict the generalizability of the findings to other rural populations with distinct cultural or socioeconomic characteristics. Finally, although the study documented notable enhancements in many factors and screening practices, it did not provide extended follow-up data to ascertain the durability of these changes.
Conclusion
The present study showed the effectiveness of TPB-based education on the constructs of awareness, attitude, perceived behavioral control, subjective norms, behavioral intention, and breast cancer screening performance. The educational sessions succeeded in enhancing participants’ understanding of breast cancer, the importance of screening behaviors, and methods such as mammography. The intervention addressed barriers to screening, promoted positive attitudes towards early detection, emphasized the role of social support networks, and bolstered participants’ confidence in their ability to undergo screening.
The study’s results underscore the importance of tailored, theory-based educational interventions in promoting breast cancer screening in underserved populations. By leveraging the TPB framework and culturally relevant educational strategies, health care providers can empower women with the knowledge and confidence to prioritize their breast health and seek timely screenings. The findings of this study have important consequences for public health policies that target the enhancement of breast cancer screening rates among women living in rural areas. The study establishes a strong framework for planning future health promotion programs by showcasing the efficacy of educational interventions based on the TPB.
These findings suggest that these interventions could play a crucial role in identifying breast cancer at an early stage, thereby potentially decreasing the illness and death rates linked to the disease in populations that lack access to adequate health care. Furthermore, the research emphasizes the significance of health education that is tailored to the culture and easily accessible, especially in rural regions where there may be a scarcity of health care resources and information. Policymakers and health care providers can utilize these observations to create and execute comparable educational initiatives, tailored to address the distinct requirements and obstacles faced by various rural regions. In conclusion, the study provides evidence to support the wider use of interventions based on the TPB as a realistic and successful method to improve public health outcomes in settings with limited resources.
Supplemental Material
Supplemental Material - The Effect of an Educational Intervention on Breast Cancer Screening of Rural Women: Application of the Theory of Planned Behavior
Supplemental Material for The Effect of an Educational Intervention on Breast Cancer Screening of Rural Women: Application of the Theory of Planned Behavior by Amirhossein Kamyab, Fatemeh Mohammadkhah, Saeedeh Asadi, Farzaneh Ghalegolab and Ali Khani Jeihooni in Cancer Control
Footnotes
Acknowledgments
This study is part of an MD thesis approved by the Fasa University of Medical Sciences. Our warm thanks go to the Research and Technology Dept. Of Fasa University of Medical Sciences, as well as women in villages of Fasa and Shiraz cities for their participation in the study.
Author’s Contributions
AK, FM, SA, FGh and AKhJ assisted in conceptualization and design of the study, oversaw data collection, conducted data analysis and drafted the manuscript. FM and AKhJ conceptualized and designed the study, assisted in data analysis and reviewed the manuscript. AK, FM, SA, FGh and AKhJ assisted in study conceptualization and reviewed the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets used and/or analyzed during the current study can be made available by the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.