
Abstract
Introduction
Multiple myeloma (MM) is associated with significant financial toxicity due to the high costs of treatment, including travel burdens. Satellite clinics aim to reduce travel burdens by bringing specialized care closer to patients’ homes. This study investigates the effectiveness of transferring established MM patients to a new satellite clinic closer to their homes.
Methods
Patients receiving care for plasma cell dyscrasias, including MM, at the primary campus were prospectively screened for eligibility to transfer to a satellite clinic within their catchment area from August to December 2023. Eligible patients were offered the option to transition their care. The proportion of actual transfers was tracked, and reasons patients were ineligible or declined to transfer were recorded.
Results
Out of 62 identified patients, 28 (45%) were deemed not transfer candidates by their provider. Among the 34 eligible patients, 10 (29%) opted to transfer. The overall transfer rate was 16% (95% CI: 8-28%). Reasons for declining transfer included comfort with current providers, preference for the primary campus, and concerns about the satellite clinic’s quality of care.
Conclusions
Most patients were either not eligible or unwilling to transfer to the satellite clinic once care had been established at the primary campus. Due to the limited uptake of this intervention, directing appropriate patients to satellite clinics at initial referral may be a more effective way to increase utilization of these sites. Enhancing satellite clinic capacity and addressing perceived quality disparities are also essential to boost their utility.
Introduction
Multiple myeloma (MM), a cancer of plasma cells, is the second most common hematologic cancer, responsible for 2% of all cancer diagnoses and deaths. 1 Advances in MM treatment have led to a dramatic increase in life expectancy, 2 but many of these new treatments are expensive. In fact, MM is among the most expensive cancers to treat, 3 with costs typically exceeding $100,000 to $200,000 USD per year.4,5
Given the high costs of treatment, a considerable proportion of patients with MM experience financial toxicity, which is psychological distress and maladaptive coping mechanisms, such as treatment non-adherence, resulting from financial burden.6-8 Financial toxicity is relatively understudied in people with MM. To our knowledge, only a few reports exist in the literature,9-16 many conducted by our group. Estimates have varied but, in general, studies have reported that about half of patients with MM experience some degree of financial toxicity.
One underappreciated contributor to financial toxicity is the travel burden associated with receiving one’s care. Travel burden includes direct costs such as fuel, tolls, parking, and public transportation, but also indirect costs such as meals and lost wages. Unlike medication and treatment costs, which are often largely subsidized by insurance or other parties, travel burden-related costs are largely out-of-pocket. Higher travel burden has been associated with lower likelihood of receiving guideline-concordant care and poorer health-related quality of life and cancer treatment outcomes.17,18 MM is associated with a high travel burden because many treatments are administered only in specialized clinics, and treatment is largely continuous throughout the disease course.
In an effort to reduce the travel burden on patients, many cancer centers operate satellite clinics—smaller, community-based extensions of larger medical centers. As of 2014, there were 62 National Cancer Institute (NCI)-designated cancer centers, and they operated 211 satellite clinics. 19 Approximately 33% of the United States (US) population is within 60 minutes of driving distance from a satellite clinic, compared to 22% within 60 minutes of driving distance from a primary campus. 19
The Siteman Cancer Center, an NCI-designated comprehensive cancer center in the middle of the US, operates 6 satellite clinics. The “North County” satellite is positioned in a region of the city where most residents identify as African American or Black (Figure 1).
20
In early 2023, it was determined that the site was being underutilized by patients with plasma cell dyscrasias, including MM, which occur at twice the rate in the Black community.
1
Most patients who resided in the catchment area, the geographic area from which the clinic expects to receive patients, of the satellite clinic were seeing providers at the primary campus, which is more than 22 miles away from the satellite clinic and can take well over an hour to travel during peak traffic or by public transportation. The catchment area of Siteman cancer Center’s North County satellite clinic
To better serve the community, a new plasma cell dyscrasia subspecialty clinic, which includes MM and related disorders, was opened at the North County Satellite clinic in the summer of 2023. For patients who had already established care with a provider at the primary campus, we performed a structured intervention to identify those living in the satellite’s catchment area, with the goal of offering them the opportunity to transition to the newly opened clinic.
Materials and Methods
In this pilot cohort study, we aimed to determine what proportion of patients who had established care with a provider at the primary campus could be transferred to a provider at a satellite clinic closer to their home. To identify candidates, the researchers prospectively screened the clinic schedules of providers who treated patients with plasma cell dyscrasias at the primary campus weekly from August to December 2023 using the electronic medical record. Patients were considered eligible for transfer if (1) they were receiving care for a plasma cell dyscrasia, including MM and related disorders, and (2) they lived within the satellite clinic catchment area. The satellite clinic catchment area was defined at the onset of the study in collaboration with the research team and the other clinical providers at the primary and satellite clinics using distance from the sites, natural boundaries, such as rivers, and human-made boundaries, such as highways.
Each week, lists of eligible patients were sent to each treating physician, who determined appropriateness of transfer. No formal criteria were provided to the treating physicians to guide their decision; it was left to their subjective opinion. The researchers anticipated that the patients’ clinical circumstances would be the largest determinant. If the patient was deemed a candidate, the physician’s clinical team offered the patient a transition of care at their visit. Patient transfers were prospectively tracked. Those declining to transfer were asked reasons for decisions. Data regarding reasons for transfer eligibility and declining transfer were captured through open-ended questions. The research team reviewed this data and coded them into themes using consensus-based methods.
The study was performed under the supervision of the Washington University IRB (202306162, approved 7/28/2023) and registered with clinicaltrials.gov (NCT05971056). Participants gave informed consent to participate prior to any research procedures being performed. The reporting of this study conforms to the STROBE guidelines. 21
Statistical Analysis
All analyses were descriptive in nature. The proportion of patients who were transferred was presented with 95% confidence intervals (CI), to provide context of what may be expected in the population. Estimates for driving distance and time were calculated using Google Maps. 22 This was a convenience sample of all patients attending the clinic and no formal sample size calculations were performed.
Results
In total, 917 unique patients with plasma cell dyscrasia were identified at the primary campus. The median age was 68 (interquartile range [IQR] 62-74), 57% were male, 80% identified as non-Hispanic White, 17% as African American or Black, and 3% as another race or ethnicity. Of these patients, 62 (7%), including 58 who had MM, were living within the satellite clinic’s catchment area and were evaluated for potential transfer. Of those evaluated for transfer, the median age was 66 (IQR 59-75), 64% were female, and 79% identified as African American or Black. Of the patients with MM, 7% were receiving first-line treatment, 41% were receiving maintenance treatment, 40% were receiving treatment for relapsed or refractory disease, and 12% were being observed off therapy. Participant flow is summarized in Figure 2 and cohort characteristics are summarized in Table 1. Participant flow diagram Participant Characteristics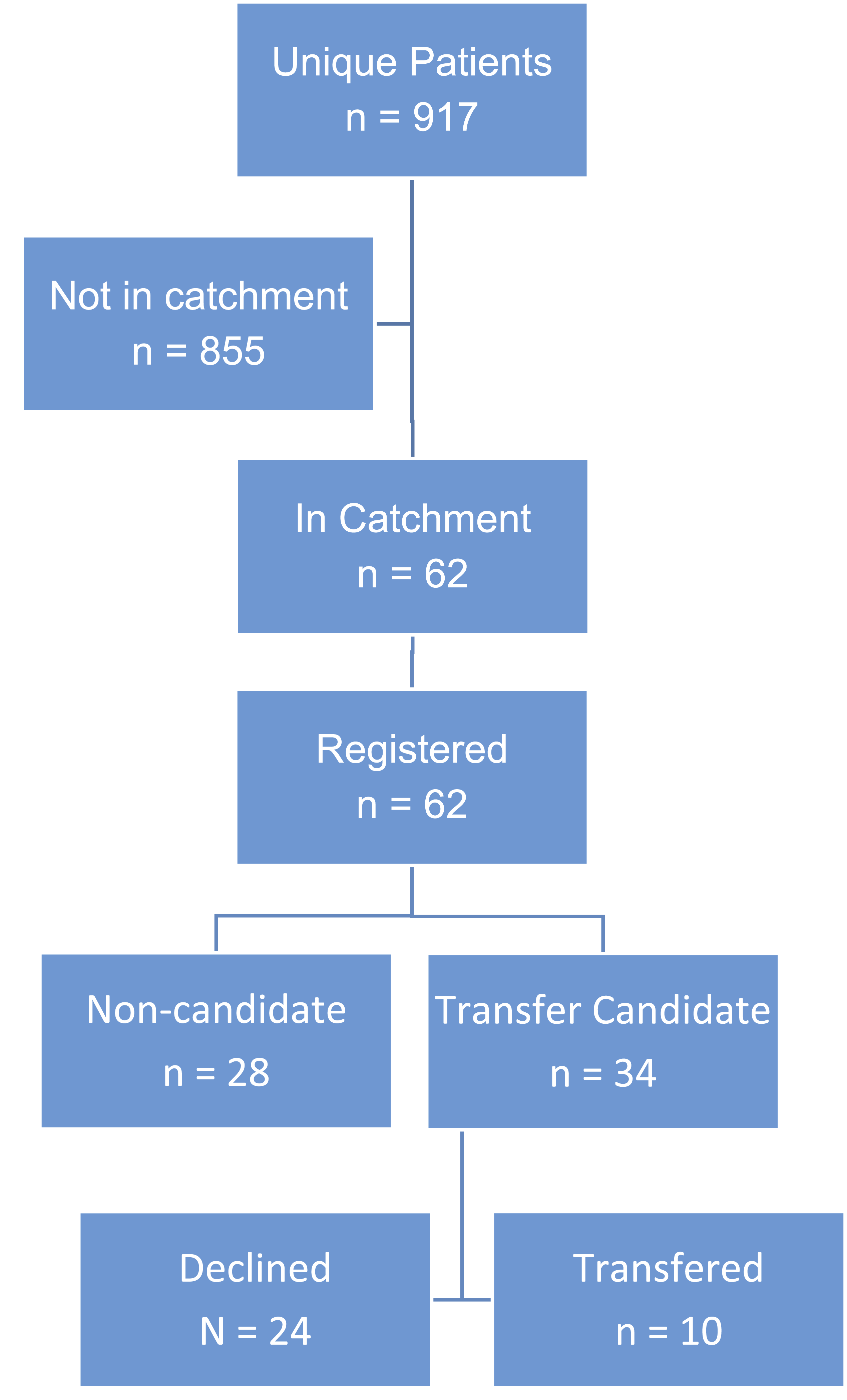

The median distance that patients lived away from the satellite clinic was 5 miles compared to 16 miles away from the primary campus. The median estimated time savings was approximately 34 minutes round trip during typical off-peak travel times.
Comparison of Patients Electing to Transfer With Those That Declined, and Were Deemed Ineligible

Discussion
Transferring patients to a provider at a satellite clinic may seem simple, but this study indicates it is complex in practice. Roughly half of patients who were identified as transfer candidates due to relative distance from their home to the satellite clinic compared to the primary campus were not deemed candidates by their current provider. Interestingly, nearly half of the exclusions were due to provider discretion and not strictly a medical necessity. Moreover, when patients were eligible and offered the opportunity to transfer, most were not interested in making that change, with remaining with their current provider and clinical site, referred to as continuity of care, being the largest cited reason.
As clinical providers for these patients, the authors have seen firsthand how important patient-provider connections are. Anecdotally, there were patients approached about transferring who the provider genuinely hoped would decline due to the patient-provider bond, shared history, and the trust built over months or years. Continuity of care is more than a matter of clinical efficiency; it is emotional security, and relationships between patients and providers are not easily “transferred.”
Despite this, transferring care to another medical provider is not uncommon in the medical system. In 2021, 30% of U.S.-based respondents to a survey reported switching their primary care provider. 23 The largest driver for 1 to change their provider is insurance coverage, with changes in plans or covered providers driving more than half of all transfers. 24 However, more than 10% of patients report parking and transportation issues as a contributing factor. 24
Proximity to the clinic can be a major contributor to the selection of a healthcare provider. In a now dated yet still informative article, Seidelman and colleagues (1983) reported on a community-based family practice in Ontario that moved to a new location, just 2 miles away. 25 Only half of patients followed their providers to the new location. The researchers surveyed patients as to the reason for discontinuing care and over half reported that the location of the new facility was the primary driver. Conversely, some patients choose to travel to hospitals and clinics outside their community, a phenomenon called “patient bypass behavior.” This has been explored most in the context of rural hospitals and clinics. Perceived quality and availability of care are the 2 most cited reasons for this. 26
There is a dearth of data regarding oncology patients transferring care and we are aware of only a few in the literature. In 2012, researchers at Memorial Sloan Kettering reported on a new chemotherapy unit in Brooklyn, approximately 6 miles away from the primary campus in Manhattan. 27 The new facility had many amenities not available at the primary campus, including private treatment rooms. The average wait time was 1 minute at the new facility compared to 66 minutes at the primary campus. Many patients preferred the geographical location of the new facility, with 79% of those attending reporting location as the primary reason for transferring. However, the researchers noted that recruiting patients from the primary campus to attend the new facility was still a challenge but did not report data regarding recruitment effectiveness. Other studies have found that mobile chemotherapy units, which can travel to community hospitals, are popular for some patients, reducing travel burden and associated costs, 28 but also did not report on the proportion of eligible patients electing to utilize the mobile units. To note, in both studies, patients only transferred to the new location for their chemotherapy administration. They continued to see their established provider at the primary campus.
The data presented herein suggests that, rather than transferring established patients, navigating patients to the site closest to their home on the initial referral is likely the more effective strategy to reduce travel-related care burden. In many cases, new patients with hematologic malignancies at the Siteman Cancer Center are referred to the “first available” provider. Location is not always integrated into consult scheduling unless the patient specifically requests 1 of the satellite clinics. Plasma cell dyscrasias, unlike other more acute hematologic malignancies, often allow for some flexibility in initial care planning and small delays in initiating treatment may not impact prognosis. 29 Therefore, incorporating location into referral consideration is prudent.
Another deterrent from transferring to the satellite clinic observed in the current study was availability and perceived quality of care. Six patients were deemed not candidates to transfer because they were enrolled on a clinical trial. Of note, at the time the study was conducted, all plasma cell dyscrasia trials open at the Siteman Cancer Center primary campus were available at the satellite clinic, but the providers still listed this as the reason for transfer ineligibility. Trial availability and enrollment can be limited at satellite clinics. An MD Anderson study reported that only 3% of Radiation Oncology clinical trial enrollments came from their satellite clinics in 2016, despite treating a much greater proportion of potentially eligible patients. 30
More broadly, some patients and providers may perceive that satellite clinics provide a lower quality of care compared to parent institutions—and existing evidence supports this concern. Reinhart and colleagues interviewed staff from NCI-designated cancer centers and found that many key survivorship services that were nearly uniformly available at the primary campus were unavailable at the satellites. 31 A recent systematic review suggests that this sentiment is not exclusive to oncology care. The researchers found that concerns about the quality of care were the most frequently mentioned factor for having a negative attitude towards relocating care from specialty centers to community facilities closer to one’s home. 32 To improve utilization of satellite clinics, hospital systems should further invest in satellite clinics to ensure that care is comparable to that being provided at the primary campus.
This study has several notable limitations. This was a US-based, single center study in an urban area, and results might not generalize to other regions of the U.S. or to international settings. The sample size was modest, and no formal sample size calculations were performed. The relatively small proportion of patients who were eligible and elected to transfer precluded meaningful comparisons; therefore, planned data collection and analyses regarding financial toxicity and patient satisfaction were abandoned. The estimated reductions in travel burden were also modest, which may have contributed to the low rate of transfer. Data regarding reasons for transfer eligibility and declining transfer were captured through open-ended questions and responses may have been subject to interviewer bias, social desirability effects, or other potential sources of bias. In addition, while the subjective exercise of provider discretion in transfer eligibility reduces generalizability, it accurately represents real-world decision-making.
Receiving care at a satellite clinic can bring services closer to home. However, most satellite clinics are in surrounding suburbs of the metropolitan area that the primary campus resides in. Across the U.S., the median estimated drive time is only 9 minutes shorter, each way, if attending a satellite clinic, 19 similar to what was observed in this study. Therefore, attending a satellite clinic may not significantly reduce travel burden.
Conclusion
In conclusion, the findings of this study highlight a barrier to satellite clinic utilization: most patients are not able or willing to transfer once their care is established at the primary campus. Nearly half of patients were deemed non-transfer candidates by their provider. Of those deemed candidates, less than one-third opted to transfer. Ultimately, only 16% of identified patients were transferred. Increasing utilization of satellite clinics—improving access, reducing travel burden, and easing primary campus congestion— likely relies largely on directing appropriate patients to those sites at the outset of their care. Additionally, efforts should focus on building capacity at satellite clinics to enhance both the perceived and actual quality of care, aligning both capacity and quality with those of the primary campus.
Footnotes
Acknowledgements
We would like to thank the patients and clinical providers who participated in this study. Additionally, we would like to thank The Siteman Cancer Center research support team who provided administrative support. The Siteman Cancer Center is supported in part by an NCI Cancer Center Support Grant #P30 CA91842.
Ethical Considerations
This study involves human participants and was approved by the Washington University Human Research Protections Office (07/28/2023, 202306162).
Consent to Participate
Participants gave informed consent to participate prior to any research procedures being performed.
Funding
This research was funded by departmental funds only.
Declaration of Conflicting Interests
The authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article to disclose.
Data Availability Statement
Deidentified participant data are available upon reasonable request to the corresponding author.