
Abstract
Introduction
Delirium is a common neuropsychiatric syndrome in hospitalized cancer patients that is associated with poor outcomes such as increased mortality and prolonged hospital stays. However, clinical predictors of delirium-related outcomes in acutely hospitalized, non-surgical cancer patients remain underexplored.
Methods
This was a retrospective cohort study of hospitalized cancer patients at a tertiary-care oncology center between May 2024 and August 2024 who developed delirium. Delirium was defined by a positive Confusion Assessment Method (CAM) screen. Patients who were admitted for surgical reasons or had an altered mental status (AMS) present on admission were excluded. Patient demographics and clinical factors associated with their hospital course were abstracted from electronic medical records. Primary outcomes analyzed were in-hospital mortality, delirium duration, and length of stay (LOS).
Results
A total of 126 patients met the inclusion criteria from a screening pool of 219 patients. The median age was 65.5 years (IQR: 58,73) and 65 patients (51.6%) were male. Nearly half (43.7%) had hematologic malignancies. Twenty patients (15.9%) died during hospitalization. Non-survivors had significantly lower albumin (3.0 vs 3.5 g/dL, P < 0.01), platelets (86 vs 190 × 103/µL, P = 0.031), BMI (23.3 vs 27.1 kg/m2, P = 0.046), and higher LDH (515 vs 273 U/L, P = 0.044). They also experienced delirium for longer (median 3 vs 1 days, P = 0.011), had a higher incidence of sepsis (27% vs 14%, P = 0.015), and received more benzodiazepines before delirium onset (0.152 vs 0.045 mg/day, P = 0.040). Prolonged delirium (>1 day) was associated with similar factors. LOS positively correlated with delirium duration and sedative exposure, and inversely with hemoglobin and platelet counts.
Conclusions
Delirium in hospitalized cancer patients may reflect underlying physiological frailty that increases susceptibility to mortality from metabolic derangements, malnutrition, sepsis, and sedative exposure. Early identification of these high-risk clinical factors in cancer inpatients with delirium may help mitigate risks posed by these abnormalities.
Plain Language Summary
Delirium is a sudden state of confusion that affects memory, thinking, and awareness that more commonly affects hospitalized older patients. Patients who develop delirium are at increased risk for prolonged hospital stays, long-term functional deficits, and even death. Our study looked at 126 cancer patients who developed delirium while staying in the hospital. We investigated which factors among these cancer patients with delirium led to worse outcomes, such as extended hospital stays and mortality. We identified a variety of clinical factors that were associated with worse outcomes. Firstly, some of the factors we identified were abnormal laboratory values, such as albumin (a protein found in the blood) and platelets (cell fragments that help stop bleeding). Additionally, patients who died experienced longer-lasting delirium and higher instances of severe infection on average. Lastly, patients who died received more anti-anxiety medications with sedative effects while hospitalized. Due to the design of this study, we can only show associations between these factors and worse outcomes. In other words, we do not claim that any of these factors necessarily caused patients to die after they developed delirium. Instead, this study shows that beyond delirium alone, other markers remain indicators of poorer outcomes among hospitalized cancer patients who develop delirium. The results emphasize the importance of the early detection of clinical warning signs and the necessity to monitor which medications are being used in this vulnerable population.
Introduction
Delirium is a syndrome characterized by an acute disturbance in attention and awareness not better explained by another underlying neurocognitive disorder.1,2 It is often accompanied by fluctuating levels of mental status, confusion, and disorganized thinking, and comes in three main subtypes. 3 Hypoactive delirium is the most common subtype and is described as pure lethargy with decreased psychomotor activity. 4 Hyperactive delirium is described as agitated with increased psychomotor activity. 5 Mixed delirium represents a fluctuation between the two extremes. Prognosis and management of patients depend on the presentation of delirium. 6
It is one of the most common neuropsychiatric disorders in hospitalized geriatric patients, affecting approximately 10-31%.7-9 This rate increases to approximately 25-42% among cancer patients and approaches 85% in geriatric cancer patients undergoing end-of-life care.10-12
The development of delirium is associated with increased short-term mortality and longer hospital stays. 9 Adverse outcomes continue after leaving the hospital with greater risks of persistent functional dependence, long-term cognitive impairment, and the inability to resume cancer treatments. 13 These consequences contribute to diminished quality of life for both patients and caregivers as well as higher healthcare costs.
Delirium is often underdiagnosed in clinical settings, with approximately 57-83% of cases being missed. 14 Identifying risk factors and preventing delirium is crucial, as its development in cancer patients is associated with a significantly increased risk of mortality (OR 8.78). 15
To diagnose delirium, clinicians developed The Confusion Assessment Method (CAM). This is the most widely used tool for screening but still requires clinical judgement. The CAM utilizes 4 features to detect the presentation of delirium: an acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. 16 Additionally, acute onset and inattention must be noted along with either disorganized thinking or an altered level of consciousness. 17 There are a number of additional validated delirium screening tools including the 4 A’s Test, Delirium Observation Screening Scale (DDOS), and Nursing Delirium Screening Scale (Nu-DESC), however the CAM score is the most robustly supported and is the assessment of choice at this cancer center.18,19
Current knowledge regarding risk factors for delirium in cancer patients is broad. In a study of 140 cancer patients with delirium, CNS involvement (brain metastases, leptomeningeal disease) were noted in roughly 1 in every 4 patients. 20 In other studies, metabolic disturbances due to electrolyte imbalances, opioids, corticosteroids, benzodiazepines, infection, dehydration, and malnutrition were also recognized as contributors to delirium.21-24 Although the clinical significance of delirium is well-recognized, the existing literature often generalizes risk factors from inpatient populations, leaving a gap in the understanding of delirium for acutely hospitalized cancer patients. It is important to reduce this gap and help clinicians address preventable risk factors for mortality in this population and improve prognosis of these patients.
In this study, we characterized clinical factors associated with delirium development in cancer patients admitted to the medical floor for non-surgical reasons. Our primary aim was to determine what factors are associated with increased mortality, prolonged delirium, and prolonged length of hospital stay (LOS) in these patients. Secondary aims included analyzing the effect of initial altered mental status (AMS) severity with delirium onset and the effect of monitored anesthesia care on altered mental status severity.
Methods
This was an IRB-approved retrospective cohort study in accordance with the Helsinki Declaration of 1975, as revised in 2024, of hospitalized cancer patients with delirium at a tertiary-care oncological hospital (Pro00039944). The need for informed consent was waived in accordance with IRB protocols. Included patients were 18 years or older, admitted to a non-ICU floor between May 2024 and August 2024 for medical management, with a positive CAM screen during their hospitalization. Exclusion criteria included AMS present on admission (POA) or being admitted solely for surgery. Patients were screened consecutively until the end date was reached. Follow-up time was limited to hospital stay only, as longer term outcomes were not assessed.
While patients were hospitalized, trained nurses performed CAM screens during each shift change to assess for delirium. Patients continued receiving screens at shift change while delirious to note if and when the delirium subsided. Since the CAM tool does not directly measure severity nor assess degree of confusion, we sought to quantify this by using a combined score of the alert, verbal, pain, and unresponsive (AVPU) scale with orientation to person, place, and time (A&O). In our combined A&O + AVPU scale, higher scores indicate greater alertness and orientation as follows. 0 = Unresponsive 1 = Responsive to pain only 2 = Responsive to verbal stimuli 3 = Alert but disoriented (A&Ox0) 4 = Alert and oriented to person (A&Ox1) 5 = Alert and oriented to person and place or time (A&Ox2) 6 = Alert and oriented to person, place, and time (A&Ox3)
Thus, this variable served as a proxy for AMS severity. The date of the positive CAM screen was used to gather each patient’s A&O + AVPU score from the medical record that documented delirium onset. Another proxy we utilized not for AMS severity, but overall hemodynamic instability on presentation was the shock index. The shock index is defined as the ratio of heart rate to systolic blood pressure and is commonly used in the emergency department as a rapid way to predict the need for inpatient admission and mortality. Higher scores reflect worse status, with scores greater than 1.3 having a high likelihood ratio for mortality. Traditional cut-offs of 0.7 or 0.9 have also been associated with worse outcomes. 25
Other variables collected were demographics, comorbidities, cancer data (type, stage, brain metastasis status, and prior treatment), time to delirium (based on positive CAM screen), duration of delirium (based on first negative CAM screen), LOS, AMS severity, interventional procedures (defined as any procedure that required the used of monitored anesthesia care), if sepsis occurred while admitted, dose per day of medications delivered prior to delirium (benzodiazepines, diphenhydramine, oral morphine-milligram-equivalents, haloperidol, ramelteon and anti-emetics), admission vital signs (including shock index), and admission lab values (sodium, potassium, chloride, calcium, phosphorous, total bilirubin, creatine, albumin, hemoglobin, platelets, white blood cell count (WBC), alkaline phosphatase (ALP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), blood urea nitrogen (BUN). Lastly, the reporting of this study conforms to the STROBE guidelines. 26
Statistical Analysis
Descriptive statistics were used to summarize baseline demographics and clinical variables. Delirious patients who died were compared to those who survived. Patients who survived were compared across continuous and categorical variables with Mann-Whitney U tests or Pearson’s chi-square tests of independence, respectively. Associations between LOS and continuous variables were analyzed using Spearman’s rank correlations, while Mann-Whitney U tests were used for categorical variables. The effects of interventional procedures on AMS severity and the effect of AMS severity on outcomes were assessed using similar methods to the above analyses. Medication dosages were normalized to allow comparisons between patients by calculating the total doses received before becoming delirious divided by the days prior to delirium onset (total dose over non-delirious days/non-delirious days). All statistical tests were two-tailed with a significance threshold of P < 0.05 and no power analysis was performed prior. Analyses were conducted using Python. 27
Results
Between May 2024 and August 2024, 219 admitted patients had positive CAM screens. A total of 126 patients were included in the final sample after inclusion/exclusion screening (Figure 1). The median age was 65.5 years (IQR: 58, 73) and 65 patients (51.6%) were male. The median BMI was 26.47 kg/m2 (IQR: 23.50, 60.59). For full patient demographics and comorbidities, refer to Table 1. Study Flow Diagram. A total of 57 Patients were Excluded: 43 Due to Surgery as the Primary Presenting Reason and 14 Due to Altered Mental Status (AMS) Present on Admission (POA) Baseline Demographics and Comorbidities for Full Cohort (n = 126) Table 1 shows the demographics and abbreviated past medical history for the full cohort of patients without regard to mortality status. Acronyms: IQR = interquartile range; BMI = body mass index.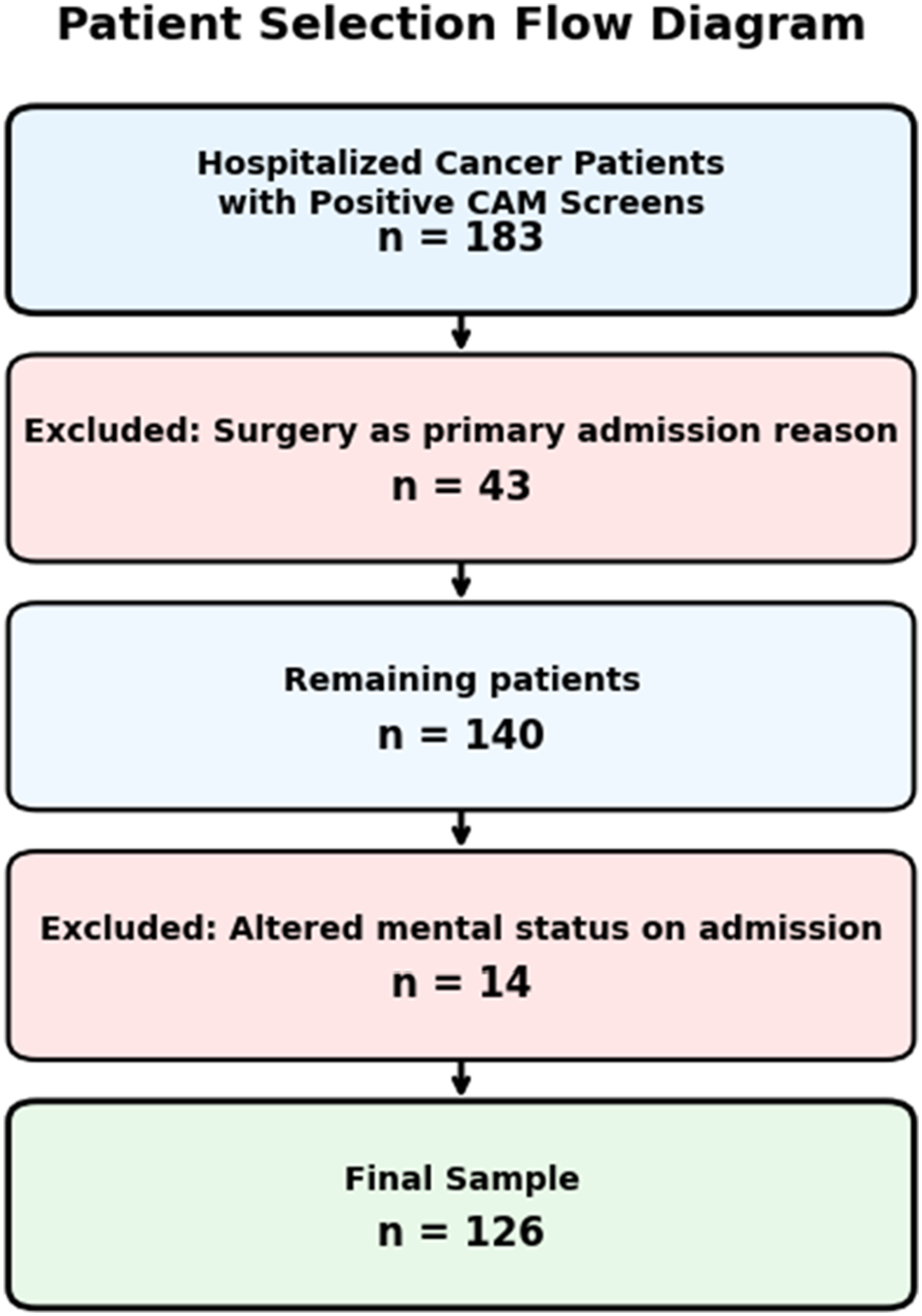

The median LOS was 11 days (IQR: 6, 22.5) and the median duration of delirium was 1 day (IQR: 1,3). Most patients developed delirium shortly after admission (median 4 days, IQR: 1.25, 13.00).
Cancer Data for Full Cohort (n = 126)
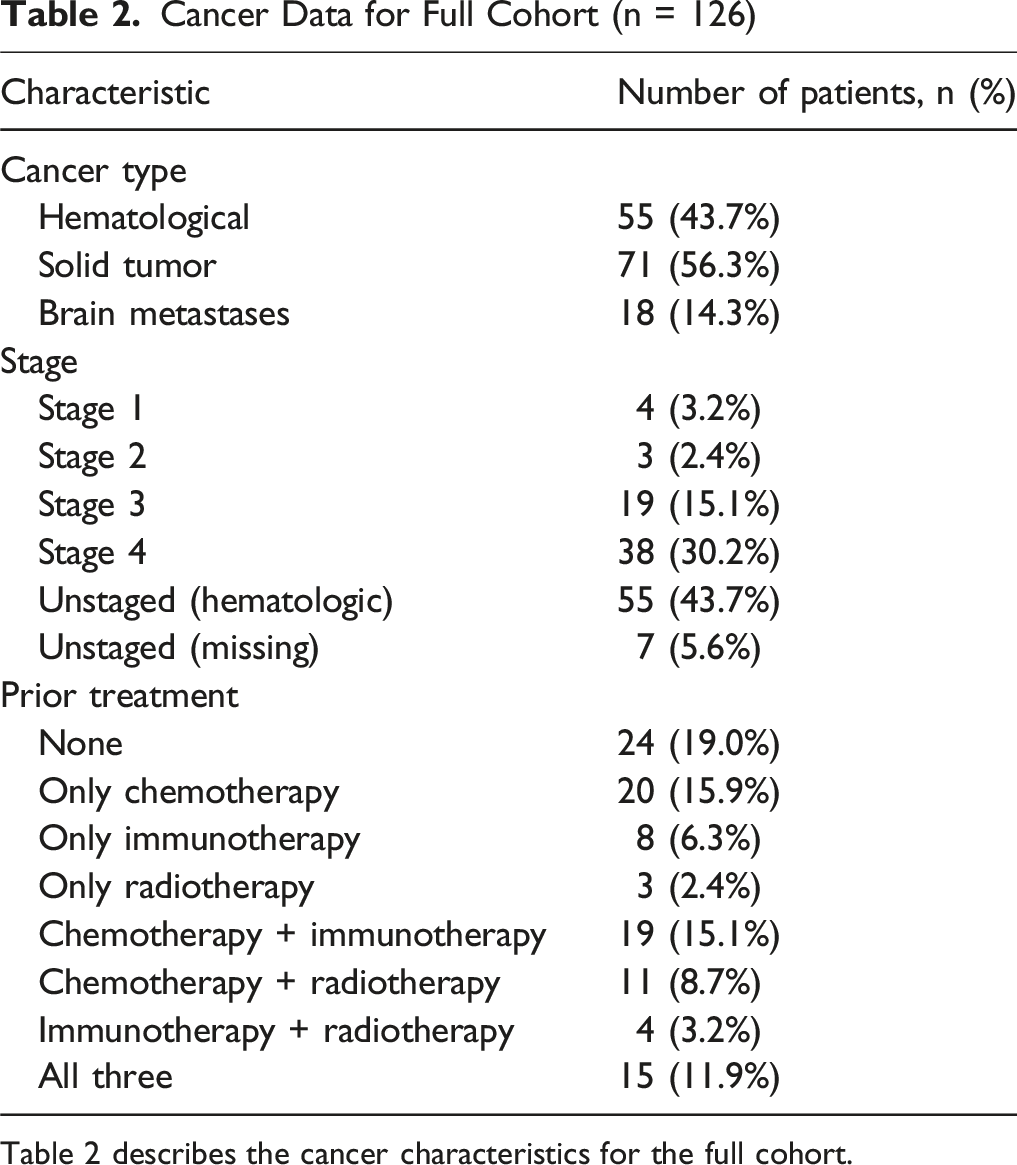
Table 2 describes the cancer characteristics for the full cohort.
On admission, patients were anemic (median 9.7 g/dL, IQR: 8.2, 11.1) with slightly lower albumin levels (median 3.4 g/dL, IQR: 3.0, 3.8). LDH values were also elevated (median 300 U/L, IQR: 214, 547). Vital signs tended to be stable on admission; however, the median shock index was slightly elevated (0.74, IQR: 0.59, 0.89).
During the hospital course, 23 patients (18.3 %) developed sepsis, and 60 patients (44.1 %) underwent an interventional procedure with monitored anesthesia care. These interventions included, but were not limited to, central line placement, G-tube placement, bone marrow biopsy, GI endoscopy, bronchoscopy, paracentesis, and thoracentesis. Notably, patients undergoing a procedure with monitored anesthesia care had significantly lower AMS scores on the day of delirium (A&O + AVPU = 4 vs A&O + AVPU = 5, P = 0.016). However, the bedside measure of our AMS scoring for confusion severity did not have any significant association with death (χ2 = 0.13, P = 0.7) or length of stay (ρ = −0.15, P = 0.09).
Mortality Comparisons

Table 3 compares differences between survivors and non-survivors. Two-tailed Mann-Whitney U tests were performed to calculate the P-values. Acronyms: LDH = lactate dehydrogenase; BMI = body mass index.

Boxplots for Key Differences between Survivors and Non-Survivors. Delirium Duration, Albumin, LDH, Platelet Count, BMI, and Calcium are Visualized Based on Mortality Status
There were 2 patients in the non-survivor groups with markedly higher LDH levels and longer delirium durations (Figure 2). The analysis was repeated with a combined IQR and min-max removal method to test robustness. All relationships remained statistically significant (P < 0.05). Subsequently, removing only the maximum LDH patient from the analysis resulted in the attenuation of differences in LDH levels between groups (P = 0.10). This group had the smallest sample size due to availability of LDH values, but the trend remained that survivors had lower LDH levels.
Total LOS was influenced by factors similar to those associated with mortality. Longer delirium, higher normalized diphenhydramine use prior to delirium, and higher normalized ramelteon use prior to delirium all weakly correlated with LOS (ρ = 0.20, P = 0.022; ρ = 0.28, P < 0.01; and ρ = 0.29, P < 0.01 respectively). The relationship between delirium duration and LOS is shown in Figure 3. Higher hemoglobin levels and platelet counts were discharged sooner (ρ = −0.30, P < 0.01 and ρ = −0.36, P < 0.01 respectively). Delirium Duration vs Total Length of Stay. This Graph Depicts Spearman’s Rho for Delirium Duration and LOS
Lastly, differences between short and long delirium were analyzed. Prolonged delirium was defined as lasting longer than 1 day (n = 60 patients). These patients had higher LDH levels (median 338 vs 228 U/L, P = 0.029), lower platelet levels (median 125 vs 212 × 103/L, P = 0.049), and a higher sepsis incidence (27% vs 11%, P = 0.036) than those with short-term delirium. Those with prolonged delirium also had a higher incidence of anxiety (18% vs 4%, P = 0.030). Notably, patients with anxiety were also significantly younger (median 58.5 vs 66 years, P = 0.031).
Discussion
In this study of cancer inpatients with delirium, we identified several key clinical and laboratory predictors of increased length of hospital stay, increased length of delirium, and mortality. Most patients in this cohort had advanced or hematologic malignancies and developed delirium early during their hospitalization. While the median duration of delirium was brief, prolonged episodes were associated with significantly worse clinical outcomes.
Among the 126 included patients, the median age was 65.5 years (IQR: 58, 73), which is lower than other studies that looked at cancer patients with acute illnesses or admitted cancer patients.28,29 This may be due to our institution being a highly specialized tertiary center, resulting in sampling bias of cancer patients with a higher disease burden. Ultimately, 15.9% died during hospitalization. Patients who died had significantly lower BMI, albumin, calcium, and platelet levels. Additionally, sepsis was significantly more prevalent among those who died (27% vs 14%). These findings align with prior literature that have identified lower BMI, hypoalbuminemia, thrombocytopenia, and sepsis as predictors of mortality in oncologic populations.30-32 Furthermore, patients who died during hospitalization had significantly higher LDH levels compared to those who survived to discharge. As an established marker for cachexia, along with BMI, there is already strong evidence for elevated LDH as a predictor for mortality in cancer patients.33,34 Collectively, these factors underscore the physiological frailty of patients who experience both delirium and mortality during cancer hospitalization.
Delirium characteristics were also significantly associated with mortality in our cohort. Patients who died experienced longer delirium episodes (median 3 vs 1 day), suggesting that duration may be a clinically relevant marker of physiologic decline. While delirium is an established predictor of mortality in cancer patients, this study adds to the growing body of evidence that the duration of delirium independently predicts in-hospital mortality as well. Highlighting this connection, Tao et al in 2024 showed that patients with late onset delirium lasting more than 3 days were 4.45 times more likely to die in the ICU than those with early-onset delirium lasting less than 2 days. 35 However, to our knowledge, our study is the first to establish this relationship for the admitted adult cancer patient on non-ICU floors.
Those who died also had significantly more normalized benzodiazepine use prior to delirium. The current literature, in general, supports this finding. Benzodiazepine use has been shown to correlate with mortality in critically ill patients in the past and some potential explanations exist for this relationship. 36 The immunosuppressive effects of benzodiazepines may increase susceptibility to infection, and their sedative properties may mask signs of clinical deteroiation.37,38 Moreover, it is well-established that benzodiazepines can worsen transient delirium. 39 They decrease the release of acetylcholine, a key neurotransmitter involved with memory, learning, and other physiological processes. Low levels of acetylcholine have been implicated in the occurrence of delirium. 40 The combination of these factors in our vulnerable cohort can explain, in part, why this association was observed.
With regards to delirium duration risk factors, patients with prolonged delirium (>1 day) exhibited clinical features similar to those seen in non-survivors, such as elevated LDH, lower platelets, and higher rates of sepsis. However, in addition, these patients had higher exposure to diphenhydramine and ramelteon. Previous literature has highlighted the risk of diphenhydramine, but ramelteon has not been previously shown to exacerbate acute delirium.41,42 Past studies suggest ramelteon actually reduces delirium risk by stabilizing sleep-wake cycles. 43 While the blunted arousal caused by ramelteon could contribute to a lack of mental clarity, we suspect ramelteon is acting as a proxy for high-risk patients rather than a potential cause of prolonged delirium.
A pre-existing diagnosis of anxiety was associated with being younger in age and prolonged delirium. Regarding age, pre-existing neuropsychiatric conditions increase susceptibility to delirium and help explain why there was a significant difference in age between those with and without anxiety. 44 In terms of delirium duration, anxiety may increase a patient’s vulnerability to delirium through chronic hyperactivation of the stress response, dysregulation of sleep, and altered neurotransmitter balance.44,45 Furthermore, with older adult inpatient cancer-patients, these effects can be exacerbated by reductions in cognitive reserve, polypharmacy, and the physiologic effects of malignancy.46,47 Screening for anxiety and depression to initiate supportive psychiatric care, if needed, may play a critical role in preventing or mitigating prolonged delirium by identifying those at higher risk.
Length of stay was similarly affected by delirium characteristics and clinical status. Longer delirium duration, diphenhydramine use, and ramelteon use were each positively correlated with increased length of stay, while higher hemoglobin and platelet counts were associated with shorter stays. These findings reinforce the need for proactive delirium prevention strategies and highlight the importance of addressing modifiable risk factors.
Interestingly, patients who underwent interventional procedures (prior to delirium) under monitored anesthesia care demonstrated significantly worse presenting AMS at delirium onset. These procedures included a range of diagnostic and therapeutic interventions, but none were done in the operating room. While this indicates that even light anesthetic with interventions may increase confusion, mental status on the day of delirium did not meaningfully impact length of stay, delirium duration, or mortality. However, given the literature and known role of anesthetics in delirium, it may have been the contributing factor for the initial development of delirium in those patients.48,49 It is also possible that this study is underpowered to draw further conclusions about the effect of light anesthesia on our other outcomes.
Because this was a retrospective cohort without extensive multiplicity control, we caution several limitations. First, it was conducted at a single site over a short time window, which may limit generalizability. Our sample size was also limited by patients that met the inclusion criteria and lack of power analysis. We therefore caution the interpretation of non-significant relationships that were found as the study may have been underpowered. Second, the CAM screening tool, while validated, may under-detect hypoactive delirium and unlike the CAM-S screening tool, the one used does not grade AMS severity. While we used a combination of the well-known A&O and AVPU scores as proxy due to retroactive availability, other measures of mental status (the Glasglow Coma Scale and Richmond Agitation Sedation Scale) have been shown to more accurately predict mortality. 50 Furthermore, our operationalization of these variables with a 6 point scale has not been validated in previous literature. Third, our study only looked at medications given prior to a positive delirium screening. We did not analyze dosing for the patients while they were delirious. Fourth, by normalizing doses of medications, we cannot identify whether the delirious effects were due to an inciting bolus or a cumulative effect. Fifth, other medication classes commonly administered to hospitalized cancer patients, such as anticholinergics, were not evaluated in our cohort. Consequently, potential confounding effects from these medications cannot be excluded, and further research is warranted to elucidate these relationships. Lastly, observational design precludes us from inferring causality.
Future research should focus on validating these associations in larger, multi-center cohorts and developing evidence-based protocols for modeling mortality risk after the development of delirium. By reframing delirium not just as a complication but as a measurable and modifiable indicator of physiologic decline in hospitalized cancer patients, alongside other clinical factors, clinicians can better tailor care and improve outcomes for this high-risk population.
Conclusion
In our retrospective cohort study of 126 hospitalized adult cancer patients, we identified several modifiable and non-modifiable factors that were associated with a poor prognosis. Hypoalbuminemia, thrombocytopenia, and elevated LDH were consistently linked to higher in-hospital mortality and prolonged delirium. The use of diphenhydramine and benzodiazepines were associated with the development of prolonged delirium and worse outcomes. Additionally, the duration of delirium emerged as a prognostic factor in this population, with longer episodes correlating to higher in-hospital mortality and extended length of stay. While AMS at the time of delirium onset was more severe in patients that had previous interventions with monitored anesthesia care, this did not translate into worse outcomes. Importantly, there was a lower median BMI and higher rate of sepsis in patients who died in the hospital. Early identification of high-risk individuals with delirium, particularly those with poor nutritional status, hematologic abnormalities, and exposure to sedative agents, may enable targeted interventions aimed at mitigating delirium severity and duration.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board of Moffitt Cancer Center (Pro00039944) on October 08, 2024, with the need for written informed consent waived.
Consent to Participate
The requirement for informed consent was waived by the institutional review board.
Author Contributions
All authors have made substantial contributions to study conception and design, BD, JK, and RB to data acquisition, BD to data analysis, BD, JK, RB, and JH to data interpretation, all authors contributed to manuscript writing and critical revision. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
A retrospective dataset was created during the study and will be maintained for 5 years from the start of the study. Deidentified patient variables may be obtained by contacting the corresponding author with approval or an exemption statement from our institutional review board.