
Abstract
Introduction
This scoping review systematically mapped the landscape of peer-reviewed publications on colorectal cancer (CRC) research in Libya to identify prevailing trends and knowledge gaps that can inform national cancer control strategies.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines, a comprehensive search of open-access databases was conducted.
Results
Findings from 42 eligible studies published between 1993 and 2024 revealed a fragmented research landscape with significant methodological and geographic disparities. Most of the studies were retrospective, hospital-based, and concentrated in northern urban centers such as Benghazi, Misrata, and Tripoli, leaving southern and peripheral regions underrepresented. Thematic analysis revealed an over-reliance on descriptive epidemiology, with minimal reporting on tumor characteristics, molecular profiling, or treatment outcomes. The research ecosystem also faces structural challenges, including dispersed authorship and inconsistent reporting of ethical and funding information, with the limited visibility of local journals further impeding their global reach.
Conclusion
These findings indicate that peer-reviewed publications on CRC research in Libya are in a nascent developmental phase, facing structural and spatial challenges. Strengthening the research ecosystem will require an active centralized cancer registry, investment in molecular diagnostic infrastructure, and the adoption of inclusive, prospective, and community-based study designs. Addressing these systemic gaps is crucial for generating actionable and representative evidence to improve cancer outcomes nationwide.
Plain Language Summary
Colorectal cancer (CRC) is a major health concern in Libya, but research on the disease is limited and unevenly distributed. In countries with fewer resources, like Libya, understanding how research is conducted and where the gaps are is essential for improving cancer care and outcomes. This study aimed to map out existing CRC research in Libya and identify areas that need more attention. Forty-two published studies on CRC in Libya from 1993 to 2024 were reviewed. The review examined covered topics, study designs, and geographical locations. Furthermore, the studies were assessed for the inclusion of key details such as cancer stage, tumor type, ethical approval, and funding sources. Most studies were based in hospitals and used patient records. Research was concentrated in northern big cities, while southern and rural regions were largely excluded. Many studies focused on basic patient statistics, with few exploring treatment outcomes, genetic factors, or prevention strategies. Limited studies reported the tumor details such as stage and anatomical location, and only a small number of studies reported ethical approval or funding. Most were published in journals with limited international reach. This review highlights the need for stronger, more inclusive cancer research in Libya. To improve CRC outcomes, future studies should include diverse populations, use modern research tools, and focus on practical solutions. Building a national cancer registry, investing in laboratory infrastructure, and supporting ethical, well-funded research are key steps forward. Importantly, researchers and policymakers must also consider cultural beliefs, health-seeking behaviors, and local system constraints when designing studies and implementing interventions. Tailoring solutions to the local unique social and healthcare context will help ensure effectiveness, sustainability, and equity across all regions of the country.
Keywords
Introduction
CRC is a prevalent malignancy and a leading cause of cancer-related mortality globally.1,2 Once considered a disease of high-income countries (HICs), CRC incidence and mortality are rising rapidly in low- and middle-income countries (LMICs) due to demographic transitions and Westernized lifestyles.1,3 This shift has created a distinct epidemiological profile in LMICs, where patients present at a younger age with a higher proportion of early-onset CRC and are often diagnosed at late stages.4,5 This late diagnosis is largely due to underdeveloped screening programs, strained healthcare systems, and limited public awareness.6,7 These challenges are particularly severe in conflict-affected regions such as Libya, where prolonged instability further compounds existing healthcare limitations. 8
Libya, a North African country, reflects these broader LMIC trends. CRC is the second most common cancer and the second leading cause of cancer-related mortality among men and women. 9 The age-standardized incidence and mortality rates are among the highest in North Africa, 10 and the cumulative risk of developing CRC before age 75 is estimated at 1.6%. 9 Notably, Libya exhibits a gender pattern reversal, with a higher CRC incidence reported among females, where it is typically more common in males. 11
Despite the growing burden of CRC, Libya’s research output is markedly limited. A bibliometric analysis of cancer research across 22 Arab countries from 2005 to 2019 found that Libya contributed only 131 cancer-related publications (less than 0.5% of the region’s total output), placing it among the lowest contributors to cancer research. While CRC has garnered increasing attention regionally, with 1169 publications identified, Libya’s contribution to this body of work was minimal according to this bibliometric analysis by Machaalani et al. in 2022. 12 More recently, a 16-year bibliometric analysis (2007-2023) published by Abbas et al. further underscored this gap: the analysis revealed that Libya had no recorded scientific production on CRC screening despite elevated national incidence and mortality rates. In contrast, high-income countries, such as Saudi Arabia and Qatar, demonstrated substantial and growing CRC research publications, which were more closely aligned with their disease burden. This disparity highlights the urgent need for context-specific evidence to inform CRC prevention, early detection, and control strategies in Libya. 13
Research output from LMICs, such as Libya, encounters barriers such as limited funding and infrastructure, and difficulties in disseminating findings in international journals due to complex submission processes and high article processing charges (APC). 14 These systemic issues create a vicious cycle in which a lack of resources hinders research, which in turn limits the evidence needed to secure funding and improve public health outcomes. Furthermore, locally published studies are often internationally inaccessible because of language barriers and inconsistent reporting standards. Consequently, the overall evidence base on CRC in Libya remains fragmented, impeding local policy-making and global understanding of the disease. Despite the rising burden of CRC in Libya, no prior review has systematically mapped the scope, quality, and accessibility of published research, which limits the ability to plan for evidence-based cancer control strategies. This is particularly urgent in post-conflict settings, where infrastructure and policy reforms are underway, and foundational evidence is needed to guide the development of resilient cancer systems.
This scoping review addresses the following question: What are the methodological patterns, thematic gaps, and structural barriers in peer-reviewed publications on CRC in Libya? Given this fragmented literature, a scoping review is well-suited to systematically map the peer-reviewed publications on CRC in Libya. Following the methodological framework proposed by Arksey and O’Malley 15 and further refined by the Joanna Briggs Institute 16 , this approach allows for a comprehensive overview of the current research landscape, which is essential for identifying critical gaps. Given the exploratory nature of the research question and the heterogeneity of study designs, a scoping review is the most appropriate method for capturing the breadth of evidence and identifying gaps in peer-reviewed publications on CRC in Libya.
This review aims to capture both locally and internationally published literature to identify gaps, thematic trends, and opportunities for future research. To our knowledge, this is the first comprehensive synthesis of peer-reviewed CRC research published in Libya.
The review seeks to: • Identify the volume and characteristics of peer-reviewed publications on CRC in Libya. • Analyze methodological trends and research design. • Explore barriers influencing the production and dissemination of peer-reviewed publications on CRC.
By addressing these objectives, this review will provide a comprehensive overview of the current state of peer-reviewed publications on CRC research in Libya, highlight critical gaps, and inform strategies to strengthen research capacity and improve patient outcomes in Libya and comparable LMIC settings. Ultimately, this study contributes to the foundational evidence needed to build resilient cancer control systems in limited-resource and post-conflict environments, as emphasized in recent global health dialogues.
Methods
This scoping review followed the PRISMA-ScR guidelines, 17 ensuring a comprehensive, transparent, and reproducible mapping of peer-reviewed publications on CRC in Libya, aligned with current best practices. The method utilized for evidence synthesis was a descriptive mixed-methods approach tailored to map the scope of CRC literature. This involved a quantitative analysis to summarize article characteristics (e.g., geographic location, publication trends, thematic focus) and a qualitative narrative synthesis to describe and interpret key findings, research gaps, and authorship patterns. This approach allowed for comprehensive mapping of the volume and nature of peer-reviewed published CRC research in Libya.
Protocol and Registration
A protocol outlining the objectives, eligibility criteria, and analytic methods was developed before the review. Although not formally registered, it adhered to the PRISMA-ScR recommendations and guided study implementation and reviewer calibration.
Eligibility Criteria
Studies were included based on the following criteria. • Population and Context: Focused on CRC in Libya, involving Libyan participants or biological samples (e.g., tissue, biopsies) from Libyan patients, regardless of the author’s nationality or affiliation. • Conceptual Scope: Covered any CRC-related topic, prevention, screening, awareness, policy, epidemiology, diagnosis, treatment, or outcomes. Sub-sites such as the colon, rectum, and sigmoid cancers were included. • Study Design: Peer-reviewed empirical studies using quantitative, qualitative, or mixed methods, as well as narrative reviews and clinical case reports. • Language: Published in English or Arabic. • Accessibility: Full texts available through public or institutional sources; abstracts without full access were excluded. • Publication Status: Published in peer-reviewed journals with accessible metadata.
Exclusion Criteria:
Studies were excluded based on the following criteria: • Did not involve Libyan human subjects or biological samples. • Focused on non-CRC malignancies or lacked contextual relevance to Libya. • Editorials, commentaries, conference abstracts without full articles, or grey literature (e.g., theses, institutional reports).
This framework ensures the inclusion of verifiable, context-specific research on CRC epidemiology and healthcare in Libya while maintaining methodological integrity.
Information Sources
A structured literature search was conducted using PubMed, Google Scholar, and African Journal Online (AJOL). PubMed and Google Scholar were chosen for their broad open-access biomedical indexing. AJOL was included to cover African-published journals, specifically Libyan-affiliated journals relevant to the review. This combination of databases ensures comprehensive and accessible coverage, particularly for researchers in LMICs with subscription restrictions. This approach emphasizes reproducibility in resource-constrained settings, aligning with evidence mapping in LMICs.
Additionally, a manual search was performed on unindexed Libyan scientific journals and reference lists of the included studies to identify missed records. The search was restricted to English and Arabic publications and was not restricted by publication status. It was applied using the maximum historical range possible, from January 1, 1900, to 2024. This broad timeframe was selected to ensure the capture of all published evidence on CRC research in the Libyan context since the inception of the major indexing databases. No contact was made with the study authors for extra data, and no automation tools were used for screening or deduplication.
Search Strategy
Search Strategies for Electronic Databases
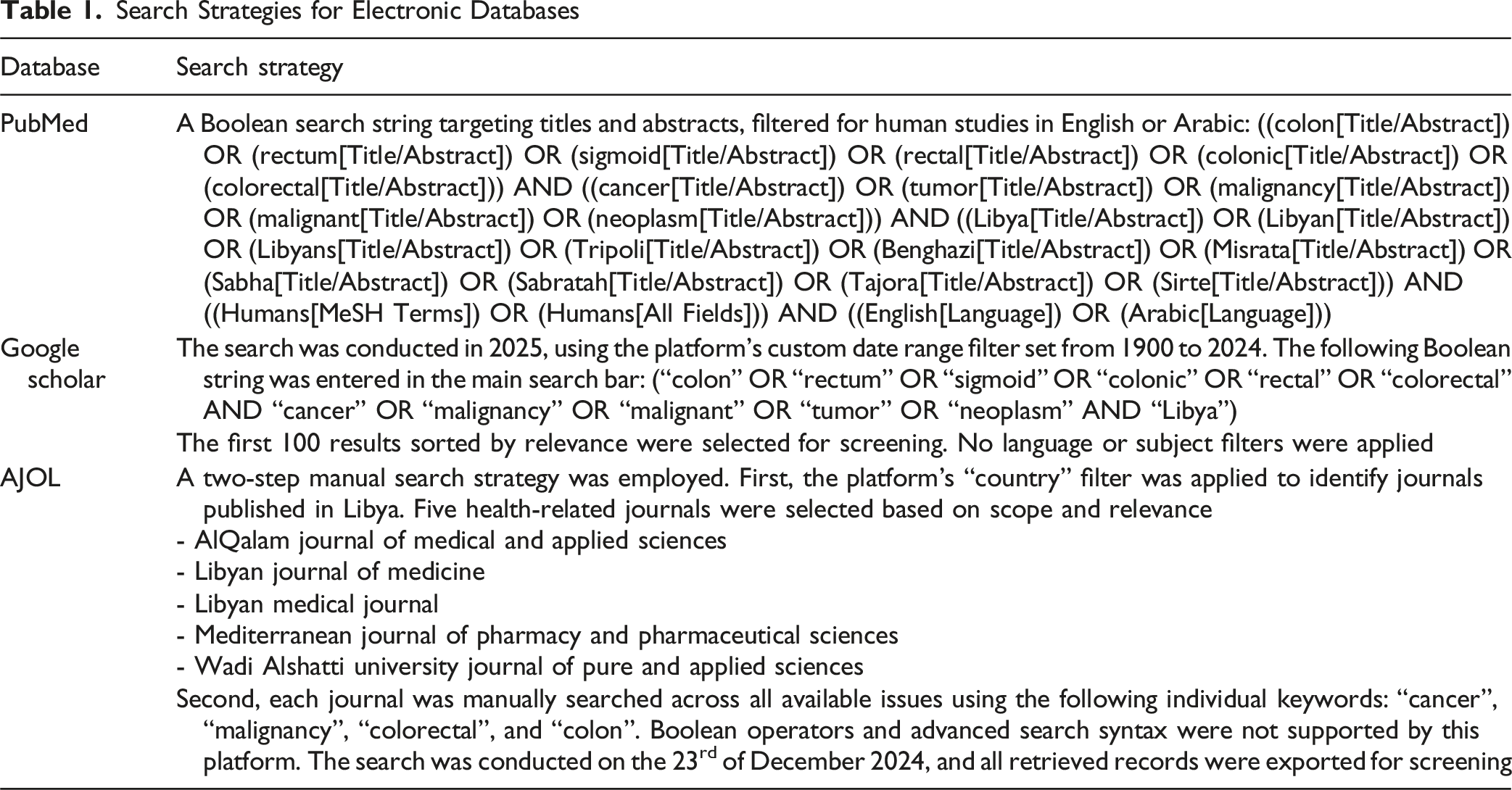
To supplement the electronic database searches and enhance the coverage of locally published research, a manual hand search was conducted in January 2025. This involved screening all available issues of 2 key Libyan health journals, the Libyan Journal of Medical Sciences and the Libyan Journal of Public Health Practices, which are not indexed in the major bibliographic databases. Relevant keywords (“cancer”, “malignancy”, “colorectal”, “colon”) were applied across titles and abstracts. Additionally, backward citation tracking was performed by reviewing the reference lists of the included articles to identify earlier studies that might have been missed in the initial searches. Records identified through these processes were exported and screened alongside the database results.
Selection of Sources of Evidence
All citations retrieved through database and manual hand searches were consolidated into a Microsoft Excel spreadsheet. Duplicate records were identified and removed, and the resulting master sheet was used to coordinate the reviewer assignments and track the decision outcomes throughout the screening process.
To ensure consistency among the reviewers, we conducted a calibration exercise before beginning the review. All 5 reviewers independently screened the same ten titles and abstracts. The results were then discussed, and any inconsistencies were resolved to refine our understanding of the eligibility criteria. This process helped standardize the screening forms and clarify how the exclusion criteria were applied. The study selection followed a two-stage, team-based protocol.
Initial Screening (Title and Abstract Review)
A team of 5 reviewers independently screened the titles and abstracts in pairs. Decisions on inclusion and exclusion were documented in a shared Google Sheet. Any conflicts were resolved by a third reviewer, and the final decision was determined by majority rule.
Full-Text Eligibility Assessment
Following the initial screening, 2 reviewers independently assessed the full texts of all potentially eligible articles. A structured Google Form developed from the study’s inclusion criteria was used. To ensure consistency, all reviewers were trained to use the form and completed a calibration exercise with a sample of 10 articles. The principal investigator provided continuous support throughout the process. For each exclusion, reviewers were required to select a reason from a predefined list: “Not conducted in Libya or study subjects are not Libyan,” “Not related to CRC,” “Not a research article,” “Not in English or Arabic,” and “Inaccessible in full text.” A third reviewer resolved any discrepancies, with the majority decision being the final decision.
This rigorous two-stage protocol ensured methodological consistency, minimized bias, and improved inter-rater reliability. A PRISMA-ScR flow diagram in the results section details the screening results.
Data Charting Process
A standardized Google Form was developed to collect information to be extracted from each study. This form was pilot-tested using a sample of the included studies to ensure a shared understanding of each field and to improve consistency across reviewers. It also served as an informal inter-rater reliability measure, aligning the interpretation of the charting criteria before full data extraction.
Each article was independently charted by 2 reviewers, with categorical and free-text responses captured based on the review objectives. No attempts were made to contact the study authors for clarification or for additional data. Once charting was complete, the lead reviewer conducted a final verification of all extracted entries to ensure each entry’s accuracy and coherence prior to synthesis. Discrepancies were adjudicated by a third reviewer, and a majority decision process was used to ensure procedural consistency and minimize bias. This process reflects a commitment to a reproducible scoping review methodology in settings constrained by limited access to centralized research metadata.
Data Items
A data charting form was developed using Google Forms to ensure a structured and consistent approach. The extracted variables were aligned with the study objectives and included the following domains: • Article and Study Characteristics: Title, DOI or access link, publication year, study design, sample size, stated aim, setting (e.g., hospital, municipal), timeframe, geographic coverage, and classification as locally led or collaborative. • Population Details: Sex and age. • Cancer-Related Attributes: Anatomic site, cancer type, stage at diagnosis, and degree of differentiation (where reported). • Authorship and Institutional Affiliation: First author’s name and gender, institutional affiliation, and city. • Ethics and Funding Transparency: Presence of ethics approval, name of the approving body (if available), funding disclosure, and declared funding sources. • Journal Metrics: Journal name, impact factor (where known), and quartile ranking (Q1–Q4, if available). • Thematic Focus: Primary study outcomes, such as screening, treatment, prevention, awareness, and epidemiological characterization. Multiple thematic codes were assigned to the data when applicable.
Missing data were documented as “Not stated,” and no imputation or assumptions were made. The collected data were managed and synthesized using Microsoft Excel software. Due to heterogeneity in age reporting (e.g., mean, median, grouped ranges), participant ages were not treated as quantitative variables but were broadly classified as adult populations.
Critical Appraisal of Individual Sources of Evidence
Consistent with the scoping review methodology, we did not perform a formal critical appraisal or risk of bias assessment of the included studies. This aligns with the guidance from PRISMA-ScR, which prioritizes mapping the breadth and thematic landscape of the available evidence over evaluating the quality of individual studies. Our intent was to provide an overview of research activity and its structural attributes, not to determine the effectiveness or validity of specific findings.
Synthesis of Results
The extracted data were compiled in Microsoft Excel and imported into the SPSS (version 26) for statistical analysis. Categorical variables were summarized using descriptive statistics, including frequency counts and proportions, to map the distribution, scope, and characteristics of the included studies.
The synthesized findings were organized across the following analytical domains: • Study Design and Data Source: Classification of methodological approaches (e.g., observational, case series) and data origins (primary vs secondary). • Geographic Distribution: Regional mapping based on institutional locations and the participant recruitment sites in Libya. • Thematic Categorization: Grouping of studies under 5 dominant CRC focus areas: ◦ Clinical Characteristics and Diagnosis ◦ Epidemiology and Incidence ◦ Molecular and Genetic Studies ◦ Treatment and Outcomes ◦ Risk Factors & Etiology • Tumor Characteristics: Documentation of histological types, anatomical sites, staging, and differentiation (when reported). • Authorship and Collaboration Patterns: Classification of studies as locally led vs internationally co-authored and analysis of the first author’s institutional affiliation. • Gender Determination and Classification: The first author’s gender was determined based on native knowledge and cultural expertise of common Libyan naming conventions. Due to the distinctive nature of these names, sex (Male or Female) was assigned based on the publication name. Authors with unfamiliar names and those not easily recognizable as Libyan and whose gender was unclear were classified as Unknown. This ensures accurate local classification while flagging ambiguous cases. • Ethical Oversight and Funding Transparency: Presence of documented ethics approval and funding disclosures, including named approving bodies and sponsors. • Journal Quality Indicators: Impact factor and quartile ranking (Q1–Q4), when available.
To maintain data integrity, studies reporting overlapping cohorts were carefully reviewed and not counted twice.
Age variables were treated descriptively because of heterogeneity in the reporting format. Mean, standard deviation, and range data were preserved when available. For studies presenting age categories (e.g., “<40 years” or “>60 years”), participants were conservatively classified as adults in accordance with broader eligibility criteria.
The results were synthesized using tables and narrative interpretation to illuminate key patterns, gaps, and structural characteristics in Libya’s peer-reviewed publications on CRC in Libya.
Ethical Considerations
This scoping review did not require ethical approval because it involved the synthesis of data from publicly available sources and did not include human participants, identifiable personal data, or biological materials. In accordance with international guidelines for research ethics, such studies are exempt from Institutional Review Board oversight.
Results
Study Selection
The initial search and selection processes followed the PRISMA-ScR guidelines, as illustrated in the flow diagram (Figure 1). A total of 287 records were identified across 4 sources: PubMed (n = 93), Google Scholar (n = first 100), AJOL (n = 83), and hand searching (n = 11). After removing 39 duplicate records, 248 unique citations were screened by title and abstract, resulting in the exclusion of 129 records. These exclusions were primarily due to a lack of relevance to the Libyan context or a focus on cancer types outside the scope of this review. Full-text retrieval was attempted for 119 articles, of which 7 were not available. Of the 112 full-text articles, 70 were excluded for the following reasons: not conducted in Libya or used non-Libyan subjects (n = 38), not CRC-focused (n = 24), not original research (n = 7), and a suspected text duplication (n = 1). Ultimately, 42 studies met the inclusion criteria and were retained for analysis. PRISMA-ScR Flow Diagram of Study Selection for Peer-Reviewed Publication on CRC Research in Libya
Characteristics of Sources of Evidence
Methodological Features of Included Studies
Summary of Study Designs, Settings, and Data Sources of CRC-Related Publications in Libya Included in this Scoping Review (n = 42)

Geographic and Institutional Distribution
Libyan peer-reviewed publications on CRC reveal an uneven geographic landscape, with marked clustering around a few urban centers in the north. Benghazi and nationwide analyses each accounted for 26.2% of the studies (n = 11), followed by 21.4% from Misrata (n = 9), 11.9% from Tripoli (n = 5), and smaller contributions from Tobruk (4.8%, n = 2), Derna, Sabha, Sabratha, and Zlitan, each with one study (2.4%). This distribution highlights persistent regional gaps, particularly in southern Libya, where minimal representation (only Sabha from the south) suggests the under-coverage of certain populations and care contexts.
The institutional affiliations of the first authors mirrored this imbalance. The University of Benghazi led with 8 studies (19%), followed by the National Cancer Institute–Misurata (16.7%, n = 7) and the Libyan International Medical University in Benghazi (7.1%, n = 3). Other contributing institutions included the University of Tripoli (9.5%, 4), University of Misurata (7.1%, 3), and several international collaborators, such as the University of Sharjah (UAE), Hamad General Hospital (Qatar), and institutions in Iran and Ethiopia. This mix of domestic and international affiliations reflects growing cross-border collaboration, although local academic centers remain the primary drivers of peer-reviewed publications on CRC research in Libya.
Thematic Focus and Population Characteristics
The 42 included studies addressed a range of topics in CRC research in Libya. The most frequently represented themes were epidemiology (35.7%, n = 15) and Clinical Characteristics & Diagnosis (33.3%, n = 14). Smaller subsets focused on Treatment and Outcomes (14.3%, n = 6), Risk Factors and Etiology (9.5%, n = 4), and Molecular and Genetic factors (7.1%, n = 3). This distribution reflects a strong emphasis on population-level patterns and clinical presentations, with fewer studies exploring the underlying biological mechanisms or intervention outcomes.
The sample sizes across the included studies ranged from single-patient case reports to a colonoscopy series involving 1858 individuals. Of the 36 studies that reported numerical data, 3 datasets were used twice. Specifically, Bodalal et al used the same sample in 2 publications10,19; Bensalah et al. did likewise20,21; and Alragig et al. and Rabie et al. reported on the same sample in separate studies.22,23 After accounting for these overlaps, the adjusted totals were as follows: data analysis records (n = 6070), human participants (n = 1259), and tissue samples (n = 216).
Most studies (92.9%, n = 39) included both male and female participants. Only 3 studies focused on a single sex: 2 case reports targeted one male each, and one case report targeted one female. The reporting of patient age varied across studies, with inconsistent formats and ranges, making standardized grouping unfeasible. However, most studies focused on adult populations that ranged from below 40 to over 90 years.
Summary of the Published 42 Studies on CRC in Libya and Included in this Scoping Review
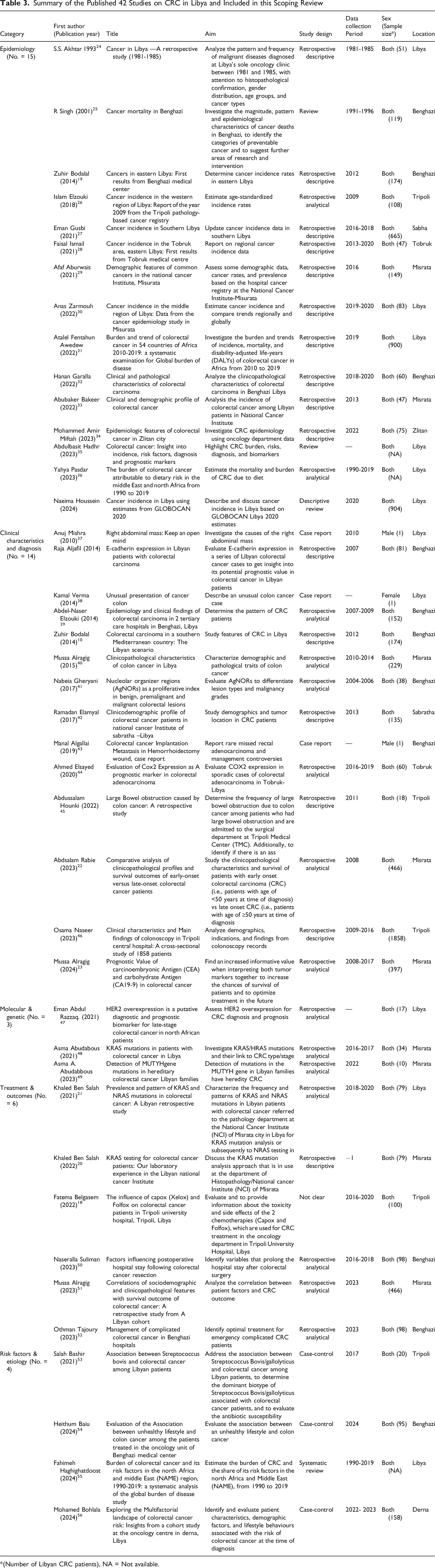
*(Number of Libyan CRC patients), NA = Not available.
Tumor Characteristics and Reporting Gaps
Reporting on tumor biology and staging varied considerably among the included studies. Histological subtype was unspecified in 71.4% of the included studies, while 9.5% identified adenocarcinoma and 19% reported multiple types.
Tumor location was described as “colorectal” without anatomical detail in 57.1% of studies; 19% included multiple locations, and only one study focused solely on rectal cancer. Notably, 21.4% of studies did not specify the tumor site.
Staging information was absent in 66.7% of studies. Among those that did report staging, 28.6% described mixed-stage populations and 4.8% focused on late-stage disease. Overall, inconsistencies and omissions in histological, locational, and staging data limit the potential for meaningful cross-study synthesis and comparative analysis.
Publication Trends and Research Capacity
CRC publication activity in Libya shows a steep rise in recent years. The peak year for publications was 2023 with 9 studies (21.4% of the total), closely followed by 2021 with 8 studies (19%), and 2022 with 6 studies (14.3%). In 2024, 5 publications (11.9%) were documented at the time of this review. International journals were the venue for 23 studies (54.8%), while 19 studies (45.2%) were published in local journals.
Of the 42 included studies, most were published in peer-reviewed journals that are not indexed or ranked in major citation databases. Specifically, 69% lacked an available impact factor, and 76.2% had no quartile ranking. Among the journals with reported metrics, impact factors ranged from 0.7 to 4.2, with most falling below 2.0. Quartile rankings were distributed across Q1 (4.8%), Q2 (7.1%), and Q3 (11.9%). Most journals claim to follow peer-review standards, although the rigor and consistency of review processes appear variable. In several cases, articles exhibited limitations in clarity, methodological rigor, or adherence to reporting standards. This distribution may influence the generalizability and methodological transparency of the included evidence.
Male first authors led the majority of studies (64.3%, n = 27), more than twice the proportion of studies led by female first authors (28.6%, n = 12). The gender of the first author could not be determined for 7.1% (n = 3) of the included publications. These 3 studies, published in 1993, 2001, and 2010, likely represent foreign research efforts, as Libyan-led first authorship only began in 2013 (n = 1 male) and 2014 (n = 1 female). This initial gap and subsequent emergence of Libyan leadership align with the major political shifts in the country, as significant foreign presence in Libya declined sharply after the 2011 revolution. Notably, 75% (9 of 12) of all female-led publications occurred in the last 4 years of the analysis (2021 to 2024), suggesting a recent acceleration in female lead authorship within the local research sphere.
Across all 42 studies, authorship was widely distributed, with 38 unique first authors contributing. Most authors (90%) appeared only once, reflecting a dispersed and episodic research landscape. Four individuals were listed as first authors on more than one publication: Mussa Alragig (n = 3; 2015, 2023, 2024), Zuhir Bodalal (n = 2; both in 2014), Khaled Ben Salah (n = 2; 2021, 2022), and Asma Abudabous (n = 2; 2021, 2023). Among these, Asma Abudabous is the only female repeat contributor. No author demonstrated consistent or consecutive annual contributions.
Of the 42 included studies, 22 (52.4%) explicitly reported a section on ethics or patient consent. Ethical reporting varied by study type: 9 out of 10 internationally collaborative studies (90%) included an ethics section, compared to only 13 out of 32 locally conducted studies (40.6%). Funding disclosure was similarly limited. Only 18 studies (42.9%) provided information about their funding sources. Among collaborative studies, 6 out of 10 (60%) included funding details, while just 12 of 32 local studies (37.5%) did so. The remaining 24 studies (57.1%) offered no funding information.
Discussion
This scoping review synthesized the evidence from 42 publications on CRC in Libya, revealing critical limitations in the current research landscape. The body of evidence, while growing, suffers from significant methodological homogeneity, profound regional disparities, and a narrow thematic focus. The majority of studies employed retrospective designs (73.8%) and relied heavily on hospital-based data (85.7%), underscoring a dependence on easily accessible institutional records and a deficit in primary, prospective data collection. Furthermore, the clinical utility and comparability of studies are severely hampered by major reporting gaps, notably the infrequency of detailed data on cancer histology and staging.
Geographically, research is concentrated in northern urban centers, particularly Benghazi, Misrata, and Tripoli, with a critical lack of representation from southern and peripheral regions. The thematic focus similarly remains restricted to Epidemiology and Clinical Characteristics, with limited exploration of treatment outcomes, molecular profiling, or risk factors necessary for precision oncology.
Despite a noticeable surge in publication volume (peaking in 2023), local research output struggles with visibility due to challenges in indexing and journal impact metrics. Compounding these limitations, analysis of authorship and reporting practices revealed structural issues: low research continuity among first authors and inconsistent ethical and funding disclosures.
These intrinsic limitations mirror and are likely exacerbated by systemic, region-wide barriers to research maturity in Libya and the Arab world. As documented in broader analyses, Libya has faced significant conflict-related disruptions, including fund diversion and brain drain, which undermine the development of a sustainable research infrastructure. 12 This environment reflects the limited geographic scope and the reliance on lower-intensity retrospective studies observed in our review. Arab universities also contend with a crisis of global recognition, struggling to prioritize and adequately fund research amidst social, economic, and political instability.13,57 Challenges such as inadequate infrastructure, limited resources for specialized training, and a shortage of well-indexed publications further restrict the global visibility and impact of Libyan science. These regional dynamics underscore the urgent need for targeted capacity-building efforts, inclusive mentorship structures, and policy reforms to enhance Libya’s contribution to peer-reviewed publications on CRC research and integrate it more effectively into global scientific discourse.
Methodology Patterns
Study Design and Setting: Current Trends and Contextual Barriers
The heavy methodological skew in peer-reviewed published CRC research in Libya is a direct reflection of reliance on readily available institutional records amid profound infrastructural, financial, and logistical constraints. While the use of secondary data enables cost-effective analysis in a resource-limited setting, it introduces an inherent epistemological bias. This methodology often excludes critical patient-reported outcomes, data on early symptomatology, and community-level risk behaviors, thereby limiting generalizability and limit the evidence needed for effective preventative strategies. 58
This situation is not unique to Libya but is common in other LMICs, where cancer research frequently adopts retrospective, single-center designs due to fragmented health information systems and a lack of formalized research strategies. 6 Parallels exist in sub-Saharan Africa, where studies face similar challenges in obtaining reliable staging data due to gaps in pathology and electronic records. 3 Such parallels underscore the need for system-level reforms that address both technical and sociocultural barriers to inclusive research.
A critical gap in Libyan CRC literature is the absence of community-based studies, likely driven by sociocultural norms and structural limitations. For instance, household-based data collection is often impractical due to safety concerns and cultural norms discouraging women from interacting with unfamiliar visitors.59,60 Resource constraints further hinder feasibility, as community-based research demands transportation, data collection tools, flexible scheduling, and participant incentives, resources typically unavailable to students and trainees lacking institutional support.
Nonetheless, Libya’s shifting social landscape offers new opportunities for culturally sensitive research. Public venues such as malls, gyms, and clubs provide safer, more accessible settings for participant recruitment and data collection. While these alternatives may reduce cultural barriers, scaling community-based designs remains challenged by persistent funding limitations.
Thematic Gaps
Geographic and Institutional Distribution: Bridging Regional Gaps and Expanding Research Collaboration
Peer-reviewed publication on CRC research in Libya is overwhelmingly concentrated in major urban centers, a trend clearly evidenced by first-author affiliations: Benghazi, Misurata, and Tripoli collectively account for over 76% of all research output. This extreme clustering, coupled with minimal contribution from peripheral areas, particularly southern Libya, creates a critical research gap that obscures regional epidemiological patterns, population-specific risk factors, and disparities in care delivery. This imbalance is driven by structural challenges, including the sparse distribution of academic institutions, limited healthcare infrastructure, and the centralization of the country’s few dedicated cancers care facilities. 61 This centralization fragments national CRC surveillance and undermines the relevance and equity of resulting control strategies.
While international collaborations represent an emerging avenue of engagement (11.8% of affiliations), the urgent need is to transition research efforts beyond isolated institutional contributions and individual partnerships. To advance equitable and comprehensive cancer control, formal, large-scale initiatives are mandatory. These strategies include the activation of a comprehensive national cancer registry, the establishment of centralized data sharing platforms, and formal academic twinning programs. These initiatives are essential for integrating fragmented data, building sustainable research capacity across all regions, and ensuring that future research is inclusive of the currently underrepresented populations in the south.
Thematic Focus and Population Characteristics: Gaps in Scope and Representation
The current thematic focus of peer-reviewed publications on CRC research in Libya demonstrates an overreliance on descriptive epidemiology, with insufficient investigation into molecular and genetic markers, modifiable risk factors, and treatment outcomes. The limited studies on genetic predispositions and environmental contributors hinder the development of context-specific prevention strategies. Additionally, the limited data on treatment outcomes restricts the formulation of localized clinical guidelines and effective resource allocation.
Compounding these issues is the underrepresentation of rural and underserved populations in hospital-based data, which predominantly reflects urban centers. These biases risk misinterpreting disease burden and may lead to policies that neglect high-risk or underdiagnosed groups. Consequently, clinicians and policymakers face challenges in tailoring interventions to local needs.
These limitations also restrict the ability to trace etiological patterns or assess care effectiveness. Such gaps, biases, and thematic imbalances have been observed across other LMIC, where peer-reviewed publication on CRC research often prioritizes facility-based data due to resource constraints and limited molecular infrastructure. A recent review of CRC screening interventions in LMICs revealed that most studies were opportunistic and clinic-based, with minimal population-level outreach or genomic profiling. These findings underscore the need for systemic investment, inclusive sampling strategies, and a broader research scope. 3
Tumor Characteristics and Reporting Gaps: Implications for Surveillance and Clinical Strategy
A significant limitation in Libyan peer-reviewed publications on CRC is the inconsistent and often absent reporting of critical tumor characteristics, particularly histological subtypes, anatomical tumor locations, and staging information. The prevalent use of vague descriptors (e.g., “colorectal” without site specificity) and the limited data on cancer staging hinder the understanding of disease progression and clinical behavior within the Libyan population.
This lack of detail obstructs both national and international comparative analyses, complicating the exploration of geographic and demographic variations in tumor patterns. Most critically, it impairs the development of stage-specific treatment strategies and early detection programs. In a healthcare landscape characterized by centralized oncology services, geographic disparities in access, and the absence of a national screening program, these reporting gaps become increasingly consequential. Without robust early detection infrastructure and widespread educational initiatives, patients are more likely to be diagnosed at advanced stages, yet the research framework remains ill-equipped to systematically capture or analyze this trend. As a result, public health planning and clinical decision-making are hampered by an incomplete understanding of disease burden and progression.
These challenges are common in other LMICs, where tumor staging and histological reporting are frequently underdeveloped due to limited pathology infrastructure, fragmented data systems, and inconsistent adoption of international classification standards. A recent study from the Philippines, for instance, revealed that over half of hospital-based cancer registries lacked staging data, particularly in treatment and follow-up modules. 62 These parallels emphasize the urgent need for systemic reforms that prioritize data completeness and clinical relevance.
Structural Barriers
Publication Trends and Research Capacity: Barriers, Equity, and Systemic Reform
The analysis of publication trends reveals a landscape characterized by dispersed authorship and minimal sustained contributions across consecutive years, suggesting a fragmented or nascent research community. While a few individuals contributed multiple times as first authors, the absence of consistent leadership or mentorship lineages points to challenges in building enduring research programs. Fluctuations in annual publication activity further reflect an inconsistent rhythm of research output.
The emergence of female authorship between 2014 and 2024, with dispersed authorship, highlights both progress in gender inclusion and the difficulty of sustaining diversity. This pattern mirrors global trends, where female authorship in oncology journals has increased modestly but remains underrepresented in senior roles. 63 Promoting equitable participation is essential to harness the full intellectual capital available in Libya.
Libyan authorship conventions differ from international norms, with the first author typically regarded as the most senior and responsible for the research rather than the last author. Accordingly, this analysis focused on first authorship.
Inconsistent reporting of ethical approval and funding across studies raises fundamental concerns regarding transparency and research oversight. Of the included studies, 47.6% did not report ethical approval, a gap primarily attributed to contextual factors within the local research environment. In some cases, research may proceed without mandatory, centralized institutional review, and local journal submission guidelines often do not explicitly require ethical declarations. This omission, particularly pronounced in locally conducted studies, suggests a research culture where transparency is not routinely enforced, potentially undermining trust and limiting reproducibility. Several of these studies were published in journals lacking formal indexing, impact metrics, or consistent ethical reporting. While such features may raise concerns about editorial rigor, they do not in themselves confirm predatory publishing. This pattern suggests that collaborative or internationally affiliated research may adhere more consistently to formal ethical reporting standards. Conversely, the absence of ethical documentation in over half of the locally conducted studies highlights a potential gap in research governance and transparency within the local research landscape. This disparity is not unique to Libya; similar patterns have been documented across LMICs, where ethical and financial reporting often lags due to limited infrastructure and inconsistent journal requirements.64,65 Further assessment of journal practices and transparency is warranted.
The publication landscape reveals a trend towards dissemination in lower-visibility or unranked journals. Many of these journals lack impact metrics or quartile rankings, making their reach and influence harder to gauge. A significant hurdle contributing to this trend is the high cost of publishing in high-impact journals. For instance, the median cost for publishing an open-access (OA) article in a medical journal is about $4600, with fees ranging widely from $2000 to $12,000.14,66
Although some journals qualify Libya for partial APC waivers as an upper-middle-income country, the lack of institutional coverage and the devaluation of the local currency render these fees prohibitive. This financial constraint disproportionately affects early-career researchers and those without external funding.
Moreover, the primary motivation for research in this setting is often tied to academic promotion, rather than broader scientific contribution or policy impact. As a result, researchers may opt for more accessible journals that, despite claiming peer-review status, may lack rigorous editorial standards. This includes the absence of ethical approval declarations, conflict of interest disclosures, and transparent peer-review processes, practices routinely enforced by higher-tier journals.
The consequence is a self-reinforcing cycle: publishing in lower-tier venues limits peer critique, reduces methodological refinement, and diminishes global visibility. This weakens the credibility of Libyan research and hinders its integration into international discourse. In the long term, this cycle undermines both academic development and institutional capacity to conduct impactful, policy-relevant research.
Recommendations and Future Directions
Methodological Patterns
This section presents recommendations focused on improving the quality, rigor, and diversity of research designs employed in CRC studies.
To address the limitations in study design, regional coverage, and thematic focus, future research efforts should adopt more robust and inclusive methodologies. Adopt Prospective and Mixed-Methods Designs: Future studies should move beyond retrospective designs to incorporate prospective and mixed-methods approaches. This will allow for richer data collection, including patient-reported outcomes and longitudinal follow-up on disease progression, which are crucial for understanding the patient journey and informing long-term care strategies. Broaden Research Scope: Research should expand beyond descriptive epidemiology to investigate critical areas like lifestyle factors, environmental exposures, and genetic markers. This will provide a more comprehensive understanding of CRC risk factors and facilitate the development of tailored prevention and screening strategies. Conduct Community-Based Studies: Innovative and culturally sensitive recruitment strategies, such as using public venues or mobile screening units, are necessary to include rural and underrepresented populations. This approach will improve the external validity and equity of findings and ensure that policy recommendations are relevant to all Libyan communities. Standardize Data Collection: National guidelines for tumor reporting should be developed and adopted to mandate the consistent collection of essential data, including histological subtypes, anatomical location, and staging. Aligning these standards with international frameworks like TNM staging will improve data comparability, research quality, and global integration.
Thematic Gaps
This section summarizes the key contributions of this review to the literature on CRC research in resource-limited settings. Addressing Structural Barriers to Inclusive Research: The review highlights how cultural norms, logistical challenges, and resource constraints in Libya have hindered the adoption of community-based and prospective research designs. These insights underscore the need for innovative, context-sensitive approaches to engage broader populations and overcome structural barriers common in LMICs. Strengthening the Research Ecosystem: The analysis of publication trends, ethical oversight, and funding disclosure reveals systemic gaps that are often pervasive in LMIC research environments. The recommendations to develop national funding mechanisms, subsidize high-impact publishing, and establish centralized monitoring systems aim to strengthen the overall integrity and visibility of Libyan CRC research, aligning with global efforts to enhance research capacity in resource-limited settings. Emphasizing Tumor Profiling and Data Standardization: The review’s focus on the critical gaps in tumor characteristics reporting underscores a common challenge in LMIC cancer research, where fragmented data systems and limited pathology infrastructure constrain the quality and comparability of evidence. The proposed strategies to standardize reporting protocols, build pathology capacity, and create centralized registries are broadly applicable to strengthen cancer surveillance and research in other LMIC contexts. Fostering Equitable and Sustainable Research Collaborations: The review’s recommendations to promote gender equity, establish long-term mentorship programs, and facilitate international partnerships respond to the need for more inclusive and enduring research ecosystems in LMIC settings. These approaches can help overcome the fragmentation and lack of institutional capacity that often hinder the development of impactful, policy-relevant cancer research in resource-constrained environments.
Structural Barriers
Strengthening Infrastructure and Collaboration
To build a more resilient and integrated research ecosystem, systemic investments in infrastructure and collaboration are essential.
Enhancing Publication and Research Integrity
To improve the visibility and credibility of Libyan research, reforms are needed to enhance publication standards, ethical practices, and international engagement.
Limitations and Scope of Findings
The findings and conclusions of this analysis are strictly limited to peer-reviewed articles published on CRC research in Libya. This study examines research output and publication practices, not the totality of all research conducted within Libya on this topic. As the activities of research and their subsequent publication are distinct processes, the identified gaps reflect limitations only within the current body of peer-reviewed literature and should not be generalized to represent the entire scope of all research activities undertaken in the country. Methodologically, this scoping review was constrained by limited access to certain subscription-based databases, which may have led to an incomplete mapping of available evidence. Furthermore, the lack of direct author engagement prevented the inclusion of unpublished or supplementary data, and despite a rigorous internal revision to exclude known repeated samples of tissue or subjects, the potential for residual overlap in reported cases cannot be guaranteed as fully resolved, which introduces uncertainty regarding the distinctiveness of study populations.
Strengths of the Scoping Review
Despite these limitations, the review employed a robust, multi-pronged search strategy and adhered strictly to PRISMA-ScR guidelines, ensuring methodological transparency and reproducibility. The interdisciplinary composition of the review team minimized bias and enhanced data extraction quality. Moreover, the study’s targeted focus on the Libyan context offers valuable, localized insights into peer-reviewed publications on CRC research within an LMIC setting.
Conclusion
In summary, the Libyan peer-reviewed publication on CRC research landscape remains in a developmental phase, characterized by methodological heterogeneity, concentrated geographic activity, and limited structural support. Despite sociopolitical challenges, including prolonged conflict, the current evidence does not suggest a significant disruption in peer-reviewed publication on CRC capacity, given the low output observed before 2011. However, persistent barriers, such as underreporting of tumor characteristics, inconsistent ethical oversight, and limited access to high-impact publishing, continue to hinder the visibility and utility of local research. Encouragingly, Libya’s evolving social dynamics offer new opportunities for ethical and culturally grounded research, particularly through alternative recruitment venues like malls and gyms. Future efforts should prioritize the adoption of mixed-methods and community-based designs, the establishment of research consortia, and the development of national funding and ethics frameworks. By embracing these strategies, Libya can cultivate a more representative and impactful peer-reviewed publication on CRC research, one capable of guiding evidence-informed policies and improving cancer outcomes across diverse population groups.
Footnotes
Acknowledgments
The authors express their sincere gratitude to Ms. Asma ElKawafi and Dr Abdelwahab Kawafi for their valuable support in proofreading the manuscript to ensure clarity and consistency throughout.
Ethical Consideration
Ethical approval was not required for this scoping review, as it involved the analysis of publicly available literature and did not include human participants, personal data, or biological samples.
Funding
The authors received no financial support for the conduct of this scoping review.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data Availability Statement
All relevant data are presented within the manuscript. Additional information is available from the corresponding author upon reasonable request.