
Abstract
Background
Colorectal cancer (CRC) predominantly affects older adults, whose treatment outcomes may be influenced by baseline health-related quality of life (HRQoL). This study aimed to identify predictors of poor preoperative HRQoL in older patients undergoing CRC surgery and to stratify them into risk groups.
Methods
We retrospectively analyzed data on patients aged ≥65 years who underwent radical CRC surgery at a single medical center in Taiwan (2016-2018). Preoperative HRQoL was assessed using the EORTC QLQ-ELD14 questionnaire and a comprehensive geriatric assessment. Patients were stratified into high or low HRQoL groups based on the median QLQ-ELD14 sum score. Logistic regression identified independent predictors of poor HRQoL, and recursive partitioning analysis (RPA) was applied for risk stratification.
Results
Among the 179 patients, the most distressing HRQoL domains were Burden of Disease, Maintaining Purpose, and Worries about Others. Independent predictors of poor HRQoL included female sex (adjusted odds ratio [OR] = 2.41, P = 0.029), frailty (adjusted OR = 1.53, P = 0.042), poor Eastern Cooperative Oncology Group (ECOG) performance status (adjusted OR = 2.19, P = 0.008), and lower educational attainment (adjusted OR = 0.23, P = 0.019). RPA identified five patient subgroups with distinct risk levels; frail female had the highest risk (71.4%), while fit patients with college education or higher had the lowest (9.5%).
Conclusion
Frailty, functional status, sex, and education level are key determinants of preoperative HRQoL in older patients with CRC. The RPA provides a simple tool to identify high-risk patients, allowing targeted preoperative interventions to optimize care and enhance surgical outcomes.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy and the second leading cause of cancer-related mortality worldwide. 1 Its incidence increases markedly with age, with approximately 60% of cases occurring in individuals aged ≥65 years.2,3 Older patients with CRC often face compounded challenges because of age-related physiological decline, comorbidities, and frailty, all of which can influence treatment decisions and outcomes. 4 Radical surgical resection remains the cornerstone of curative CRC treatment. However, elderly patients are at higher risks of postoperative complications, prolonged recovery, and diminished functional independence.5-7
Health-related quality of life (HRQoL) integrates physical, functional, psychological, and social well-being and is increasingly recognized as clinically actionable in CRC, particularly among older adults who face age-related vulnerabilities. 8 In CRC surgery, lower preoperative HRQoL has been associated with higher risks of postoperative complications, prolonged length of stay, delayed functional recovery, and worse long-term outcomes, while better baseline HRQoL predicts enhanced recovery and survivorship.9-13 Nevertheless, determinants of poor preoperative HRQoL in older CRC patients remain incompletely characterized, and few studies have combined a geriatric lens with CRC-specific surgical pathways to identify who is most at risk before the operation.14-20
To address this gap, we evaluated preoperative HRQoL using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Elderly Cancer Patients Module (EORTC QLQ-ELD14), 21 an elderly-specific, validated instrument, and integrated a comprehensive geriatric assessment (CGA). Our aims were to (1) identify independent predictors of poor preoperative HRQoL among older adults scheduled for radical CRC surgery and (2) develop a simple, clinically interpretable risk stratification using recursive partitioning analysis (RPA) 22 to pinpoint high-risk subgroups who may benefit from targeted prehabilitation and supportive care.
Materials and Methods
Patient Selection
This was a retrospective cohort study conducted at a single tertiary medical center in Taiwan. The reporting of this study conforms to the STROBE guidelines for cohort studies. 23 Eligible patients were consecutively enrolled between 2016 and 2018. All patient details were de-identified prior to analysis. Eligible patients were aged ≥65 years with histologically confirmed colon or rectal adenocarcinoma scheduled for elective, radical resection. We excluded patients who (i) received neoadjuvant chemotherapy and/or radiotherapy, (ii) underwent emergency or palliative procedures, or (iii) were unable or unwilling to provide informed consent. Consecutive eligible patients were approached during the pre-operative clinic visit; all participants provided written informed consent. The Institutional Review Board of Chang Gung Memorial Hospital approved the study (IRB No. 201600916B0).
Data Collection
The patient demographics included age (continuous and categorized by median), sex (male/female), education level (<high school, high school graduate, ≥college), employment (yes/no), smoking and drinking history (current vs not), marital status (married vs other), primary caregiver (spouse vs other), and Eastern Cooperative Oncology Group (ECOG) performance status (0, 1, 2). Tumor characteristics included primary tumor location (colon/rectum), American Joint Committee on Cancer (AJCC) stage (I–IVa), and histological grade (well, moderately, poorly).
Assessment Tools
A trained nurse-research assistant administered all instruments in Mandarin within 7 days prior to surgery during a face-to-face encounter. Standardized scripts were used. When needed, items were read aloud and clarified without interpretation.
The QLQ-ELD14 comprises 14 items across seven domains (Mobility, Family Support, Joint Stiffness, Burden of Disease, Maintaining Purpose, Worries for the Future, Worries about Others). 21 Items use a 4-point Likert scale (“not at all” to “very much”) and were scored per the EORTC manual: raw scores were linearly transformed to 0-100. For the QLQ-ELD14, higher scores in symptom-related domains (eg, Burden of Disease, Worries about Others) reflect greater impairment and poorer HRQoL, whereas higher scores in functional domains (eg, Mobility, Family Support) reflect better function and thus better HRQoL. The total sum score was calculated by summing all 14 transformed items, with higher values indicating poorer overall HRQoL. Poor preoperative HRQoL was defined as a total sum score above the cohort median of 125 (range: 0-489). In the absence of established universal cut-offs for the QLQ-ELD14, we used the cohort median as a pragmatic threshold, consistent with prior HRQoL research in elderly cancer populations.24,25 This approach balances group sizes for multivariable regression and recursive partitioning analysis, facilitating clinically meaningful risk stratification.
The CGA covered eight dimensions: function (Activities of Daily Living [ADL] <100 or Instrumental Activities of Daily Living [IADL] ≤7), comorbidity (Charlson Comorbidity Index ≥2), polypharmacy (≥5 regular medications), falls (≥2 fall in prior 6 months), mood (4-item Geriatric Depression Scale [GDS-4] ≥2), cognition (Mini-Mental State Examination [MMSE] ≤23), nutrition (Mini Nutritional Assessment-Short Form [MNA-SF] ≤11), and social support (living alone, yes or no). 26 Frailty was defined as impairment in ≥2 CGA domains, which is consistent with previous geriatric oncology studies, 26 though consensus definitions in elderly CRC remain debated (Supplemental Table 1 details cutoffs/tools).
Statistical Analysis
Continuous variables are presented as median (range) or mean (SD) as appropriate; categorical variables as counts (%). Group comparisons of the QLQ-ELD14 sum score used two-sided t-tests (or Welch’s t-test when variances were unequal). For the primary outcome (poor vs better HRQoL), we fitted logistic regression. Variables with P < 0.10 in univariate analyses entered the multivariable model; we report odds ratios (ORs) with 95% CIs. Collinearity was assessed via variance inflation factors (all <2). Missing data were minimal (<5% per variable) and were incorporated into the analyses using complete-case analysis. Thus, all results presented throughout the manuscript reflect this approach rather than a separate sensitivity analysis.
Prespecified candidate predictors included: age (continuous and dichotomized at the cohort median), sex, marital status, education (<high school, high school, ≥college), employment (yes/no), primary caregiver (spouse vs other), smoking/drinking (current vs not), ECOG PS (0 vs 1-2), tumor site (colon vs rectum), AJCC stage (I–IVa), tumor grade (well/moderate/poor), and CGA frailty status. These variables were used in univariate logistic regression, multivariable models, and recursive partitioning analysis (RPA). 22 RPA used a classification tree with the Gini index; split candidacy required P < 0.05 by chi-square, minimum node size n = 20, and maximum tree depth of 4. These values represent default parameters commonly recommended to reduce overfitting in smaller datasets. 22 We then estimated ORs of poor HRQoL across terminal nodes using univariate logistic regression. Analyses were performed in IBM SPSS Statistics v23 (IBM Corp., Armonk, NY, USA). Two-sided P < 0.05 denoted statistical significance.
Results
Patient Characteristics
Patient Characteristics

AJCC, American Joint Committee on Cancer; ECOG, Eastern Cooperative Oncology Group.
aAge is presented as median (range). n (%) does not apply to this row.
The tumors were primarily located in the colon (74.9%) and rectum (25.1%). Most tumors were stage II (28.5%) or III (32.4%), with fewer tumors in stages I (25.1%) and IV (14.0%). Regarding differentiation, 72.1% were moderately differentiated, 19.0% were well differentiated, and 8.9% were poorly differentiated.
HRQoL Domains Measured by the QLQ-ELD14
The mean scores for the HRQoL domains assessed using the QLQ-ELD14 questionnaire are shown in Figure 1. The Burden of Disease domain had the highest mean score, followed by Maintaining Purpose, Worries about Others, and Worries for the Future. In contrast, Joint Stiffness and Mobility had lower mean scores, whereas Family Support had the lowest score among all assessed domains. Mean Scores for Each HRQoL Domain From the QLQ-ELD14 Questionnaire. HRQoL, Health-Related Quality of Life; QLQ-ELD14, Quality of Life Questionnaire – Elderly Module (14 Items)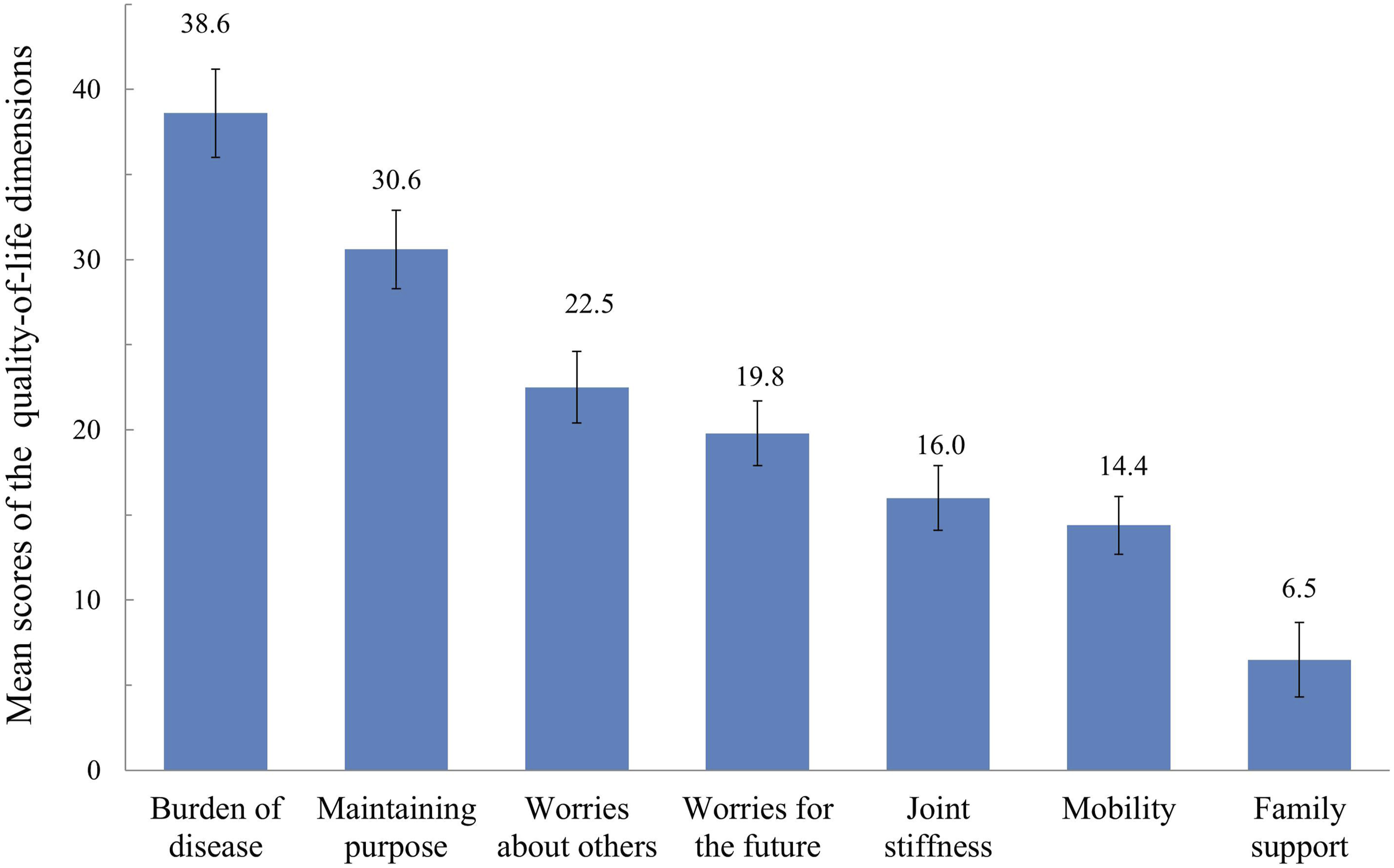
Patients were stratified into high or low HRQoL groups based on whether their sum scores were above or below the cohort median of 125 (range: 0-489). Those above this cut-off were categorized as having “poor HRQoL,” while those at or below were classified as having “better HRQoL.”
Univariate and Multivariable Analysis of Predictor Factor for HRQoL
Univariate and Multivariable for Health-Related Quality of Life

OR, odds ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer.
aBetter HRQoL = QLQ-ELD14 sum score ≤125; Poorer HRQoL = sum score >125.
Recursive Partitioning Analysis
The RPA results are illustrated in Figure 2. Patients were categorized into five groups, ranging from the lowest to the highest possibility of poor HRQoL. Patients who were fit and had a college or higher degree of education had the lowest ratios of poor HRQoL (9.5%, categorized as the reference). In contrast, frail and female patients had the highest ratio of poor HRQoL (71.4%). Poor HRQoL differed significantly between patients in the reference classification and those in classifications 2-5, with odds ratios ranging from 6.11 to 23.8 (Supplemental Table 2). Recursive Partitioning Analysis of Total Study Participants (n = 179). The Classification Mode, which is Used for Univariate Logistic Regression Analysis in Supplemental Table 2, is Presented as the Number Below the Node of the Decision Tree
Analysis of HRQoL Domains by Key Predictors
Figure 3 illustrates the mean scores for the various HRQoL domains stratified by frailty status, ECOG performance status, sex, and educational level. Frail individuals exhibited significantly poorer scores in Joint Stiffness, Mobility, Worries for the Future, Maintaining Purpose, and Burden of Disease than their fit counterparts. Similarly, patients with worse ECOG performance status reported notably lower scores for Mobility, Joint Stiffness, Worries for the Future, and Maintaining Purpose. Although female participants generally showed higher scores across multiple domains, only Mobility showed a statistically significant difference. Additionally, individuals with lower educational attainment reported significantly greater Joint Stiffness, Worries for the Future, Maintaining Purpose, and a higher perceived Burden of Disease than those with a college degree or higher. Mean Scores for Each HRQoL Domain From the QLQ-ELD14 Stratified by Frailty Status (A), ECOG Performance Status (B), Sex (C), and Education Level (D). HRQoL, Health-Related Quality of Life; QLQ-ELD14, Quality of Life Questionnaire – Elderly Module (14 Items); ECOG, Eastern Cooperative Oncology Group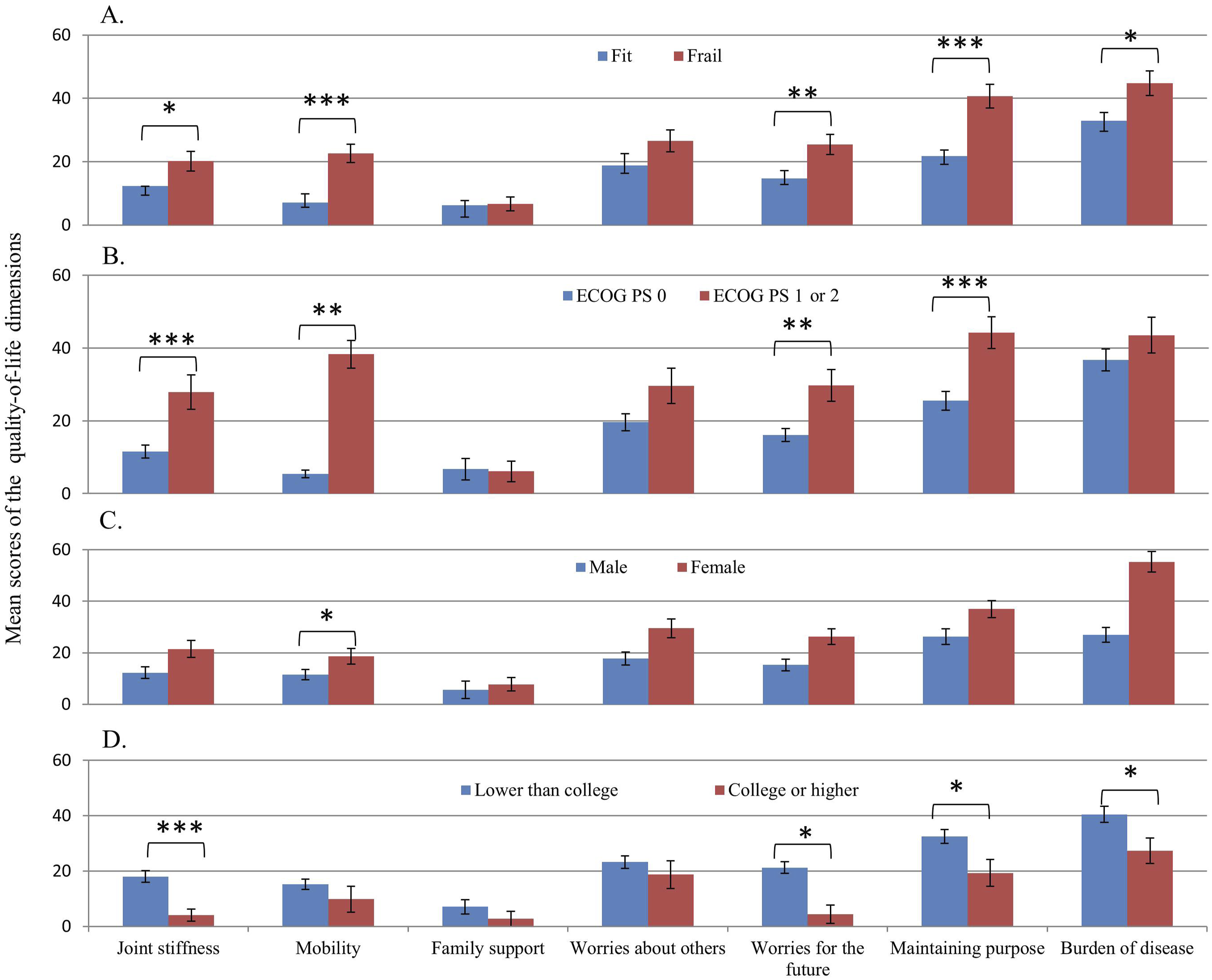
Effect of CGA Dimensions on QLQ-ELD14 Sum Score
Effect of Each Frailty Dimension on EORTC-ELD14 QLQ Total Score (n = 179)

SE, standard error; EORTC-ELD14 QLQ, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Elderly Cancer Patients Module (14 items).
Discussion
This study investigated preoperative HRQoL in older patients with CRC using the QLQ-ELD14 questionnaire and examined its association with clinical and demographic factors. The findings revealed that frailty, poor ECOG performance, female sex, and low educational attainment were independently associated with poor HRQoL. The analysis of HRQoL domains showed the highest distress for Burden of disease, Maintaining purpose, and Worries about others, while Family support and Mobility were the least distressing domains. Patients with frailty and poor ECOG performance experienced significantly greater limitations in Mobility, increased Worries about the future, and difficulty Maintaining purpose in life. In contrast, tumor-related factors, such as tumor staging and differentiation, did not significantly affect HRQoL. This lack of association between tumor stage/grade and preoperative HRQoL contrasts with prior reports linking advanced disease to lower HRQoL. Several factors may account for this finding. First, our assessments were performed during the preoperative period, before patients experienced postoperative complications or systemic treatment side effects, which may attenuate the impact of disease stage on perceived HRQoL. Second, older adults may exhibit a degree of psychological adaptation or resilience, focusing more on maintaining daily function and social support rather than on tumor characteristics. Third, the relatively high proportion of patients with good performance status (ECOG 0-1, 89.4% of participants) in our cohort may have buffered stage-related differences. Future longitudinal research is needed to evaluate how tumor burden and treatment course influence HRQoL trajectories over time.
The use of the RPA in this study enabled the identification of distinct subgroups of older patients with CRC at varying risk levels of poor preoperative HRQoL. By incorporating significant predictors (frailty, sex, ECOG performance status, and educational level), the RPA allowed for the stratification of patients into five hierarchical classifications with clearly differentiated probabilities of poor HRQoL. Notably, the subgroup comprising frail female patients had the highest risk (71.4%), whereas fit patients with college or higher education had the lowest risk (9.5%). This risk-based stratification provides a framework for clinicians to preoperatively identify vulnerable patients with poor HRQoL. Moreover, the intuitive decision-tree structure of the RPA enhances its applicability in routine clinical settings, supporting shared decision-making and facilitating the targeted allocation of supportive care resources to improve surgical preparedness and patient-centered outcomes. Nonetheless, the RPA model presented here should be regarded as a proof-of-concept tool. While its intuitive structure and ease of use make it promising for clinical decision-making, it requires further validation. Prospective studies in larger, multi-center cohorts are warranted to confirm its predictive utility and to determine whether incorporating this stratification into preoperative care pathways can improve patient outcomes in routine practice.
Our data showed that Burden of disease, Maintaining purpose, and Worries about others were the most distressing HRQoL domains among older Taiwanese patients with CRC. The high Burden of disease score suggests that patients perceived that cancer has a significant impact on their daily lives, including functional limitations, physical discomfort, and the psychological toll of managing their condition.27,28 This aligns with previous studies showing that older patients with cancer often struggle with the uncertainty of disease progression, treatment complications, and the potential loss of independence. 29 Maintaining purpose emerged as another major challenge, indicating that older patients with CRC may feel a sense of reduced self-worth or a diminished role in society because of their diagnosis and treatment. Psychological factors such as depression, anxiety, and the fear of becoming a burden on caregivers likely contribute to this distress. 30 Worries about others also scored high, suggesting that patients were deeply concerned about how their illnesses would affect family members and caregivers. 31 Many older patients prioritize the well-being of their loved ones and may experience emotional strain over concerns about caregiving burden and financial stress.
In contrast, Family support and Mobility were the least distressing HRQoL domains. The low distress score for Family support may indicate that most patients in our study had sufficient social support, particularly given that a large proportion of them were married and had caregivers. 32 Additionally, family support is generally strong in Asian populations, which may also contribute to this finding. 33 The relatively low distress in Mobility likely reflects the relatively preserved functional status in our study population, with most patients having an ECOG score of 0-1. This suggests that the patients included in this study retained a good level of functional mobility before their scheduled radical surgery.
In this study, frailty, ECOG performance status, sex, and education level were independent variables associated with poor HRQoL, consistent with previous findings.24,25,32-39 Frailty is significantly associated with worse HRQoL, reinforcing its role as a critical predictor of postoperative outcomes and overall well-being in elderly patients.24,25 Poor ECOG performance status was also associated with worse HRQoL in the present study, supporting prior evidence of the close association between declining physical function and psychological distress and decreased independence in patients with cancer. 34 The sex differences in HRQoL are notable, with female patients reporting significantly worse HRQoL.35,36 This finding is consistent with previous research suggesting that women with CRC often report higher levels of anxiety, fatigue, and emotional distress than men. 36 The possible explanations for these differences include greater psychological sensitivity to illness, differences in coping mechanisms, and hormonal influences on mood regulation. 37
Additionally, education level emerged as a protective factor in this study, with patients who had a college degree reporting significantly better HRQoL than those with lower educational attainment. This finding is consistent with existing literature, suggesting that higher education is associated with better health literacy, stronger coping strategies, and greater access to healthcare resources, all of which contribute to improved HRQoL outcomes in patients with cancer.38,39
Our study results showed that frail patients experienced significantly greater impairment in mobility, increased psychological distress, and higher disease burden. The multidimensional nature of frailty, encompassing functional, cognitive, nutritional, and psychological domains, suggests that interventions aimed at improving HRQoL should adopt a comprehensive geriatric approach. 40 As nutritional deficiencies, functional impairment, and mood disorders were the most significant factors affecting HRQoL in this study, targeted interventions addressing these aspects may yield the greatest benefit in improving patient well-being. 41 Strategies such as prehabilitation programs, nutritional support, psychological counseling, and physical therapy may help mitigate the negative impact of frailty on HRQoL in older patients with CRC. 42
The strengths of this study include its prospective design and retrospective data analysis, which allowed for a comprehensive evaluation of preoperative HRQoL in older patients with CRC. The QLQ-ELD14, a validated tool specifically designed for older patients with cancer, provides a nuanced assessment of HRQoL, addressing aspects that are often overlooked in standard HRQoL instruments. Additionally, including CGA allowed for a multidimensional evaluation of frailty and its impact on HRQoL, strengthening the clinical relevance of the findings.
However, this study has several limitations, including the inherent risk of bias due to missing or incomplete medical records in retrospective data. Second, while this study included a wide range of clinical and demographic variables, the observational nature limited our ability to draw causal conclusions. Third, while the QLQ-ELD14 is widely used to assess quality of life in older populations, 21 it lacks a dedicated measure of overall quality of life. While this study used a summative score derived from 14 questionnaire items to represent the overall quality of life, the suitability of this approach remains uncertain. Finally, HRQoL was assessed at a single time point, which may not capture the full range of changes in QoL throughout treatment and recovery. 43 Furthermore, the generalizability of our findings may be limited by the use of a Taiwanese cohort, where cultural norms and typically strong family support structures could influence certain HRQoL domains, such as “Worries About Others.” Caution is therefore warranted when extrapolating these results to populations with different sociocultural contexts. In addition, our definition of frailty—impairment in ≥2 CGA domains—aligns with prior geriatric oncology studies,24,25 but consensus on standardized frailty thresholds for elderly CRC patients remains lacking. Future research should aim to validate and harmonize frailty criteria to optimize risk stratification across diverse settings.
Our study results revealed the significant influences of frailty, functional status, sex, and educational level on preoperative HRQoL in older patients undergoing CRC surgery. Using the QLQ-ELD14 instrument, we found that the most distressing domains were related to Burden of disease, Maintaining purpose, and Worries about others, emphasizing the psychological and social challenges faced by this population. Importantly, the application of RPA enabled effective risk stratification to identify subgroups of patients, particularly frail females, with the highest risk of poor HRQoL.
These findings support the integration of multidimensional preoperative assessments, including geriatric and HRQoL evaluations, into routine surgical planning for older patients with CRC. Recognizing patients at greatest risk allows for targeted, personalized interventions—such as prehabilitation, nutritional support, and psychosocial care—that may improve both quality of life and surgical outcomes. Future research should focus on validating these risk profiles in diverse populations and exploring intervention strategies that can meaningfully enhance the preoperative experience and postoperative recovery in this vulnerable group.
Supplemental Material
Supplemental material - Predictors of Preoperative Quality of Life in Older Patients With Colorectal Cancer in Taiwan: A Retrospective Cohort Study
Supplemental material for Predictors of Preoperative Quality of Life in Older Patients With Colorectal Cancer in Taiwan: A Retrospective Cohort Study by Cheng-Chou Lai, MD, Shih-Ying Chen, RN, Shu-Huan Huang, MD, Chun-Kai Liao, MD, Hao-Wei Kou, MD, Yi-Fu Chen, MD, Yu-Shin Hung, MD, Wen-Chi Chou, MD, PhD in Cancer Control
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance of the patients who participated in this study.
Ethical Considerations
The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Taiwan (IRB No. 201600916B0). The approval date was Aug, 08, 2016. This IRB approval covers a prospective institutional project (2016-2020) designed to enroll cancer patients receiving frailty assessment before the initiation of antitumor treatment. The current study represents a secondary analysis of that project, focusing on the impact of frailty on health-related quality of life in patients with colorectal cancer undergoing surgery. All participants provided written informed consent.
Author Contributions
Conception and design of study: CCL, SYC, SHH, CKL, HWK, YFC, YSH, WCC; Acquisition of data: CCL, SHH, CKL, YSH, WCC; Analysis and interpretation of data: CCL, SYC, SHH, CKL, YSH, WCC; Drafting of the manuscript: CCL, YSC, SHH, CKL, HWK, YFC, YSH, WCC.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chang Gung Memorial Foundation (CMRPG3L1611 and CORPG3N0151); Taiwan Ministry of Health and Welfare (MOHW112-TDU-B-222-124011); and Taiwan National Science and Technology Council (NSTC 111-2314-B-182A-162, NSTC 112-2314-B-182A-152, and NSTC 113-2314-B-182A-147).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Author WCC is a Section Editor of Cancer Control but did not participate in the editorial handling or peer review process of the article.
Data Availability Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.