
Abstract
Introduction
Patients with cancer may overestimate their ability to adhere to oral anticancer treatments (OAT) which may significantly reduce adherence rates. However, only few studies have investigated the specific role of personality traits and cognitive distortions in the definition of the adherence trajectory in the cancer field.
Methods
This study is nested in the Pfizer project (65080791), and it is a secondary, observational analysis of prospectively collected data from a randomized controlled trial (RCT). To avoid potential bias from comparing measurements across different time points, we limited the evaluation of associations among variables to the baseline data. 94 metastatic breast cancer (MBC) patients (mean age 56.8) receiving OAT for MBC have been enrolled. Each participant filled a set of measures assessing personality (Big Five), adherence (AAI-28 and MMAS-8) (© 2006 Donald E Morisky), and optimistic bias (VAS), and Quality of Life (EORTC QLQ-C30 and EORTC QLQ-BR23).
Results
A discrepancy between self-oriented and other-oriented evaluation of the capacity to take the therapy in the doses, frequencies, and times prescribed was observed (P < 0.001). A negative association between adherence rate and the self-perception of treatment adherence was identified (P < 0.001). Further, conscientiousness correlated positively with the perception of risk to their own health (P = 0.034), and negative association between extraversion and self-perception of treatment adherence (P = 0.05) and between agreeableness and self-perception of treatment adherence have been observed (P = 0.029).
Conclusions
Our findings suggest that optimistic bias and personality may contribute to shaping adherence in MBC patients. Personality traits influence adherence both directly, by increasing the perception of health risks, and indirectly, by influencing coping strategies and emotion regulation. MBC patients having an OB may underestimate the important side effects and physical comorbidities, as well as difficulties in the daily management and adjustment of therapy due to disease progression.
Keywords
Introduction
The widespread use of oral chemotherapeutic agents for cancer treatment has contributed to a substantial increase in the survival rate in metastatic breast cancer (MBC), transforming the landscape in cancer treatment and bringing attention to patient self-management of care. Even if oral anticancer treatments (OATs) have several advantages over intravenous administration, adherence is becoming a critical issue in the clinical management of cancer patients. The severity of the disease may be a critical factor in inducing cancer patients to be adherent to their medication intervention, even though scientific literature highlights that this is not always true, and adherence rates for medicine vary between 16% and 100% depending on the medication and measurement method. 1 Evidence highlighted that cancer patients reported preferring OATs compared to intravenous treatments. However, patients overestimate their ability to take them regularly and, as with other diseases, adherence to oral therapies is suboptimal. 2 Studies have reported that in the specific case of MBC, nonadherence rates decrease with time since treatment initiation. 3 Nonadherence severely affects treatment efficacy, symptom burden, disease progression, and survival. Considering the importance of nonadherence in terms of both individual and healthcare costs, early identification of MBC patients at risk of nonadherence by mapping the drivers of nonadherence is fundamental to improving health status and quality of life (QoL) along the cancer survivorship trajectory.3-7
Even if a gold standard definition of adherence does not exist, adherence might be defined as a multi-component process determined by cognition and feelings related to the therapies and disease. 8 Coherent with this definition, adherence behavior results from different components related to socio-economic aspects, the type of the disease and its features, treatments, and health system-related and individual-related characteristics. 9 From a psycho-cognitive perspective, studies emphasized attitudes, beliefs, and perceptions about the disease, treatments, and side effects, as well as the availability of social support, which are critical in determining adherence behavior.9,10 Further, patient perception of the disease and beliefs, adaptation, and related health behaviors are modeled by personality traits and cognitive distortions, helping to understand the adoption of health behaviors better and merge the longwinded evidence on adherence behaviors.11-14 For example, Rychter and colleagues (2023) found that chronic myeloid leukemia patients who declared missing doses displayed a greater intensity of type A personality traits. Moreover, in the case of the type D personality, a higher level of negative affect decreased adherence to the tyrosine kinase inhibitors (TKIs). 15 Further, a study investigating the relationship between personality and nonadherence using the five-factor model found that conscientiousness and agreeableness correlated with increased adherence. 16 Related to this last finding, another study on 220 cancer outpatients showed that being more accepting and tolerable, as well as having a greater willingness to please others, may help facilitate the adoption of behavior and habit changes necessary for better adherence to treatment. 17 The relationship between personality and adherence may be indirect. This means that personality might influence individual coping strategies related to the disease and its adaptations, modifying patients’ engagement, commitment to treatment, and decision-making regarding their health. 16
Along with personality traits, some authors have highlighted the role of cognitive biases in explaining the mental implicit processes behind medication nonadherence. 18 Specifically, the role of optimistic bias has been highlighted as a potential modulator of unhealthy behaviors (eg, tobacco smoking, unhealthy diet, alcohol consumption) and adherence to participation in cancer clinical trials.12,19-22 The optimistic bias23-25 refers to an imbalance in risk perception, and it might be considered one example of an array of self-serving beliefs. This cognitive bias made people think they would have a better future outcome than those with analogous features (peers) in the same situation. Jansen and colleagues have reported that more than 60% of patients enrolled in a clinical trial (phase I°) believed they were more likely to experience health benefits from the clinical trial.21,26 Furthermore, tobacco cigarette smokers underestimate their personal risk of developing cancer or other smoking-related diseases, reinforcing smoking over time.20,24,27 Despite its role in modulating health behavior, only one study has examined its role in modulating adherence and in a non-cancer population. For example, Suh and colleagues reported that participants who showed a high optimistic bias believed they would not have adverse health consequences if they failed to take the antihypertensive therapy. 28
In conclusion, the international scientific community has highlighted that the important advances made with the introduction of OATs require a better understanding of the key elements that define nonadherence and how to address them to improve patient survival.2,29,30 As far as we know, the interaction between optimistic bias, personality, and adherence in patients with MBC is a matter that needs to be explored further. Indeed, previous studies presented some methodological limitations related to the sample size used for the evaluation of the adherence using non standardized measures 16 and a cross-sectional design. 17 Furthermore, no studies are available investigating this relationship in MBC patients. Coherently, the main aim of this study was to analyze the role of the optimistic bias and personality traits in the modulation of nonadherence to therapeutic recommendations in MBC patients.
Methods
Study Design
This study was a secondary, retrospective observational analysis of prospectively collected data from a randomized controlled trial (RCT). We aimed to evaluate the association among optimistic bias, personality, adherence, and QoL. More in detail, we evaluated the role of optimistic bias, personality traits, and QoL in shaping adherence to OATs in a population of MBC patients. We describe this study following the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) 31 guideline and CHAMP (CHecklist for statistical Assessment of Medical Papers) 32 statement.
Procedure
This study is nested in the Pfizer project (65080791) titled “Enhancing therapy adherence among metastatic breast cancer patients”, aimed at developing and testing an adherence risk predictive model in the field of OATs and a decision support system for MBC patients (clinicaltrials.gov NCT06161181). The results discussed here are related to the secondary analysis (and refer to secondary outcomes of the Pfizer study) conducted to evaluate the psychological, cognitive, and personal factors involved in adherence to OATs. The study was conducted in accordance with the recommendations of the Helsinki Declaration and obtained ethical approval from the European Institute of Oncology (IEO, Milan - Italy) Ethical Committee (R1786/22-IEO 1907) on December 22, 2022. All participants have signed the informed consent. A dedicated researcher screened patients’ electronic health records for eligibility and approached eligible MBC patients by telephone. Interested and eligible MBC patients signed written informed consent in person and were randomly assigned to either the intervention group (a decision support system designed to promote adherence to OATs) or the control group (no intervention) in a 1:1 ratio. After randomization, participants completed a set of self-report measures at baseline (T0), month 1 (T1), month 2 (T2), and month 3 (T3) online. At the baseline (T0), MBC patients filled all measures (MMAS-8,33-35 AAI-28, 36 EORTC-QLQ-C30,37,38 EORTC-QLQ-BR23, 39 BFI, 40 and the optimistic bias items described below), while at T1, T2, and T3, adherence and QoL were evaluated. The full protocol of the study is published elsewhere. 41 The sample size for the cohort analyzed in this study was defined for the original RCT, and the current study reuses that existing dataset. 41 As a result, no additional sample size calculation was performed specifically for this secondary analysis. Therefore, the findings should be interpreted with caution. Because optimistic bias and personality traits were measured only at baseline, this secondary analysis includes baseline data only. To avoid potential bias from comparing measurements across different time points, we limited the evaluation of associations among variables to the baseline data. All patient information was de-identified prior to analysis.
Participants
Inclusion criteria involved female patients diagnosed with metastatic breast cancer (MBC), aged 18 years and above, prescribed oral medication (such as oral chemotherapy, hormonal therapy, cyclin-dependent kinase 4/6 inhibitors), with internet connectivity and a personal smartphone or tablet, and capable of reading and signing the informed consent. We excluded patients with any primary psychiatric or neurological conditions.
Instruments
Optimistic Bias (OB)
The OB was evaluated using four ad hoc items evaluating adherence to OATs. 18 The items were designed based on absolute judgments. 42 Two items were designed evaluating the probability of experiencing nonadherence to OAT and health risk perception associated to nonadherence compared to an average target person of one’s own age and sex (other-oriented evaluation) (Item 3: “How likely do you think it is that a woman with the same illness as you would be unable to take the therapy in the doses, frequencies and times prescribed?”; Item 4: “How risky do you think it is for the health of a woman with the same illness as you that she does not take the prescribed therapy correctly?”). Furthermore, the other two items were designed to evaluate one’s own probability of experiencing nonadherence to OAT in one’s own care pathway and health risk perception associated to nonadherence (self-oriented evaluation) (Item 1: “How likely do you think it is that you will not be able to take the therapy in the doses, frequencies and times that have been prescribed?”; Item 2: “How risky do you think it is for your health not to take the prescribed therapy correctly?”). The mean ratings obtained in each item are compared, and optimistic bias is reckoned if the mean rating for the self-oriented items is more favorable than the mean rating for the other-oriented items.
MMAS-8 Self-Report Questionnaire (© 2006 Donald E Morisky)
33,34,43 is a validated questionnaire assessing treatment adherence. In detail, the MMAS-8 is composed of 8 items evaluating the following dimensions related to individual adherence: medication-taking behaviour, side effects, problems, and forgetfulness. The Cronbach’s alpha, a measure of internal consistency reliability, was moderately high (α = 0.83), 35 indicating that the items within the scale are measuring the same underlying construct with good coherence.
Adherence Attitude Inventory (AAI)
This comprehensive rapid assessment tool comprises 28 Likert-type scaled items. The AAI delineates four key constructs - cognitive functioning, patient-provider communication, self-efficacy, and commitment to adherence - that aid in understanding medication adherence 36 (α = 0.80).
EORTC QLQ-C30
EORTC QLQ-C30 is a self-administered instrument offering a multidimensional approach to assessing QoL in cancer patients composed of 30 items. The items are categorized into five functional domains: role, physical, cognitive, emotional, and social. Additionally, the instrument includes three symptom scales addressing fatigue, pain, nausea/vomiting, and individual inquiries regarding common symptoms experienced by cancer patients. Lastly, there are two questions dedicated to evaluating the overall quality of life (α = 0.85).37,38
EORTC QLQ-BR23
The Breast Cancer (QLQ-BR23) module is designed to complement the QLQ-C30 questionnaire. Explicitly developed to study the QoL in breast cancer patients, the QLQ-BR23 aims to capture more relevant patient-reported outcomes. It comprises five multi-item scales addressing body image, sexual functioning, side effects of systemic therapy, breast symptoms, and arm symptoms. Additionally, single items evaluate sexual enjoyment, future perspective, and emotional responses to hair loss (α = 0.87). 39
Big Five (BFI)
Big Five (BFI) is a self-report inventory designed for efficient and flexible assessment of the five personality dimensions. With 44 items, it utilizes short phrases with easily understandable language. Participants rate each item on a 5-point scale, ranging from 1 (disagree strongly) to 5 (agree strongly). The Big Five is composed of five subscales: openness to experience (α = 0.78), conscientiousness (α = 0.81), extraversion (α = 0.87), agreeableness (α = 0.81), and neuroticism (α = 0.82). 40
Data Analysis
Outcomes
The primary outcomes of interest in this study were to evaluate the role of optimistic bias, personality traits, and QoL in shaping adherence to OATs in a population of MBC patients. Adherence was assessed using two validated self-report tools: the MMAS-8 Self-Report Questionnaire (© 2006 Donald E Morisky) and the Adherence Attitude Inventory (AAI-28), as described above. Specifically, the following adherence-related measures were evaluated at baseline (T0): cognitive function score, patient-provider interaction score, self-efficacy score, commitment to adherence score, AAI-28 total score, and MMAS-8 total score. QoL outcomes were evaluated using the EORTC QLQ-C30 and the breast cancer-specific module QLQ-BR23.
Predictors
The predictor variables in this study encompassed both OB and personality-related factors. The OB predictors included the following self-reported measures: self-perception of treatment adherence, perceived risk to one’s own health, perception of others’ adherence to treatment, and perceived risk to others’ health. In addition, personality traits were assessed using the BFI, with individual scores for extraversion, agreeableness, conscientiousness, neuroticism, and openness serving as personality-related predictors.
Potential Confounders
We selected potential confounders based on a combination of clinical judgment and evidence from the literature, as this integrated approach has been shown to outperform the use of either criterion alone. 44 Specifically, the following variables were included as confounders: age, marital status (married individuals vs unmarried), educational level (higher education vs other), employment status (employed vs other), and geographic location (participants residing in northern Italy vs central or southern Italy).
Exploratory Analyses
We assessed the distribution of all numeric variables, including age and the scores from the validated scales (MMAS-8, AAI-28, EORTC QLQ-C30, EORTC QLQ-BR23, and BFI), along with their corresponding patterns of missing values. 45 Variables with a missing rate above 50% were excluded from the analyses. For variables that did not follow a normal distribution, we considered appropriate transformations, such as logarithmic and Box-Cox, to improve normality. We also used correlation plots as an exploratory analysis tool to better understand the relationships among variables related to risk perception, adherence, personality traits, and quality of life. Pearson correlation coefficients were computed for all pairwise combinations of numeric variables, as appropriate. We employed the rcorr function in R, which calculates correlation coefficients and corresponding P-values, handling missing data by pairwise deletion. 46 The resulting correlation matrix was visualized using a heatmap, allowing simultaneous inspection of the strength and direction of associations across all variables included in the analysis.
Modeling
A series of generalized linear models (GLMs) were employed with a Gaussian family (ie, linear regression) to examine associations between the outcomes (adherence and quality of life) and predictors (optimistic bias and personality traits). All models were adjusted for potential confounders, including age, marital status, educational level, employment status, and region of residence. Results are presented as the Beta (β) coefficient with corresponding 95% confidence intervals (CIs) and P-values. The β coefficient in a Gaussian family model represents the expected change in the outcome variable for a one-unit change in the predictor, assuming all other variables are held constant. It quantifies both the direction and magnitude of the association between a predictor and the continuous outcome. Results were considered statistically significant if the P-value was less than 0.05. We performed all analyses using the R language.
Results
The results presented were organized in different sub-paragraphs as follow. In the first sub-paragraph were reported a series of descriptive statistics performed to depict socio-demographic (status, education and profession), and treatment information (type of OAT, and starting date of the treatment) of the participants. In the second paragraph, the OB was measured comparing the mean scores for ratings for self-oriented items (Item 1 and Item 2) with the mean scores for ratings for other-oriented items (Item 3 and Item 4) using a paired-samples t-test. A series of correlational analysis was performed aimed to detect associations between adherence measured by MMAS-8 and AA1-28 and OB measured by self-oriented items (Item 1 and Item 2) and other-oriented items (Item 3 and Item 4); as well as between OB and BIF, EORTC QLQ-C30, and EORTC QLQ-BR23. Finally, In the last sub-paragraph, results of the generalized linear models with a Gaussian family were reported (ie, multiple linear regression models, modeling the association among risk perception, adherence, and personality traits, adjusted for age, marital status, education level, employment status, and region).
Descriptive Statistics Results
Figure 1 displays our study flowchart. Of the 308 patients assessed for eligibility in the RCT, a sample of 94 MBC patients with mean age 56.8 (SD = 11) receiving OAT for MBC have been enrolled at the Division of Medical Senology of the European Institute of Oncology (IEO). A total of 214 patients were excluded for various reasons. These included not taking oral anticancer treatments, a lack of motivation to participate in the study, the perception of an excessive burden in participating in the study, poor health status and not having autonomous access to a laptop or mobile phone. Study Flowchart
Socio-Demographic Variables

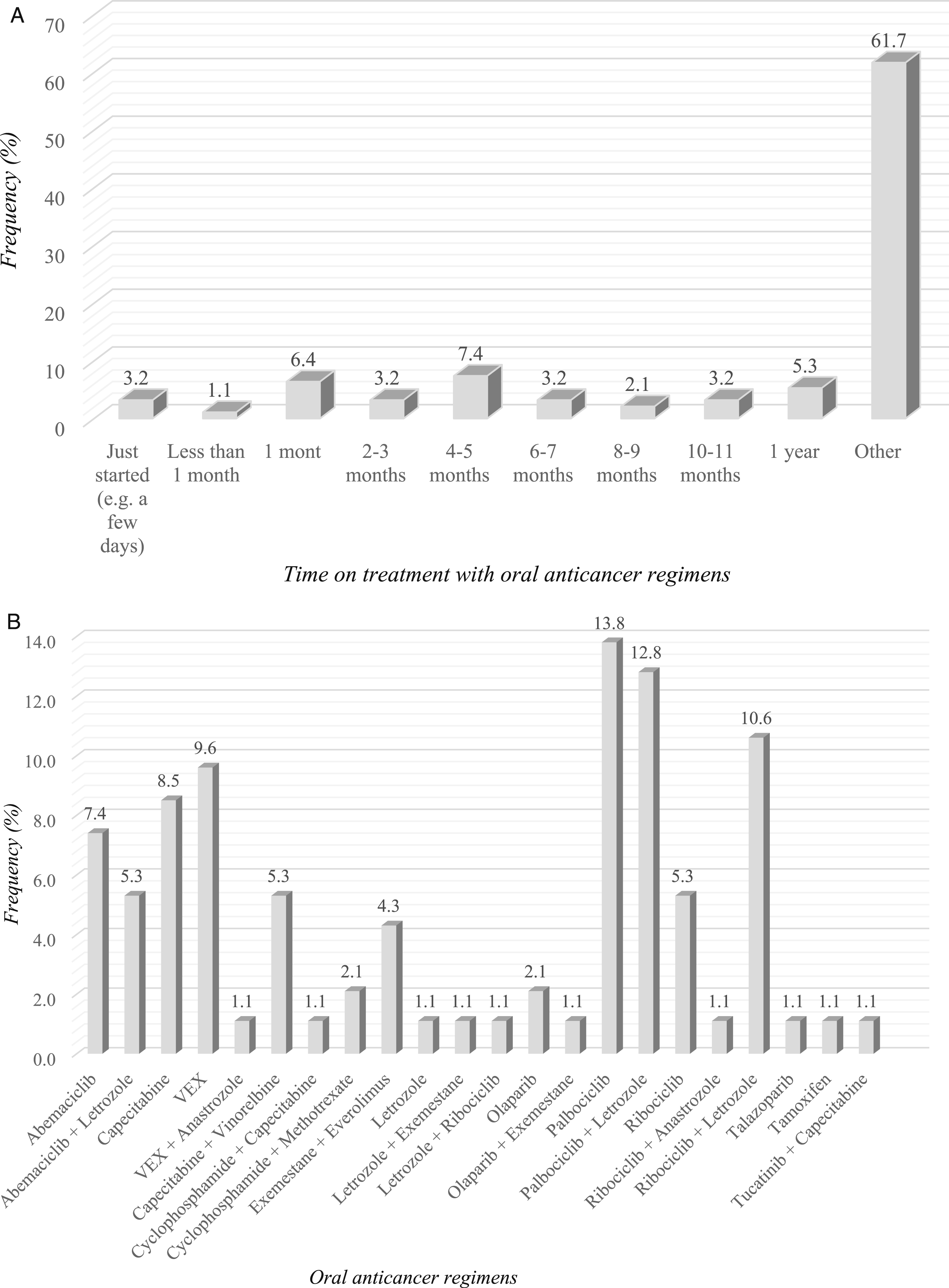
(A) Frequency Distribution of the OAT - Item: “When did You Start Taking the Current Oral Therapy?” (B) Frequency Distribution of the OAT - Item: “What Oral Therapy Are You Currently Taking?”
The Optimistic Bias for Adherence to OATs and Its Health Consequences: Differences Between Self-Oriented and Other-Oriented Risk Items
The possible existence of unrealistic optimism was assessed by comparing the mean scores for ratings for self-oriented items (Item 1 and Item 2) with the mean scores for ratings for other-oriented items (Item 3 and Item 4). Since both ratings were provided by the same participants, differences between means were tested using a paired-samples t-test.
In the Table Have Been Reported Baseline Assessments (T0) of: Personality Traits (BFI Subscales), Adherence (AAI-28 and MMAS-8 Total Score), and Self-Oriented (Item 1 and 2), Other-Oriented Items (Item 3 and 4) and QoL (EORTC QLQ-C30 and EORTC QLQ-BR23). For Each Variable has Been Reported Mean (M) and Standard Deviation Values (SD)
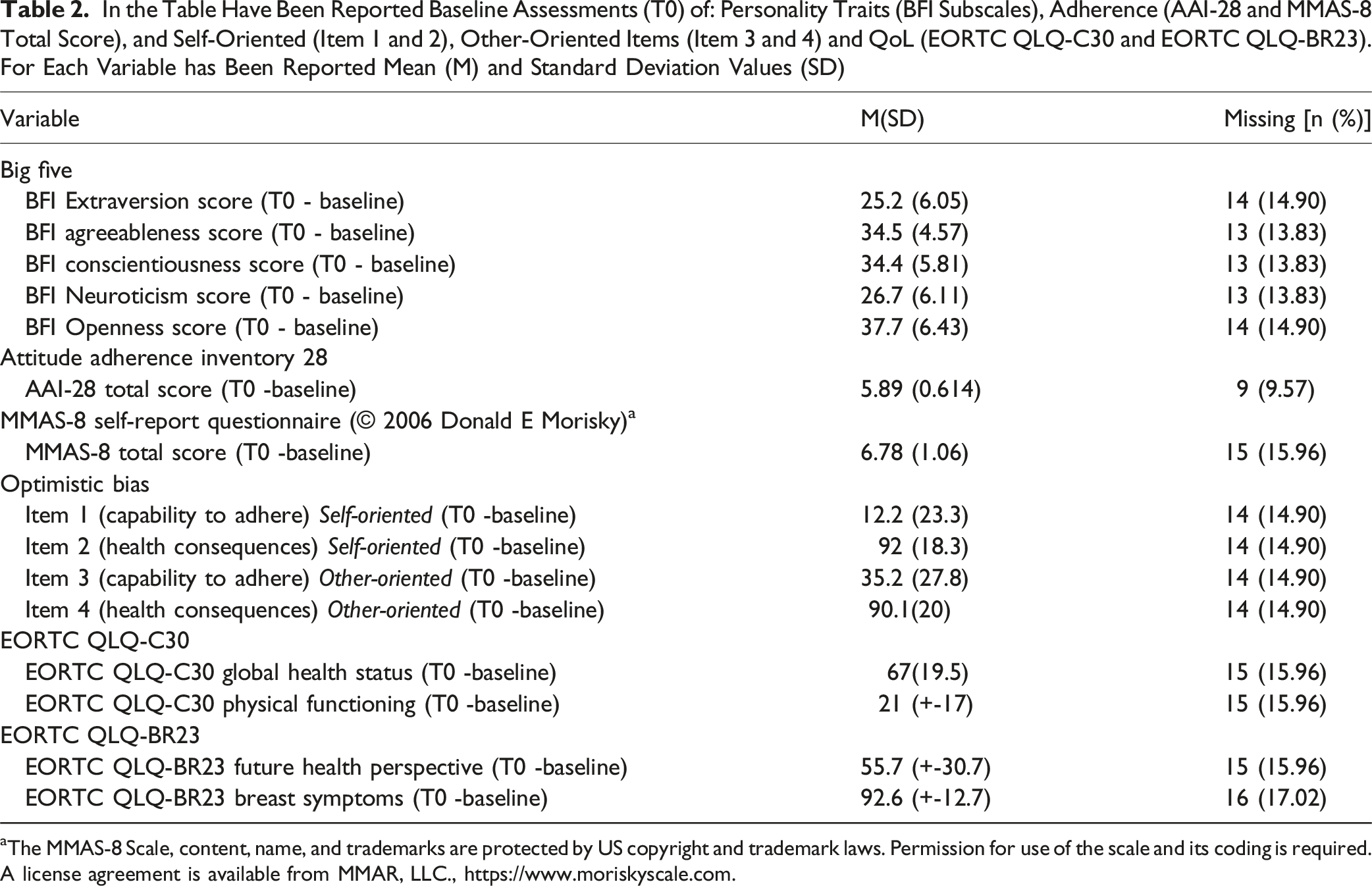
aThe MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., https://www.moriskyscale.com.
Correlations Between Self-Oriented and Other Oriented Items and Adherence Rate to OATs Measured by MMAS-8 and AAI-28
Figure 3 presents the correlation between other-oriented items (respectively, Item 3 evaluates capability to adhere, and Item 4 evaluates health consequences risk of nonadherence) and self-oriented items respectively, Item 1 evaluates capability to adhere, and Item 2 evaluates health consequences risk of nonadherence), and adherence rate measured by AAI-28 and MMAS-8. A strong and significant positive correlation was observed between the perceived risk to other people’s health and the perception of risk to own health (r = 0.754, P < 0.001). Significant Correlations Between Self-Oriented (Item 1 and 2) and Other-Oriented Items (Item 3 and 4), Adherence (MMAS-8 Total and AAI-28 Total Score), Personality Traits (BFI), and Quality of Life (EORTC QLQ-BR23and EORTC QLQ-C30). For Each Significant Correlation r and P-value Have Been Reported. *The MMAS-8 Scale, Content, Name, and Trademarks are Protected by US Copyright and Trademark Laws. Permission for Use of the Scale and Its Coding is Required. A License Agreement is Available From MMAR, LLC., https://www.moriskyscale.com
Several adherence measures are significantly associated with Items 1, 2, 3, and 4. Notably, the AAI-28 total score was negatively correlated with the self-perception of treatment adherence (r = −0.386, P < 0.001), suggesting that individuals who perceive themselves as more able to be adherent (Item 1) may score lower on overall adherence within AAI-28. The MMAS-8 total score was negatively associated with the self-perception of treatment adherence (r = −0.238, P = 0.034), supporting a similar trend where individuals who perceive themselves as highly adherent report lower adherence to the MMAS-8.
Additionally, the AAI-28 commitment to adherence score was positively correlated with the perceived risk to other people’s health (Item 4) (r = 0.249, P = 0.027), indicating that individuals who perceive a higher risk to others’ health tend to show stronger commitment to adherence. Moreover, the AAI-28 patient and provider score negatively correlated with the self-perception of treatment adherence (Item 1) (r = −0.265, P = 0.018), suggesting that individuals who perceive themselves as highly adherent rate lower in the patient-provider adherence measure. The AAI-28 commitment to adherence scores also presented a negative correlation with the self-perception of treatment adherence (Item 1) (r = −0.290, P = 0.01).
Optimistic Bias, Personality Traits and QoL: A Correlation Analysis Between Self-Oriented and Other-Oriented Items, BIF5, EORTC QLQ-C30 and EORTC QLQ-BR23
The results indicate significant associations between other-oriented and self-oriented items and personality traits (see Figure 3). The BFI conscientiousness score correlated positively with the perception of risk to own health (Item 2) (r = 0.238, P = 0.034). The BFI conscientiousness score was also negatively correlated with the perception of adherence to treatment by other people (Item 3) (r = −0.232, P = 0.038). Moreover, the BFI extraversion score was negatively correlated with the self-perception of treatment adherence (Item 1) (r = −0.225, P = 0.046). Furthermore, perception of risk to own health (Item 2) was negatively correlated with EORTC QLQ-BR23 future health perspective (r = −0.278, P = 0.013). Similarly, perception of risk to other people’s health (Item 4) was negatively correlated with EORTC QLQ-BR23 future perspective (r = −0.250, P = 0.026). Besides, perception of adherence to treatment by others (Item 3) was positively correlated with EORTC QLQ-BR23 breast symptoms (r = 0.260, P = 0.022) and EORTC QLQ-C30 physical functioning (r = 0.246, P = 0.029).
Generalized Linear Models
Reported Significant Associations Obtained Running Generalized Linear Models With a Gaussian Family, Between Self-Oriented (Item 1 and 2) and Other-Oriented Items (Item 3 and 4), Adherence (Respectively, MMAS-8 Total Score and AAI-28 Subscales), Personality Traits (BFI), and Quality of Life (Respectively, EORTC QLQ-BR23 and EORTC QLQ-C30). For Each Variable the Interval Confidence (95% CI) and Associated P-Value Have Been Reported. All Models Were Adjusted for Age, Marital Status, Education Level, Employment Status, and Region

aThe MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., https://www.moriskyscale.com.
Multiple associations between personality traits, risk perception, and EORTC QLQ-C30 quality of life domains were found. Physical functioning was positively associated with risk perception of adherence to others (β = 0.154, 95% CI: 0.026, 0.283, P = 0.02) but negatively associated with BFI conscientiousness (β = −0.852, 95% CI: −1.46, −0.243, P = 0.007) and openness (β = −0.649, 95% CI: −1.21, −0.083, P = 0.025). Significant associations were also identified between optimistic bias, personality traits, and breast cancer-specific QoL domains from the EORTC QLQ-BR23. Future health perspective scores were negatively correlated with the perceived risk to others’ health (β = −0.399, 95% CI: −0.771, −0.027, P = 0.036) and perceived risk to one’s own health (β = −0.505, 95% CI: −0.933, −0.077, P = 0.021). EORTC QLQ-C30’s global health status measure was positively associated with BFI extraversion score (β = 0.842, 95% CI: 0.118, 1.56, P = 0.023), conscientiousness (β = 0.978, 95% CI: 0.22, 1.74, P = 0.012), and openness (β = 0.789, 95% CI: 0.083, 1.5, P = 0.029).
Discussion
An enhanced understanding of key elements related to adherence to the OATs and an ability to predict adherence in a given MBC patient can improve their treatment effectiveness and long-term health outcomes. Despite the importance of the individual aspects in the modulation of adherence, the impact of patient personality and cognitive distortions has remained underexplored. 16 The current study focused on the role of optimistic bias and personality traits as potential modulators of medication adherence in MBC patients. The obtained results provide some meaningful insights for a more comprehensive understanding of OAT adherence and the clinical management of nonadherent patients. Boilersuit results highlighted that overestimating one’s own adherence and underestimating the potential risks of being nonadherent may hurt adherence to the cancer treatments along the care pathway. Moreover, results informed about the potential role of consciousness and extroversion as additional determinants of adherence.
Concerning the relationship between OB and adherence, our results suggest that the discrepancy observed between self-oriented and other-oriented evaluation of the capacity to take the therapy in the doses, frequencies, and times prescribed may show an optimistic bias related to the possible expected barriers to adherence (P < 0.001). In this vein, MBC patients seem to perceive a lower risk of being nonadherent to the medication protocol than other patients with the same disease and condition, confirming the presence of OB. They perceive themselves as more able to take therapy regularly without mentalizing possible future difficulties related to the therapy.
In the same vein, the negative association observed between adherence rate (measured by AAI-28 and MMAS-8) and the self-perception of treatment adherence (self-oriented evaluation) highlighted that MBC patients who perceive themselves as more adherent may score lower on overall adherence within AAI-28 (P < 0.001), as well as, within MMAS-8 (P = 0.034). Overall, these negative correlations imply that patients’ self-perceived adherence might differ from standardized adherence scales, potentially reflecting overconfidence in self-assessment. Then, the positive correlation observed between the perceived risk to other people’s health (other-oriented evaluation) and the perception of risk to own health (self-oriented evaluation) (P < 0.001) hints that MBC patients who perceive a higher risk to their own health, may also be more likely to provide more accurate estimations also for the others’ health. We argue that this overconfidence in their ability to adhere to the therapy may lead to an underestimation of the important side effects and physical comorbidities associated with OAT, as well as difficulties in the daily management of therapy and its adjustments due to disease evolution. Indeed, living with metastatic cancer produces important physical side effects and psychological and social consequences. Previous findings suggest that MBC patients may experience hepatotoxicity, neuropathic and gastrointestinal problems, as well as neurocognitive impairments, often involving learning and memory abilities. Additionally, cognitive dysfunctionalities have often been related to emotional vulnerability since MBC with low perceived cognitive function reported higher levels of depression, with social support moderating this relationship and protecting from low mood disturbance.42,44,47-50 MBC and its treatment have a debilitating effect on patients coping strategies and emotional wellbeing (eg, anxiety, fear) and QoL.41,51 Besides, the feelings of fear and worry, and the uncertainty related to the constant risk of the disease spread accompany the MBC patients’ trajectory. In the early phase of the diagnosis, MBC patients are focused on choosing the best treatment available, and to cure their disease. These results are coherent with several theoretical models, such as the Health Belief Model. As reported by Klein and Kunda (1994) the underestimation of one’s own risk of facing a negative health outcome may lead patients to be less inclined to assume preventive behaviors. Conversely, those who overestimate their ability to control an outcome may be more prone to making risky decisions and engaging in unsafe behaviors. 52
Further associations have been found between self-oriented, other-oriented items and QoL. In particular, we found that future health perspective was negatively associated with the perceived risk to others’ health (P = 0.036) and to one’s own health (P = 0.021). Probably, MBC patients having a more positive expectation about their future health might tend to provide a more realistic estimation of their capabilities to be adherent, and the future impacts on their health. Moreover, a higher perception of adherence to treatment by others was positively associated with better physical functioning (P = 0.02). We claim that a good personal perception of physical wellbeing (eg, feeling active or having few side-effects) might activate constructive thoughts and mental images regarding adherence. The more availability in the individual memory of such positive mental representations related to the medication adherence will contribute to increasing the judgement about self and others expected adherence behaviors. Otherwise, this better perception of adherence seems to be facilitated by an automatic process such as availability heuristic. 53 Coherent with dual process theory, the human mind uses heuristics to make decisions, particularly when the information is incomplete or missing, there is a high level of uncertainty, and when emotional factors are involved.54,55
Another interesting finding was the positive association between adherence commitment and perceived risk to others’ health (P = 0.027) and the negative association with self-perception of adherence (P = 0.01). These results suggest that people who perceive a higher risk to other people’s health may tend to be more determined to overcome barriers to adherence. Conversely, patients who are more confident in their ability to adhere to treatment may be less determined to deal with potential difficulties related to adherence. In addition, patients who perceive themselves as highly adherent could be less likely to discuss and share thoughts and feelings about adherence with their physicians (P = 0.018). Overall, these findings suggest that MBC patients who exhibit an optimistic bias may overestimate their personal ability to adhere and may be also less resolute in facing the difficulties that may arise along the care pathway due to the clinical complexity of cancer treatments. This attitude may be hazardous for the fulfillment of treatments: patients may be more likely to skip or alter doses, miss appointments, or stop treatment early, negatively affecting clinical outcomes. 56 This will also affect the communication and relationship between oncologists and patients regarding the potential issues related to the treatments and the risk of being nonadherent despite the health outcomes. Suboptimal patient adherence can impair a clinician’s ability to accurately evaluate treatment efficacy, potentially resulting in preventable hospitalizations, elevated mortality risk, and increased healthcare costs. 57
Additional novel findings are related to the function of the personality traits and their interaction with the optimistic bias. Our results indicate that conscientiousness correlated positively with the perception of risk to their own health (P = 0.034), indicating that individuals with higher conscientiousness tend to perceive a greater personal health risk associated with nonadherence. Conscious patients may be more engaged in taking care of their health by adopting preventive behaviors, and they show a more proactive attitude toward health. Consistently, previous studies have already detected a significant relationship between consciousness trait and health-promoting behaviors, thus encouraging patients to better understand issues related to their health and adopt an active coping strategy to protect their wellbeing. 58 For this reason, we argue that conscious MBC patients may show a more realistic picture of their adherence to the therapy, anticipating some expected risks due to the complexity of the medical protocols and their disease. Thus, they are less exposed to the risk of experiencing optimistic distortions. Therefore, conscious individuals may be willing participants in the patient-physician interaction and are likely to develop higher levels of patient-physician trust. These findings are consistent with the results retrieved in the literature on the relationship between personality and medication adherence in chronic conditions, reporting that higher conscientiousness was significantly associated with greater medication adherence, shared decision-making, and willingness to seek information about treatment. 59 Indeed, individuals with low conscientiousness may either take insufficient or excessive amounts of their medication, leading to a lack of therapeutic benefit or, in some cases, an increased risk of harm. Conversely, individuals with high conscientiousness are more likely to adapt their health behaviors, seek help when needed, and modify their habits during treatment. Moreover, they tend to think more long-term, which enhances their ability to assess the health consequences of their actions over time. 17
Conclusively, the results of the generalized linear models detected a significant negative association between extraversion and self-perception of treatment adherence (P = 0.05) and between agreeableness and self-perception of treatment adherence (P = 0.029). Considering that individuals with high agreeableness and extraversion scores are typically characterized by cooperativeness, sociability, assertiveness, and “willingness to please others”, a negative association between this personality trait and their own perception of medication adherence could be explained by hypothesizing that MBC patients tend to underestimate their medical adherence and wait for others’ feedback on their coping attitude. Accordingly, patients with extraverted and agreeable traits are more likely to maintain consistent social interactions and foster positive relationships with others (eg, healthcare professionals).60,61 In this framework, we hypothesize that MBC patients with higher agreeableness and extraversion rates could be more prone to focus on others’ perceptions, thus diminishing possible interpersonal conflicts. Moreover, our results highlighted that extraversion, conscientiousness, and openness might contribute to define a better QoL trajectory.
Limitations
This study presents some limitations that have to be considered. First, adherence has been evaluated using two self-reported measures, which might have affected the overall adherence rate. Indeed, the overall adherence rate was high in the sample. We argue that this high adherence rate was due to the use of the self-report measures (AAI-28 and MMAS-8), that might overvalue adherence compared to the other prospective methods. Further, patients with MBC are highly motivated to take the therapy, leading to greater adherence to the OATs prescribed at the beginning of the therapy.41,62 Secondly, the menopause has not been included in the collected variables, even though it is associated with an increased breast cancer risk. Similarly, the socio-economic status of the participants has not been evaluated. This variable might have an indirect impact on the overall adherence rate. Third, we have reported some missing data at T3. Fourth, although data were collected as part of a randomized controlled trial, the present analysis was cross-sectional in nature, as it focused exclusively on baseline measures. Therefore, the study’s cross-sectional nature limits our ability to draw conclusions about causal relationships across optimistic bias, personality traits, adherence, and QoL. Additionally, the study is based on a relatively small and potentially unrepresentative sample, which may limit the generalizability of the findings to the broader MBC population. Moreover, while we have considered several relevant factors, there may be unmeasured confounders (eg, psychological factors or support systems) that influence adherence but were not captured in this study. Lastly, the generalizability of the findings might also be affected by the specific clinical setting in which the study was conducted, which may differ from other healthcare environments.
Conclusions
To our knowledge, this is the first study conducted in patients with advanced cancer to evaluate the possible predictors of medication adherence. The current findings highlight the need for further exploration of the factors driving nonadherence and the implementation of tailored, evidence-based interventions to prevent and/or address these behaviors. Our findings suggest that optimistic bias and personality may shape adherence in MBC patients. Personality traits may influence adherence in two ways: directly, by increasing the perception of health risks associated with nonadherence, and indirectly, by influencing coping strategies and emotion regulation. In addition, OB may lead to an underestimation of the important side effects and physical comorbidities associated with OAT, as well as difficulties in the daily management and adjustment of therapy due to disease progression. As a result, when patients experience difficulties, they may not have sufficient internal resources to deal with them. In the century of artificial intelligence and machine learning models applied to healthcare, we argue that these findings will provide novel insights into both understanding medication adherence to OATs in advanced metastatic breast cancer and contribute to building the ontology of predictive models for early identification of MBC patients at risk of nonadherence.
Footnotes
Acknowledgments
Property/Identifier Issue/Registration Date/Category
• U.S. Reg. No. 5,837,273 August 20, 2019 Trade/Service Mark
• U.S. Reg. No. TX-8-285-390 June 12, 2016 Copyright
• U.S. Reg. No. TX-8-632-533 September 21, 2018 Copyright
Ethical Approval
The study obtained the ethical approval from the European Institute of Oncology (IEO, Milan - Italy) Ethical Committee (R1786/22-IEO 1907) on December 22, 2022. All participants have signed the informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been funded by a Pfizer grant: Enhancing therapy adherence among patients with metastatic breast cancer (65080791).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available from the corresponding author upon reasonable request.