
Abstract
Introduction
Taxane-based cytotoxic anticancer drugs are a cornerstone of advanced lung cancer chemotherapy; however, they often result in chemotherapy-induced peripheral neuropathy (CIPN). Along with prolonged recovery, CIPN may cause irreversible damage. Consequently, dose reduction or discontinuation is justified, potentially impacting therapeutic efficacy. With no established treatment for CIPN, low-dose duloxetine is generally used as a supportive drug. However, studies have shown the potential effect of mirogabalin on CIPN. Therefore, at our hospital, patients with advanced lung cancer experiencing CIPN during taxane-based first-line therapy received low-dose duloxetine, and were subsequently treated with mirogabalin.
Methods
In this study, we conducted a retrospective observational cohort study of the impact of mirogabalin administration on 14 advanced lung cancer patients when duloxetine alone was deemed insufficient. The median age was 71 years (52-89 years), with 9 male and 5 female patients. The Numerical Rating Scale (NRS) was utilized to evaluate outcomes, and Wilcoxon’s signed rank-sum test was used in statistical analysis.
Results
The median Numerical Rating Scale (NRS) score decreased from 5.5 (interquartile range [IQR]: 4.5-7.0) before to 4.0 (IQR: 3.0-5.0) after mirogabalin administration (P = 0.041), indicating significant pain reduction.
Conclusion
The addition of mirogabalin to duloxetine shows promise in alleviating CIPN in advanced lung cancer patients treated with taxane anticancer agents. These findings warrant further investigation and consideration for their integration into clinical practice for managing CIPN.
Introduction
In recent years, various first-line chemotherapy treatment options have emerged for advanced lung cancer lacking genetic mutations. These include carboplatin + nab-paclitaxel + atezolizumab therapy approved in the IMpower130 study 1 and carboplatin + paclitaxel + bevacizumab + atezolizumab therapy approved in the IMpower150 study for non-small cell non-squamous cell carcinoma. 2 In addition to carboplatin + nab-paclitaxel + pembrolizumab therapy approved in the Keynote 407 study 3 and taxane-based cytocidal anticancer drug combinations with immunotherapy, they have become the standard treatment for squamous cell carcinoma. However, the increasing use of taxane-based cytocidal anticancer drugs has led to chemotherapy-induced peripheral neuropathy (CIPN) emerging as a major concern.
CIPN manifests diversely, including tactile and temperature disturbances, vibration and arthropathy, neuropathic pain, movement disorders, and autonomic neuropathy, 4 significantly impacting daily life. CIPN often persists long after treatment, significantly impairing patients’ quality of life (QoL). Recent evidence has underscored the global burden of chronic painful neuropathy among patients with CIPN. A systematic review and meta-analysis involving data from 28 countries found that more than half of patients with CIPN experience chronic pain symptoms that can significantly impair quality of life and functional independence. 5 This further emphasizes the urgent need for effective and tolerable interventions in clinical settings.
Histopathologically, taxane-based cytocidal anticancer drugs induce axonopathy, primarily affecting thick and long axons. However, the neuronal cell body is relatively preserved, and secondary marrow damage occurs. In some cases, the sheath (Schwann cells) is also damaged. 6 CIPN clinical symptoms include mixed polyneuropathy, glove-and-stocking-type paresthesia starting from the extremities, burning sensation predominantly in the distal extremities when the cumulative dose is high, sensorimotor disturbance, and bradyarrhythmia. Moreover, it often causes autonomic neuropathy,7,8 necessitating dose reduction or discontinuation, thereby affecting chemotherapy regimens and patient outcomes. Currently, duloxetine, a serotonin/norepinephrine reuptake inhibitor (SNRI), is the only scientifically proven medication for CIPN-related pain, according to the guidelines published by the American Society of Clinical Oncology (ASCO). 9 However, in clinical practice, many patients experience limited efficacy or poor tolerability.
In such cases, other gabapentinoids such as pregabalin and gabapentin are also widely recommended as alternatives in several clinical guidelines, including those from ASCO, 10 ESMO, 11 and NeuPSIG. 12 These agents modulate calcium channels and have shown effectiveness in neuropathic pain, although their use may be limited by central nervous system side effects.
However, adverse events such as somnolence, headache, dizziness, malaise, nausea, and loss of appetite hinder its use and often result in treatment discontinuation.13,14
Recently, several observational and interventional studies have suggested the efficacy of mirogabalin for treating painful CIPN in various cancer types. The MiroCIP prospective trial demonstrated meaningful symptom relief in taxane-induced CIPN patients. 15 In addition, comparative research has indicated that mirogabalin may offer comparable or superior efficacy to pregabalin, with potentially fewer central nervous system side effects. 16 Similar therapeutic benefits have also been observed in perioperative patients with breast cancer receiving taxane-based chemotherapy. 17 Mirogabalin is indicated for peripheral neuropathic pain, and its mechanism of action indicates binding to the voltage-gated calcium channel (VGCC) α2δ subunit. 18 Therefore, in our hospital, low-dose duloxetine was administered to 14 patients with painful CIPN whose advanced lung cancer were treated with a taxane cytotoxic anticancer drug (eg, paclitaxel, nab-paclitaxel) as the first line of treatment.
Furthermore, mirogabalin was administered to patients who exhibited an inadequate response to low-dose duloxetine. The effect of additional mirogabalin on chemotherapy-induced peripheral neuropathy was then investigated.
Mirogabalin is a novel gabapentinoid that differs pharmacologically from pregabalin and gabapentin. Specifically, it exhibits higher binding affinity and selectivity for the α2δ-1 subunit of voltage-gated calcium channels, which is closely associated with analgesic efficacy. At the same time, it shows lower affinity for the α2δ-2 subunit, which has been implicated in central nervous system (CNS) side effects such as somnolence and dizziness. This receptor selectivity profile may contribute to improved tolerability while maintaining efficacy compared to other gabapentinoids.
We hypothesized that the addition of mirogabalin to duloxetine may provide synergistic analgesic effects in patients with taxane-induced CIPN by targeting complementary mechanisms. Duloxetine, a serotonin-norepinephrine reuptake inhibitor, modulates central descending pain pathways, while mirogabalin acts peripherally via high-affinity binding to the α2δ-1 subunit of voltage-gated calcium channels. This combination may thus enhance analgesic efficacy while maintaining tolerability.
Materials and Methods
Patients
This study was designed as a retrospective observational cohort study and was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 19
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Clinical Research Ethics Review Committee of the Society of St. Franciscan Himeji St. Mary’s Hospital (St. Mary’s Hospital, Himeji, Hyogo, Japan; approval number: S023-08; date of approval: May 23, 2023). The title of the approved protocol was “Enhancing Duloxetine with Mirogabalin for Treating Taxane-Induced Peripheral Neuropathy in Advanced Lung Cancer”. The approved registration period was from April 2020 to July 2022, and the data analysis period was from June 2023 to December 2023. Written informed consent was obtained from all participants prior to inclusion in the study. All patient data were anonymized to ensure confidentiality. From April 3, 2020, to July 31, 2022, we enrolled 14 consecutive patients with advanced lung cancer who received a taxane-containing regimen as the first-line treatment at our hospital. They were subsequently initiated on mirogabalin for CIPN-associated pain following inadequate response to low-dose (20 mg/day) duloxetine, which was selected considering tolerability and the typical starting dose for older patients.
All patient data were fully anonymized to protect personal identity.
As this was a retrospective observational cohort study, no formal sample size calculation was performed in advance. All eligible consecutive cases during the study period were included. The absence of a priori sample size estimation is acknowledged as a limitation of this study.
Procedures
Dose adjustments during mirogabalin administration aimed to balance efficacy and side effects. Pain intensity was comparatively measured using the Numerical Rating Scale (NRS) from the day of initiation to determine the efficacy of mirogabalin. The dose was gradually increased to the lowest effective dose (a one-step increase), and subsequently to the recommended effective dose (a two-step increase).
When the NRS score decreased after the additional introduction of mirogabalin, the best effect-determination period was defined as the number of days taken to capture the NRS score at the time of the lowest decrease. Side effects of mirogabalin were evaluated using the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE ver.5).
Additional Methodological Details for Reproducibility
Pain intensity was assessed by trained healthcare professionals using a verbal 11-point Numerical Rating Scale (NRS), ranging from 0 (no pain) to 10 (worst imaginable pain), and was recorded once daily during hospitalization or at each outpatient visit.
Mirogabalin was initiated at a dose of 5 mg twice daily and titrated upwards in 5 mg increments every 7 days based on patient tolerance, with a maximum dose of 15 mg twice daily. Patients receiving concurrent strong opioids were included, and morphine equivalent doses were recorded. Exclusion criteria included pre-existing peripheral neuropathy from other etiologies, ongoing treatment with other gabapentinoids, and severe renal impairment (eGFR <30 mL/min/1.73 m2).
Statistical Analysis
NRS scores pre and post-mirogabalin treatment were analyzed as paired data, using the Wilcoxon’s signed rank-sum test to evaluate their significance. Duloxetine compliance was not sufficiently confirmed in 2 patients; therefore, they were excluded from the count of concomitant drugs. Statistical analyses were conducted using SAS, version 9.3 (SAS Institute Inc., Cary, NC, USA), with P < 0.05 considered statistically significant.
The choice of Wilcoxon’s signed-rank test was appropriate given the paired and non-normally distributed nature of the data. While the sample size was limited, this study was exploratory in nature and aimed to generate preliminary insights. Therefore, statistical conclusions were interpreted with caution. There were no critical issues regarding the applied statistical procedures.
Results
Patient Background

Changes in NRS Before and After Administration of Mirogabalin and Regimen
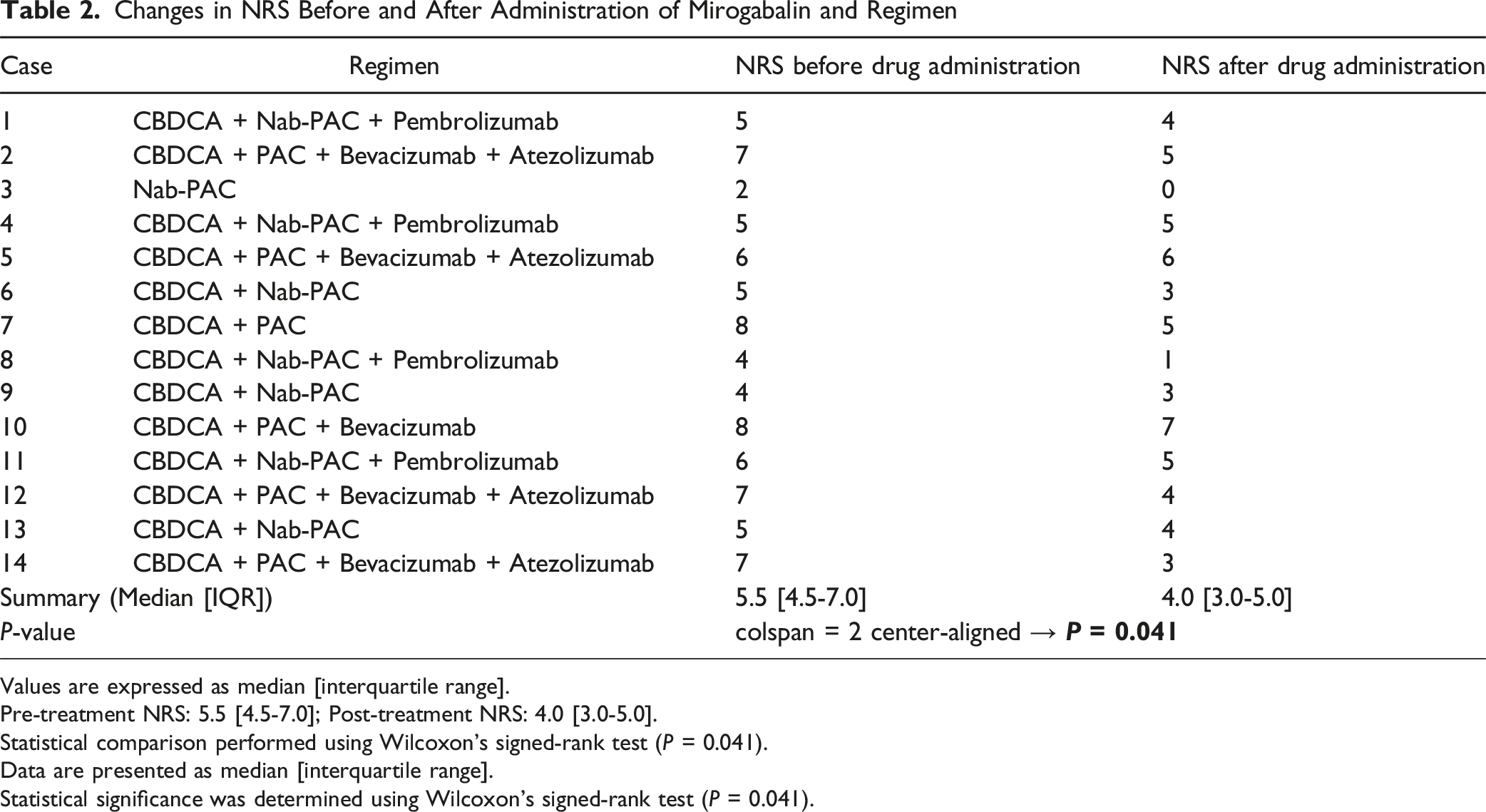
Values are expressed as median [interquartile range].
Pre-treatment NRS: 5.5 [4.5-7.0]; Post-treatment NRS: 4.0 [3.0-5.0].
Statistical comparison performed using Wilcoxon’s signed-rank test (P = 0.041).
Data are presented as median [interquartile range].
Statistical significance was determined using Wilcoxon’s signed-rank test (P = 0.041).

Changes in the NRS before and after Mirogabalin Administration (Wilcoxon Signed Rank-Sum Test)
The median Numerical Rating Scale (NRS) score decreased from 5.5 (interquartile range [IQR]: 4.5-7.0) before treatment to 4.0 (IQR: 3.0-5.0) after mirogabalin administration. This difference was statistically significant (P = 0.041, Wilcoxon’s signed-rank test). These findings are summarized in Table 2.
Among the 14 patients who started administration at the starting dose, 8 (57.1%) achieved the best response at the lowest effective dose (a one-step increase) and 4 (28.6%) achieved the best response at the recommended effective dose (a two-step increase).
Adverse reactions to mirogabalin included drowsiness in 3 of 14 patients (21.4%), with grade 1, 2, and 3 drowsiness in 1 patient each. The grade 3 side effect of drowsiness improved with dose reduction. No other adverse effects were observed. Drowsiness incidence exceeded package insert expectations, potentially due to concurrent duloxetine use, since all side effects occurred in patients previously given duloxetine.
Discussion
CIPN diagnosis remains challenging due to subjective symptoms. 20 The absence of a standard evaluation method 21 and the variety of tools used for evaluation further complicate the situation. 22 Prevalence rates of CIPN fluctuate over time, noted at 68.1% within 1 month post-chemotherapy, 60.0% at 3 months, and 30.0% after 6 months or more. 23 CIPN evaluation techniques are classified as subjective or objective techniques. 21 One subjective technique is the Common Terminology Criteria for Adverse Events of the National Cancer Institute (NCI-CTCAE), in which physicians rate symptoms on a five-grade scale, from grade 1 to grade 5, based on symptoms. 24 However, patient awareness may be underestimated. 25 Objective techniques include quantitative sensory testing (QST) and nerve conduction studies (NCS), which can help identify areas of injury but have limited discriminatory power. 26 Moreover, the total neuropathy score (TNS), combining both approaches, are rarely used in practice. 27 Moreover, clinical diagnosis often involves assessing nerve damage associated with neuromuscular diseases like Guillain–Barré syndrome and chronic inflammatory demyelinating polyradiculoneuropathy. Diagnosis by exclusion is the norm, whereby disorders such as diabetic neuropathy, uremia, connective tissue disease, vitamin B1 deficiency, and hand-foot syndrome are ruled out before a definitive diagnosis is made.
Diabetes is a recognized CIPN risk factor,28,29 alongside advanced age, chemotherapy regimen, neuropathy, symptom severity, and treatment cycles, among other risk factors. 30 Additionally, genetic predispositions to neurotoxin susceptibility also contribute to CIPN risk. 31
For example, after oxidative stress, Paclitaxel induces mitochondrial damage and disrupts pro-apoptotic Bax and anti-apoptotic BclII family protein balance in dorsal root ganglion (DRG) neurons, leading to CIPN.32,33
The ASCO, European Society for Medical Oncology, European Oncology Nurses Society, and European Association of Neuro-Oncology28,34 guidelines only recommend duloxetine for the treatment of painful CIPN based on the results of a large-scale randomized controlled trial (RCT). 35
Duloxetine’s analgesic mechanism likely involves blocking serotonin and norepinephrine transporters, as well as sodium channel currents. This affects descending inhibitory pain neural networks,36-38 inhibiting spontaneous nerve impulses from the peripheral to the central nervous system.
Despite the lack of RCTs for mirogabalin, 1 observational study and 2 retrospective studies are showing promising initial results. Kimura et al. conducted a multicenter, prospective, single-arm, open-label observational study involving patients experiencing CIPN pain. They evaluated the change in the visual analog scale (VAS) score by switching from pregabalin to mirogabalin, which significantly decreased the average VAS score (Δ15.7 mm, P < 0.0001). 39 In a comparative trial investigating the efficacy of mirogabalin vs pregabalin for CIPN in patients with pancreatic cancer receiving FOLFIRINOX (Oxaliplatin, Irinotecan, Leucovorin, and 5-Fluorouracil) therapy with oxaliplatin or gemcitabine plus nab-paclitaxel, both groups demonstrated significant improvements. Furthermore, the CIPN improvement rate in the mirogabalin group at weeks 2, 4, and 6 was significantly higher than that in the pregabalin group (84.6% vs 33.3%, P = 0.005; weeks 4 and 6: 92.3% vs 33.3%, P = 0.001). 40 Kanbayashi investigated 133 patients (including 16 with CIPN) who received mirogabalin for the relief of neuropathic pain, including CIPN. The patients were classified into a highly effective group (9 patients, including 8 with CIPN) and a very effective group (9 patients, including 2 with CIPN). Consequently, a correlation was suggested between the efficacy of mirogabalin, the maintenance dose (≤20 mg/day), and the concurrent use of opioids and neurotropin. 41
In addition, while combination therapy with duloxetine and mirogabalin may offer enhanced analgesic effects, there is a potential risk of additive side effects, particularly central nervous system-related adverse events such as sedation and drowsiness. These effects have been reported with both agents independently, and co-administration may increase their frequency or severity. Therefore, careful monitoring and individualized dose adjustment are essential when considering combination therapy, especially in older adults.
Mirogabalin, a selective ligand targeting the α2δ subunit of voltage-gated calcium channels (VGCC), is developed for neuropathic pain management. It was approved for peripheral neuropathic pain based on Japanese clinical trials on patients with diabetic peripheral neuropathic pain and postherpetic neuralgia. The ligand selectivity of mirogabalin for α2δ-1 and α2δ-2 and the slower rate of dissociation for α2δ-1 relative to the α2δ-2 subunit of VGCC explain its potent analgesic effects, wide safety margins, and relatively low side effects.
While our findings suggest that mirogabalin may provide benefit in duloxetine-refractory cases of CIPN, it is important to position this treatment option in the context of existing clinical guidelines.
According to ASCO, ESMO, and NeuPSIG guidelines, pregabalin and gabapentin are also recommended as second-line treatments for neuropathic pain, including CIPN, especially when duloxetine is ineffective or poorly tolerated.
Mirogabalin’s distinct pharmacological profile may offer advantages over these agents; however, direct comparative studies are lacking and should be prioritized in future research.
However, this study had limitations. Bias existed in the number of regimen cases surveyed, necessitating future studies with larger sample sizes. Additionally, investigating the effects of mirogabalin alone, without low-dose duloxetine, but with standard-dose duloxetine, is warranted.
Furthermore, emerging therapies such as neuromodulation have shown promise in managing refractory CIPN pain. Spinal cord stimulation, in particular, has been reported to alleviate neuropathic symptoms in selected patients with chemotherapy-induced peripheral neuropathy, and may be considered in future research and clinical practice as an option for patients who do not respond to pharmacologic interventions.
In conclusion, this study is the first to examine the adjunctive effects of mirogabalin in patients with lung cancer undergoing duloxetine therapy for CIPN. Given its manageable side effects, mirogabalin could serve as a valuable supportive therapy for CIPN in patients with lung cancer.
Conclusion
This retrospective observational cohort study suggests that the addition of mirogabalin to duloxetine may provide symptomatic relief in patients with advanced lung cancer who experience taxane-induced peripheral neuropathy and show insufficient response to duloxetine alone. Despite the limited sample size and lack of a control arm, the observed improvements in patient-reported pain scores indicate the potential utility of this combination therapy in clinical practice. Given the paucity of effective treatments for CIPN and the limited recommendations in current guidelines, our findings contribute preliminary evidence supporting further investigation of mirogabalin as a component of multimodal management. Future prospective, randomized, and comparative studies are warranted to validate efficacy, clarify its position relative to other gabapentinoids, and assess safety in broader populations.
Limitations
This study has several limitations. First, it was a retrospective observational cohort study conducted at a single center, and the sample size was small. As such, the statistical power was limited, and the findings should be interpreted with caution. Second, there was potential selection bias in the chemotherapy regimens used, as some treatment arms included only a small number of patients. Third, the study utilized low-dose duloxetine (20 mg/day) based on tolerability considerations for older patients; therefore, it remains uncertain whether a standard-dose duloxetine regimen (40-60 mg/day) might have produced a therapeutic response on its own. Fourth, the analgesic effect of mirogabalin alone was not evaluated, making it difficult to determine the relative contribution of each agent in the combination therapy. Fifth, our study did not compare mirogabalin with other commonly used gabapentinoids such as pregabalin or gabapentin. Therefore, we cannot determine whether mirogabalin is more effective or better tolerated than these agents. Direct head-to-head randomized controlled trials would be necessary to address this question, but such a comparison was beyond the scope of our single-arm retrospective observational study.
Sixth, pain intensity was assessed using a patient-reported Numerical Rating Scale (NRS), which is inherently subjective and may be influenced by reporting bias. Seventh, the study lacked objective functional outcomes such as changes in morphine equivalent daily dose (MEDD) or standardized neuropathic pain questionnaires. Finally, duloxetine adherence was uncertain in 2 patients, and therefore they were excluded from the analysis of concomitant medications, which may have affected the overall interpretation.
Footnotes
Acknowledgements
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board of Himeji St. Mary’s Hospital (Date: 2023/5/23, Approval No. S023-08).
Authors’ contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.