
Abstract
Introduction
The COVID-19 pandemic caused marked disruptions in healthcare services, including cancelation or deferral of routine and non-emergent procedures. We used the database of the largest health maintenance organization (HMO) in Israel, Clalit Health Services (CHS), to collect data of all members between the ages 50-74 years who were eligible for colorectal cancer screening.
Methods
Three timeframes were defined: pre-COVID-19; 1st year, and 2nd year of the pandemic. We evaluated the frequencies of subjects who underwent CRC screening and described any trends along each demographic.
Results
The pre-pandemic, 1st year and 2nd year cohorts included 926,852, 937,403, and 941,704 subjects, respectively. Compared to the baseline year, the screening rates overall were 2.1% and 2.7% lower in the 1st and 2nd year, respectively. Steeper declines in screening were observed among Arab and Orthodox Jewish populations. There was no statistically significant difference in the number of patients who completed a colonoscopy following a positive FIT, and no difference found between various ages, genders, and other population groups.
Conclusion
Our findings could have implications for early detection and treatment of CRC within these two specific demographic groups.
Introduction
Colorectal cancer (CRC) is the third most common malignancy in the developed world and the second most common oncological cause of death, following lung cancer. 1 Screening programs have been devised as a primary prevention strategy, with yearly fecal immunochemistry test (FIT) and periodic colonoscopy being the two most common screening modalities. These screening programs were demonstrated to have significant health benefits,2,3 as well as cost-effectiveness. 4 In most national and international guidelines, current recommendations for the average-risk individual are to initiate CRC screening at the age of 50 with either an annual FIT test or a screening colonoscopy performed once every 10 years, ending at the age of 75.5-7
The screening for CRC relies on the completion of a full colonoscopy following a positive FIT, for the detection of colorectal cancer or advanced pre-malignant adenomatous polyps. Previous studies have demonstrated that longer intervals between a positive FIT and the completion of colonoscopy (termed “time-to-colonoscopy”) result in significantly higher rates of advanced adenomas, colorectal cancer in general, and advanced stage CRC.8-10 Thus, in most national and international guidelines, the time to colonoscopy should ideally be within 6 months following a positive FIT.
In early 2020, the Coronavirus-19 pandemic (COVID-19) caused substantial disruptions in healthcare services worldwide ranging from a pattern of reduced tendency to seek emergency medical services, 11 to diminished activity of urgent and non-urgent cardiovascular interventions, 12 to a reduction in routine screening tests such as mammography and cervical cytology sampling.13,14
Delays in screening programs for colorectal cancer due to the COVID-19 pandemic are likely to contribute to excess diagnoses of later-stage CRC cases, and as a result, possibly increased mortality from CRC in the years to come. Studies conducted in other areas of cancer epidemiology have shown a “shift” of newly diagnosed cases to more advanced-stage disease, 15 and mathematical models predict as much as a 2% increase in cancer-related mortality due to pandemic associated delays in the upcoming decade. 16 Few studies examined the impact of COVID-19 pandemic on CRC screening programs.
In this study, we evaluated the effects of the COVID-19 pandemic on CRC screening rates and on the completion of a diagnostic colonoscopy after a positive FIT test in various demographic groups of the Israeli population.
Methods
Study Design and Participants
We conducted an observational, retrospective, population-based cohort study on data obtained from the electronic medical records of Clalit Health Services (CHS), the largest health maintenance organization (HMO) in Israel which provides care for 4.8 million individuals (51% of the population). The study was approved by the Institutional Ethics Committee for Human Studies of CHS (authorization number 0175-20-COM1). The methodology of data collection, definitions, and linkage of the CHS data files has previously been reported in detail. 17 This study complies with the RECORD guidelines. 18
The study population included all Clalit Health Services patients aged 50-75 with an average risk for colorectal cancer. Data was collected for each subject from March 1st 2019 to August 31st 2022, or until death or leaving CHS, whichever occurred earlier. Three cohorts were defined: pre-Covid (March 1st, 2019-February 29th 2020), the 1st COVID-year (March 1st, 2020- February 28th 2021), and the 2nd COVID-year (March 1st 2021-February 28th 2022). Eligible individuals in age groups 50-59, 60-69, and 70-75 at the starting point of each of the three study periods were included in each cohort. Individuals with colorectal cancer diagnosed prior to each of the comparison periods, and those with higher-than-average risk for CRC (eg, Lynch syndrome, familial adenomatous polyposis) were excluded.
Outcomes and Covariates of Interest
The primary endpoint was screening rate, defined as the performance of FIT within the last year, colonoscopy within the last 10 years, or virtual colonoscopy within the last five years, according to the American College of Gastroenterology (ACG) clinical guidelines. 6 The secondary endpoint was performance of colonoscopy within 6 months of a positive FIT, following the ACG guidelines.
Patient-level covariates of interest included age, sex, and population groups (general-Jewish, Arabs, and ultra-orthodox Jewish).
Statistical Analysis
Screening rates were compared using the rate ratio (RR). To quantify the uncertainty around the estimated RR, the Wilson score interval method was applied to calculate the lower and upper bounds of the 95% confidence interval (CI). Additionally, the percent change from baseline was calculated. Sub-group analyses were conducted using stratification by sex, age groups, and population groups. In order to account for the lack of independence between the cohorts, assuming individuals may be present in all of the three cohorts, a mixed-effects logistic regression analysis was performed with the screening periods as the fixed effect and screened subjects as the random effect. Results for this analysis were reported as the odds ratio of screening.
Analyses were conducted using SPSS 25.0 software. A P-value <0.05 was considered statistically significant. All reported P-values are two-tailed.
Results
Study Population
Population Characteristics

Screening Rates
Screening Rates
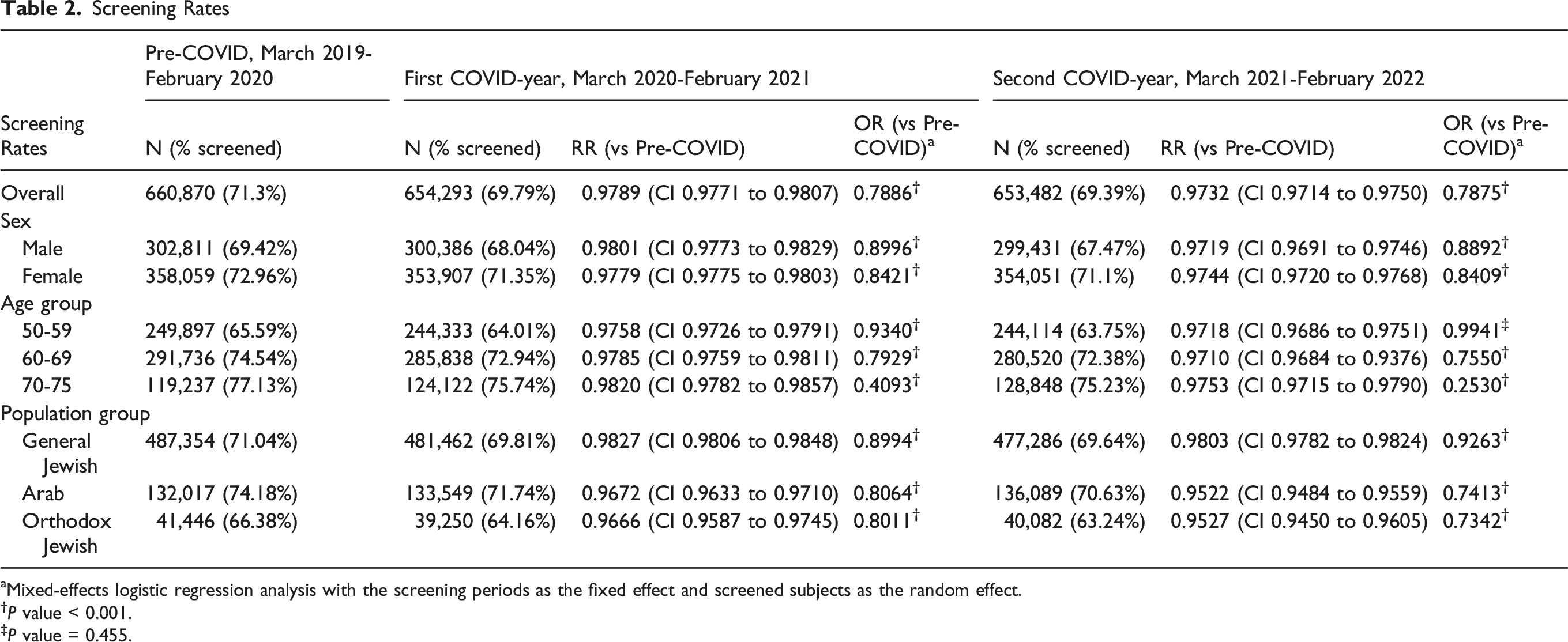
aMixed-effects logistic regression analysis with the screening periods as the fixed effect and screened subjects as the random effect.
†P value < 0.001.
‡P value = 0.455.
In the first pandemic year, overall screening rate decreased to 69.79, dropping by 2.1% (RR 0.979, 95% CI 0.977-0.991). The relative decrease was similar in males and females, as well as across age groups. However, when stratifying by population group, the decrease was sharper in the Arab Israeli group, with a 3.3% lower chance of screening (RR 0.967, 95% CI 0.963-0.971), and screening rates dropping from 74.18% in the baseline year to 71.74% in the first pandemic year. A similar decrease of 3.34% (RR 0.9666, 95% CI 0.9587-0.9745) was observed in Orthodox Jews as screening rates dropped from a 66.38% rate in the baseline year to 64.16% in the first pandemic year. However, in the general Jewish group a milder disruption in screening rates was observed, dropping by only 1.7% (RR 0.983, 95% CI 0.981-0.985) compared to the baseline year (Figure 1, Table 2). Percent Change in Screening Rates in the First COVID-19 Year Compared to Pre-pandemic Year, by Sociodemographic Characteristics
In the 2nd COVID-year, the overall screening rates declined by 2.7% (RR 0.973, 95% CI 0.971-0.975) compared to the baseline year. As described for the first pandemic year, the relative decrease was similar in male and female and across age groups, but differences between population groups were observed. The sharper decrease in the two minority groups persisted in the second pandemic year. Screening rates dropped by 4.8% (RR 0.952, 95% CI 0.948-0.956) in the Arab group, and by 4.7% (RR 0.952, 95% CI 0.9450-0.9605) in the orthodox Jewish group, whilst in the general Jewish group the drop in screening rate compared to the baseline year was more moderate, decreasing by 2.0% (0.980, 95% CI 0.978-0.982) (Figure 2, Table 2). Percent Change in Screening Rates in the Second COVID-19 Year Compared to Pre-pandemic Year, by Sociodemographic Characteristics
With a mixed-effect logistic regression analysis, the OR of being screened for CRC reduced during both pandemic years. Similar degrees of statistically significant screening rate reductions were observed in the sub-group analyses, with the exception of the 50-59 age group, which showed a small, non-statistically significant reduction in screening rate during the 2nd pandemic year (Table 2).
Colonoscopy Performance within Six Months of a Positive FIT
Colonoscopy Performance Within Six Months of a Positive FIT

Discussion
Our study showed an overall decrease in CRC screening rates in the 1st and the 2nd years of the COVID-19 pandemic compared to the pre-pandemic baseline year. The most pronounced reductions in screening during the study periods were observed among the Arab Israeli and Orthodox Jewish populations, reaching 4.8% and 4.7% respectively in the second pandemic year. The study showed no reduction in the completion of colonoscopies within 6 months in individuals with a positive FIT test. This finding was consistent across age, sex, and ethnic population groups.
The overall drop in screening rates was modest during the first pandemic year, and a similar drop was noted in the second year. This is comparable to previous studies in the field of CRC screening19-21 as well as other cancer screening programs, although some studies found a small “rebound” period in the second year of the pandemic.22-24 This decline in screening rates is likely to have a negative impact on patients, as recent studies using projection models have calculated a significant mortality increase among patients who discontinue screening following the COVID-19 pandemic.25,26
Other studies have shown that the pandemic and the associated lockdowns and healthcare restrictions had a disproportionate impact on certain population social groups—with older, lower socioeconomic status, and minority groups tending to be more affected than the rest of the population.22,23,27,28 In our study, we did not find significant differences in CRC screening rates between sex or age cohorts. However, a disproportionally larger decrease in screening rates over the pandemic years was observed among the two largest minority groups in Israeli society, namely Orthodox Jews and Arab Israelis. A recent large population study from Canada also showed significant reductions in the up-to-date screening status comparing pre-pandemic and post-pandemic years, with the more prominent disparity among patients in lower socio-economic classes and those of immigrant status. 29 There are several possible explanations for these findings. Firstly, minority groups are also more likely to have a lower socio-economic status, and historically been disadvantaged with regards to access to medical services. 30 Secondly, they often suffer from a greater comorbidity burden—for example, the Arab Israeli elderly are more likely to require help with activities of daily living (ADL) and more likely to be home-bound than the corresponding ages in the general Israeli population. 31 Furthermore, previous studies identified religious beliefs and exposure barriers as major factors in the reduced participation of Orthodox Jewish women in breast cancer screening programs, 32 and it is likely that similar factors are relevant in our case as well. Lastly, it is possible that during an international crisis of such magnitude as in the early years of the COVID-19 pandemic, the national response was not focused on providing culturally-appropriate information and adequate proactive measures to social minorities, which could have led to lower awareness of the importance of routine screening even during a national crisis and the existence of alternative, at-home screening methods such as the FIT test.
Our study also looked at another critical point in the CRC diagnostic pathway, namely a full colonoscopy evaluation following a positive FIT test. Previous studies have shown that with longer delays between a positive FIT result and colonoscopy, more CRC cases are detected as well as more advanced stage disease at diagnosis.8,33 In our study, there was no difference between the percent of patients completing the guidelines-recommended colonoscopy exam in under 6 months during either of the pandemic periods, compared to the baseline. There were no differences noted even when assessing for age, sex and the two largest minority groups in Israeli society. Other studies done in this field had conflicting results, with some showing similar median time interval between positive FIT and colonoscopy,34,35 while others observed delays in the time to colonoscopy ranging from a delay of 40 days 36 to over 60 days. 37 Several other studies have shown a reduction in the overall number of patients completing colonoscopies following a positive FIT in under a year 38 or without mention of a time frame. 39 This finding is encouraging with regards to the ability of the Israeli healthcare system to function under stressful and emergency conditions.
Our study mirrors results of other studies conducted on cancer screening trends during the COVID-19 pandemic. A previous study in Washington state 39 found that Asian, African-American and multi-racial women, women who did not have private insurance, and those living in rural areas had significantly lower breast cancer screening rates in 2020 compared to pre-pandemic cohorts. Another study found that women of Native American and Asian/Pacific Islander background had the steepest decline in cervical and breast cancer screenings during the pandemic. 28 However, other studies24,40,41 showed that the use of telehealth during the pandemic increased screening rates for various cancer screening programs, by allowing patients to receive medical consultations, and to reschedule screening appointments that were cancelled during pandemic disruptions. This provides a potential strategy to implement in future states of emergency in order to bridge the gap of healthcare access for vulnerable populations.
This study presents several limitations. First, our study relies in part on national data for screening rates, and does not include Clalit patients who may have performed colonoscopies in private institutions. This can ultimately become a significant number of patients counted as “unscreened” for the purpose of this study, who did in fact perform a screening procedure during the studied period. Second, other potential factors that were not considered in the scope of this study, such as socio-economic status and geographical location (rural vs urban), or the co-morbid burden of patients, which may have influenced their decision whether to access healthcare services during the early pandemic period. Third, as a retrospective study, only past performance could be studied, without the ability to predict future implications of any observed delays and disparities.
Conclusion
There was a modest decline in CRC screening rates across the board, without any recovery in the second pandemic year. The population groups seemingly most impacted by this were the Israeli Arabs and Orthodox Jewish. Although further studies will be needed to elucidate the particular clinical significance of such delays, these findings may indicate the construction of proactive measures to bolster the availability of CRC screening tests in future health crises or other national/international states of emergency, especially amongst minority groups and the under-privileged.
Footnotes
Ethics Approval
This study was approved by the ethics committee of Clalit Health Services, authorization number 0175-20-COM1, dated 03/11/2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.