
Abstract
Introduction
Colorectal cancer (CRC) has a lengthy cellular mutation period and early onset (EOCRC) is linked to lifestyle-related factors. Primary prevention approaches earlier in the life course are needed. Emerging adulthood (age 18-25) is a critical stage for shaping health trajectories, and future orientation influences health behavior decisions. Little is known about emerging adults’ consideration of future cancer risk (CFC-Cancer), or perceived CRC risk. This study characterizes emerging adult CFC-Cancer, perceived CRC risk, and how they relate to EOCRC lifestyle related factors and cancer prevention behaviors.
Methods
We conducted a cross-sectional survey of college students at a public university. Measures included demographics, stress, family cancer history, and CRC knowledge. Previously validated measures for diet, sedentariness, smoking, alcohol consumption, and stress management assessed adherence with lifestyle prevention guidelines. HPV vaccination and skin checks appraised cancer prevention. Outcomes included perceived CRC risk (0%–100%) and CFC-Cancer adapted scale. Adjusted linear regression models examined CFC-Cancer and perceived CRC risk predictability.
Results
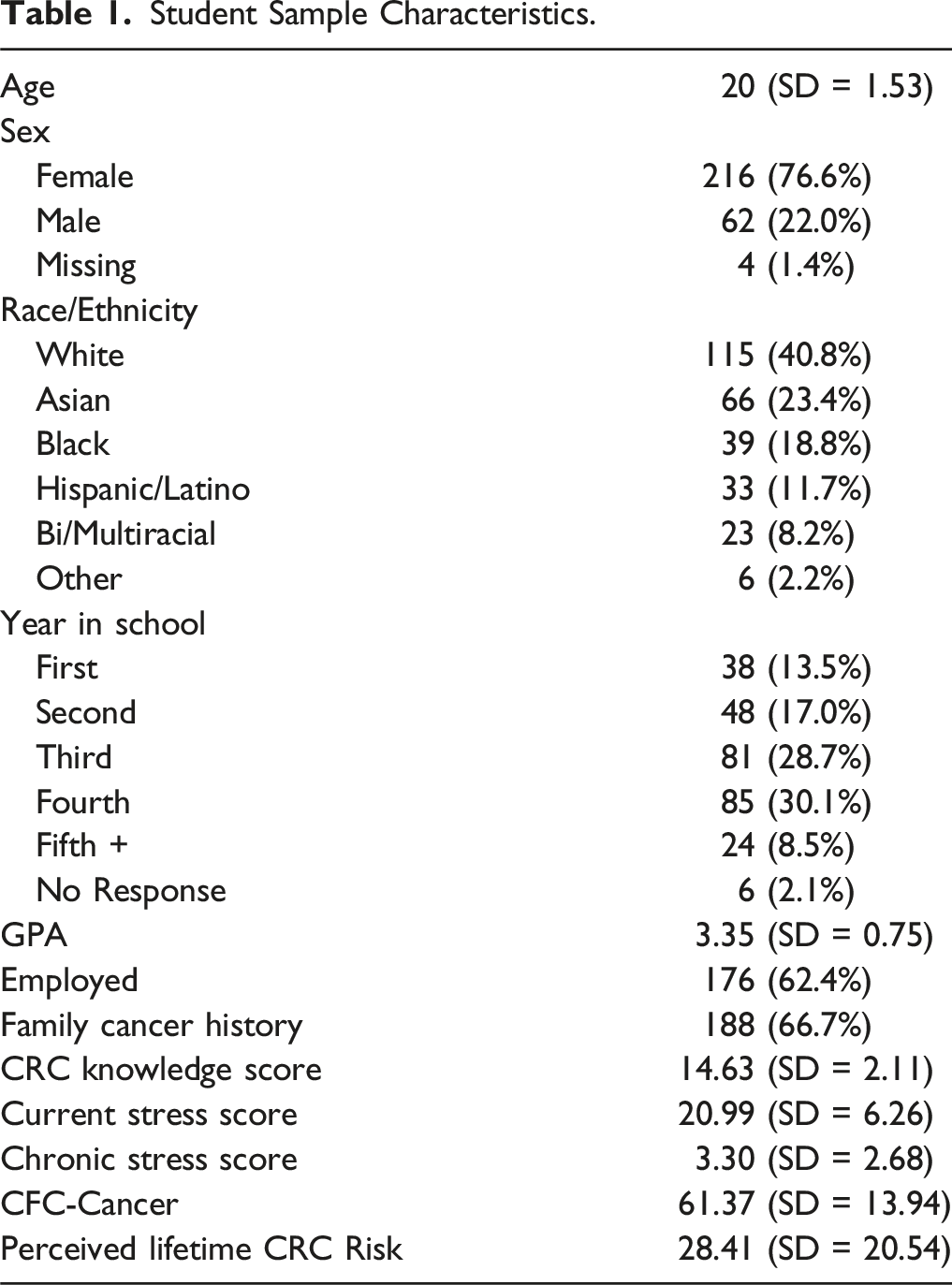
The sample (N = 282) mean age was 20 years, 77% were female, 40% were White, and 67% had family cancer history. CRC knowledge μ = 14, and current stress was moderate. 18% completed both cancer prevention behaviors, and protective lifestyle behavior scores ranged between 2-15, μ = 8. Perceived CRC risk = 28%, and CFC-Cancer was moderate (μ = 61). CFC-Cancer model included significant predictors of GPA, CRC knowledge, and lifestyle health behavior score, while Perceived CRC Risk model included age and being employed.
Conclusion
Emerging adults overestimate CRC risk but also have moderate CFC-Cancer. Accurate CRC knowledge provided to this age group may help redirect CRC health trajectories through integration of EOCRC protective lifestyle health behaviors and sustaining them into adulthood.
Introduction
Colorectal cancer (CRC) is increasingly diagnosed among younger adults not eligible for preventive screening. As many as 70% of early-onset colorectal cancer (EOCRC) cases have been linked to modifiable lifestyle factors. 1 CRC primary prevention encourages lifestyle integration of specific dietary and physical activity recommendations to reduce risk. 2 Precancerous cellular modifications begin as early as 10-20 years prior to CRC diagnosis. 3 Given this lengthy latency period, a CRC diagnosis made at age 45 would likely have mutation risk factors for colon polyps beginning as early as age 25-35. 3 Current CRC prevention efforts deploy interventions too late in life and focus on secondary (interception) rather than primary prevention. 4 Upstream, primary prevention that includes emerging adults (18-25 years) is needed for EOCRC risk reduction. 5
During emerging adulthood elevated autonomy contributes to some of the most substantial changes to personal lifestyle health behaviors. 6 At conclusion of second year in college, a pattern of decreased physical activity and food diversity, along with increased alcohol consumption and sedentariness has been identified when compared to high school behaviors. 7 Longitudinal studies show engagement in health behaviors (i.e., diet, exercise, sleep, screen time, smoking and alcohol consumption) often group together as low-,moderate-, or high-risk.6,7 College students who experience greater chronic stress and daily stressors have elevated risk for maladaptive health behaviors. 8 Furthermore these behaviors, protective and maladaptive, are sustained into adulthood and related to health outcomes. 6 In a cohort study, increasing leisure time physical activity between ages 20-24 years was associated with healthier diet, better sleep and overall self-rated health observed at age 60-64 years. 9 Thus lifestyle-related health behaviors established during this developmental stage shape trajectories for health outcomes including CRC.
Explorations of college student knowledge of cancer risk factors consistently find that students can correctly identify highly publicized health behaviors such as tanning, smoking, drinking alcohol, and HPV vaccination; but often miss dietary or sedentary risks.10-12 HPV vaccination is recommended at ages 11-12 years, and dermatologist endorse annual skin exams beginning around age 20. These are the only clinical cancer prevention guidelines for emerging adults addressed in medical appointments which may contribute to their knowledge and perceived importance. Preventive behaviors for cervical and skins cancers are predicted by self-efficacy and knowledge, and perceived importance among college students (skin checks only). 13 Among college females, those who had greater cancer worry or perceive breast cancer to be a serious health risk were more likely to engage in higher levels of physical activity. 12 Students overestimate their general cancer risk which has been partially attributed to highly visible communications such as the breast cancer pink ribbon campaign. 14
One mechanism that facilitates decisions to engage in preventive health behaviors is future orientation. 15 Future orientation is defined as “a time perspective that is focused on the future, especially on how to achieve one’s desired goals”.15,16 Consideration of future consequences (CFC) operationalizes future orientation as the extent to which one’s decisions are guided by future vs immediate consequences. 17 A meta-analysis identified that CFC predicts many lifestyle health behaviors among college students. 15 Future orientation also moderated the relationship between perceived stress and physical activity for students. 18 Both cervical and skin cancer prevention (i.e., HPV vaccination and sunscreen use) are positively related to CFC within this population. 15 Researchers adapted the CFC scale to assess proximal decision making in consideration of future health among college students and found that the new scale explained variance in diet and exercise behavior significantly more than general CFC scale. 19
Prior research explored associations between emerging adults’ CFC globally and cancer prevention behaviors for more proximal cancer concerns (i.e., cervical and skin); but has yet to investigate cancers traditionally considered a distal risk, like CRC. Given recent population trends and long latency of CRC, this risk may be less distal. Research on knowledge, perceived risk, and health behavior-based risk factors specific to CRC among this population is critical given EOCRC trends but is limited to date. Exploration of college students’ future orientation pertaining to CRC is needed to understand how their consideration of future cancer risk (CFC-Cancer) may be associated with current behaviors that direct CRC health trajectories during a critical life course stage.
The present study objective was to characterize emerging adult CFC-Cancer and lifetime perceived CRC risk and assess how they relate to EOCRC lifestyle related risk factors and clinical cancer prevention behaviors. We had two hypotheses (1) protective clinical cancer prevention and lifestyle health behaviors are positively associated with CFC-Cancer, and inversely associated with perceived lifetime CRC risk; and (2) CFC-Cancer and perceived lifetime CRC risk will covary with CRC knowledge, family cancer history, and stress.
Materials & Methods
Data Sample
The reporting of this study conforms to STROBE guidelines. 20 A random sample (N = 2100) of undergraduate students at a 4-year public institution were invited to participate in the study. Findings from a meta-analysis of CFC related to health promoting behavior [r = 0.09, (95% CI: 0.06-0.130, P-value <.001)] 21 were extrapolated and entered into nQuery software to calculate sample size needed for statical regression analyses with significance level α = 0.05 and 90% power, (N = 614). The sample pool (N = 2100) was calculated to model a prior web-survey study among college students that acquired a 30% response rate. 22 Eligible students for the sample were aged 18 to 25 years, enrolled full-time and English speaking. An encrypted file containing contact information (name and school email) was uploaded into REDCap.23,24 Students self-consented to the electronic survey via computer or mobile. A modified Dillman method that effectively improved Belgian college student survey response rates was utilized. 22 Invitations were delivered at the conclusion of the academic year, and non-responders received up to eight reminders from May to August. Reminder content included survey completion time, current number of participants, and progress towards response rate goal. Completers received $5 Starbucks gift card and entered into a randomized drawing of Amazon gift cards ranging $10-$20 to incentivize participation; gift cards were distributed by email.
Measures
Students reported their age, sex at birth, race/ethnicity, employment (yes/no), year in school (first-, second-, third-, fourth-, or fifth-year plus) and cumulative GPA. Current stress was evaluated with the Perceived Stress Scale; scores range 0-40, higher scores indicate greater perceived stress. 25 Chronic stress was appraised with the Early Life Stress Questionnaire, asking students whether they experienced 17 various adverse childhood experiences; scores range 0-17, higher scores indicate more early life stress. 26 NCI’s Screen to Save survey assessed CRC knowledge with 14 items for a score ranging 0-18 with higher score indicating greater knowledge. 27 Students were asked about having any family history of cancer (yes/no). Family history of cancer was asked broader than first-degree relative because knowledge of any family member with cancer may raise awareness.
Given that these are the only two clinical cancer prevention guidelines relevant to emerging adults we asked one item for each behavior as to whether they adhered (yes/no). Their responses summed for an aggregate cancer prevention behavior score ranging from 0 to 2.
Lifestyle health behaviors associated with EOCRC including diet, sedentariness, smoking tobacco, and alcohol consumption were assessed with previously validated self-report measures.28-30 Students were asked about frequency (i.e., Usually/Often, Sometimes, Rarely/Never) of meeting CRC protective dietary recommendations for fiber, fruits, vegetables, processed meats and fried foods. 28 Dietary behaviors were assessed for meeting CRC prevention guidelines by consuming ≥2 servings of fiber, fruits and vegetables per day and limiting processed meats and fried food. Total hours spent sedentary during waking hours ranging from 0 to 20 was reported. 29 One item assessed whether participants abstain from smoking tobacco products (yes/no). Alcohol consumption was measured with two items, number of days consuming ≥ 1 drink in prior 30 days, and number of drinks consumed on those days to calculate average drinks per day; heavy drinking behavior for females was identified as ≥ 1 drink/day, and for males ≥ 2 drinks/day. 30
Stress management and sleep were appraised as behavior-based constructs for controlling metabolic stress levels. 31 Nine items from the Inventory for assessment of stress management skills (IBSF) inventory of stress management skills were included to assess use of cognitive strategies, social support, and recognition of bodily tension to cope with stress, with higher scores indicating greater use of stress management behaviors. 25 The Brief Pittsburgh Sleep Quality Index was used to assess sleep latency, disturbance, and quality for a total sleep score ranging 0-12, with higher scores indicating better sleep. 32
Health behaviors were dichotomized as to whether current prevention guidelines for diet, 33 sedentariness, 34 tobacco smoking, alcohol consumption, 33 sleep 35 and stress management 31 were met and then summed together for an aggregate protective health behavior score.
Three scales were used to examine study outcomes of future orientation related to cancer, and perceived CRC risk. Consideration of Future Consequences (CFC) is a fourteen item scale that appraises immediate vs future-orientated patterns in decision making. 17 Each item has a seven-point Likert response ranging from 1 = ”Not at all like me” to 7 = ”Very much like me,” which are summed together (range of 14-95) with higher scores indicating more future-oriented. Based on prior success adapting CFC to be health specific (CFC-Health), 19 we adapted the CFC scale to assess future consideration of cancer risk (CFC-Cancer).
Perceived lifetime CRC risk was evaluated by asking participants to use a sliding scale of 0% to 100% to indicate what they thought their lifetime risk of developing colorectal cancer would be. This measure was effectively used previously in a study of adults that assessed accuracy of perceived risk. 33 The percent measure for perceived risk can be compared to NCI’s reported CRC risk for the general public, 4.1%. 36
Analysis
Missingness was appraised and identified 9.4% of participants with ≥1 scale item missing. Multiple imputations were administered for scale items. Data was normally distributed. Students were asked general CFC items and CFC-Cancer to assess performance of the new scale and we report on correlation between these scales. A manuscript further assessing performance of the CFC-Cancer scale is under preparation. Composite scores for protective clinical cancer prevention and lifestyle health behaviors were generated by dichotomizing whether the participant met current prevention guidelines for individual items and then summed. All variables were descriptively analyzed. Performance of CFC-Cancer was evaluated by Cronbach’s alpha and correlations with the original CFC scale. A Cronbach’s alpha >0.70 was deemed acceptable. 37
Categorical variables Sex and Race/Ethnicity were dummy coded in preparation of Pearson Correlation tests to determine associations between sociodemographic variables, CRC knowledge, family cancer history, stress, clinical cancer prevention and lifestyle health behavior scores with CFC-Cancer and perceived lifetime CRC. Linear regression models were conducted to test hypotheses that clinical cancer prevention and lifestyle health behaviors predict CFC-Cancer and perceived CRC lifetime risk. Significant sociodemographic variables, cancer history, CRC knowledge and stress were controlled for in full models. Statistical analyses utilized α = .05 to detect significance. SPSS 29 software was used. 38
Results
Student Sample Characteristics.
Correlation Tests for Outcomes of CFC-Cancer and Perceived Lifetime CRC Risk.

Clinical Cancer Prevention
Majority (72%) of the sample reported they had received the full HPV vaccination series. A sizeable proportion (17%) reported being unsure about their vaccination status. Less than a quarter (22%) reported participating in annual self- or healthcare provider skin examinations. Composite cancer prevention behavior scores ranged 0-2 with a quarter (25%) reporting neither behavior and 18% who reported completing both.
Lifestyle Health Behaviors
Dietary guideline adherence was as follows: fiber 35%, fruits 29%, vegetables 37%, processed meats 24% and fried foods 27%. A quarter of participants (23%) didn’t meet any CRC protective diet habits, and 20% met ≥3 of the guidelines. 41% met guidelines for preventive sedentary time. Majority (95%) reported ≥1 type of stress management behavior. Cognitive exercises including perspective, balancing thoughts, knowledge, ease or confidence in coping were reported among 83% of the sample, with 65% reporting more than one. Half (55%) reported they could rely on social support for help, and 63% were aware of bodily tension increasing under stress. Approximately 29% of students appraised their sleep quality as good, and 31% reported getting recommended ≥7 hours of sleep nightly. Among this sample only 7% met criteria for heavy drinking behavior, and the vast majority (83%) reported abstaining from smoking tobacco products. Composite protective lifestyle health behavior scores ranged 2-15, (μ = 8, SD = 3) and Cronbach’s alpha was 0.65.
Consideration of Future Cancer
CFC-Cancer had a range = 21-95, (μ = 61.4, SD = 13.9) among the student sample. CFC-Cancer had a significant correlation with the CFC-General (r(282) = 0.63, P < 0.001), and yielded a higher Cronbach’s Alpha (α = 0.87) compared to CFC-General (α = 0.84). These results indicate that the adapted CFC-Cancer scale has convergent validity and greater consistency compared to CFC-General. Correlation tests with sociodemographic variables and stress exposure identified significant associations with GPA (r(282) = 0.2, P < 0.01) and current perceived stress (r(282) = -0.2, P < 0.001). CFC-Cancer model would be adjusted for GPA, while also controlling for Cancer History, CRC knowledge and current stress to explore associations with healthy lifestyle behaviors and cancer preventive behaviors in a linear regression model.
Perceived Lifetime CRC Risk
Perceived lifetime CRC risk had a wide range, 0-100, and (μ = 28.4, SD = 20.5). Average perceived lifetime CRC risk among students was 28.4%. Perceived risk had significant correlations with age (r(282) = 0.2, P < .001), school year (r(282) = .2, P = .002), employment status (r(282) = 0.2, P < .001), and current perceived stress (r(282) = 0.1, P = .03). Age and year in school had a positive association (r(282) = .7, P < .001), thus we included age in the final model since it had a slightly stronger association with perceived lifetime CRC risk. Thus, perceived lifetime CRC risk model was adjusted for age, and employment status; control variables included Cancer History, CRC knowledge, and current stress, and independent variables lifestyle health behavior and cancer preventive behavior scores.
Full models
Significant Linear Regression Model Parameter Estimates for CFC-Cancer and Perceived CRC Risk.

***P-value <.001, **P-value < .01, *P-value < .05.
aCFC-Cancer model was adjusted for GPA.
bPerceived Lifetime CRC Risk model was adjusted for Age and Employment.
The full perceived lifetime CRC risk model is significant, F(7) = 4.54, P < .01. Again, current perceived stress was not a significant predictor of perceived CRC risk with the other variables present. Age and work status were the only significant predictors; perceived lifetime CRC risk = .34(employment)+2.52(age). Perceived lifetime CRC risk score increased by .34 if students were employed, and 2.52 for each increase in age. Parameter estimates are displayed in Table 3.
Discussion
In this cross-sectional survey of emerging adults attending college, we found that students have moderate consideration of their future cancer risk when making health behavior choices (i.e., CFC-Cancer), but overestimate their lifetime CRC risk. Our hypothesis that protective lifestyle health behaviors would be a significant predictor was correct for CFC-Cancer but not perceived lifetime CRC risk. Clinical-based cancer prevention behaviors were not significantly associated with either outcome. As we predicted, CFC-Cancer and perceived CRC risk covaried with CRC knowledge and current perceived stress, but not with family cancer history. In our final adjusted models, perceived stress was not significant in the presence of other factors; but CRC knowledge remained a significant predictor for CFC-Cancer.
Students had a wide range of perceived risk (0%-100%). On average participants perceived they had a 28% chance of CRC in their lifetime; this is seven times greater than general lifetime CRC risk (4%) based upon NCI data trends. 36 Incongruence between perceived lifetime risk and actual prevalence of cancer, cardiovascular disease, diabetes and obesity has been observed among college students before. 14 It’s suggested that highly visible breast cancer campaigns may contribute to female students estimating they are more likely to get cancer than heart disease, the leading cause of death among women. 14 Younger age predicted higher perceived CRC risk in other studies.39,40 CRC communications target those of screening age eligibility and consequently younger populations may be less informed about prevalence and overestimate risk. It’s possible that younger individuals see many years of life left or recall stories of younger celebrities who have been diagnosed and/or died from CRC, and perceive greater CRC risk compared to someone with fewer years left of life. Upperclassmen perceived a greater risk of developing CRC in this study, and for cardiovascular disease 41 and diabetes 42 in other studies. Further investigation is needed to understand upperclassmen experiences that may foster greater apprehension of cancer and chronic diseases. The top three concerns among students include academic performance, pressure to succeed and post-graduation plans 43 ; it may be that the approaching conclusion of studies realigns concerns for upperclassmen to include one’s health.
Lifestyle behaviors did not predict perceived CRC risk among our sample of emerging adults, a finding similar to a recent study of middle-aged adults (45+ years) 40 ; however behaviors did predict CFC-Cancer. Students reporting more protective behaviors were more future orientated to reduce cancer risk when navigating health-related decisions. Overall, the sample had moderate consideration for their future cancer risk, which is significant considering that overall health ranks seventh among student concerns. 43 As of 2018, roughly 22% of those age 18-26 had completed HPV vaccination, 44 in our sample completion rate was 75% which may reflect that our college student sample had moderate CFC-Cancer. Our results suggest that while health may not be a main concern for students, they do still consider their future cancer risk when making choices which may limit the generalizability of our findings to college enrolled emerging adults. This supports investment in EOCRC efforts to improve lifestyle related health behaviors of college students which will also positively influence students’ cancer-related future orientation and hopefully alter their health trajectory.
Lifestyle health behaviors are sensitive to stress as individuals’ use exercise, eating, smoking and alcohol consumption as coping mechanisms 45 and college students are not immune to this effect. 8 It’s been recommended that lifestyle behavior interventions should include stress management given this relationship. 45 Perhaps because our lifestyle health behavior variable included appraisal of stress management techniques we identified that perceived stress was not a predictor of CFC-Cancer in the presence of protective lifestyle health behaviors. This suggests that students still consider future cancer risk when navigating health behavior decisions regardless of current or chronic stress and reinforces the argument that lifestyle health interventions should integrate stress management.
Limitations
The survey response rate was low but aligns with cross-sectional web-survey participation rates for college students which are averaging less than 20%. 22 For example, the National College Health Assessment utilizes a stratified random sample and averages an 11% response rate across institutions. 46 Distribution at the end of the academic year may have contributed to lower response rate. While low sample size can limit generalizability our demographic and CFC cancer results indicate that we successfully enrolled students with varying levels of cancer prevention orientation and were aligned with key demographics of sex, year in school and race. 47 Moreover, the high racial and ethnic diversity among participants was a major strength. Given timing of the survey, self-reported health behaviors and perceived stress may not reflect those constructs under influence of student obligations during the academic year which would alter our predictive models. Self-report measures may over- or under-estimate lifestyle health behaviors; however, the study was intentional in selection of previously validated instruments tested among college students. Future studies could benefit from objective measures using ecological momentary assessments, wearable devices and/or biometrics during the academic year. Education level has been identified as a risk factor for CRC, those with higher education are less likely to have a CRC diagnosis. 48 The present study utilized college enrolled emerging adults and thus their educational background may be a possible moderator for perceived CRC risk and CFC-Cancer. To increase generalizability of findings, a sample of emerging adults not aligned with college attendance should be used in the future to assess whether outcomes differ based on educational experiences that afford access to and opportunities to engage with health knowledge.
Conclusion
The life course paradigm proposes that 1) the longer someone engages in preventive behavior the greater likelihood it will be sustained, and 2) younger adults have greater likelihood of initiating preventive health behaviors through social transitions. 49 The present study’s findings about CFC-Cancer justify a paradigm shift for CRC primary prevention to adopt a life course perspective and introduce strategies to reframe cancer prevention orientation during emerging adulthood when individuals experience some of the greatest life transitions. This period is a critical time for intervention given neuroplasticity and brain development of cognitive processes, including CRC risk behavior modification, reaches maturation around age 25. 50 Current CRC prevention efforts happen too late 4 by focusing on screening, a secondary rather than primary prevention approach. CRC knowledge is a significant predictor for cancer prevention future orientation which is associated with protective lifestyle health behaviors, and thus evidence-based strategies to improve knowledge could reduce CRC risk. Recently, a cancer health education program yielded significant improvement in cancer knowledge, lifestyle health behaviors, cancer fear/fatalism, and family discussions about health among high school students 51 ; this program could be replicated more broadly in school settings, including higher education since we found that perceived CRC risk increases with age. CFC-Cancer is moderate during this life stage and thus if emerging adults are provided with accurate knowledge of how to reduce risk it is likely they will implement and sustain those practices into later adulthood. Notably, given that EOCRC modifiable lifestyle risk factors are common with many chronic conditions there would a significant public health impact with effective prevention strategies for emerging adults.
Footnotes
Consent Statement
The study was exempt status, student participants were provided a research information form and self-selected to consent to participate with the electronic survey.
Author Contribution
J. Knight Wilt designed and implemented the research study, performed the analyses and wrote the manuscript in consultation with MD. Thomson. MD. Thomson verified analytical methods and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Irb Review Statement
The Institutional Review Board at Virginia Commonwealth University determined the study to be exempt status (HM20026461).