
Abstract
Introduction
Gastric cancer (GC) is still a great threat to human health worldwide 1 ; although its incidence and mortality rates have steadily declined in China, 2 the 5-year overall survival (OS) rate is still less than 50% for patients with stages greater than IIA, even those who receive surgical treatment. 3 Radical resection with D2 lymphadenectomy is still the mandatory backbone in management of the disease with curative intent 4 ; however, postoperative complications such as infection are unavoidable 5 and can greatly impair the long-term OS of patients. 6
The use of antibiotic (Abx) is a standard method to decrease postoperative infection in patients who undergo gastrectomy7-9; however, there is still a lack of consensus on the type and duration of Abx use in such a scenario. In general, patients are administered these agents within 24 h before surgery and for 3-7 days (d) after the operation.7-9 Interestingly, accumulating evidence has indicated that the use of ABX in locally advanced or metastatic malignancies is negatively correlated with survival.10,11 A plausible explanation for this finding is that the use of Abx can cause significant dysbiosis of the gut microbiota, which is a key player in controlling anticancer immunity12,13 and in regulating cancer cell proliferation, 14 metastasis, 15 drug resistance 16 and other processes. 17 However, the prognostic value concerning the use of Abx in gastrointestinal cancers is controversial. For example, exposure to Abx correlated with poor survival in metastatic colorectal cancer (CRC) patients who received bevacizumab-based chemotherapy 18 ; in contrast, Abx treatment reportedly improved treatment efficacy in advanced CRC patients who received oxaliplatin-containing regimens. 19 However, this correlation was eliminated in metastatic CRC patients who were characterized as MSI-H/dMMR and who received immune checkpoint blockade therapies. 20 In line with these findings, another study indicated that Abx therapy can contribute to good treatment efficacy in advanced GC patients receiving oxaliplatin-based chemotherapy. 21 Nonetheless, all these studies were conducted in advanced or metastatic settings, and the prognostic value of the use of Abx during surgery is still largely unknown.
In this context, we aimed to test the associations of the cumulative dosage of Abx and multiple Abx types with outcomes in stage I-III GC patients.
Methods
Patients
The data of consecutive patients with gastric adenocarcinoma who underwent radical resection at Hainan Hospital of PLA General Hospital from December 2012 to June 2019 were collected retrospectively. Patients who received preoperative adjuvant therapies, had preoperative active infections and had received any kind of Abx, had a long history of glucocorticoid use for any comorbidities, had signs of remote lesions according to preoperative imaging examinations, had any missing data for TNM information in postoperative pathological reports, had in situ or stump lesions, or had follow-up problems were excluded. Clinical data, including age (<60 years [y] vs ≥ 60 years), sex (female vs male), surgery (laparoscopy vs laparotomy), total gastrectomy (yes vs no), pathological differentiation (poor vs good + moderate), and smoking/drinking history (yes vs no), were also collected from the archived digital medical records. Additionally, data concerning the use of proton pump inhibitors (PPIs, including lansoprazole, omeprazole and its derivatives, pantoprazole, and rabeprazole) during surgery were also collected. The study was supervised by the ethics committee of Hainan Hospital of PLA General Hospital. Written or oral informed consent was not needed since it was conducted retrospectively with anonymized data, according to the national legislation. All patient details were de-identified. The reporting of this study conforms to STROBE guidelines. 22
Collecting the Inflammatory Cell Count in Pre- and Postoperative Peripheral Blood Tests
The data concerning inflammatory cells, including the absolute white blood cell count (WBC), absolute neutrophil count (N), absolute lymphocyte count (L), absolute monocyte count (M) and absolute platelet count (PLT), were collected from peripheral blood tests preoperatively (within 1 week before surgery) and postoperatively (2 weeks to 1 month [m] after surgery) according to previously reported methods. 23
Collection of Abx Data, Including the Cumulative Defined Daily Dose (cDDD) and Type
The cDDD and type of Abx were collected from the archived digital medical records for patients before discharge. cDDD was calculated as the sum of each individualized Abx multiplied by the defined daily dose (DDD), divided by the length of hospitalization (d).
Statistical Analysis
OS was set as the primary endpoint for the study because of its importance in clinical studies, 24 and the follow-up procedure was conducted as previously described. 25 Patients were divided into low- or high-cDDD subgroups and ≤2- or ≥3-type subgroups according to the median of these data. The differences in the collected clinical data among these subgroups were calculated via the χ2 test or Fisher’s exact test for categorical variables and by independent samples t tests or Mann‒Whitney U tests when the data did not fit a Gaussian distribution for continuous variables. OS differences in these subgroups were checked by Kaplan‒Meier (K‒M) survival analysis followed by log-rank tests. Risk factors for OS were validated by a Cox proportional hazards model. All the data were processed by using SPSS 20.0 (SPSS Inc., Chicago, IL, USA), and a two-sided P value ≤0.050 was considered statistically significant.
Results
Basic Features of the Patients
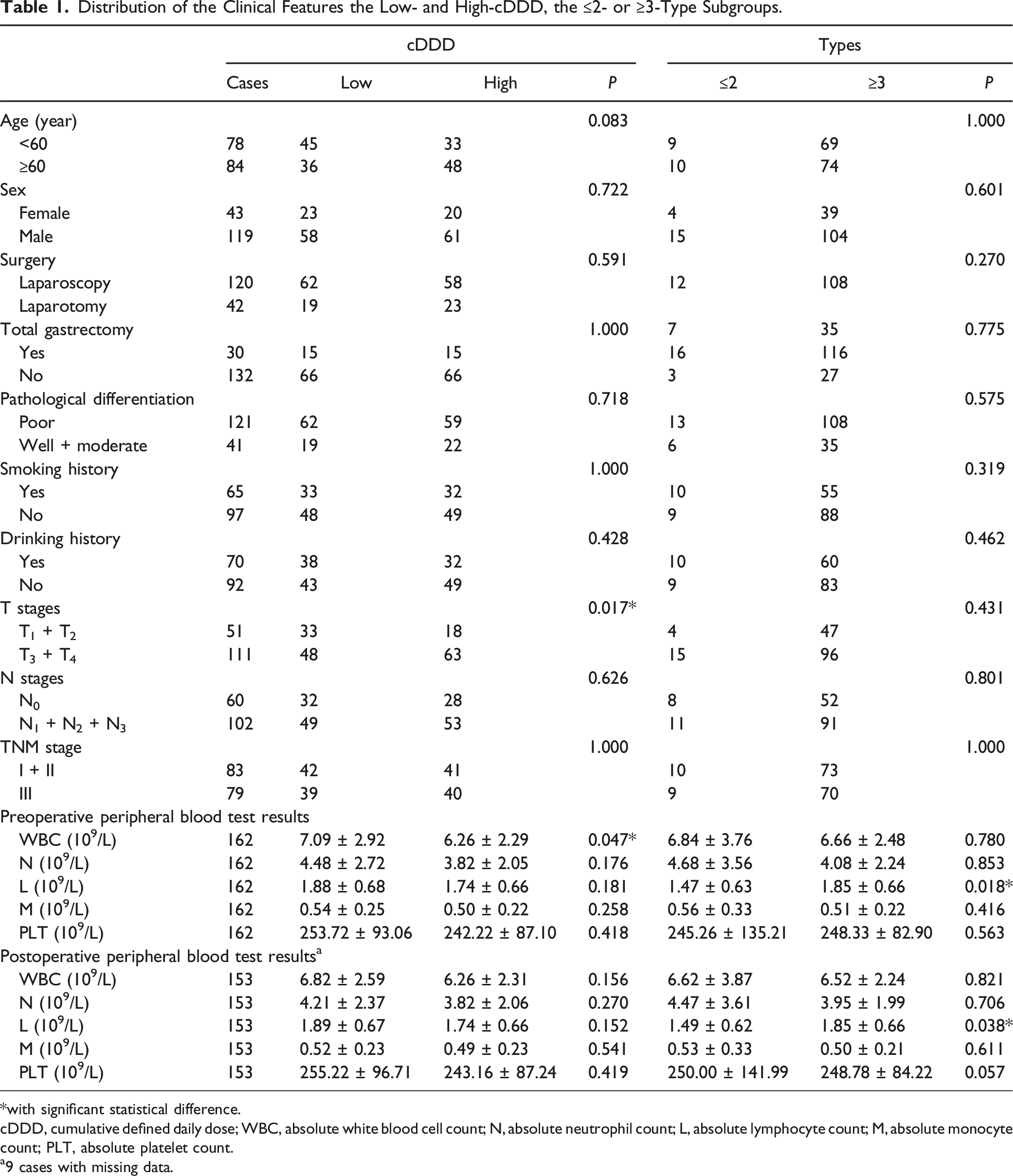
A total of 162 patients were included in the final dataset (Figure 1), which included 43 females and 119 males. The median age of the patients was 60 years (range: 26-94 years), and the median follow-up was 46.5 months (range: 3-132 months). At the termination of the study, 2, 12 and 52 patients in stages I, II and III died, respectively. The median length of hospitalization was 23.5 days (range: 10-81 days). With respect to the PPIs, 147 patients took at least 1 kind of PPI with a median dosage of 600 mg (range: 0-2670 mg), and 15 patients took none of these agents. The median cDDD was 7.22 (range: 0.69-23.18), and the median number of types was 3. Specifically, 3 patients received only 1 type; 16 patients received 2 types; 68 patients received 3 types; 50 patients received 5 types; and the remaining patients received more than 5 types. With respect to individual type, macrolides (mainly erythromycin) with vs without: 137 vs 25; fluoroquinolones (levofloxacin and moxifloxacin) with vs without: 144 vs 18. On the basis of the median cDDD and number of types, 81 patients were assigned to the low- and high-cDDD subgroups, and 19 and 143 patients were assigned to ≤2 or ≥3 Abx type subgroups. As shown in Table 1, no significant difference was found in the collected clinical data between the low- and high-cDDD subgroups the ≤2- or ≥3-type subgroups, except that patients in the low-cDDD subgroup had significantly greater WBC counts than did those in the high-cDDD subgroup, and the ≥3-type subgroup presented significantly greater preoperative and postoperative L counts than did the ≤2-type subgroup. The Inclusion and Exclusion of the Patient Distribution of the Clinical Features the Low- and High-cDDD, the ≤2- or ≥3-Type Subgroups. *with significant statistical difference. cDDD, cumulative defined daily dose; WBC, absolute white blood cell count; N, absolute neutrophil count; L, absolute lymphocyte count; M, absolute monocyte count; PLT, absolute platelet count. a9 cases with missing data.
Survival Differences Among the Low- and High-cDDD and the ≤2- or ≥3-Type Subgroups
K‒M survival analysis revealed that in the whole dataset, patients in the low- and high-cDDD subgroups (log rank = 2.21, P = 0.137) had no significant difference in OS, but the ≤2- and ≥3-type subgroups (log rank = 4.58, P = 0.032) did show significant difference (Figure 2A and B). Next, we divided patients into 2 subsets with and without total gastrectomy and tested the differences in OS. The results indicated that in patients who underwent total gastrectomy, the low- and high-cDDD subgroups (log rank = 3.83, P = 0.050) but not the ≤2- and ≥3- type subgroup (log rank<0.001, P = 0.982) presented a significant difference in OS (Figure 2C and D). However, in patients who did not undergo total gastrectomy, the difference in OS was significant between both the low- and high-cDDD subgroups (log rank = 7.92, P = 0.005) and the ≤2- and ≥3-type subgroups (log rank = 6.52, P = 0.011) (Figure 2E and F). In addition, we also investigated the differences in OS among specific types, including macrolides and fluoroquinolones. The results indicated that patients treated with macrolides tended to have better OS (log rank = 3.54, P = 0.060); however, no such trend was found for treatment with or without fluoroquinolones (log rank<0.01, P = 0.978) (Figure 3). OS Differences Among cDDD Low or High Subgroups in the Whole Cohort (A); in Patients With Total Gastrectomy (C); in Patients Without Total Gastrectomy (E); OS Differences Among ≤2 or ≥3 Types Subgroups in the Whole Cohort (B); in Patients With Total Gastrectomy (D); in Patients Without Total Gastrectomy (F) OS: Overall Survival; cDDD: Cumulative Defined Daily Dose. OS Differences Among Patients With or Without macrolides (A), fluoroquinolones (B) OS: Overall Survival.

Risk Factors for OS Validated by Univariate and Multivariate Analyses
Validation of the Risk Factors for OS by Univariate and Multivariate Analyses.

*with significant statistical difference.
cDDD: cumulative defined daily dose.
Discussion
In this study, we found that prophylactic Abx use during surgery was a significant predictor of OS in stage I-III GC patients. Notably, cDDD and multiple Abx types presented opposite indicator functions in predicting the outcome; patients with ≥3 types of Abx displayed significantly better OS than those with ≤2 types of Abx, particularly among patients who did not undergo total gastrectomy. More importantly, type was identified as an independent risk factor for OS. To the best of our knowledge, this is the first report concerning the prognostic value of Abx use in GC patients in such a scenario.
In recent years, investigations on the correlation of Abx use with survival in cancer patients have become increasingly popular, and many studies have indicated the negative role of these agents in many malignancies,10,11 with the exception of hepatocellular carcinoma26-28 and CRC. 19 However, the algorithms used to define Abx use in these studies are notably heterogeneous. For example, patients with any duration and type of Abx exposure were taken into account in those who received immune checkpoint blockade therapies for non-small cell lung cancer; however, the initial point for Abx exposure was intricate and included 21 d before or after, 29 30 d before or after, 30 30 d before,31,32 30 d after, 33 and 60 d before and 30 d after34,35 the start of the treatment. Similar examples were also reported for CRC18-20 and GC. 21 In addition, other studies have considered the duration of Abx treatment18,36,37 or specifically focused on certain types of Abx.38,39 These studies may be limited in reflecting the truth of Abx exposure, since the duration and types of Abx exposure in the clinic can be very complicated. Interestingly, some studies have adopted cDDD as an index of Abx exposure when investigating the causal relationship between Abx use and cancer initiation.40,41 In fact, DDD is a unit of comparison for drug statistics according to recommendations by the World Health Organization, and the cumulative value of this index can be a good indicator of actual Abx use in practice. In our study, we used cDDD as an index of the cumulative dosage of each Abx and its duration. The results indicated that cDDD could serve as a potential prognostic marker in the whole cohort (P = 0.137) and was particularly efficient in patients who underwent total gastrectomy (P = 0.050), which was partially consistent with the findings of a previous study. 38 We believe its usefulness could be further validated in other malignancies in the future.
Mechanically, dysbiosis of the gut microbiota is thought to be the imminent cause of poor survival in cancer patients exposed to Abx, as an increasing number of reports have indicated that these dysbiotic microbiomes play a vital role in controlling anticancer immunity, which includes impairing T-cell immunity 42 and modulating the trafficking of these cells into lesions 43 as well as clusters of T regulatory and plasmacytoid dendritic cells in the microenvironment 44 ; moreover, these microbiomes contribute directly to cancer cell proliferation, 14 metastasis, 15 treatment resistance 16 and others. 17 Notably, short-term Abx treatment, 44 let alone long-term therapeutic regimens, 45 can have a long-lasting effect on these microbiomes in some patients. In our study, cDDD reflects the cumulative dosage and serves as a useful label for the strength of Abx exposure, and it was found to be positively correlated with the severity of dysbiosis of the microbiomes in the gastrointestinal tract. 46 Notably, the use of multiple types of Abx is conventionally regarded as a risk factor for an imbalance in the normal gut ecological state in practice. 47 From this perspective, both cDDD and type should be considered in the prediction of outcomes in these patients, but this approach is inconsistent with the findings of our study. We believe that the underlying explanation could be attributed to Helicobacter pylori (H. pylori) infection in GC. H. pylori infection has long been known to play a key role in promoting GC initiation, progression and metastasis.48,49 Persistent H. pylori infection can not only attenuate the efficacy of immunotherapy in advanced GC patients50,51 but also correlate with poor survival in GC patients who undergo radical resection. 52 Accordingly, eradication of the gut microbiome can effectively prevent postoperative recurrence in early GC patients and is associated with a good prognosis.53,54 Notably, the prevalence of H. pylori infection in noncardiac GC (NCGC) is as high as 66.5%, and its seroprevalence can exceed 92% in GC in China.55,56 Coincidentally, according to the expert consensus in Shanghai (2019), a 10-14 day quadruple Abx strategy with a gastric acid inhibitor was recommended for the eradication of H. pylori, 57 which was more or less in line with the use of multiple Abx types in our study. On the basis of these data, it is plausible that the multiple Abx types in our study could lose their positive value in patients with total gastrectomy and that the cDDD could then be a more robust prognostic indicator, whereas the protective role of multiple Abx types in patients without total gastrectomy can be preserved, as in line with previous studies.53,54
In addition, the role of Abx in cancer patient prognosis may also be attributed to their ability to reduce systematic inflammation. 11 It was found that in CRC, the use of Abx, which was mainly prophylactically, can clearly decrease the WBC and N counts during the postoperative period. 58 In our study, patients who received multiple types of ABXs presented relatively low WBC counts and N values (a similar trend was not observed between the cDDD subgroups), which was in line with the findings of a previous study. 59 In particular, these patients had persistent high L values both preoperatively and postoperatively, which was also supported by previous studies showing that patients with high L values in such a scenario can have significantly better OS.59,60
Our study has several clinical applications. First, as some studies have attempted to demonstrate the safety of short-term 9 or no prophylactic Abx 61 (equivalent to a relatively low cDDD in our study) in preventing postoperative infections in GC patients who have undergone surgery, our results suggest that such a strategy should be cautious for total gastrectomy patients; second, taking into consideration the recommendation for H. pylori eradication in China, 57 it would be better for GC patients without total gastrectomy to receive multiple types of Abx (at least 3 types; however, Abx types with high resistance, including metronidazole, levofloxacin, and clarithromycin, should be avoided, 62 and macrolides might be a preferred options according to our study) during surgery with a controlled cDDD but with a balance to prevent postoperative infection. In addition, as some previous studies have indicated that cephalosporins or other beta-lactamase inhibitors, in particular, with a relative extended duration, played an important role in reducing postoperative infections, these types of Abx can also be an alternative option.63,64 Third, it was notable that some other complications, such as surgery-induced sarcopenia are of high prevalence in these patients (32.93% according to a report 65 ), which was closely correlated with postoperative infections and poor outcomes.66,67 Building on these data, it was not only that these patients should be routinely consulted with multidisciplinary oncology group to receive enhanced recovery after surgery-based nursing or additional parenteral nutrition support,68-70 but other approaches should also be highlighted, such as the use of Abx. Nonetheless, these applications would be more convincing if the effects could be validated in randomized controlled trials in the future.
Our study also has several limitations. First, owing to its retrospective nature and relatively small sample size (of note, the sample size of present study did not underwent calculation and justification), particularly for patients with total gastrectomy (n = 30), without macrolides (n = 25), or without fluoroquinolones (n = 18), some bias cannot be excluded satisfactorily and the conclusion may not be exclusive. Second, it was notable that some Abx may play an important role in manipulating the cancer cells directly. Taken fluoroquinolones as an example, it was reported that moxifloxacin can led to S-phase arrest and enhance cisplatin-induced cell apoptosis in pancreatic cancer 71 or it can suppress tumor growth in breast cancer. 72 In addition, levofloxacin can inhibit cell proliferation and increase cell apoptosis in lung cancer. 73 Although not validated in gastric cancer, these data suggested another explanation for the positive role of Abx in prognosis in our study; however, due to the multiple uses of these agents in practice, it was impossible to deduce an exclusive conclusion in our study. Third, although the prevalence of H. pylori infection in China is very high, 55 we still lack the relevant data for this study, and thus our deduction regarding the underlying mechanisms for the prognostic value of cDDD and multiple types in patients cannot be well supported. We advocate that offering tests for HP infection, such as rapid urease tests, to these patients should be mandatory in the future.
Conclusion
Overall, our study is the first to indicate that Abx use during surgery in patients with stage I-III GC may potentially correlate with the prognosis. Patients who received ≥3 types of Abx were more likely to have good outcomes, particularly in those without total gastrectomy.
Footnotes
Ethical Statement
Author Contributions
Lijuan Ding was responsible for the conception of the work; Lijuan Ding, Xiaoming Zhang and Qianwen Ye obtained the data; Lijuan Ding, Mengyu Zhou and Jiahui Yin analyzed, wrote the manuscript. Niansong Qian critically revised the manuscript. All of the authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key Research and Development Projects of Hainan Province (grant no. ZDYF2023SHFZ117) and Beijing Science and Technology New Star Program Cross-cooperation Project (grant no. 20240484544).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated or analyzed during the current study are available from the corresponding author (Niansong Qian) on reasonable request.