
Abstract
Background
In the global scenario of public health, cervical cancer poses a major threat with high mortality rates, especially in women. New incidence cases and prevalence vary across different regions, as recently shown by GLOBOCAN data. The development of cervical cancer is primarily due to persistent infection by high-risk genotypes of human papillomavirus (HPV), which is a multifaceted process that is influenced by genetic, environmental, and lifestyle factors.
Purpose
The goal of this study is to thoroughly investigate cervical cancer, including its etiology, molecular mechanisms, progression, diagnosis strategies, and current therapies. This review further highlights the transformative power of HPV vaccination and screening programs in curbing the disease’s burden and potentially promising novel approaches like immunotherapy and targeted therapy.
Research Design
This is a narrative review article that summarizes previous literatures regarding cervical cancer in terms of molecular mechanism, etiology, clinical developments, and prevention.
Study Sample
The review encompassed studies from diverse sources, including experimental, observational, and clinical research published between 1992 and 2025.
Data Collection and/or Analysis
Data were collected through comprehensive literature searches using databases such as PubMed, Scopus, and the Cochrane Library with defined inclusion and exclusion criteria.
Results
Nonetheless, there are gaps in research and controversies regarding vaccine coverage, screening practices, and treatment accessibility for poor populations. Precision medicine trends are emerging along with new biomarkers for early detection and personalized treatment, which also form part of this discussion. Key findings include the critical role of prevention measures in controlling the global impact of cervical cancer.
Conclusions
The paper synthesizes the existing knowledge and identifies gaps that require further research, which is significant in augmenting prevention, diagnosis, and treatment of cervical cancer towards addressing its public health implications worldwide.
Plain Language Summary
This review addresses the critical global health challenge of cervical cancer, emphasizing its molecular mechanisms, epidemiology, and innovative therapeutic approaches.
Introduction
Cancer still remains a tremendous global challenge, making it one of the major impacting illnesses for millions of people in the world as well as healthcare settings. In addition to causing huge emotional and physical stress on patients as well as their families, the treatment and research costs are also high. Having a sensitive perspective on what constitutes cancer and how it develops is crucial for both medical practitioners and ordinary people. 1
Cancer is a complex group of diseases characterized by uncontrolled growth and spread of abnormal cells. 2 Normally, cells grow and reproduce in well-organized patterns, but when this regulatory mechanism breaks down, it leads to an accumulation of mutations and the development of neoplasms or malignant tumors. Malignant tumors invade nearby tissues and can spread through metastasis, increasing the fatality rates. 3 Cancer originates from changes in the DNA sequence within cells, with genes providing instructions for functioning, growth, and division. Erroneous instructions cause cancer if not corrected, leading to uncontrolled growth. 4 Environmental factors like tobacco smoke, chemicals, and ultraviolet light, along with internal factors like inherited mutations, hormone levels, and immune conditions, can provoke carcinogenesis. 5 Experts have identified over one hundred different forms of cancer, based on the cell type it originated from, though many share similar processes. Understanding cancer’s mechanisms is crucial for developing treatment opportunities and prevention techniques. This ongoing research enhances our understanding and suggests new avenues for managing and treating cancer. 6
Cervical cancer develops in the cervix, the lower part of the uterus that links it to the vagina. This is one of the most common varieties of cancer that occurs among women all over the world and consequently heavily influences the health of the public. The key factor leading to cervical cancer development is persistent high-risk human papillomavirus (HPV) infection. In some cases, if not removed by the immune system, such infections may lead to a cellular alteration in the cervix, resulting in cancer in the long term. A woman who has contracted an HPV infection will require at least 15 to 20 years before being diagnosed with cervical cancer.
7
Cervical cancer mainly develops from chronic HPV infection with high oncogenic risk types, mainly HPV 16 and HPV 18. The molecular mechanism suggests the fact that HPV DNA gets integrated into the host genome and the expression of viral oncoproteins E6 and E7 occurs (Figure 1). These oncoproteins, therefore, interfere with the control mechanisms of cells by being able to neutralize proteins that are capable of inhibiting tumor formation—p53 and Rb. Mutation of p53 results in the inhibition of apoptosis and thus the resulting increase in genetic mutations, while the degradation of Rb consequently leads to uncontrolled cell division and cellular proliferation. In the same regard, E6 and E7 affect other cellular pathways, which include support of genomic instability, angiogenesis, and organization of escape from the immune system. Mechanism by which HPV Disrupts Critical Cellular Processes to Promote Cancer Development Through its Viral Oncoproteins E6 and E7.
These molecular changes play a part in changing normal cervical epithelial cells to malignant ones, hence leading to the development of cervical cancer. 8 Cervical precancerous conditions are diagnosed, and it becomes possible to treat them through the screening tests, such as Pap smears and DNA HPV tests; thus, rates of cervical cancers and mortality are reduced in countries where effective screening programs are established. 9 Brisson and colleagues hypothesize that the use of preventive HPV vaccines has been more helpful in stopping HPV infection, which led to a dramatic decline in the cases of cervical cancer among women, achieving public health programs against it. 10 On the other hand, these developments have proven to be more challenging in the low- and middle-income countries (LMICs) that have limited access to the vaccines against HPV and the procedure to screen for cervical cancers. The role of early detection and treatment is highlighted to the point of progression of disease from precancerous lesion to malignant cancer. Cervical cancer management is stage-related to diagnosis and may involve surgery, radiotherapy, or chemotherapy, as per the studies conducted by Pfaendler and colleagues. 11
To reduce the global burden of cervical cancers, ongoing research and international cooperation are very important. This includes increasing access to preventive vaccines and enhancing screening and treatment programs, among other things, for example, reducing inequalities in cervical cancer incidence and mortality worldwide. This review specifically aims to provide a comprehensive discussion on the factors that contribute to the development of cervical cancer, the related molecular processes, and the course of the disease, diagnostic approaches, and existing treatment modalities. It also underlines the changes brought by HPV vaccinations and screening programs on the epidemiologic profile of the disease and discusses newer treatment modalities, including immunotherapy and targeted therapy. Issues regarding research limitations, debate on coverage, screening, and access to treatment for the underprivileged are raised. New advancements in individualized medicine and novel biomarkers about early diagnosis and therapy are outlined to improve the prevention, diagnosis, and treatment of cervical cancer to reduce its global health burden.
Methodology
This is a narrative review article that summarizes previous literature regarding cervical cancer in terms of molecular mechanism, etiology, clinical developments, and prevention. The aim is to provide a comprehensive, interpretative synthesis of evidence from diverse sources, including experimental, observational, and clinical studies, to contextualize current knowledge and identify gaps.
Eligibility Criteria
Scope
• Studies addressing cervical cancer etiology, HPV pathogenesis, molecular biomarkers, screening, therapies, prevention, or epidemiology. • Peer-reviewed articles, clinical guidelines, and authoritative reports (e.g., WHO, GLOBOCAN). • Emphasis on high-impact studies published between 1992-2025.
Exclusion
• Non-English studies, case reports, and opinion pieces without empirical data.
Information Sources & Search Strategy
Databases such as PubMed, Scopus, and the Cochrane Library were broadly searched to identify seminal and recent studies. A combination of Boolean operators (AND/OR) and MeSH terms refined the search. Search terms included combinations of keywords such as “cervical cancer,” “HPV,” “molecular mechanisms,” “epidemiology,” “screening,” “immunotherapy,” and “prevention.” Additionally, gray literature sources, including WHO reports, CDC guidelines, and clinical trial registries (e.g., ClinicalTrials.gov), were reviewed to provide contextual and policy-related insights.
Synthesis Approach
The narrative was structured to find the findings into thematic sections such as molecular pathogenesis, screening, and therapies. Although formal quality assessment tools such as GRADE were not applied, large-scale studies, randomized controlled trials (RCTs), and meta-analyses were given priority, while observational studies and pre-clinical data were included to illustrate new directions. Greater emphasis was placed on consensus guidelines from organizations like WHO and NCCN, as well as studies with robust methodology.
Organization and Synthesis of Information
After the data extraction, the results were organized according to the major domains of cervical cancer research into thematic sections. These included epidemiology, risk factors, molecular pathogenesis, screening and diagnostic strategies, existing therapies (surgery, radiotherapy, chemotherapy), emerging approaches (immunotherapy, targeted agents), and prevention measures (HPV vaccination, public health initiatives). In each thematic area, the authors synthesized data from multiple studies, highlighting convergent and divergent findings. This narrative integration emphasizes critical connections—such as how risk factor data align with molecular mechanisms or how screening outcomes feed into treatment strategies—and underscores where additional research is needed.
Data Interpretation
A general interpretation of the synthesis reveals that preventing the incidence of cervical cancer continues to hinge on early prevention (notably through sufficient coverage of HPV vaccine) and organized screening programs. These show marked incidence rates decline where they are implemented effectively. These observations are fully corroborated by existing knowledge and new data, and thus reinforce the high certainty probability that vaccination of adolescent girls against HPV should be a priority. Meanwhile, methods for screening with HPV testing either alone or in co-testing with cytology are moderate to high in certainty for detecting high-grade precancerous lesions.
However, many of these studies demonstrate methodological variation or are accentuated on the settings of higher income, thus making the generalization of their outcomes to the ones of lower-resource possible. Moreover, immunotherapy and targeted therapies do provide promising opportunities; however, the given evidence is too diverse, sometimes includes only a few patients in the study samples, expensive, and lacks long-term follow-up data. These are some of the reasons why it is not possible to state that the results are generalizable and sustainable at this stage.
Based on these considerations, this review highlights the possibility of a dramatic change brought by novel interventions, especially if transformable for different healthcare systems. The weakness of this type of review, such as lack of peer review using a strict protocol and possible sample selection bias, should be acknowledged. Thus, the discussion provides attention to areas where data are robust enough to inform practice and policy and others where more rigorous research is needed, particularly in areas with the highest incidence of cervical cancer but that are least populated and least represented in the data.
Epidemiology of Cervical Cancer
Cervical cancer still remains one of the most significant health issues around the world, with that weight unfairly falling on women living in many countries, both low and middle income. Approximately 570 000 cases and 311 000 deaths from cervical cancer were identified as an incidence and a cause of death, respectively, in 2018 worldwide, and it is the fourth most common new cancer and the fourth most common cause of cancer-related deaths worldwide. 9 However, despite the above progress, cervical cancer still remains the third leading cause of cancer-related deaths among women in the world, with nearly 85% of these related deaths occurring in underdeveloped and developing nations, and with a mortality rate from cervical cancer in low- and middle-income countries 18 times that in the high-income countries. 12
Trends in Cervical Cancer Incidence Before and After the Implementation of HPV Vaccination Programs in Various Countries.

There is still a high mortality rate from cervical cancer in areas where there are few healthcare resources, although its incidence has been decreasing in some regions. Besides leading to death, morbidity associated with this sickness is equally very significant among survivors who undergo physical, psychological, and financial suffering. 9 The struggle against cervical cancer on a more global level must be considered in multiple ways.
Different goals are set through the World Health Organization’s Global Strategy to Accelerate Elimination of Cervical Cancer as a Public Health Problem: by 2030, plan to complete the mission of vaccinating 90% of girls with the HPV vaccine by age 15, screening 70% of women once using a high-performance test before age 35 and again before 45, and treating 90% of women who are discovered to have cervical disease. 22 Globally, the number of new cases of cervical cancer may decrease greatly where these objectives are achieved because the global health community will be one step closer to realizing its objective of completely eradicating this common health condition.
Causes and Risk Factors of Cervical Cancer
The knowledge of cervical cancer and precursors that lead to its development is absolutely necessary in connection to the preventive, diagnostic, and eventual management interventions. In regard to cervical cancer causes, general susceptibility factors are acknowledged. However, persistent infection with high-risk HPV subtypes stands for the principal etiology.
Human Papillomavirus (HPV) Infection
The chief underlying factor implicative of precancerous as well as cancerous cervical lesions is infection with high-risk or oncogenic HPV types. Research has demonstrated a strong correlation between the incidence of high-risk HPV infection and cervical cancer. There are 14 types of high-risk HPV, namely HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, and 73. 12 It is a known fact that cervical cancer is caused by infection with HPV 16 and 18 on most occasions. In human populations, high-risk types, especially HPV 16, are reported to be present in high prevalence. It is principally acquired through sexual activities, and most of the sexually active people will get it in their lives at some point. This results in the development of the squamous intraepithelial lesions. Many of these lesions resolve on their own by 6−12 months because of immunologic clearance. But a small percentage of these lesions remain and increase the rates of developing cancer. Frequently becoming infected with this high-risk HPV can lead to the development of precancerous lesions, which may progress to cervical cancer if not detected and treated promptly. 23
HPV Genotype Diversity and Oncogenic Risk
HPV-16 and HPV-18 have been recognized as the most oncogenic genotypes, to be responsible for about 70% of cervical cancers worldwide. 24 Within these, HPV-16 consistently presents the most lethal carcinogenic potential due to its highly effective E6 and E7 oncoproteins. Together, other high-risk genotypes such as HPV-31, HPV-33, HPV-45, HPV-52, and HPV-58 together represent 20-30% of the cases. While the hallmark pathway is p53 and retinoblastoma protein inactivation, there are possible different viral loads and gene expression profiles that contribute to distinct oncogenic risk. 25 For example, HPV-31 often displays high prevalence in parts of Europe, and HPV-58 is also highly prevalent in East Asia. 26 HPV-45 is a particular endemic in sub-Saharan Africa, while Central and South American regions sometimes have a higher incidence of HPV-33 and HPV-45 than HPV-18. Such geographic patterns are presumably the result of a host’s genetics, mating networks in situ, and current vaccination coverage. Although these less frequent high-risk variants HPV 35, 39, 56, 59, and 68, their distribution is more irregular, and they are less prevalent. Moreover, some studies even indicate that such regional clustering might be attributed to the co-infection dynamics, healthcare access, or sociocultural practices. Although less aggressive than HPV-16, these genotypes will help contribute to the overall disease burden if they remain undetected or untreated.
HPV co-infections happen when various high-risk genotypes from the HPV family coexist in the same host, where the molecular events that drive cervical carcinogenesis are further amplified. 27 In each case, each genotype is capable of producing its own E6 and E7 oncoproteins, further inactivating overall tumor suppressor pathways. But when there is more than one high-risk type present, these effects become cumulative, increasing the chance that cells can get away from normal growth controls. Furthermore, this synergy also allows for persistent infection, as one genotype might inhibit local immune defenses or epithelial integrity so that the additional strains encounter a more permissive environment. Thus, women infected with more than one genotype of HPV may undergo a faster progression than those with infection by a single genotype from low-grade dysplasia to high-grade lesions and finally to invasive cancer. 28 Additionally, the elevated viral load and variety of viral antigens may make screening more difficult owing to the mimicking of subtle cytological changes. Molecular testing that can detect multiple genotypes at the same time may be useful and has been useful in screening programs in areas with a high co-infection rate. 29
Vaccine effectiveness can also be affected by co-infections. HPV vaccines are mostly prophylactic for the most common oncogenic types (such as HPV16, HPV18, and some others) without covering certain strains. 30 In populations of diverse genotype, protective effect against one or two genotypes may be undermined if other oncogenic types remain active or become dominant. In addition, if the infection contains a vaccine-covered genotype and an uncovered genotype, disease progression may still occur through the latter. However, in human immune evasion, viral recombination or release of persistent infection with non-vaccine strains may fuel such events at lower frequencies but with still significant impact. 31 These findings help indicate from a public health perspective, the need for both broad-spectrum vaccination approaches and ongoing surveillance for changing genotype prevalence as a strategy for control of HPV-related disease. In regions of high burden, the combination of vaccination with sensitive molecular assays capable of detecting multiple high-risk HPVs may give rise to the optimal overall prevention. Integrating such efforts can limit the spread of non-vaccine strains and prevent co-infection scenarios from overtaking the great progress achieved with current HPV vaccination programs.
Smoking
There is a well-documented relationship between smoking and cervical cancer, with a raised risk in developing cervical cancer, especially in women who are infected with human papillomavirus (HPV), the main etiological agent for cervical cancer. 32 Plummer and his associates report that current smokers have about 2 times more risk of developing cervical cancer than non-smokers. 32 Smoking results in a decrease in the efficiency of the immune system, which will allow cervical cancer initiation, as HPV infections are not cleared as they should be in their regular process. These are potent carcinogens, which are allowed to enter the body due to tar and nicotine by the introduction of tobacco-specific nitrosamines and polycyclic aromatic hydrocarbons as the means by which the carcinogenic effects of smoking are primarily mediated. 33
These substances can cause DNA damage and help form cancer of normal cervical epithelial cells. Besides the formation of reactive oxygen species (ROS), smoking also induces the formation of ROS, which can undergo oxidative stress and, again, damage the DNA. Over time, this damage can initiate mutations causing the growth of cancer. 34 Smoking has been shown to have immunosuppressive consequences, suppressing the body’s capacity to get rid of HPV infections. 35 Women who smoke are at increased risk of developing high-grade cervical intraepithelial neoplasia (CIN), a precursor of invasive cervical cancer. 36 In particular, smoking may potentiate the carcinogenic effects of HPV on a viral persistence conducive to disease progression from HPV infection to cervical neoplasia. Also, smoking can change the cervical mucus, making it more vulnerable to HPV infection and other sexually transmitted infections (STIs), which then elevate the risk of cervical cancer. 36
Immunodeficiency
Chronic immunosuppression, whether congenital or acquired, impairs immune surveillance and elimination of HPV and the subsequent histopathological changes, such as cervical intraepithelial neoplasia (CIN), that can lead to invasive cancer. The human immune system has a primary function in the regulation of HPV persistence and progression to cancer. The body’s immune system would indeed ordinarily detect and reject HPV-infected cellular tissues through the immune system’s natural and acquired defenses. If the immune system is weakened by congenital immunodeficiency, HIV infection, or immunosuppression for other medical reasons, including organ transplantation, the chances of eradicating HPV infections are sharply reduced.
This stronger propensity to develop persistent HPV infection is the main way that immunodeficiency affects cervical carcinogen exposure. 37 Children with inherited immunodeficiencies, including severe combined immunodeficiency (SCID) or common variable immunodeficiency (CVID), are typically commonly infected with HPV and other viruses. Failure to develop a proper immune response against HPV results in chronic infections that pose a high risk to cervical cancer. Medical research has found out that women with congenital immunodeficiencies are more prone to developing CIN and cervical cancer than women in the general population, which brings out the fact that a fully functioning immune system is protective in cervical carcinogenesis. 38 It is widely known that immunosuppression, and more specifically HIV, increases the risk for cervical cancer. The risk of sexually transmitted HPV and progression to persistent high-risk HPV infection and/or CIN and invasively malignant cervical cancer is higher among HIV-positive women.
Such poor immune response as seen through HIV-mediated CD4 + T cell loss affects the body’s ability to eliminate HPV strains. HIV-positive women are more likely to contract HPV and progress faster through the stages of CIN to cervical cancer. This immune improvement is due to antiretroviral therapy (ART), since countries affected by HIV still remain at high risk of cervical cancer, as reported in the study by Ghebre and colleagues. 39 This is particularly the case in patients with organ transplants who receive immunosuppressive drugs, patients receiving chemotherapy, and others. Medications taken to prevent organ transplant rejections or to manage autoimmune disorders impair the immune response that clears HPV infections. This otherwise results in a prolonged immunosuppressive state that allows HPV to persist and the pre-malignant lesions such as CIN 1, to develop into invasive cervical cancer. Some investigations have revealed that cervical cancer is more likely to affect women who have undergone organ transplantation compared to women in the general population because the immune system helps prevent HPV-associated malignancies. 40
Long-Term Use of Oral Contraceptives
Oral contraceptive pills (OCs) are used widely to prevent pregnancy; however, they are associated with cervical cancer if used for a long time. Cervical cancer is signified as being one of the diseases that may be associated with the use of OCs by the biological pathway involving estrogen and progesterone, which are key components of OCs. One of the ways by which OCs can cause cervical cancer has to do with the hormones used in those contraceptives: estrogen and progesterone. Thus, these hormones may alter the cellular circumstances of the cervix to increase its vulnerability to human papillomavirus (HPV)—the main cause of cervical cancer. The estrogen receptor was found to stimulate cell proliferation in HPV-positive cells, while on the other hand, the progesterone receptor was believed to inhibit the immune system, thereby making the body unable to get rid of the virus. 41
These hormonal consequences enhance the probability of the promotion of HPV infection to cervical cancer. Also, OCs are capable of inducing endometrial atrophy and cervical epithelium modifications that might predispose a woman to HPV carcinogenic effects. The synthetic hormones found in OCs may affect the cervical mucus and epithelial lining in a manner that can increase the stability of the high-risk HPV sorts that are most likely to produce cervical carcinoma. 42 In a large cohort study conducted, the authors reported that women who used OCs for 10 years or more had nearly twice the risk of developing cervical cancer than women who have never used OCs. 43 Furthermore, the responders provided indications that genetic predisposition can modify how oral contraceptives act as a factor within the context of cancer. Some risks contributed to by the prolonged use of OC are more severe in women possessing certain genetic polymorphisms. 44
Young People’s Early Exposure to Sex
A study by Akarolo-Anthony and colleagues revealed that the onset of coital relations was one of the most significant risk factors in cervical cancer because the cervix is most permeable to the penetration of the HPV virus during the youthful ages. 45 It also found that the probability of being exposed to HPV rises when individuals participate in sexual relations at a youthful age since youth sexual debut signifies extended years of sexual practices as well as numerous partners. The immature cervix, especially the transformation zone where columnar epithelial cells are exposed during adolescence, is more susceptible to HPV. 46
Furthermore, improved compliance with contraceptives has not occurred and as such younger women are likely to lapse on contraceptives, thus enhancing HPV transmission and cervical dysplasia. 47 Some research also has established that women who engage in sexual activities before attaining the age of 18 years have a higher cervical cancer risk than women who have their first intercourse later in life. 48 It is evident that clues concerning sexual involvement and cervical carcinoma relate to socioeconomic status and education. A lower socioeconomic background has been attributed to a narrow access to sexual health services and information products, pregnancies at a young age, and lower HPV vaccinations and routine cervical smears. 49
Lack of information and education, as well as limited access to means to prevent or treat the disease, increases vulnerability to HPV and cervical cancer. Other important risk factors that predispose the cervical tissues to cancer include early sexual activity, since the tissues of adolescents are biologically susceptible. It is also widely accepted that the transformation zone in which HPV is most likely to become resident is different in the immature cervix and is altered by metaplastic change during puberty. This area is particularly susceptible to HPV-induced cellular changes, which can lead to the development of cervical intraepithelial neoplasia (CIN) and eventually cervical cancer if not detected and treated early. 20 Additionally, the immune system defense of young women may be insufficient to clear HPV efficiently and thus develop chronic infections that may easily transform to malignancy.
Molecular Pathogenesis of Cervical Cancer
Cancer occurs as a result of a series of steps that start when high-risk human papillomavirus (HPV) types infect the epithelial cells within the cervix. This viral and host cell interplay transitions normal cells into precancerous lesions, ending up in invasive cervical cancer. The primary etiological factor in the development of cervical cancer is persistent infection with high-risk types of human papillomavirus (HPV), including HPV 16, 18, 31, 33, 45, 52, and 58, where HPV 16 is found in approximately 60% of the cervical cancer cases. 50 The molecular pathogenesis of cervical cancer is a multifaceted process that involves the integration of HPV DNA into the host genome, dysregulation of critical cellular pathways, and the eventual malignant transformation of cervical epithelial cells.
Cervical Cancer Pathogenesis
Cervical carcinoma is developed through a sequence of genetic changes that occur after the infection of the cervical epithelium with high-risk HPV types. The initial infection takes place at the basal cells of the squamous epithelium at the transformation zone of the cervix, where both columnar and squamous epithelia are found. 51 This area is vulnerable to HPV infection because of the high rate of cellular turnover and the exposure of basal cells, to which HPV preferentially binds. After infection, HPV gains entry into the host cell through microabrasions, or any break or crack at the epithelial layer for accessing the base layer of the epithelium. 52 Upon entering the host cell nucleus through the microtubules, the HPV genome remains as an extrachromosomal element and starts synthesizing early proteins; E6 and E7 restrict the normal cell cycle.
These viral proteins interfere with and degrade major tumor suppressor proteins (Figure 2), including p53 and retinoblastoma protein (pRb), hence allowing unrestricted cell growth.
53
Over time, some of the viral DNA may become incorporated into the host cell protoplasm, and this is a major event that transforms a benign HPV infection into an intraepithelial neoplasia.
54
The DNA of the virus is integrated, which causes the contrary regulation of viral oncogenes, which leads to the constant generation of E6 and E7. This leads to still heavier suppression of tumor suppressor pathways, enhanced frequency of chromosomal abnormalities, and the build-up of additional mutations that contribute to the transition from low-grade cervical intraepithelial neoplasia (CIN 1) to high-grade (CIN 3) and the development of cervical cancer.
55
Cervical cancer is described pathologically to go through the following staging in terms of histopathological changes that include CIN with grading depending on the degree of the dysplasia seen in the cervical epithelial cells. CIN1 is a moderate degree of cytological abnormality that is located at the lower third of the epithelium, whereas CIN2 and CIN3 are severe cytological grades of abnormality that involves two-thirds or more of the thickness of the epithelial layer.
23
CIN3, if not treated, may upgrade to invasive cancer, defined as the presence of malignant cells that have penetrated through the basement membrane to the underlying stroma. Viral Oncoprotein-Mediated Disruption of Tumor Suppressors (p53 and RB), Persistent Infection, Viral Genome Integration, and Gradual Accumulation of Genetic and Epigenetic Changes Leading to Dysplasia and Eventually Invasive Cervical Cancer.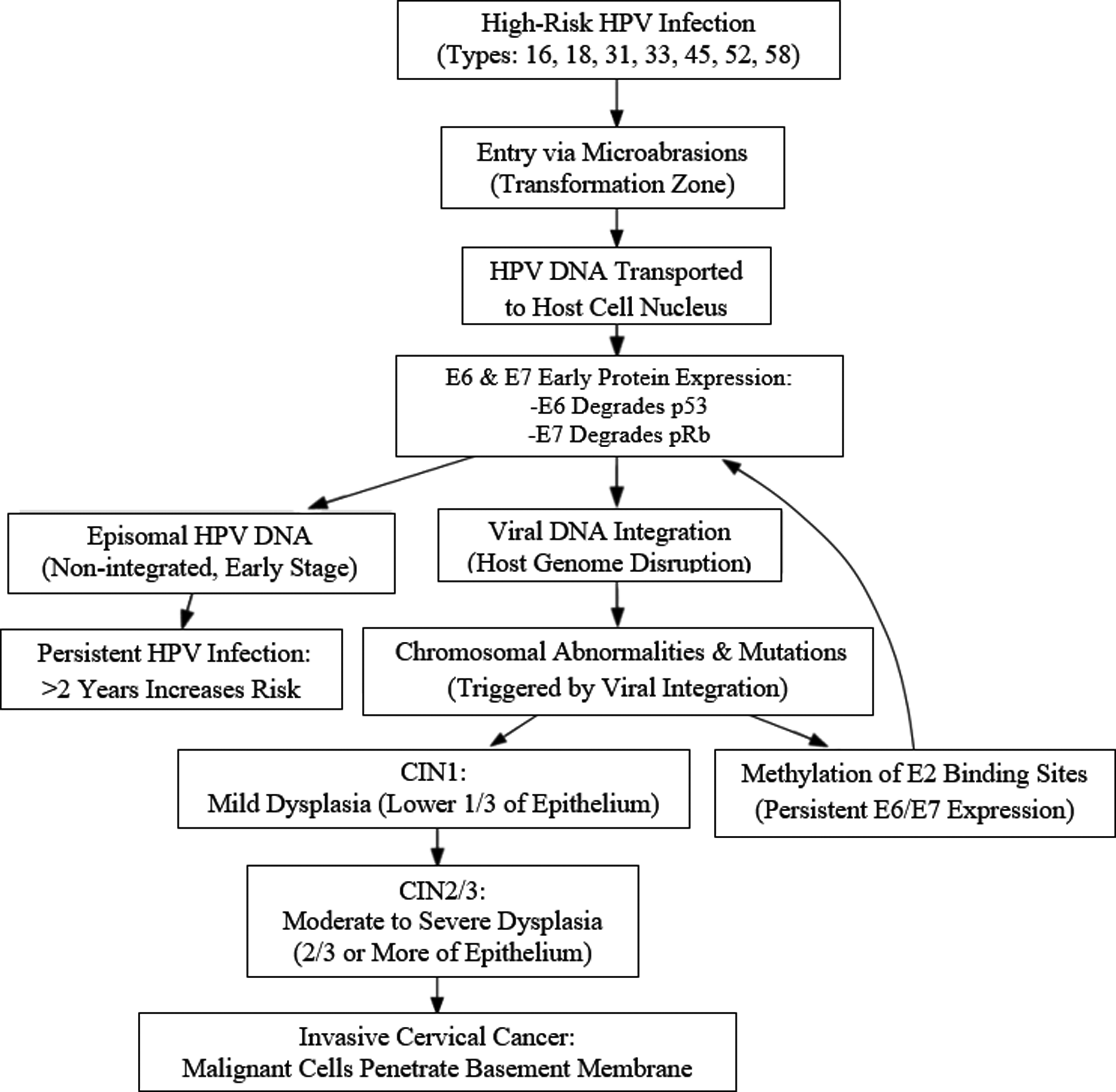
The majority of the HPV infections are clinically inconsequential; the majority, 60% of HPV infections, resolve within one year, and 90% resolve within two years. 56 Persistent infections that last greater than two years have also been associated with an elevated risk for cervical intraepithelial neoplasia (CIN). 57 According to the research conducted by Chen and his associates, only 0.6% of HPV infections result in cancer, though a 16-year follow-up research study showed that women with persistent high-risk HPV infections have a 75.4 times higher probability of developing cancer than women with no HPV infection. 58 It is proposed that during persistent HPV infections, mutations and chromosomal abnormalities accumulate over time, promoting integration of the viral genome into the cellular genome and contributing to cancer progression. 59 In most cases of cervical cancer, the viral genome integrates mainly at the E1 and E2 regions, interrupting their normal functioning and thus increasing the expression of oncogenes E6 and E7. The preservation of the tumor phenotype depends on the steady presence of E6/E7 viral oncogenes. 60 However, viral integration does not occur in all cervical cancer; in some cases, HPV DNA remains as an episome, 61 and methylation at E2 binding sites within the locus control region (LCR) has been shown to prevent E2 binding and consequently promote the continued expression of the viral oncoproteins. 62
HPV-Associated Cervical Cancer Oncogenesis
HPV is an important factor in the oncogenesis of cervical cancer. The oncogenic process associated with high-risk HPV types, especially HPV-16 and HPV-18, is characterized by the integration of the viral genome into the host genome and the disruption of cell cycle regulation. The E5, E6, and E7 proteins are the major oncoproteins in HPV-related cervical cancer (Figure 3). These viral oncoproteins disrupt normal regulatory processes in host cells, allowing the virus to escape normal cellular restraints and stimulate cell growth. They interfere with the physiological control of cell signaling pathways that are implicated in cell division, DNA repair, immune response, cell death, and metabolism.
63
Collaborative Effects of E5, E6, and E7 Promote Hyperproliferation, Immune Evasion, and Genomic Instability, Ultimately Leading to Cervical Cancer Malignancy.
The E5 protein is a small hydrophobic protein that is mainly associated with the endoplasmic reticulum, Golgi apparatus, and plasma membrane. E5 has been shown to have oncogenic properties through various ways, such as altering growth factor receptor signaling, suppressing apoptosis, and immune evasion. 64 Epidermal growth factor receptor (EGFR) is one of the main targets of E5; it is a cell surface receptor that is involved in the regulation of cell growth, proliferation, and survival. E5 modulates endosomal pH and prevents the binding of EGFR to c-Cbl ubiquitinase, thus reducing its degradation and enhancing mitogenic signal transduction. 65 E5 interferes with the CDK inhibitors p27Kip-1 and p21Waf-1 in a negative way, 66 which keeps the cell in the cell cycle, and thus the virus persists. E5 also inhibits keratinocyte differentiation by downregulating KGFR and enhances the activity of EGFR, which reduces the rate of differentiation. 67 This sustained activation of EGFR can help to explain the hyperproliferative phenotype of HPV-infected cells and the subsequent genetic changes that lead to malignancy.
Besides the interaction with EGFR, E5 can also influence other signaling pathways, including the PI3K/AKT pathway that is related to cell survival and metabolism. Through this pathway, E5 is able to block apoptosis in infected cells, enabling them to acquire the mutations required for cancer growth. 68 E5 has been found to inhibit apoptosis, a cell death process that is essential in the removal of abnormal or infected cells. E5 can influence the activity of several apoptotic regulators, such as the Bcl-2 family of proteins, and thereby protect the cell from stress or immune-mediated killing. 69 E5 prevents apoptosis, thus enabling HPV-infected cells to continue to divide even if they contain DNA damage or other oncogenic stimuli. E5 is also involved in immune evasion, especially in the initial stages of HPV infection. E5 can also reduce the surface expression of MHC class I molecules on infected cells, thus making the cells invisible to CTLs. 70 E5 also impacts MHC-II antigen presentation by inhibiting the degradation of invariant chain through endosome alkalinization and thereby decreasing the activity of this molecule on the cell surface. 71 Notably, HPV16 × 105 has been reported to down-regulate the expression of keratinocyte-specific IFN and the subsequent inactivation of the JAK/STAT pathway and the suppression of IFN-stimulated genes, which in turn affect the maintenance and integrity of the viral episomes. 72
Key Factors in Initiation of Cervical Cancer
The transformation of HPV-infected cervical epithelial cells into cervical cancer is a stepwise process characterized by the continuous acquisition of additional genetic and epigenetic alterations in oncogenes and tumor suppressor genes. HPV penetrates the host through microabrasions and gains access into the basal squamous cells. This integration triggers replication of the virus and genetic changes that lead to neoplastic changes. Morever, CIN 1 is characterized by chronic infection, and transition from precancerous stages to malignant cancer form requires 10-12 years. If CIN 1 changes are not reversible, they are capable of progressing to CIN 2/3 within 2-3 years. 73 Due to infection, the host’s first line and the second line of defense, referred to as the immune response, are triggered. The general histocompatibility genes of class I and II molecules present antigens to cytotoxic and helper T cells, respectively. In HPV infection, toll-like receptors (TLRs) are induced by viral elements and follow activation of NF-κB and interferon response factor-3 (IRF3) for cytokine synthesis.74,75 TLRs also stimulate MHC class I and II. Future research must investigate how TLR activation results in MHC class I and II expression.
However, HPV oncoproteins E5 and E6 block MHC class I and interferon regulatory factor 3, respectively, thus allowing the virus to escape immune recognition. 70 Thus, TLRs involved in antiviral immunity include TLR3, 4, 7, 8, and 9 in terms of IFN production. TLR-9 is expressed at different grades of cervical cancer during the progression of cervical intraepithelial neoplasia to squamous cell carcinoma (SCC). Some HPV E6-E7-positive transformed cell lines show reduced TLR-9 expression; this would reduce interferon response and contribute to chronic infection. 76 HPV also stimulates EGFR, which leads to IFRD1 because it inhibits NF-κB cytokine production. 77 Despite the immunogenic nature of HPV, it is capable of becoming latent-like by integrating into epithelial cells. Dendritic cells and other antigen-presenting cells (APCs) present HPV peptides to MHCs to activate CD4+ and CD8 + T lymphocytes. This results in an increase in the cytokines such as IFN-γ and tumor necrosis factor alpha, which leads to inflammation and immune response towards tumors.
It is worth mentioning that the regulatory T cells (Tregs), which are stimulated by APC, secrete cytokines such as IL-10 and TGF-β that suppress the function of APC and reduce immune response. Persistent HPV-16-positive women have higher Treg levels, and TGF-β1 concentrations rise as CIN lesions progress to invasive cervical cancer. 78 At the initial stages of HPV, the virus tampers with genes that are associated with immunity, for instance, IFNAR1, EMP1, and IL1RN. Another study has found that downregulation of IL1R2 is related to cervical cancer progression. 79 The Hippo-YAP pathway has been found to contribute to the cervical cancer development; specifically, the YAP1 protein is very key in the development of cervical cancer. The YAP1 protein is involved in the interaction with the HPV E6 oncoprotein, as YAP1 contributes to the enhancement of cancer growth due to E6-mediated YAP1 stabilization.
Overexpression of YAP1 in cervical cancers has also been reported, and the YAP1 overexpression can induce SCC in animal models.
80
Overstimulated YAP1 raises the risk of contracting HPV by promoting the expression of HPV receptors such as EGFR, ITGRA6, and SDC1. YAP1 also inhibits the expression of TLR2 and 4, which are proteins involved in innate immunity and TBK1 activity. contributing to HPV evasion.
81
All in all, HPV-mediated cervical cancer formation depends on the virus’ capacity to escape the host’s immune response and impair cell processes (Figure 4). Based on the involvement of YAP1 in the HPV-associated carcinogenic process, YAP1 might serve as a biomarker for cervical carcinoma.
82
Cervical Cancer Initiation Begins with HPV Genome Integration, Immune Evasion (via E5 and E6 Proteins), and Persistent Infection Leading to Cytokine Dysregulation, YAP1 Overexpression, and Lesion Progression to SCC.
Immune Avoidance
Human papillomaviruses have a few mechanisms to evade the immune system: they inhibit interferon production and stimulate interleukin (IL)-10 and transforming growth factor (TGF)-β1 (Figure 5). Accordingly, cells within the tumor microenvironment cause an immunosuppressive stroma and change in tumor surface antigens that impair the immune response.
78
In individuals with high-risk HPV infections of the cervix and with squamous intraepithelial lesions (SIL), IL-10 and TGF-β1 may initially promote factors that inhibit the lesion’s immunosuppressive microenvironment and can adversely impact the cellular immune response.78,83 Such a microenvironment can lead to the persistence of viruses, resulting in cervical cancer.
84
From individuals with low-grade SIL, high-grade SIL, high-risk HPV infections, and cervical cancer, the serum and cervical tissues contain the cytokines IL-10 and TGF-β1.84,85 HPV Immune Avoidance Creates an Immunosuppressive Environment via IL-10, TGF-β1, E6/E7 Suppression of Interferon and MHC, Treg Recruitment, and Peripheral Tolerance, Enabling Persistent Infection and Cancer Progression.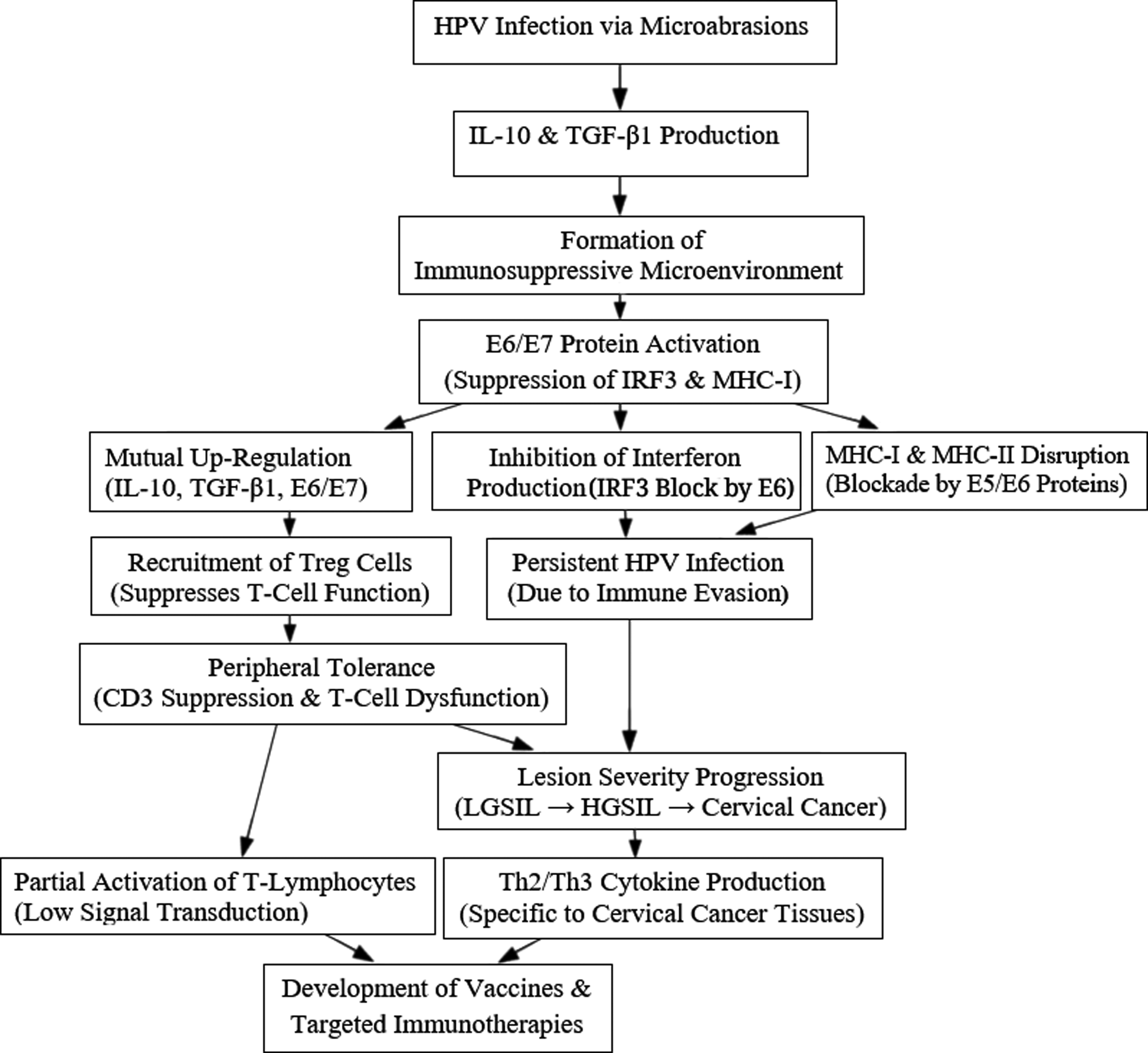
The concentration of these cytokines is directly proportional to the severity of the lesion. 86 An earlier look revealed that the autologous immunosuppression is unique to cervical cancer and is related to Th2/Th3 cytokines. These data are consistent with cervical biopsy data on Th2/Th3 cytokine production in cervical cancer tissues that is not detected in normal cervical tissue: HPV infection leads to immunosuppressive cytokine transcription to avoid the host’s immune response. 87 Hence, there is a mutual up-regulation between the immunosuppressive cytokine interleukin-10 and TGF-β1. They also stimulate HPV-16 × 106 and E7 proteins that in turn activate TGF-beta1 and IL-10 genes, thus forming a vicious cycle as identified by Peralta-Zaragoza and his mates. 88 IL-10 and TGF-β1 inhibit the expression of CD3, and this has a significant function on T-cells. Finally, IL-10 and TGF-β1 recruit Treg cells, leading to severe peripheral tolerance.
Thus, it is assumed that IL-10 and TGF-β1 contribute to immune system avoidance by creating an immunosuppressive environment in the cervixes of HPV-positive women. These findings will be particularly useful for HPV vaccine production and the creation of new target-specific immunotherapies to treat women who have LGSIL, HGSIL, or cervical cancer. 89 It has been demonstrated that circulating T-lymphocytes are only partly activated in patients with cervical lesions and cervical cancer and that few signal transduction molecules, which relate to the full activation of T-lymphocytes, are expressed and functional. Hence, it is of particular importance to assess whether type Th1 cytokines are capable of down-regulating these molecules and whether scientists can generate fully functional HPV-specific T-lymphocytes.
Genetic and Epigenetic Changes
Epigenetic Markers for Diagnosis/Prognosis, Screening of Cervical Cancer.

Therefore, when p53 function is mutated, cells acquire the ability to resist apoptosis after DNA damage, while cells devoid of pRb become unregulated during the cell cycle. Moreover, other significant genes can also be altered, such as the PIK3CA gene, which is involved in the production of a subunit of the PI3K enzyme related to the cell growth and survival pathways as presented in cervical cancer cells. 106 Findings have reported epigenetic changes where multiple aspects of cervical carcinogenesis are related to DNA methylation and histone states, as well as miRNA patterns. Such changes can disrupt apoptosis signal pathways, which may lead to the suppression of tumor suppressor genes or activation of oncogenes without affecting the organism’s energy flow.
For instance, cervical cancer is exemplarily characterized by hypermethylation patterns of promoter regions of tumor suppressor genes, which include CDKN2A (p16^INK4a) and RASSF1A. These changes in the mechanism of action are by suppressing the genes involved in helping the cancerous cells in cycle division and evading death. 107 Furthermore, post-transcriptional regulation, including microRNA (miRNA), is ascertained to be pertinent to cervical cancer advancement. Some can act as oncomiRs or suppressor gene cells, while others are dysregulated, resulting in the interference of various cellular pathways, including those related to HPV cervical carcinogenesis. 108 Hypermethylation-induced gene silencing may occur as a secondary effect of changes influencing gene expression, such as chromatin modifications, where methylation aids in preserving the gene’s silenced state. Strong evidence for this perspective comes from studies that revealed the methylation of histone H3 lysine 9, a form of chromatin modification, coinciding with the re-silencing of the p16 gene in the absence of DNA methylation in cells where p16 had previously been reactivated by knocking out DNA methyltransferase. 109 Additionally, data from mammary epithelial cells that bypassed senescence and had demethylated the promoter further supported the silencing of p16. 110
Screening of Cervical Cancer
While preventing the identification and unnecessary treatment of transient HPV infection and its associated benign lesions, the ultimate goal of cervical cancer screening is to detect high-grade cancer precursor lesions and early asymptomatic invasive cervical cancer. Finding these temporary lesions carries a significant risk of harm because most HPV infections and many CIN 1 and CIN 2 cases are temporary. This risk includes mental stress, physical discomfort from additional diagnostic and treatment procedures (e.g., vaginal pain, bleeding, infection), and an increased risk of maternity complications like preterm delivery following treatment. 47
Cervical Cytology Tests
Cervical smear tests come in two types, conventional and liquid-based cytology. In the conventional method, cells are taken from the neck of the cervix, and then the cells are spread on a standard glass slide. In the liquid-based cytology method, cells are taken from the neck of the cervix, but instead of being placed on a glass slide, the cells are put in a small vial of fixative solution. Much has been said about which form is better than the other. The current data suggests there is no distinguishable disparity in terms of the sensitivity or specificity of liquid-based cytology and conventional cytology. 111 According to Moyer & U.S. Preventive Services Task Force, both these methods are of substantial net benefit when delivered in the recommended age groups at the right interval. 112
HPV Testing
One shortcoming of the Pap test is that it has a high false positive cytology, as has been made evident by Rijkaart and colleagues in their extensive survey of its effectiveness in screening in different countries, 113 irrespective of its high effectiveness for screening in countries that are capable of implementing the Pap test to a big percentage of the population. With this detection, there was improved understanding of the role of HPV with cervical cancer, resulting in the creation of new molecular tests for HPV that are more sensitive, with a sensitivity of approximately 90%. 114 Nevertheless, there is slightly lower sensitivity for CIN2 and CIN3 relative to cytology data. This currently available DNA test identifies only a range of high-risk HPV types and has higher inter-observer reproducibility than cytology. The HPV test is a solution hybridization that has the potential to enhance signals of amplification in the assays of the 13 HPV high-risk types. 115
Thus, the HPV test should be done only on women aged 30 years and above since women below 30 years are likely to have transient infections and low risk of underlying high-grade lesions. 112 Therefore, accepting the HPV DNA testing in the group of women younger than 30 years old results in unnecessary evaluation and treatment. 112 At the present time, HPV DNA testing is the most sensitive and can be used in conjunction with Pap smears (co-testing) for the best diagnosis of high-grade cervical intraepithelial neoplasia. 114 If a woman has mild or borderline abnormal Pap results, the Pap-plus-HPV test might be more fruitful because a negative HPV-DNA test can help convince a woman that her Pap abnormality report is false; on the other hand, these women may undergo HPV-DNA positive result treatment earlier since this test is highly sensitive. 116
Visual Inspection with Acetic Acid
The low- and middle-income countries (LMICs) are confronted with a scarcity of basic commodities for health in general, not to mention the insufficient stock for women’s preventative health activities. In this regard, LMICs explore the feasible screening type that can fit various societal constraints practiced by women in such countries. Most of these LMICs lack the present resources to fund cytology-based cervical cancer prevention programs. 117 These societies also present a host of operational obstacles that diminish the quality of the Pap test: follow-up of multiple visits for screening and later post-diagnosis therapy, inadequate recall and referral systems, insufficient resources for screening and treatment, and competing health priorities in the systems. 117
In these societies, the operational factors that have an impact on the quality of the Pap test are follow-up difficulties of multiple visits for screening and post-diagnosis treatment, inefficient recall and referral systems, and structural obstacles in the form of inadequate facilities for screening and treatment and priorities in the health care management systems. 117 A viable substitute to the Pap test has been achieved here, mainly due to the low-cost factor, along with the “see-and-treat” factor in a single visit. Cryotherapy-based treatment of VIA-positive lesions, combined with the test known as visual inspection with acetic acid (VIA), is a testing method that we have seen has been easily adopted by non-physician providers and has been studied widely as a potential substitute for the Pap smear. 118
FIGO Staging of Cervical Cancer.

Therapy for Cervical Cancer
Surgery
Surgery is a proven and frequently employed method of treating different varieties of early-stage cancers, as it aims at excision of the cancerous tissue. It can, however, also be applied to remove metastatic tissue. 122 The different surgeries done today include total hysterectomy, radical hysterectomy, loop electrosurgical excision procedure (LEEP), conization, trachelectomy, and cryosurgery. 123 The type of surgery largely depends on the disease and the degree of invasion. 124 In patients who have reached the postmenopausal stage, the recommended surgical approach is the total abdominal hysterectomy with or without the bilateral salpingo-oophorectomy. Radical hysterectomy is mostly performed in cases of cervical cancer with larger lesions (tumors up to 4 cm in diameter) and requires excision of the uterus, cervix, parametria, and the upper part of the vaginal canal. 125
The Laparoscopic Approach to Cervical Cancer (LACC) trial showed that while radical hysterectomy by laparoscopy was less invasive, it also meant a higher rate of recurrence, an inability to conceive, and potential urinary problems in the future. 126 Open approach radical hysterectomy is therefore preferred, particularly for tumors larger than 2 cm in diameter. In women who are childbearing age and those with early-stage cervical cancer, a less invasive approach needs to be applied, and these are LEEP, conization, and trachelectomy. 125 LEEP employs the use of a thin wire that excises the pathological tissue from the cervix, with a successful outcome being achievable using local anesthesia in low-cost clinical environments common in LMICs. Conization involves removal of a conical tissue, including the transformation zone and either the entire cervical canal or a part of it; this calls for hospitalization, and it is relatively more expensive than LEEP. 125 Using vaginal, laparoscopic, or robot-assisted techniques, a radical trachelectomy removes the cervix, surrounding tissue (parametrium), and upper vagina. 126
Radiotherapy
Radiotherapy exposes the body to high-energy X-rays; it is a central component of the therapy for cervical cancer. 127 The three forms of radiation therapy that are currently used to manage cervical cancer are external beam radiation therapy (EBRT), intensity-modulated radiotherapy (IMRT), and brachytherapy. The diagnostic tools, like computerized tomography (CT) scans and magnetic resonance imaging (MRI), have also enhanced precise assessment of the extent of the primary tumor, the invasiveness of the tumor, and metastasis that have, in turn, helped in radiotherapy planning. 127 In a nutshell, EBRT directs high-energy radiation beams external to the body into the tumor and is the most conventional radiotherapy utilized for the treatment of cancer. IMRT is a treatment technique that is a form of radiotherapy; here the treatment applied in the form of photon and proton beams is shaped like the tumor and is used in both cancerous and benign ones.
Similar to IMRT, brachytherapy also protects the nearby tissue structures by either giving a massive dose of radiation to the tumor or inserting a radioactive implant at the tumor location.
128
However, there are several side effects commonly related to radiotherapy, and these include diarrhea, abdominal cramps and pelvic pain, skin toxicity, lymphedema, and sexual dysfunction.
129
Thus, with stage IIA-IIIB cervical cancer, there is an absolute response in 68.3% of patients, and radiotherapy only is ineffective in controlling the progression of locally advanced disease in 20-50% of women.
130
To increase the effectiveness of radiotherapy, the disease is often treated with chemotherapy, particularly in cervical cancer cases with large tumor sizes (more than 4 cm in width).
131
Upon analysing the mechanisms of immunomodulation in radiotherapy, it can be observed that the interplay between tumor cells, immune activation, and immunosuppression in the tumor microenvironment induces tumor cell death, leading to the release of neoantigens, their uptake by dendritic cells, and the activation of T cells (Figure 6). Mechanisms of Immune Modulation in Radiotherapy.
Chemotherapy
Adjuvant chemotherapy is used in cervical cancer as a standard treatment when extreme prognostic tumor characteristics increase the risk of recurrence after surgery, used in combination with radiotherapy as already explained, and finally in locally advanced ailment. 132 Of all the molecules that have been applied for the past three decades with a view of eradicating cervical cancer, one turns out to be the most effective; this single agent is cisplatin, which is a platinum-based chemotherapeutic. 133 However, patient response to cisplatin is often followed by drug resistance during the course of the treatment, limiting the effectiveness of the several second-line platinum-based chemotherapeutic agents. 134
This has been followed by the observation that the combination of cisplatin with other agents may be more effective than the single-agent treatment. 133 Consequently, a study by Long and colleagues found that while cisplatin on its own only gave a 20% response rate, when taken in conjunction with topotecan, the response rate was 39%. 135 Another study made a similar finding when cisplatin was used in combination with paclitaxel. 136 Presently, topotecan and paclitaxel, alongside other chemotherapeutic agents including 5-fluorouracil and bleomycin, are hence utilized together with cisplatin in the treatment of cervical cancer. This leads to substantial and statistically relevant gain in the median survival. 133 Chemotherapy is also applied alongside radiotherapy, especially for locally advanced disease. This regimen is aimed at reducing the chance of disease relapse, but its complications include adverse effects and chronic morbidity.
Chemoradiotherapy has been shown to enhance standard survival and progression-free survival and lessen the incidence of localized and distant cervical carcinoma recurrences, according to one meta-analysis. 137 Finally, palliative chemotherapy is given for improving the patient’s quality of life and for the control of the disease’s symptoms, although they may not cure the tumor. 138 Also, as multidrug resistance in cancer cells affects the effectiveness of chemotherapy, it is also critical to find and develop novel and improved medicines. 139
Immunotherapy
Immunotherapy targeting HPV oncoproteins has been identified as a strategy with specificity owing to its ability to selectively target both dysplastic and malignant cervical epithelial cells that express HPV oncoproteins. 89 This approach has produced products like therapeutic vaccines, immune checkpoint inhibitors (ICIs), and adoptive T cell therapy (ACT) with varying levels of efficacy and many current trials. 140 HPV-16-specific therapeutic vaccines undergoing clinical trials proved to have a response rate of 79% in grade 3 vulvar intraepithelial neoplasia. These vaccines that are designed to counter HPV-16 and -18 oncoproteins, E6 and E7, respectively, are based on live vectors or peptides. 141
The following ICIs include FDA-approved pembrolizumab in PD-L1-positive metastatic cervical cancer and nivolumab in metastatic cervical cancer.
142
ICIs target the PDL-1/PD-1 pathway that inhibits the function of T cells and aids HPV persistence
143
(Figure 7). Antibodies like ipilimumab, which is a CTLA-4 inhibitor, boost the T cell activation even though their ability to treat cervical cancer on their own is still limited. However, when PD-1 inhibitors are combined with CTLA-4 inhibitors like nivolumab and ipilimumab, those cases exhibit relatively sustained clinical activity and tolerable side effects.
144
A type of immunotherapy known as ACT means isolating and culturing tumor-infiltrating lymphocytes (TILs) collected from the tumor area of individual patients for effective reinfusion against target cancer cells.
145
The LN-145 TIL treatment in a phase II trial showed an overall disease control rate of 89% and an objective response rate of 44%; however, more research is required.
146
ACT could be augmented by lymphodepletion; this attenuates immunosuppressive T cells while raising cytokine interface, improving therapy efficacy.
147
Trials where patients received LN-145 TIL and interleukin-2 (IL-2) have also been conducted in earlier trials.
148
Immunotherapy with Checkpoint Inhibitors Targeting PD-1, PD-L1, and CTLA-4 Boosts CD8 + T Cells to Target Tumor Antigens and Kill Cancer Cells via Perforin and Granzyme B, Aided by Vaccines.
Immunotherapies combined with or incorporated into the existing treatment modalities have also revealed a chance to raise response rates. For instance, ipilimumab after chemoradiotherapy improved antitumor immunity in patients with cervical cancer. 149 Such combination approaches are efficient to overcome the limitation of monotherapy and enhance the synergistic impacts of the combined agents. 150 In general, immunotherapy presents personalized and novel therapeutic approaches to cervical cancer. Despite the fact that more individual treatments are still under exploration, the improvements in vaccines, ICIs, and ACTs brighten the possibilities to complement current treatments and eliminate dependence on conventional chemotherapy. 151
Targeted Therapy
Chemotherapy drugs target cancer cells as well as normal dividing cells, leading to severe side effects that include anemia and hair loss.
152
Targeted therapies aim to deliberately block the tumor-associated molecules, especially proteins that are exclusively produced by cancer cells to regulate cell division, growth, and metastasis.
153
It is thus expected that targeted therapies would have better therapeutic effects and fewer toxicities than conventional chemotherapies because they are more selective to cancers than normal cells (Figure 8). Targeted Therapies for Cervical Cancer Focusing on Disrupting Key Processes Like the Cell Cycle, Growth Signaling Pathways, Angiogenesis and DNA Repair Mechanisms which Aim to Inhibit Tumor Growth and Progression.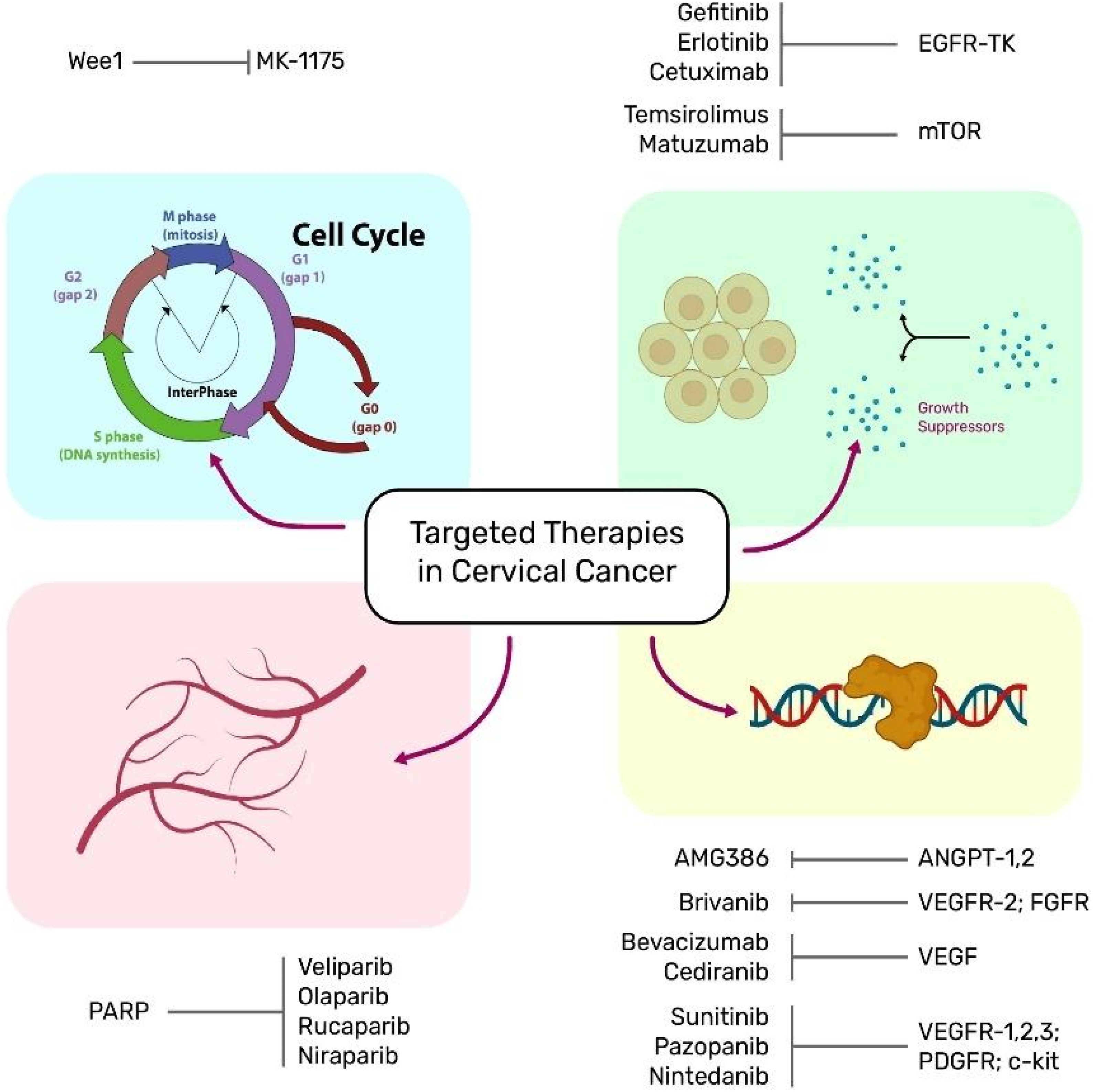
As the knowledge about cervical cancer at the molecular level has improved, it has become possible to recognize molecules involved in oncogenic signaling, which may be potential drug targets. It has been particularly relevant for patients with metastatic or recurrent cervical carcinoma because they have a poor survival rate. 153 Another area targeted therapy focuses on is the mechanisms of tumor drug resistance because this is one issue that has been a major concern in the current conventional therapies. 152
Combination Therapy
Cervical cancer is a diverse and persistent disease, and current treatments are not very effective, which is partly because of tumor drug resistance associated with current monotherapies. 153 A combination of therapies may be superior to each individual therapy because they affect multiple and/or redundant pro-survival signaling pathways in cervical cancer cells. 137 Furthermore, the integration of interventions allows minimizing the dosage, the price per cycle, the cycle number, and the side effects of monotherapy with high doses. 154 As with most treatments, effective treatment combinations are normally determined through computational methods, bioinformatics, functional biology studies, and high-throughput screening. 155
Chemotherapy with radiotherapy, immunotherapy, or targeted therapy has been used in cervical cancer. Another way of treating cervical cancer is the combined usage of chemotherapy with radiotherapy; this shrinks tumor size, suppresses micro-metastasis, and prevents the tumor’s ability to repair itself from damage and the development of drug resistance in cancer cells and amplifies the radio-sensitivity of hypoxic cells in the cervix. 156 Other researchers have also looked at the possibility of integrating immunotherapy with chemotherapy, because, first, immunotherapy can act as a marker that makes cervical cancer tumors sensitive to chemotherapy. The immunosuppressive effects of chemotherapeutic medicines on dividing immune cells, however, may limit this combination. 157 Nonetheless, certain immunotherapeutic strategies cause tumor cell immunogenicity or activate the immune system by creating a temporary lymphopenia.
Thus, a combination of chemotherapy and immunotherapy can be considered as a new direction in cervical cancer treatment. 158 Increased effectiveness against cervical cancer has also been shown when targeted medicines are used in conjunction with chemotherapy. For instance, VEGF antibodies or TKI monotherapy largely lack antitumor efficacy in the direct clinical setting for cervical cancer; however, when combined with standard chemotherapeutic drugs, progression-free and overall survival is prolonged. 155 Hence, it was truly a combination of bevacizumab added to chemotherapy with cisplatin and either paclitaxel or topotecan that was shown to have improved median overall survival of 16.8 months vs chemotherapy alone at 13.3 months.
Additionally, 28 out of 220 patients receiving this combination achieved a complete response, while 14 out of 219 receiving chemotherapy alone had a complete response. 156 Some promising results have been seen in combining chemotherapy with targeted drugs for the treatment of cervical cancer, but results of a number of trials investigating this combination for the treatment of cervical cancer have been inconclusive, and this should be further investigated. Such investigations might benefit from positive clinical evidence from combination therapeutic approaches that are currently used in other cancers.
Prevention of Cervical Cancer
HPV Vaccination and Screening Programs
Vaccines such as Gardasil and Cervarix are designed against HPV types 16 and 18, which we know are responsible for nearly 70% of cervical cancer cases 159 and can be regarded as huge steps forward in preventing cervical cancer. The World Health Organization advises that girls in the age of 9 to 14 should take the HPV vaccine, with cervical cancer prevention being the best method. 22 Besides vaccination, cervical smear in the form of a Pap test or human papillomavirus test assists in early detection of precancerous conditions or early cervical cancer, both of which are easily treatable.
The two principal procedures that can be used for screening purposes include the collection of cervical cells through the Pap test, commonly referred to as the Pap smear, and the detection of high-risk HPV DNA in cervical cell samples. Current recommendations indicate that cervical cancer screening should start no later than age 21 and continue through 65 years of age at the very least; screening intervals are dependent on age in years and type of test used. 47
Public Health Initiatives
Promotive factors aimed at cervical cancer may include increasing people’s awareness of HPV and cervical cancer, promoting safe sex practices to reduce HPV transmission, and offering HPV vaccines besides cervical cancer screening programs. Often, such programs are aimed at the high-risk group and aim to address disparities in cervical cancer incidence and mortality occasioned by unequal access to early screening. Organ-specific vaccines have been introduced, proven to be incredible in controlling the incidences of HPV and its related precancerous diseases; it has been noted that there was as much as a 90% reduction of HPV 16 and 18. 146 The Pap smears and HPV DNA tests must be conducted on a routine basis to identify the initial changes that may lead to the development of precancerous cells.
Furthermore, the use of health education campaigns is another way through which knowledge parity concerning cervical cancer, vaccination, and screening is created. For instance, the integration of education programs into community health has increased the vaccination and the screening of those in the underprivileged community. 149 If adequate measures are not taken, it is going to be difficult for governments, organizations, and healthcare providers to meet the WHO global strategy to neutralize cervical cancer as a public health threat by 2030 without compromising on equity in the delivery of these lifesaving services.
Future Directions in Research and Policy
New evidence indicates that next-generation HPV vaccines could deliver substantial improvements in cervical cancer prevention that target the prophylactic and therapeutic pathways simultaneously. Specifically, therapeutic HPV vaccines directed toward viral oncoproteins E6 and E7 have potential for eradication of established infections and preinvasive lesions. 160 The feasibility of inducing robust T cell responses to HPV-transformed cells using peptide or mRNA formulations has been evaluated in research. 161 The optimal antigen combinations, adjuvant systems, and delivery methods based on the combination of risk level and persistence of HPV infections should be further defined to maximize the therapeutic efficacy.
As vaccine research kicks in, new screening technologies may greatly improve the early detection of cervical cancer. Artificial intelligence (AI)-assisted cytology platform (automatically identifies atypical cells) is a faster and a more standardized interpretation of Pap tests than traditional Pap tests. 162 These systems may be especially valuable places where cytopathology expertise is limited, as they would minimize observer variation and accelerate turnaround times. Also, self-sampling HPV tests, already used in several pilot programs, can reach underserved or remote communities, by helping to overcome barriers of transportation, stigma, and lack of clinical infrastructure. 163 Preliminary data on these devices suggest that self-collection and high-quality HPV assays can generate reliable results with a great increase in the coverage of screening while remaining cost-effective, and ongoing trials are evaluating the sensitivity and specificity of the device reported.
From a policy point of view, efforts have to be made to ensure equitable vaccine and screening tool access to reduce cervical cancer incidence in low-and middle-income countries (LMICs). To reduce the cost for end users, governments and international agencies should be in partnership in terms of financing models such as tiered vaccine pricing, pooled procurement, and strengthening of health insurance schemes. With public–private partnerships, self-sampling test kits and AI-based cytology devices can also be widely distributed. All of this should involve task-shifting efforts that train community health workers or nurses to administer vaccines, educate local populations, and screen in settings troubled by physician shortages. Importantly, policy frameworks must include culturally sensitive educational programs related to vaccine hesitancy, addressing myths of HPV infection, and highlighting the lifesaving benefits of early detection.
Challenges in Cervical Cancer Prevention and Vaccine Accessibility
Although screening techniques have been pioneered by the Pap smear and HPV DNA testing, they have their limitations. These are in the form of false negatives, which means the test misses the presence of abnormal cells or HPV, thus delaying treatment and diagnosis. 164 Also, false-positive findings cause stress to the patient, and they are subjected to other invasive methods of examination that are not necessary. Issues such as the time intervals of screening and the proper age of starting or ceasing screenings also remain contentious, together with the efficacy of screening, particularly in communities whereby high vaccination rates are realized. 165 The availability of HPV vaccines has therefore been viewed as being a breakthrough in preventing cervical cancer. Despite these advancements, vaccination uptake still remains low in most regions, especially in LMICs, where cervical cancer dominates. 166
Reasons that could have led to low vaccination rates include the cost of the vaccines, lack of awareness, cultural and religious beliefs, and logistical challenges in vaccine delivery. However, there are also significant challenges and concerns in vaccine safety and effectiveness that have questioned vaccination, although there are sufficient empirical studies showing vaccine safety. 167 To bridge these gaps, concerted efforts are needed in the form of promoting education and/or awareness about the importance of screening/vaccination, enhancing infrastructure for delivering vaccines across the healthcare systems, and conducting primary research to design appropriate screening strategies and engineer the future generations of vaccines. Another area of focus is to dispel myths surrounding the vaccines and to encourage the masses to come forward and get vaccinated through health promotion campaigns.
Socioeconomic and Cultural Barriers to HPV Prevention and Cervical Cancer Control
Basic socioeconomic and cultural factors exert a huge influence on the HPV vaccination coverage and adherence to cervical cancer screening, especially in low-resource settings. Researchers found low general awareness of HPV and, surprisingly, high willingness to vaccinate among caregivers in a multi-state telephone survey of Abia, Adamawa, Bayelsa, Benue, Enugu, the Federal Capital Territory (FCT), Jigawa, and Taraba. 168 These findings show how awareness, perceived severity, and perceived susceptibility affect preventive health behavior. Even those who were generally willing to accept the vaccine found the access to services—limited by financial constraints, travel costs, and worries about missing work—remained a critical barrier. In rural areas, these socioeconomic impediments had to work with a dearth of public health infrastructure. In addition, regional disparities were also noted by the survey. In some Northern states, caregivers were more aware of HPV and felt more strongly that it is severe and highly infectious compared to their Southern counterparts. This difference implies having different interactions with public health campaigns. Some communities in which few people talk about sexually transmitted infections allow their local cultural norms to further swell silence and misinformation. On this basis, stigma may discourage conversations about vaccination, especially among fathers or male guardians who contribute to the decision-making on the matter of family health. Both no-cost and subsidized vaccination efforts can be held back by such entrenched views.
The power of culturally attuned strategies can be demonstrated using data from the above study. For instance, a planned community awareness campaign in Taraba led by local leaders in partnership with faith-based organizations focused on increasing caregivers’ disposition to vaccinate because it emphasized the religious and moral imperative to childcare protection. 168 This is an example of the need to adapt interventions so as not to clash with community values or misinformation. Just as important is ensuring that community influencers have access to accurate, evidence-based information. Although some areas harbor misinformation, such as the fear of vaccines causing infertility, if not addressed this, such sentiment can erode trust in immunization programs. It is necessary to take a step forward to remove these socioeconomic and cultural hurdles simultaneously with bigger policy initiatives. 169 Access can be strengthened by developing and strengthening the primary healthcare system, allocating budgetary resources for the continuous supply of vaccines, and integrating HPV education into the routine immunization outreach. In addition, meaningful community engagement involving collaborative dialogues with parents, youth, elders, and religious leaders on the myths around vaccines, along with the preventive intent of the HPV vaccines, can help dispel myths about the vaccines and reinforce the preventive intent for HPV vaccines. Community-specific belief acknowledgement, cost barrier reduction, and sustained health education can improve vaccine coverage and reduce incidence of cervical cancer.
Emerging Trends in Cervical Cancer Research and Treatment Using Novel Therapeutic Targets
Advances in Molecular Diagnostics
Cervical carcinoma has benefited from modern molecular diagnostic techniques in early diagnosis, risk assessment, and treatment. The availability of HPV DNA testing has greatly impacted screening programs by characterizing oncogenic HPV genotypes with a high degree of sensitivity and specificity. 170 HC2 and PCR are common for the detection of HPV DNA, which is actually a more competent diagnostic tool as compared to cytology alone. 9 Also, biomarkers such as p16INK4a and Ki-67 have improved the specificity in the discrimination between transient infection by HPV and the progressive lesions. Co-testing using p16INK4a and Ki-67 has now been established as a less invasive approach in cases involving HPV-positive with the potential to minimize clinic follow-up and colposcopy. 171
Beyond E6/E7 mRNA testing, other RNA-based technologies enhance risk prediction because they measure active expression of viral oncogenes associated with malignancy. 172 Advanced molecular technologies such as NGS help classify cervical cancer and characterize genomic alterations, DNA methylation, and changes in gene expression. These allow the development of individualized management plans and enhance prediction. 173 Implementing these molecular diagnostic improvements into clinical medicine has an outlook of improving cervical cancer early detection and thereby decreasing morbidity and mortality.
Bioactive Metabolites Derived From Microorganisms
Plant-derived products and bioactive molecules have been reported as a rich source for newly developed chemotherapeutic agents due to their privileged structures and well-defined pharmacokinetic profiles. Almost all therapeutic natural products originate from plant sources. Microorganisms are diverse in numbers and widespread and can produce a substantial number of secondary metabolites. Although numerous human diseases are treated and healed by antibiotics and other microbially derived medicines, microbial products are still a valuable source for people to search for new drastic precursors for drugs. Numerous reports have evidenced that a broad range of microorganisms and their secondary metabolites display anticancer properties, especially actinomycetes, fungi, and bacteria. 174
For example, an extract of Penicillium sclerotiorum, an endophytic fungus isolated from Cassia fistula L., was shown to bring about cell cycle arrest and thus apoptosis through the activation of mitochondrial membrane depolarization in human cervical cancer cells 175 The most well-known compound of Aspergillus sydowii, gliotoxin, was also isolated from marine fungus, and polysaccharides prepared from Enterobacter cloacae also cause apoptosis of cervical cancer cells through an intrinsic apoptotic pathway, according to Nguyen and his team. 176 An active fraction of the ethyl acetate extract of Streptomyces spp. OA293 for an mTOR inhibitor was reported by Dan and colleagues, which effectively elicited Bax-mediated intrinsic apoptosis and autophagy by targeting the mTOR signaling pathway in cervical cancer cell lines. 177 Another isolated natural diterpenoid, Rosoloactone, from the endophytic fungus Trichothecium roseum of Thai ginger, showed in vitro anti-tumor efficacy against human cervical cancer cells that were deleted through endoplasmic reticulum stress and mitochondrial injury. 178
Synthetically Modified Drugs
Phytochemical compounds are now considered possibly in relation to cervical cancer remedy. Of these, plant polyphenols, which are secondary metabolites possessing polyphenolic structures, abundant in plants, have a significant antitumor effect by influencing cell proliferation, tumor development, angiogenesis, metastasis, inflammation, and apoptosis. 179 Some typical examples of polyphenolic phytoalexins that show anti-tumor properties are resveratrol, flavonoids, and anthocyanins. 180 Nevertheless, their main disadvantage is that they possess low bioavailability, which poses a challenge to their clinical use. In an effort to overcome the aforementioned problem, the researchers have directed their effort towards structural engineering of the plant polyphenols.
Other works investigate modified derivatives like flavonoid analogs (WYC02-9), 181 curcumin analogs (MS17), 182 resveratrol analogs (MPDB), 183 and anthocyanin analogs (idaein chloride), 184 for these derivatives have proved to trigger apoptosis via both intrinsic mitochondrial and extrinsic Fas receptor signals as well as cause cell cycle arrest at the G2/M phase, downregulating the E6 and E7 oncogenes in cervical cancer cells. 185 The other conceivable area that has great potential for generating inhibitors of cancer development is the synthesis of biologically active compounds, besides phytochemicals. Several compounds, including newly synthesized biphenylureas, TPD7, 186 piperazine derivatives consisting of 1-phenylpiperazine connected to 2-azetidione derivatives, 187 and quinazoline analogs, CP-31398, 188 have demonstrated promising antitumor abilities. The (1S, 4S)-2,5-diazabicyclo heptane system has been found to be more potent than the piperazine moiety in selectively inducing cancer cell death by stimulating caspase 3 and inducing apoptosis. 189 In addition, compounds 2-8, a series of triphenylstannyl 4-((arylimino)methyl)benzoates, have better cytotoxicity than cisplatin through apoptotic death, which is attributed to tin-mediated reactive oxygen species (ROS) formation. 185
Medications and Drug Combinations
At present, due to the continuous progress of scientific research, all kinds of new drugs have appeared, and the field is developing all the time, which may be worthy of encouragement for patients. Nevertheless, there remains a dearth of precise and profound comprehension of new agents and other aspects, such as concern about their use and side effects. Consequently, there are sometimes some disparities in it from clinical application, for instance, the reduction of drug efficacy or the emergence of unwanted side effects. Hence, the appearance and widespread utilization of a new drug entail a large number of clinical trials to authenticate its safety and efficacy, which will demand a great deal of time, effort, cost, and quality assets. Propofol is an ambulatory anesthetic agent used for induction as well as for maintenance of general anesthesia.
In addition to multiple anesthetic benefits, propofol has many non-anesthetic activities, among them being anti-tumor. Several works have shown that propofol possesses anticancer properties in different types of tumor cancers, including breast cancer, 190 lung cancer, 191 and other cancer diseases. In cervical cancer, propofol enhances cell apoptosis through the inhibition of the HOTAIR-mediated mTOR pathway. 192 It was also observed that propofol could improve the effect of cisplatin appearance on cervical cancer cells by inhibiting the EGFR/JAK2/STAT3 pathway. 193 Zoledronic acid is prescribed for and utilized in the management and prevention of various forms of osteoporosis, hypercalcemia of malignancy, multiple myeloma, bone metastases in solid tumors, and Paget’s disease of bone. There is evidence that zoledronic acid acts as a biological agent for cancer, as it influences tumor-associated angiogenesis and immune response and can be considered as a prospective antineoplastic agent. 194 Lately, gene interventional technology has offered an efficient medical technique for gene therapy of malignant tumors.
To meet the objective of the treatment of disease, certain approaches are employed to prevent the gene from being expressed or even to annihilate the structure of the gene. In addition to oncogenes, due to the growth of research and development of technology with the development of targets for genetic intervention, microRNAs, noncoding RNAs, and circular RNAs have their biological activity. As previous studies have pointed out, gene intervention can offset drug resistance, increase the sensitivity of chemotherapy drugs, or decrease the toxic side effects of drugs as shown in several studies. 195 For instance, they revealed that downregulation of long noncoding RNA NCK1-AS1 enhanced chemosensitization to cisplatin by enhancing apoptosis caused by cisplatin in cervical carcinoma. 196 The study also demonstrated that cervical cancer cell apoptosis induced by cisplatin may be reduced through the upregulation of GAS5 by affecting STAT3 signaling through miR-21. 197 These studies place NCK1-AS1 and GAS5 in a newly identified category of targets that may boost the chemotherapeutic outcome and survival of cervical cancer patients.
Economic Burden and Cost-Effectiveness of Cervical Cancer Prevention
Although efforts to reduce vaccine access and screening disparities are important, the economic cost burden of cervical cancer and the cost-effectiveness of prevention programs are equally important as well. Any large-scale health intervention in LMICs must be proved to be worth the expenditure of resources where they are severely constrained. 198 This is of particular relevance for vaccination and screening programs of HPV, which require significant upfront investment yet are highly cost-saving for future healthcare in the long run due to the averted costs of cervical cancer treatment. Furthermore, direct costs of cervical cancer usually relate to hospitalization, surgical intervention, chemotherapy, or palliative care. These expenditures often represent a large portion of the national health budget in LMICs, away from other essential services. 199 Absenteeism of women in their prime working years from work compounds the problem with indirect costs such as productivity loss and caregiver burdens, leaving women with prolonged absences from work or with family members quitting jobs to care for them on a long-term basis. As a result, entire households (and sometimes entire communities) are economically destabilized. Indirect costs are quantified in order to further demonstrate the criticality of preventive measures to prevent future treatment and care costs.
The evidence from cost-effectiveness studies is building that HPV vaccination for preadolescent girls is among the most financially advantageous interventions for preventing cervical cancer. 200 By contrast, simulation models that compare vaccinated and unvaccinated cohorts uniformly reveal that the reduction in disease incidence, together with diminished expenses for linked treatment, recovers the expended initial costs of vaccines. Specifically, trends are observed even when coverage is not 100%, but as long as the programs have moderate efficacy and reasonable uptake. HPV immunization is often likely to cost less than established thresholds for cost-effectiveness in LMIC contexts. Optimized screening programs also have substantial economic benefits under local conditions. 201 For example, cytology-based Pap smears are generally less sensitive but are initially more costly than HPV DNA testing. In regions with limited medical infrastructure, a single-visit combination of HPV testing with immediate treatment of positive cases (“screen and treat”) would dramatically reduce follow-up losses and the overall cost of the program. The integrated model compromises to minimize the multiple clinic visits, reduces transportation expenses incurred by patients, reduces dropout rates, and reduces healthcare worker utilization. In the long run, decision makers consider these savings vs what would otherwise occur as a surge in late-stage cervical cancer treatment, and high-sensitivity screening tests are often the more cost-effective choice.
Conclusion
Cervical cancer to date continues to be a major problem, with nearly half a million deaths occurring annually, a number that is expected to increase, especially in LMICs, due to increasing cancer incidence rates among women. Advances in screening techniques, including PAP smears and human papillomavirus DNA testing, and the efficacy of human papillomavirus vaccination have enhanced early diagnosis and prevention. Also, molecular diagnostics and immunotherapy have enhanced therapy options for metastatic cervical carcinoma. However, emerging issues suggest that it is still necessary to make efforts to enhance diagnostics, prophylactics, and therapies in the context of the respective pathology. Practices and measures against cervical cancer are expected to be promoted not only through medical research and development but also through vigorous policies and powerful healthcare systems. Thus, preventive educational crusades covering matters such as vaccination, screening, and awareness play a vital role in minimizing the disease effects across the society. Additionally, stronger cooperation with higher authorities and with other healthcare practitioners and governments should also actively be made throughout the world in order to utilize the great achievements in prevention and treatment for all, with no respect to the geographical or economic status. More effort, research, and funding commitments are required to consolidate and extend the achievements made over the last few years at national and international levels. Finally, this paper found that eradicating cervical cancer as a public health issue, as the WHO has set it for 2030, requires concerted international action. It ought to embark on equal vaccination, improvement of the screening programs, health awareness campaigns, and new drug target identification, among others. Closure of these gaps will not only decrease the disease load but also contribute towards a holistic approach to managing other HPV-associated cancers.
Footnotes
Acknowledgements
A special thanks to the the corresponding author Dr S M Bakhtiar UL Islam for his supervision in the manuscript. His active involvement and assistance in nurturing the idea and monitoring the progress substantially enhanced the quality of the manuscript.
Author Contribution
RUH, TA and SMBUI conceived the idea and prepared the outline of the review. RUH and TA performed the literature search and data extraction, analysis of extracted data and manuscript preparation. SMBUI supervised the manuscript preparation and prepared the final draft. The authors read and accepted the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declarations Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.