
Abstract
Background
Limited-stage small cell lung cancer (LS-SCLC) is a highly aggressive tumor characterized by a poor prognosis. While concurrent chemoradiotherapy (CCRT) remains the standard treatment, the high rates of recurrence and poor long-term survival highlight the pressing need for novel therapeutic approaches.
Purpose
In recent years, the introduction of immunotherapy, particularly immune checkpoint inhibitors (ICIs), has opened new avenues for the treatment of LS-SCLC. This review highlights the clinical advancements of ICIs in CCRT, consolidation therapy, and neoadjuvant therapy, emphasizing their potential to improve progression-free survival (PFS) and overall survival (OS). This review also discusses management of immunotherapy-related side effects.
Research Design
This is a review article that synthesizes recent research findings on immunotherapy for LS-SCLC.
Study Sample
Not applicable (review of existing literature).
Data Collection and/or Analysis
This review summarizes key studies exploring the application of immunotherapy in limited-stage small cell lung cancer.Additionally, it examines the role of the tumor microenvironment, tumor mutation burden (TMB), and Programmed cell death 1 ligand 1(PD-L1) as biomarkers for predicting the efficacy of immunotherapy.
Results
This review emphasizes their potential to improve PFS and OS.
Conclusions
Despite the significant advancements in research, the use of ICIs in LS-SCLC continues to face challenges, including the identification of optimal treatment regimens, validation of long-term efficacy, and development of personalized predictive biomarkers. Future research should prioritize large-scale, multicenter clinical trials to refine combination therapy strategies, establish customized treatment approaches, and enhance patient outcomes.
Introduction
Lung cancer remains a leading cause of cancer-related mortality worldwide, with small-cell lung cancer (SCLC) recognized as one of the most aggressive and lethal subtypes. SCLC is distinguished by its highly invasive behavior and rapid growth, frequently leading to early and extensive metastasis. This subtype accounts for approximately 10-15% of all lung cancer cases. 1 According to the two-stage classification system established by the Veterans Administration Lung Cancer Study Group, SCLC is categorized into limited-stage (LS-SCLC) and extensive-stage (ES-SCLC). LS-SCLC is a defined as disease confined to one side of the chest, where all tumors can be encompassed within a single radiation field. 2 In contrast, the American Joint Committee on Cancer staging system classifies LS-SCLC as stages I through III (any T, any N, M0), provided the disease remains amenable to curative doses of radiation therapy. However, this excludes cases involving multiple pulmonary nodules or large tumor volumes (T3-T4) that cannot be fully encompassed within a tolerable radiation plan. The standard treatment for LS-SCLC involves platinum-based chemotherapy combined with concurrent chemoradiotherapy (CCRT). 3 According to the National Comprehensive Cancer Network guidelines, for patients who respond well to initial treatment (such as chemotherapy and radiotherapy), particularly those who achieve complete response (CR) or partial response (PR), prophylactic cranial irradiation (PCI) is recommended to reduce the high risk of brain metastasis, even in the absence of radiological evidence of brain involvement. 4 Although chemoradiotherapy achieves a high initial tumor response rate, with CR rates of 70-80%, most patients experience local recurrence or distant metastasis within 6 to 12 months after treatment. Post-recurrence treatment options are limited, and the prognosis remains poor for the majority of these patients, with a 5-year survival rate below 20%. 5 Based on the landmark findings of the IMpower-133 and CASPIAN studies, the U.S. Food and Drug Administration (FDA) approved the programmed cell death-ligand 1 (PD-L1) immune checkpoint inhibitors (ICIs), atezolizumab and durvalumab, for use in combination with platinum-based drugs and etoposide as a first-line treatment for ES-SCLC.6,7 This breakthrough provides a new direction for the treatment of LS-SCLC. LS-SCLC remains an urgent medical challenge due to its high recurrence rate and poor prognosis, driving the need for new treatments like immunotherapy. Currently, several clinical trials involving ICIs are underway. This review summarizes the clinical immunotherapy studies in LS-SCLC, covering three main stages: CCRT, consolidation therapy, and neoadjuvant therapy. It also briefly discusses the predictive role of biomarkers in immunotherapy, intending to provide data support for clinical applications.
Combined Strategies of Immunotherapy and Conventional Therapy
Optimization of Standard Treatment for Limited-Stage Small Cell Lung Cancer
The early management of LS-SCLC has evolved from unimodal therapy to CCRT, which now represents the standard of care. Pioneering studies in the 1990s established the superiority of CCRT over sequential approaches. A landmark Canadian trial demonstrated that early initiation of thoracic radiotherapy (cycle 2 vs cycle 6 of chemotherapy) significantly improved median OS (OS: 21.2 vs 16.0 months, P = .008) and PFS (PFS: 15.4 vs 11.8 months, P = .036).
8
Subsequent phase III trials confirmed that CCRT should commence within the first two chemotherapy cycles.9,10Radiation dose and fractionation were further refined through pivotal studies. The Intergroup 0096 trial established twice-daily radiotherapy (45 Gy in 1.5 Gy fractions BID) as a benchmark, achieving a 5-year survival rate of 26% compared to 16% with once-daily regimens.
11
Although later trials (CONVERT, RTOG 0538) found no survival difference between 45 Gy BID and 66-70 Gy QD regimens,12,13 current guidelines recommend both protocols for LS-SCLC patients based on equivalent efficacy and toxicity profiles.12,14Despite these advancements, CCRT outcomes remain suboptimal, with 5-year survival rates stagnating below 30%. Consequently, novel strategies integrating immunotherapy are urgently needed to transform LS-SCLC management. The developmental timeline of LS-SCLC therapeutics is summarized in Figure 1.
Prophylactic Cranial Irradiation
PCI in LS-SCLC has long been considered standard due to the high risk of brain metastasis (50%-70%). However, its necessity has become contentious with the widespread adoption of brain Magnetic Resonance Imaging (MRI) surveillance. Current debates center on three key aspects: (1) The challenge of PCI’s survival benefit in the era of advanced imaging. A retrospective study 19 demonstrated that while PCI reduces brain metastasis risk, it fails to improve OS compared to routine brain MRI monitoring, suggesting MRI surveillance may be preferable for LS-SCLC. (2) Neurocognitive toxicity concerns. The NRG CC001 trial 20 confirmed that hippocampal-avoidance PCI (HA-PCI) mitigates cognitive decline, though its impact on metastasis control requires validation. An ongoing prospective study (NCT02635009) 21 is further evaluating hippocampal-sparing approaches. (3) Individualized patient selection challenges, particularly for elderly (>65 years) or neurologically compromised patients who risk quality-of-life deterioration from side effects, compounded by the lack of validated predictive biomarkers. The therapeutic landscape has been reshaped by immunotherapy breakthroughs, exemplified by the ADRIATIC study where durvalumab consolidation extended median OS to 55.9 months, potentially diminishing PCI’s relevance. Current dilemmas involve balancing efficacy against neurotoxicity, insufficient evidence for alternative strategies (e.g., MRI-guided stereotactic radiotherapy), and the absence of precision biomarkers. Future directions include optimizing radiotherapy techniques (HA-PCI with intensity modulation), exploring synergies between immunotherapy (e.g., durvalumab) and PCI, and conducting head-to-head phase III trials comparing PCI plus surveillance vs surveillance alone. Modern PCI implementation requires personalized risk-benefit assessment: younger patients with good performance status may benefit from HA-PCI, while elderly or neurocognition-risk-averse patients could opt for MRI surveillance.
Immunotherapy and Radiation Therapy Synergism
The rationale for combining ICIs with CCRT lies in the ability of radiotherapy to induce tumor antigen release and activate dendritic cells via Deoxyribonucleic Acid damage and Stimulator of Interferon Genes pathway signaling, thereby orchestrating a pro-inflammatory “hot” tumor microenvironment.22,23 Specific mechanisms are illustrated in Figure 2. Through these complex mechanisms, radiotherapy can enhance the efficacy of immunotherapy. The clinical effectiveness of combining radiotherapy with ICIs has been demonstrated in early-stage non-small cell lung cancer (NSCLC), where the 4-year relapse-free survival rate increased from 53% to 77%, with a hazard ratio (HR) of 0.3.
24
In addition, a synergistic effect has been initially observed in patients with ES-SCLC, demonstrating the potential to prolong survival.
25
The clinical study results of combining ICIs with CCRT in LS-SCLC patients are promising and may expand treatment options for this patient population. While combination therapy strategies have significantly advanced cancer treatment, they also introduce potential adverse reactions, especially when immunotherapy, chemotherapy, and radiotherapy are used in alternation. Managing these side effects becomes particularly complex in such cases. Understanding these potential complications is essential for both the treatment and prognosis of patients. Cisplatin and etoposide combined with CCRT remain the standard treatment regimen for LS-SCLC. Common side effects include fatigue, myelosuppression, esophagitis, and gastrointestinal discomfort. Severe adverse reactions may also occur, such as febrile neutropenia, severe esophagitis, and pneumonia.
12
When platinum-based chemotherapy or etoposide is combined with ICIs, immune-related adverse effects may occur, including rash, hypothyroidism, hepatitis, and infusion reactions. Severe side effects, such as pneumonia and diarrhea/colitis, may also arise. In the treatment of LS-SCLC, the addition of chest radiotherapy may increase the risk of pulmonary toxicity (e.g., pneumonia), though further investigation is needed.6,7 To better assess safety, clinical trials should specifically focus on pulmonary adverse events (AEs) and consider the implementation strategies and pacing of different treatment regimens. (A). Anti-PD1 Immunotherapy Enhances T Cell-Mediated Tumor Killing. (B) Radiation-Induced Immune Activation via DAMP Signaling and the cGAS-STING Pathway. Radiotherapy Induces DNA Damage in Tumor Cells, Triggering the Release of Tumor-specific Antigens and Damage-Associated Molecular Patterns. These Signals Promote the Maturation of Dendritic Cells and Enhance Their Antigen-Presenting Function, Thereby Activating Natural Killer Cells, CD4 + T Cells, and CD8 + T Cells to Strengthen the Anti-Tumor Immune Response. Abbreviations: DAMPDamage-Associated Molecular pattern; DC, Dendritic Cell; cGAS, Cyclic GMP-AMP Synthase; STING, Stimulator of Interferon Genes; CTL, Cytotoxic T Lymphocyte; IFN, Interferon; NF-κB, Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells; HMGB1, High Mobility Group Box 1; TCR, T Cell Receptor; MHC, Major Histocompatibility Complex; PD-1, Programmed Cell Death Protein 1; PD-L1/2, Programmed Death-Ligand 1/2; APC, Antigen-Presenting Cell.
Frontier Exploration of Immunotherapy in Limited-Stage Small Cell Lung Cancer
Consolidation Therapy after Concurrent Chemoradiotherapy
Specific Information on the Clinical Trial of Immunotherapy Combined With CCRT and Immunotherapy Consolidation for LS-SCLC.
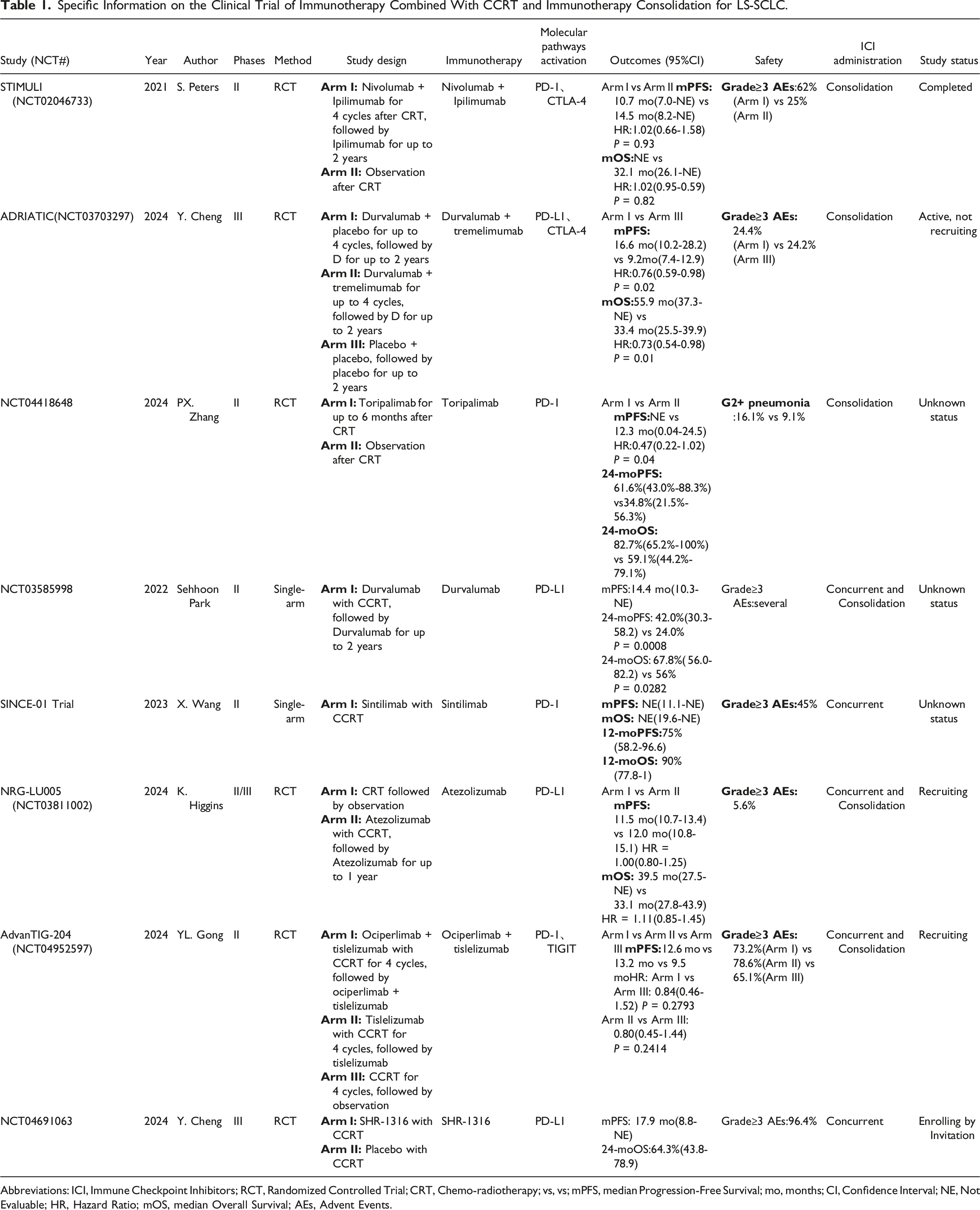
Abbreviations: ICI, Immune Checkpoint Inhibitors; RCT, Randomized Controlled Trial; CRT, Chemo-radiotherapy; vs, vs; mPFS, median Progression-Free Survival; mo, months; CI, Confidence Interval; NE, Not Evaluable; HR, Hazard Ratio; mOS, median Overall Survival; AEs, Advent Events.
Concurrent Chemoradiotherapy Combined Treatment
The incorporation of immunotherapy during the induction treatment phase represents an innovative strategy for managing LS-SCLC. Preliminary findings from several small-sample studies have been reported. A phase II study assessed the efficacy and safety of durvalumab in combination with CCRT. The study reported a median PFS of 14.4 months(95%CI:10.3-NE), while OS had not yet been reached. The 24-month PFS and OS rates were 42% and 67.8%, respectively. Patients who received PCI experienced a significantly lower incidence of brain metastases (13.6% vs 42.9%). 30 The treatment was generally well-tolerated, with common AEs, including immune-related hepatitis, pancreatitis, and fatigue, effectively managed through supportive care. These findings suggest that durvalumab combined with CCRT has the potential to improve survival outcomes while maintaining a manageable safety profile, supporting the need for further validation. Another single-arm phase II study assessed the efficacy and safety of sintilimab in combination with CCRT. The study enrolled 20 patients and reported 2-year PFS and OS rates of 59.1% and 69.3%, respectively. Grade ≥3 AEs were observed in 45% of patients, while immune-related adverse events (irAEs) occurred in 35% (7 cases), primarily presenting as pneumonia, liver function impairment, hyperglycemia, and hypothyroidism. Furthermore, 30% of patients experienced radiotherapy-related adverse reactions. 31 At recent annual meetings of the American Society for Radiation Oncology and the American Association for Cancer Research, findings from the NRG-LU005 and AdvanTIG-204 studies showcased the latest progress in integrating immunotherapy with chemoradiotherapy for LS-SCLC. The NRG-LU005 study demonstrated that adding atezolizumab to CCRT did not result in a significant improvement in overall OS. With a median follow-up of 21 months, the 3-year survival rate in the combination therapy group was 44.7%, compared to 50.3% in the group receiving chemoradiotherapy alone. 32 The AdvanTIG-204 study demonstrated the potential benefit of combining tislelizumab with chemoradiotherapy in improving PFS. The median PFS was 13.2 months in the combination therapy group compared to 9.5 months with chemoradiotherapy alone [HR:0.80(0.45-1.44); P = .2414]. Safety analysis revealed that TRAEs, such as fatigue and anemia, were generally manageable. These findings offer valuable insights for optimizing future treatment strategies for LS-SCLC. 33 The SHR-1316-III-302 study is a phase III RCT designed to evaluate the efficacy of adebrelimab in combination with CCRT for LS-SCLC. Adebrelimab was administered alongside chemotherapy starting from the first cycle, while thoracic radiotherapy began with the third cycle. The study included two phases: a safety lead-in phase and a randomized controlled phase. Results from the safety lead-in phase, presented at this year’s European Society For Medical Oncology (ESMO), involved 28 patients. The most common AEs were hematologic toxicities, with treatment-related pneumonia reported in 14.3% of patients, all of which were grade 2. No unexpected toxicities were observed. The median PFS was 17.9 months(95%CI:8.8-NE), and the 2-year OS rate was 64.3%. 34 These findings support the continuation of randomized controlled trials, with patient enrollment for the current phase now complete. Whether initiating immunotherapy during the induction treatment phase can improve survival outcomes for LS-SCLC while maintaining a favorable safety profile remains uncertain and will be clarified by the results of these phase III trials.
Poly(ADP-ribose) polymerase (PARP)inhibitors exert their effects by disrupting Deoxyribonucleic Acid (DNA) repair pathways, resulting in the accumulation of DNA damage in tumor cells. This damage activates the cGAS-STING signaling pathway, triggering the expression of inflammation-related genes, including interferon-β and IL-10, which promote the recruitment and activation of T cells. Furthermore, DNA damage caused by PARP inhibitors upregulates PD-L1 expression, potentially enhancing the effectiveness of PD-1/PD-L1 inhibitors.35,36 A single-arm phase II study showed that olaparib combined with durvalumab exhibited limited antitumor activity, with PR observed in some patients. The objective response rate (ORR) was 10.5%, while the median PFS and OS were 1.8 months and 4.1 months, respectively. 37 Considering the potential synergy between PD-1/PD-L1 inhibitors and PARP inhibitors, a phase III trial is currently underway to assess the efficacy of pembrolizumab combined with CCRT, followed by consolidation therapy with pembrolizumab ± olaparib, in patients with LS-SCLC. The combination of immunotherapy and PARP inhibitors has introduced new possibilities for the treatment of LS-SCLC. In the era of precision medicine, this strategy holds promise as a vital component of personalized treatment approaches. However, challenges persist regarding efficacy, biomarker validation, and the management of adverse effects, underscoring the need for larger-scale clinical trials and in-depth mechanistic studies to address these issues.
At present, 10 registered clinical trials are evaluating combination therapies during the CCRT phase in LS-SCLC. Most of these studies focus on ICIs, while others investigate anti-angiogenic targeted agents and PARP inhibitors. Supplemental Table 2 presents a comprehensive summary of these trials.
Neoadjuvant Immunotherapy
In recent years, neoadjuvant immunotherapy has been successfully utilized in the treatment of various cancers, including NSCLC, triple-negative breast cancer (TNBC), and other malignancies. Based on the results of the KEYNOTE-671 and CheckMate-816 studies, the National Medical Products Administration has approved the use of pembrolizumab and nivolumab as neoadjuvant immunotherapies for resectable NSCLC.38,39 In the field of TNBC, the results of the KEYNOTE-522 trial have shown that pembrolizumab combined with chemotherapy has been approved as a neoadjuvant treatment for high-risk early-stage TNBC, significantly improving the pathological complete response (pCR) rate. 40 Building on its successful application in NSCLC, TNBC, and melanoma, its potential use in LS-SCLC represents a promising frontier in cancer treatment. As a result, researchers are actively exploring the application of neoadjuvant immunotherapy in LS-SCLC. A study presented at the 2024 ESMO conference compared the efficacy and safety of neoadjuvant immunochemotherapy (neoCIT) with neoadjuvant chemotherapy (neoCT). The findings revealed a significantly higher pCR rate in the neoCIT group(50.0%,95%CI:28.0-72.0) compared to the neoCT group (6.7%, 95%CI:0.3-29.8)[odds ratio(OR):14.00;95%CI:1.71-164.20;P = .016)]. Similarly, the major pathologic response (MPR) rate in the neoCIT group was 87.5%(95%CI:64.0-97.8), markedly exceeding the 20.0%(95%CI:7.0-45.2)observed in the neoCT group [OR:28.00;95%CI:4.23-150.50;P < .001)]. After 24 months of follow-up, the event-free survival (EFS) rate was 87.5% in the neoCIT group vs 46.2% in the neoCT group(95%CI:0.06-0.78;HR:0.20). 41 These findings suggest that the neoCIT regimen provides survival and safety advantages, highlighting the potential value of neoadjuvant immunochemotherapy in the treatment of LS-SCLC. In another retrospective study presented at the ASCO conference, 21 patients with LS-SCLC underwent 2 to 6 cycles of neoadjuvant chemotherapy combined with immunotherapy, achieving a pCR rate of 42.9% and an MPR rate of 47.6%. The overall R0 resection rate was 95.2%, with a rate of 94.1% , specifically among stage III patients. 42 After a median follow-up of 11.2 months, the recurrence rate remained low, and the median disease-free survival had not yet been reached, demonstrating the promising efficacy and feasibility of this regimen. Further studies are required to validate its long-term benefits. Another multicenter single-arm study (neoSCI) investigated the efficacy of atezolizumab combined with chemotherapy as a neoadjuvant or conversion therapy for LS-SCLC. Preliminary results revealed a pCR rate of 61.5% and an MPR rate of 92.3% among 13 patients, 43 suggesting that neoadjuvant immunotherapy may achieve a high pCR rate in LS-SCLC. The LungMate-005 study assessed the safety and efficacy of TQB2450 combined with chemotherapy as induction therapy, followed by surgery or radiotherapy in patients with LS-SCLC. The study included 40 patients with stage III disease. In the surgery group, the pCR rate was 42.9%, and the MPR rate was 61.9%, with 81% of patients achieving downstaging. The 1-year EFS and OS rates in the surgery group were 82.0% and 100%, respectively, significantly higher than the 49.2% and 88.9% observed in the radiotherapy group. 44 This study demonstrated the survival benefits of the surgery group, and a phase III randomized controlled trial (RCT) is currently in progress. In summary, neoadjuvant immunotherapy combined with chemotherapy has demonstrated promising potential in the treatment of LS-SCLC. Ongoing clinical trials (Supplemental Table 3) are further investigating its long-term efficacy and safety, providing essential evidence to optimize treatment strategies for LS-SCLC.
Emerging Advances in Other Immunotherapies
DLL3-Targeting Bispecific T-Cell Engager
Tarlatamab (AMG 757), a bispecific antibody targeting Delta-like ligand 3 (DLL3) and CD3, activates T cells to selectively eliminate DLL3-expressing SCLC cells. DLL3 is highly expressed in 80%–85% of SCLC tumors but exhibits minimal expression in normal tissues, conferring exceptional target specificity. A 2024 study 45 demonstrated that Tarlatamab achieved an ORR of 40% and a median OS exceeding 12 months in patients with relapsed/refractory SCLC, alongside favorable tolerability. Additionally, a phase 3 RCT (NCT06117774) is currently underway to evaluate Tarlatamab as consolidation therapy in LS-SCLC.
Antibody-Drug Conjugates
Recent advances in antibody-drug conjugates (ADCs), such as sacituzumab govitecan, have demonstrated promising efficacy in metastatic SCLC. Sacituzumab govitecan is a humanized anti-Trop-2 antibody conjugated to SN-38, the active metabolite of irinotecan. In a phase II trial involving 50 heavily pretreated patients, ADC-targeted therapy induced tumor reduction in 60% of participants, with an ORR of 14% and a median duration of response (DoR) of 5.7 months, highlighting its potential as a novel therapeutic option. 46 Furthermore, updated results from a phase I/II study 47 presented at the 2023 ESMO Congress revealed that treatment with ifinatamab deruxtecan (I-DXd; DS-7300) achieved an ORR of 52.4%, a mPFS of 5.6 months, and a median OS of 12.2 months in extensively pretreated SCLC patients, suggesting its potential to address the historically poor prognosis and limited survival outcomes in this population. However, additional large-scale studies are warranted to validate these findings.
Immunocellular Therapies
(1) CAR-T Cell Therapy: Recent advances in chimeric antigen receptor (CAR)-T cell therapy targeting DLL3 have demonstrated significant antitumor activity in preclinical models. A 2022 study
48
confirmed that DLL3-CAR-T cells effectively eradicated SCLC xenografts and prolonged survival in murine models. A phase I clinical trial (NCT05680922)
49
is currently underway to evaluate this approach in humans, with results eagerly anticipated.
The immunotherapy landscape for LS-SCLC is transitioning into a multimodal era, with emerging strategies such as DLL3-targeted bispecific antibodies and CAR-T therapies showing promise. Concurrently, ADC and combination approaches are expanding therapeutic options. However, large-scale clinical trials are imperative to validate long-term efficacy, address resistance mechanisms, and optimize toxicity management.
Predictive Biomarkers for Immunotherapy in Small Cell Lung Cancer
SCLC is highly aggressive and is often diagnosed at an advanced stage, making treatment challenging and leading to poor survival outcomes. In recent years, immunotherapy, remarkably ICIs, has emerged as a promising treatment option for SCLC. To develop more precise immunotherapy strategies, researchers are actively investigating specific biomarkers. These biomarkers may consist of molecules, cells, or genetic components found in bodily fluids, on cell surfaces, or within other biological contexts. Despite the promising potential of immunotherapy in SCLC, identifying effective predictive biomarkers remains a major clinical challenge. Current research predominantly focuses on ES-SCLC, while studies targeting LS-SCLC, particularly in the context of predictive biomarkers, are relatively scarce. This section will explore the currently identified predictive biomarkers associated with immunotherapy in SCLC, with a specific emphasis on those relevant to LS-SCLC.
Tumor Microenvironment-Related Biomarkers
The composition of the tumor microenvironment, particularly the various subsets of tumor-infiltrating lymphocytes (TILs), plays a critical role in shaping the response to immunotherapy. However, there is currently insufficient evidence to support the use of any single component as a definitive predictive biomarker in clinical practice. Studies have demonstrated that higher levels of tumor infiltration and tumor-associated lymphocytes, including elevated expression of markers such as CD3, CD20, and CD45, are associated with improved prognosis and higher OS rates, regardless of disease stage or surgical feasibility.52-55 In contrast, SCLC patients with a higher proportion of FOXP3 + cells are associated with poorer prognoses. Conversely, patients with better outcomes often exhibit a higher proportion of CD45RO + memory T cells within the TIL population. As the tumor microenvironment consists of various cell types, including dendritic cells, myeloid-derived suppressor cells, macrophages, and neutrophils, future research should focus on exploring the expression patterns of other immune cell markers and immune-active proteins, such as immune checkpoints and cytokines, to improve the efficacy of immunotherapy.55-59
Tumor Mutation Burden
The high somatic mutation rate in SCLC is frequently linked to defects in DNA repair mechanisms. These mutational characteristics are primarily driven by genetic alterations caused by long-term smoking, along with chronic inflammation and exposure to chemical compounds in cigarette smoke. Tumor mutational burden (TMB) has been recognized as an important predictive factor for immunotherapy, particularly in melanoma and NSCLC. This indicates that TMB may also have potential as a predictive biomarker in SCLC.60-62 Research findings indicate that TMB is a promising predictive biomarker for checkpoint inhibitor therapy, particularly in metastatic SCLC. It is also regarded as the first reliable tissue biomarker for immune checkpoint blockade in this context. Moreover, studies suggest that patients with higher TMB levels, observed in approximately one-quarter of SCLC cases, may experience durable clinical benefits from treatment with nivolumab monotherapy or nivolumab combined with ipilimumab.63-65 However, challenges in current clinical practice include obtaining high-quality biopsy samples and conducting in-depth analyses of mutational characteristics. While biomarkers such as TMB and PD-L1 expression hold theoretical promise for guiding immunotherapy in LS-SCLC, their clinical application faces significant challenges. Although TMB is mechanistically linked to neoantigen burden and immune activation, methodological discrepancies in its quantification across sequencing platforms and tissue samples persist. The absence of standardized thresholds defining “high” vs “low” TMB in SCLC creates ambiguity in clinical decision-making, compounded by the difficulty of obtaining sufficient tumor tissue for genomic analysis in this biopsy-averse malignancy. Furthermore, the temporal dynamics of TMB during treatment and its spatial heterogeneity within tumors raise concerns about the reliability of single-timepoint assessments. Consequently, future investigations should prioritize the standardization of detection protocols and precise characterization of mutational signatures to refine the clinical utility of TMB as a predictive biomarker for immunotherapy in SCLC.
PD-L1 Expression
The interaction between PD-1 and PD-L1 is a key mechanism by which tumors evade immune surveillance. In various solid tumors, PD-L1 expression on the surface of tumor cells is regarded as an important indicator for predicting the efficacy of PD-1 inhibitors. While some studies have suggested that high PD-L1 expression is associated with limited-stage disease and improved prognosis, its predictive value in SCLC patients remains unclear. 66 This controversy primarily stems from the heterogeneity and low expression rate of PD-L1. Some research suggests that PD-L1 expression in the stroma may be more predictive than its expression in tumor cells. However, multiple clinical trials have shown no significant correlation between PD-L1 expression levels and the clinical efficacy of chemotherapy combined ICIs.64,67-69 This suggests that PD-L1 expression is not a reliable predictive biomarker for SCLC patients undergoing chemotherapy combined with ICIs. PD-L1 expression exhibits significant limitations in LS-SCLC. Unlike NSCLC, where frontline immunotherapy decisions are guided by PD-L1 immunohistochemistry, SCLC demonstrates low PD-L1 positivity rates (most studies report <20%) with pronounced intratumoral and intertumoral heterogeneity. The stromal localization of PD-L1 + immune cells—rather than tumor cells—complicates scoring interpretation, while transient induction by prior chemoradiation may confound predictive value. Considering the biological heterogeneity and plasticity of SCLC, future research should extend beyond PD-L1 evaluation to explore broader biomarkers that can effectively guide personalized immunotherapy strategies for SCLC patients.70-73
TIGIT
TIGIT is a poliovirus receptor-like protein characterized by a cytoplasmic domain, an extracellular variable immunoglobulin domain, a type I transmembrane domain, and a cytoplasmic tail. The cytoplasmic tail contains two inhibitory motifs conserved in both mice and humans: the immunoreceptor tyrosine-based inhibitory motif ITIM and the immunoglobulin tyrosine tail ITT-like motif.74,75 TIGIT is highly expressed in NSCLC tumor tissues and TILs and is associated with poor prognosis. Patients with elevated TIGIT expression typically have shorter OS and PFS. Mechanistically, TIGIT inhibits CD8+ T cell function by binding to CD155, resulting in reduced proliferation, cytotoxicity, and cytokine secretion. Furthermore, TIGIT enhances the immunosuppressive function of regulatory T cells (Tregs), thereby suppressing anti-tumor immune responses and promoting tumor immune evasion. 76 Studies have shown that TIGIT/CD155 is highly expressed in SCLC tumor tissues. Moreover, TIGIT expression is strongly correlated with CD8+ T cell infiltration and PD-1 expression on T cells. Patients with overexpression of TIGIT/CD155 in SCLC have shorter PFS and OS. 77 Further research investigating TIGIT as a biomarker or therapeutic target in limited-stage SCLC is needed to better understand its role and therapeutic potential.
BTLA-4
B- and T-lymphocyte attenuator-4 (BTLA-4) is an immune checkpoint molecule that interacts with its ligand HVEM to inhibit T cell activation and proliferation, thereby modulating the body’s antitumor immune response. BTLA is expressed in NSCLC tumor tissues, with higher expression observed in patients with clinical risk factors, and is positively correlated with PD-L1 expression. Elevated BTLA expression, or concurrent positivity for both BTLA and PD-L1, is associated with shorter relapse-free survival and OS, suggesting that high BTLA expression may indicate poorer prognosis in NSCLC patients. BTLA has the potential to serve as a new target for immunotherapy, and combined blockade of BTLA and PD-L1 could offer a more effective treatment strategy, potentially opening new avenues for lung cancer therapy. 78 Studies suggest that lung cancer patients with high BTLA-4 expression may be more responsive to ICIs therapy, while those with low expression may show poorer treatment outcomes. 78 Assessing the expression levels of BTLA-4 in tumor tissues or blood samples from lung cancer patients could provide clinicians with valuable information regarding disease progression and prognosis, aiding in more informed treatment decisions.
MRD
Research on the clinical utility of minimal residual disease (MRD) detection in NSCLC, particularly for efficacy evaluation, recurrence monitoring, and prognosis prediction in early-stage NSCLC, has demonstrated promising advantages.79,80 However, investigations into MRD applications in SCLC remain scarce. A recent prospective study revealed that patients in the post-radiotherapy MRD-cleared subgroup exhibited superior PFS (PFS: 16.53 months vs 9.70 months; HR = 0.37; P = .01) OS (OS: not reached [NR] vs 22.77 months; HR = 0.26; P = .01) compared to those in the MRD-persistent subgroup. Notably, no significant differences in PFS or OS were observed between the pre-radiotherapy circulating tumor DNA (ctDNA)-negative and post-radiotherapy MRD-cleared subgroups. Of particular interest, among 46 patients with post-radiotherapy MRD negativity, two exhibited MRD re-emergence following PCI, with rapid confirmation of disease progression through imaging at 2.47 and 2.65 months after MRD recurrence, indicating significantly higher relapse risk compared to PCI-treated patients maintaining MRD negativity. 81 This prospective study represents the first systematic evaluation of the prognostic value of ctDNA-based MRD monitoring in a large cohort of LS-SCLC patients undergoing chemoradiotherapy. These findings suggest substantial potential for MRD-guided clinical management in LS-SCLC. However, these possibilities remain speculative, and further exploration is imperative to validate MRD’s clinical utility in SCLC. With the accumulation of additional evidence from ongoing studies, MRD monitoring is anticipated to transition into clinical practice, ultimately enabling more precise and personalized therapeutic strategies for SCLC patients.
Other Potential Predictive Biomarkers
In SCLC, various inflammatory cytokines and immune markers are considered potential predictive biomarkers for immunotherapy response. These include interleukin-2 (IL-2), interleukin-4 (IL-4), tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), the pulmonary immune prognostic index (LIPI), the neutrophil-to-lymphocyte ratio, the platelet-to-lymphocyte ratio (PLR), galectin-9, and human leukocyte antigen expression. One study assessed the value of inflammatory cytokines as predictive indicators of immunotherapy response by comparing SCLC patients treated with chemotherapy alone vs chemotherapy combined with ipilimumab. The results revealed changes in the levels of several cytokines. Specifically, elevated IL-2 and IL-4 levels were associated with improved OS, while high levels of TNF-α and IL-6 were linked to resistance to ipilimumab treatment. 82 Additionally, a multicenter retrospective study demonstrated a significant association between pre-treatment LIPI and poor outcomes with ICI therapy. 83 Recent studies have further confirmed the predictive value of LIPI in SCLC, showing correlations with both PFS and OS. 84 Paraneoplastic syndromes (PNS) are closely associated with a “hot” tumor microenvironment and may influence a patient’s immune response. In a prospective study, Maddison et al 85 found that a higher proportion of patients with neuronal antibodies and neurological PNS survived beyond 48 months in limited-stage disease. Another phase II study evaluating ipilimumab combined with carboplatin and etoposide showed that ANNA-1-positive patients had significantly prolonged PFS (10.2 months vs 6.9 months, P = .032), 86 suggesting that positive neuronal antibodies, such as ANNA-1, may indicate a better prognosis in SCLC patients. Gay C.M. et al. 87 categorized SCLC into four subtypes: SCLC-A (ASCL1), SCLC-N (NEUROD1), SCLC-P (POU2F3), and SCLC-I. The SCLC-I subtype, characterized by high expression of immune-related genes, exhibited significant CD8A- and CD8B-mediated immune infiltration and was more likely to benefit from immunotherapy. Other promising prognostic markers include the density of T-cell receptors on T lymphocytes and the methylation status of circulating free DNA. Further prospective studies are needed to confirm the clinical utility of these markers and optimize personalized treatment strategies for SCLC patients.70,88
Research on predictive biomarkers for immunotherapy in LS-SCLC remains relatively limited, but some evidence suggests that specific biomarkers may have potential clinical value. At the 2024 ASCO conference, a study evaluated Cyclin-Dependent Kinase 7
Summary
SCLC is among the most aggressive and malignant subtypes of lung cancer. While patients with LS-SCLC often exhibit high tumor response rates to initial treatment with conventional CCRT, their long-term survival rates remain low, and recurrence rates are high. In recent years, the introduction of ICIs has offered new promise in treatment. When combined with CCRT, ICIs have shown the potential to improve PFS and OS, with particularly notable effects in consolidation therapy. The ADRIATIC study highlights how immunotherapy is transforming the treatment landscape of LS-SCLC and driving further investigation into immunotherapy strategies. These advancements have also encouraged researchers to reevaluate the role of surgery in the management of LS-SCLC. Additionally, biomarkers such as the tumor microenvironment, TMB and PD-L1 expression demonstrate potential clinical value in predicting immunotherapy outcomes. However, the application of biomarkers in LS-SCLC continues to face substantial challenges. Current biomarkers (e.g., TMB, PD-L1) exhibit dual limitations in LS-SCLC: biologically, they are constrained by dynamic tumor microenvironment alterations (e.g., radiotherapy-induced immune phenotypic remodeling), while technically, standardized detection protocols remain lacking. More critically, all existing biomarker studies rely on retrospective analyses or extrapolation from extensive-stage SCLC data, with an absence of prospective validation cohorts specific to LS-SCLC. Future investigations should prioritize multimodal integration strategies, including: (1) temporal biomarker profiling via longitudinal ctDNA monitoring to track therapeutic sensitivity evolution; (2) spatial heterogeneity correction through multiplex fluorescence immunohistochemistry to map immune cell topological distributions; and (3) host-tumor interplay analysis incorporating gut microbiota and systemic inflammatory indices with tumor-intrinsic features. The stability and predictive validity of such biomarkers warrant rigorous prospective evaluation to advance personalized therapeutic paradigms in LS-SCLC. Furthermore, managing and preventing immunotherapy-related side effects in LS-SCLC is critical. Patients often have reduced tissue repair ability after chemoradiotherapy, leading to side effects that differ from other lung cancers. However, key challenges remain. First, we lack clear criteria to distinguish radiation-induced pneumonitis from immune-related pneumonitis. Second, the role of corticosteroids in preventing radiation esophagitis while managing colitis is unclear. Third, tools to predict risks based on organ function or biomarkers are missing. To address these challenges, future research must prioritize LS-SCLC-specific irAEs investigations, focusing on three key developments: radiomics-based models for early discrimination between radiotherapy-induced damage and immune-driven inflammation; novel immunomodulators targeting pathways such as IL-6/JAK-STAT to achieve selective anti-inflammatory effects; and patient-reported outcome (PRO) tools designed to capture quality-of-life metrics beyond conventional CTCAE criteria. These advancements are critical for optimizing therapeutic safety in the era of multimodal LS-SCLC treatment paradigms. The necessity of PCI remains a topic of debate, emphasizing the importance of regular brain monitoring. Cranial MRI enables timely disease assessment and helps mitigate the potential impact of PCI on patients’ quality of life. The application of combination therapy strategies involving ICIs in LS-SCLC remains in the exploratory phase. The optimal timing for initiating immunotherapy and its potential clinical benefits require further validation. Future research should prioritize optimizing combination therapy regimens, investigating the integration of ICIs with chemoradiotherapy or other novel treatments, and developing more specific and sensitive biomarkers to facilitate personalized treatment approaches. Additionally, minimizing irAEs, particularly through the prevention and management of toxic reactions such as radiation pneumonitis, will be a key focus of future research.
Future Perspectives
The findings of this review provide critical insights for updating clinical guidelines in LS-SCLC, with particular emphasis on immunotherapy integration. First, supported by the survival benefits demonstrated in the ADRIATIC trial (median OS: 55.9 vs 33.4 months) and FDA approval, durvalumab consolidation therapy post-chemoradiotherapy should be standardized in National Comprehensive Cancer Network /ESMO guidelines, while proactive surveillance may replace PCI in selected cases. Second, conditional recommendations are warranted for immunotherapy-CCRT and neoadjuvant immunochemotherapy, pending Phase III validation—particularly in resectable tumors or biomarker-selected populations (e.g., high TMB, SCLC-I subtype). Third, guidelines should prioritize biomarker-driven strategies (TMB, PD-L1, tumor-infiltrating lymphocytes) for patient stratification and toxicity management protocols tailored to LS-SCLC-specific irAEs (e.g., enhanced pneumonitis surveillance). These updates aim to harmonize therapeutic efficacy with precision oncology principles in LS-SCLC management. In summary, immunotherapy represents a promising therapeutic frontier for LS-SCLC patients. Based on current evidence and limitations, future research priorities should focus on four key domains: (1) Precision timing optimization: Phase III trials are needed to determine whether initiating immunotherapy during CCRT yields superior outcomes to consolidation approaches, with mechanistic studies elucidating post-radiation immune microenvironment dynamics (e.g., T-cell clonal expansion peaks) to guide personalized dosing schedules. (2) Stepwise development of novel combinations: This includes evaluating sequential DLL3/CD3 bispecific antibodies (e.g., tarlatamab) with PD-L1 inhibitors while addressing T-cell exhaustion; assessing PARP inhibitors (e.g., olaparib) for Stimulator of Interferon Genes Pathway (STING) pathway-mediated immunogenicity enhancement; and optimizing multimodal regimens (e.g., SHR-1701 with stereotactic radiotherapy) through refined target delineation and dose fractionation. (3) Noninvasive biomarker system innovation: Priorities encompass dynamic response prediction models leveraging ctDNA methylation signatures (e.g., SOX2 methylation levels), validation of exosomal PD-L1 mRNA as a response correlate, and LS-SCLC-specific liquid biopsy panels integrating genomic (TMB), epigenomic (cfDNA fragmentation patterns), and immunologic (circulating TCR diversity) multi-omics data. (4) Large-scale validation infrastructure: Establishing a global LS-SCLC consortium to standardize biomarker assays (e.g., TMB whole-slide imaging calibration) and irAE definitions, alongside leveraging the FDA Sentinel Initiative to build immunotherapy registries analyzing long-term survivors (>3 years) for molecular signatures and cumulative toxicity risks.
In conclusion, immunotherapy represents a highly promising treatment option for patients with LS-SCLC. We strongly recommend the initiation of multicenter, large-scale clinical trials to validate the efficacy and safety of immunotherapeutic strategies in this patient population. Such studies are anticipated to play a pivotal role in optimizing treatment protocols and ultimately improving the prognosis of LS-SCLC patients.
Conclusion
Immunotherapy has transformed the therapeutic landscape of LS-SCLC, particularly with durvalumab consolidation post-chemoradiotherapy demonstrating unprecedented survival benefits in the ADRIATIC trial. While biomarkers such as TMB and PD-L1 show potential, their clinical utility remains limited by standardization challenges and dynamic tumor microenvironment interactions. Future efforts must prioritize optimizing combination strategies, validating personalized biomarkers, and addressing immunotherapy-related toxicities through multicenter trials. These advancements will refine precision approaches and improve long-term outcomes for LS-SCLC patients.
Supplemental Material
Supplemental Material - Immunotherapy for Limited-Stage Small Cell Lung Cancer: Innovative Treatments and Future Perspectives
Supplemental Material for Immunotherapy for Limited-Stage Small Cell Lung Cancer: Innovative Treatments and Future Perspectives by Xiaoni Jin, Weixing Zhao, Guoyuan Li, and Jun Jiang in Cancer Control
ORCID iDs
Xiaoni Jin https://orcid.org/0009-0004-9117-0829
Weixing Zhao https://orcid.org/0009-0001-1291-4788
Footnotes
Statements and Declarations
Author Contributions
Xiaoni Jin,and Weixing Zhao organized the data and wrote the manuscript. Guoyuan Li,and Jun Jiang proposed the research concept, checked the reliability of the data, revised the manuscript, and were responsible for the quality of the article. All authors contributed to manuscript revision, and read and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Science and Technology Agency of Qinghai Province (2022-ZJ-719).
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data availability is not applicable to this article as no new data were created or analyzed in this study.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.