
Abstract
Introduction
Cancer patients often face challenges in managing their disease, particularly with regard to contraindications related to medications, foods, and physical activity, which can negatively affect treatment outcomes. This study aimed to evaluate cancer patients’ awareness of these contraindications and to explore the influence of sociodemographic factors, support systems, comorbidities, and medication use on their knowledge.
Methods
A cross-sectional prospective study was conducted with 125 cancer patients in Saudi Arabia between December 2022 and February 2023. Participants were selected using purposive sampling, and data were collected through a validated questionnaire. Multinomial regression analysis was employed to identify the predictors of awareness of contraindicated medications, foods, and other environmental factors.
Results
Nationality, co-morbidities, and cancer duration were significant predictors of awareness regarding contraindicated drugs. Saudi patients were more likely to be aware of contraindicated medications (P = 0.010), and those without chronic diseases were 15 times more likely to know about drug contraindications (OR = 15.076, 95% CI: 3.442-66.042). Cancer diagnosis (P = 0.033) and cancer duration (P = 0.022) were also significant for food contraindications. Over 58% were unaware of the need to regulate body temperature during treatment. Location influenced exercise awareness (P = 0.064) and complementary and alternative medicine (CAM) awareness, with rural participants showing higher CAM knowledge (P = 0.001).
Conclusion
This study emphasizes the need to improve cancer patients’ awareness of contraindications, particularly regarding medications and foods. Key factors influencing awareness include nationality, co-morbidities, and cancer duration. While family support is beneficial, it doesn’t directly enhance knowledge, highlighting the importance of targeted educational interventions to improve patient outcomes and safety.
Plain Language Summary
Awareness of Health Risks: How Cancer Patients in Saudi Arabia Understand Medication, Food, and Activity Contraindications: This study highlights the importance of improving cancer patients’ awareness of contraindications related to medications, foods, and other environmental factors that can affect treatment outcomes. Conducted with 125 cancer patients in Saudi Arabia, the study found that nationality, co-morbidities, and cancer duration significantly influenced awareness of drug and food contraindications. Saudi patients and those without chronic diseases were more likely to be aware of harmful drug interactions, while cancer type and duration were key to understanding food-related risks. The study also revealed that awareness of body temperature regulation during treatment and complementary and alternative medicine (CAM) use was limited, with rural patients showing higher CAM knowledge. These findings emphasize the need for targeted educational interventions to enhance patient safety and treatment efficacy, as family support, though beneficial, did not directly improve knowledge of contraindications.
Introduction
Advances in cancer treatment have significantly improved survival rates and life expectancy for patients. However, this extended lifespan often necessitates the management of multiple chronic conditions, complicating treatment regimens and leading to polypharmacy. Polypharmacy, defined as the use of multiple medications, is increasingly common and presents substantial challenges in managing both cancer and its associated comorbidities.1,2 A study revealed that 35% of elderly patients diagnosed with breast, lung, colon, rectal, prostate, or ovarian cancer were taking more than 5 medications. 3 Additionally, the World Health Organization (WHO) reports that over 50% of patients worldwide do not adhere to prescribed medication regimens, and more than 50% of medications are improperly prescribed, sold, or distributed. 4 This highlights the urgent need for effective medication management and monitoring strategies.
Cancer treatments such as chemotherapy, radiation, and surgery can lead to a range of side effects affecting multiple body systems. 5 These treatments carry individual or combined risks that can be exacerbated by pre-existing comorbidities and concurrent medication use. 6 Interactions between anticancer therapies and other medications may increase the risk of adverse effects and complicate treatment outcomes. 7 Understanding the extent of polypharmacy is crucial for optimizing patient care and minimizing potential risks.
Numerous studies have shown that cancer can significantly alter food preferences, with these changes influenced by the type of treatment or disease stage.8,9 For example, patients with head and neck cancers often experience shifts in their food-related expectations, which can lead to changes in the “meaning of food” and result in various physical, emotional, and social losses. 10 After curative gastrectomy, patients commonly face increased dysphagia, eating restrictions, anxiety, changes in taste, and body image issues, although these concerns generally diminish over 12 months. 11 Additionally, radiotherapy is well-documented to adversely affect taste perception both during and after treatment.12,13 Chemotherapy (CT) regimens also influence taste changes and food preferences, with significant correlations observed between ageusia and dry mouth, bitter taste and appetite loss, sour taste and nausea, and anorexia and dry mouth. 14 However, systematic reviews indicate that the effects of CT on food preferences have not been consistently established.15,16 Ultimately, the extent to which these disturbances influence dietary behavior during and after treatment remains largely unknown. Consequently, there is a notable lack of information regarding the practical management of food intake, particularly concerning meal and food preferences within a cultural context among cancer patients undergoing treatment.
The use of complementary and alternative medicine (CAM) among cancer patients adds another layer of complexity. Research indicates that a significant portion of cancer patients utilize CAM therapies alongside conventional treatments. For instance, in Europe, 36% of cancer patients reported using CAM, including dietary supplements and herbal remedies. 17 CAM can interact with conventional cancer therapies, potentially affecting treatment efficacy and safety. A cross-sectional study by Zeller et al found that 65% of cancer patients using CAM supplements were at risk of “likely” or “possible” interactions with their cancer treatments. 18 While CAM is widely utilized among cancer patients, many struggle to discuss their CAM practices with health care providers.19,20 This gap underscores the need to enhance patients’ understanding of CAM to facilitate better communication with health care professionals.
Physical activity (PA) is recognized for improving the quality of life, physical performance, and mental well-being of cancer patients. Evidence suggests that PA is associated with reduced mortality risk and better treatment outcomes.21,22 However, PA may be contraindicated in certain situations, such as severe anemia, fatigue, or acute infections, which are common among cancer patients. 23 Consequently, medical professionals often exercise caution when recommending PA during treatment. Engaging in leisure-time PA at the recommended level of 7.5-15 MET hours per week is associated with a 6%-29% reduction in risk for various cancers, including colon, breast, endometrial, kidney, myeloma, liver, and non-Hodgkin lymphoma (in women). Exercising beyond this recommended level may further decrease the risk for some cancers, but not all, indicating fundamental differences in the biological mechanisms related to different cancer types. 24 Therefore, it is essential to develop patient- and cancer-specific protocols to enhance the well-being of cancer patients.
Comprehensive studies that address interactions between drugs and concurrent diseases, dietary factors, CAM, and physical activity are relatively scarce. This gap emphasizes the need for research that encompasses a broader spectrum of potential interactions affecting cancer patients. Recent cross-sectional studies have begun to address these issues by examining the frequency and severity of drug interactions involving anticancer medications. For example, Khorami et al. 2 highlighted significant drug interactions between anticancer agents and medications for chronic conditions, emphasizing the importance of careful medication management. Similarly, Patel et al. 25 found that interactions between CAM and conventional treatments can complicate cancer management and affect patient outcomes. Other research, such as that by Fernandez et al., 26 has explored the impact of dietary factors and physical activity 27 on cancer treatment efficacy, noting the need for integrated management strategies.
Given these considerations, this study aims to assess the extent of contraindicated drug use, dietary preferences, use of complementary and alternative medicine (CAM), and other pertinent factors among cancer patients. By examining these areas, this research intends to contribute valuable insights to improve cancer care management within this specific demographic and to address existing gaps in the current literature.
Methods
Study Design
An observational prospective cross-sectional study was conducted in Saudi Arabia between December 2022 and February 2023. To collect data, Google Forms surveys were utilized, allowing for efficient gathering of participant responses. The study employed purposive sampling to select participants, ensuring that individuals who fulfilled the relevant inclusion requirements were included. Interviews were conducted using a structured questionnaire, administered at any of the study sites, in the Riyadh region of Saudi Arabia. The reporting of this study adheres to the STROBE guidelines, ensuring that the methodology and findings are presented in a transparent and standardized manner. 28 This adherence reinforces the credibility of the research and its relevance to ongoing discussions in the field. The sample size was determined using the latest report on cancer patients in the Riyadh region, which identifies a total of 4493 patients. 29 Based on our recent findings, 30 we estimated that 11% of these patients receive contraindicated medications. To ensure accuracy, we maintained a margin of error of 5% and a confidence level of 90%, utilizing the online sample size calculator Raosoft (https://www.raosoft.com/samplesize.html). The calculated sample size required for a representative analysis of the eligible population was 104. For this study, a total of 125 samples were included in the analysis, providing a robust representation of the available population at the study location.
Participants
All cancer patients willing to participate in the study and receive treatment at any of the study sites in the Riyadh region of Saudi Arabia were considered eligible for inclusion. To ensure a focused and relevant participant group, specific inclusion and exclusion criteria were established.
Inclusion Criteria:
Diagnosis of Cancer: Participants must have a confirmed diagnosis of cancer.
Current Treatment: Individuals must be actively undergoing treatment for cancer, regardless of the type of therapy (eg, chemotherapy, radiation, surgery).
Willingness to Participate: Participants must be willing to provide informed consent and engage with the study.
Exclusion Criteria:
Inability to Provide Consent: Individuals unable to understand the study’s purpose or unable to provide informed consent due to cognitive impairments or language barriers were excluded.
Non-cancer Related Conditions: Patients with non-cancerous conditions that required treatment but did not have a cancer diagnosis were not included.
Recent Participation in Other Studies: Participants who had recently been involved in other clinical trials or studies that may influence their responses were excluded to minimize bias.
Ethical Consideration
The Institutional Review Board of AlMaarefa University granted ethical approval for this study (IRB09-04122022-101). Before participation, all individuals were thoroughly informed about the study’s aims, methodology, potential outcomes, and the voluntary nature of their involvement. Participants were assured of the confidentiality of their responses and were made aware that they could choose to decline or withdraw from the study at any point without any negative repercussions. Only those who provided their informed consent were included in the study, ensuring that all participants were comfortable and willing to contribute to the research.
Study Instrument
The study instrument, a structured questionnaire, was meticulously developed with the collaboration of qualified researchers, academicians, and practitioners in the field. The research team drew upon relevant published literature to ensure the questionnaire’s comprehensiveness and relevance. To enhance the validity of the instrument, experts in oncology and health research were consulted to review the construct, content, and criteria of the questionnaire. The questionnaire demonstrated good internal consistency, with a Cronbach’s alpha of 0.706.
The questionnaire was organized into 4 distinct sections:
Sociodemographic Characteristics of the Participants
This section comprised ten items designed to capture essential demographic information. Participants were asked about their age, gender, nationality, educational level, location, income, marital status, employment status, and the nature of family and spouse support. This information is crucial for understanding the diverse backgrounds of the participants and how these factors may influence their health behaviors and perceptions.
Co-morbidities Status of the Participants
This section was further divided into 2 sub-sections:
Sub-section 1: Focused on inquiring whether participants were suffering from any chronic illnesses, allowing for the identification of additional health challenges that may affect cancer management.
Sub-section 2: Gathered detailed information about the medications participants were taking to manage their co-morbidities. This data is vital for understanding the potential impact of polypharmacy on cancer treatment and outcomes.
Details About Cancer
This section included 6 items to collect pertinent information regarding the participants’ cancer experiences. Questions in this section explored the type of cancer diagnosed, the duration of the cancer, the length of time participants had been undergoing chemotherapy, and whether they had received counseling related to their condition. This information helps to contextualize the participants' cancer journeys and the support systems in place.
Status of Food preferences, CAM use, and Physical activity
This final section comprised 5 questions aimed at assessing the participants’ awareness of contraindicated drugs related to their cancer treatment. The questions further explored several key areas including:
Contraindicated foods: Participants were asked to identify specific foods that may adversely affect their treatment or health outcomes.
Complementary and Alternative Medicines (CAM): The questionnaire sought to gauge the participants’ understanding of the potential interactions between CAM therapies and conventional cancer treatments.
Recommended Physical Activities: Questions in this section addressed the participants’ awareness of suitable physical activities (yoga, nerve gliding exercise, sensorimotor-based exercise) that are safe to engage in during cancer treatment.
Sources of Information: Participants were also asked to identify where they obtained their information about contraindications, including health care providers, literature, and personal research.
Impact of Hyperthermia: A question to assess participants’ awareness of whether elevated body temperature is contraindicated during cancer chemotherapy.
This section aims to evaluate participants’ awareness and understanding of how various factors, such as dietary choices, CAM use, and physical activity, can interact with their cancer treatments. By assessing this knowledge, the study seeks to identify gaps in understanding that could impact patient care and health outcomes.
Overall, the questionnaire was designed to provide comprehensive insights into the experiences and knowledge of cancer patients in Saudi Arabia, facilitating the study’s objectives of understanding their health behaviors and decision-making processes.
Statistical Analysis
Data from the study were entered and analyzed using SPSS, employing both descriptive and inferential analysis techniques. Participants’ awareness of contraindications to drugs, foods, CAM, exercise, and body temperature was compared against their sociodemographic traits as well as their clinical and treatment characteristics using the Pearson Chi-square test, with statistical significance set at a P-value below 0.05. Additionally, multinomial regression analysis was performed to identify factors influencing cancer patients’ awareness, with results reported as odds ratios, confidence intervals (upper and lower limits), and P-values.
Results
Sociodemographic Characteristics of the Participants
Demographic Characteristics of the Participants.

Clinical and Treatment Characteristics
Clinical and Treatment Characteristics of the Participants.
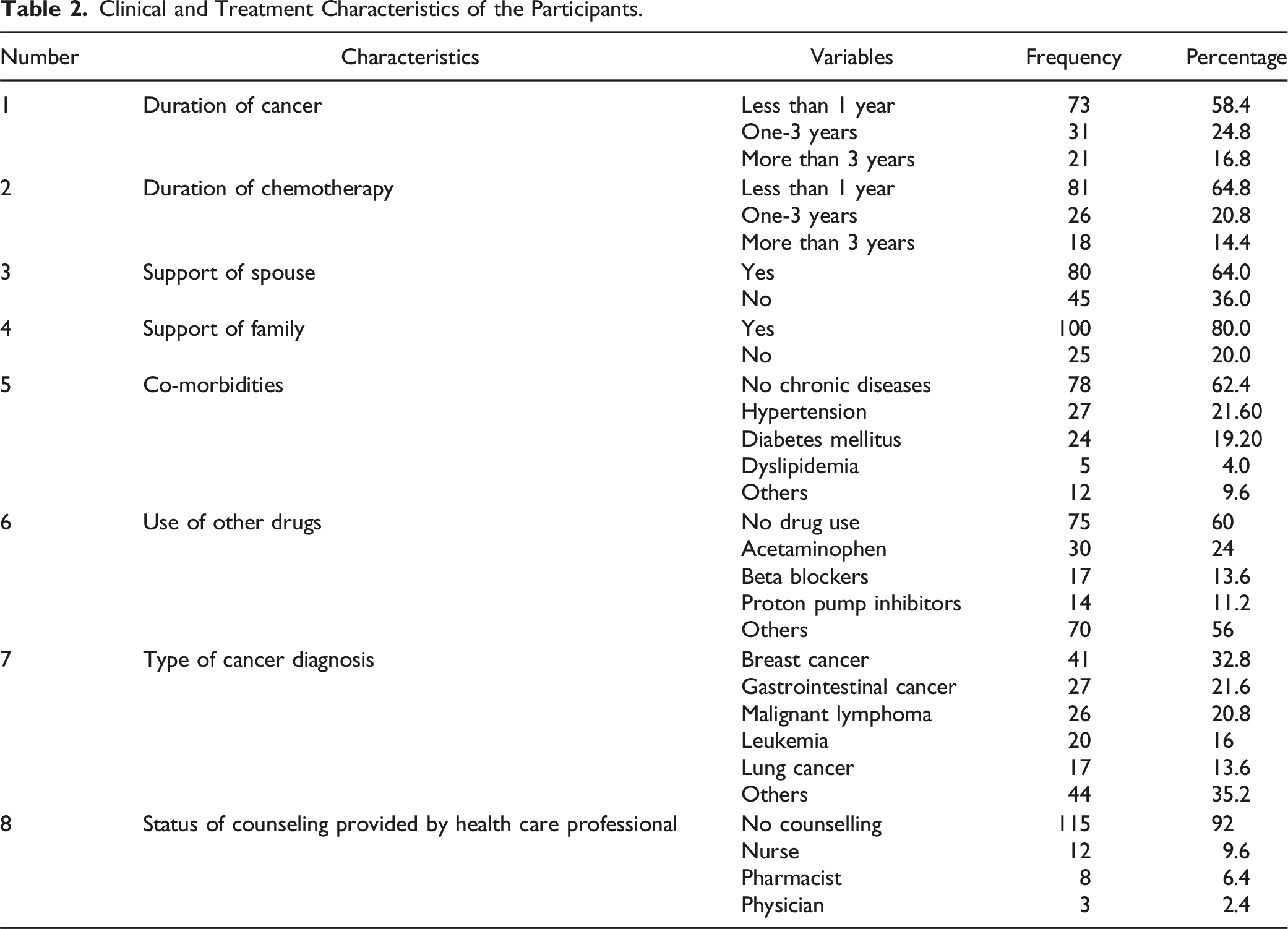
Support from spouses and family was reported by 64.0% and 80.0% of participants, respectively. Concerning co-morbidities, 62.4% of participants reported no chronic diseases, while hypertension and diabetes mellitus were the most common co-morbidities, affecting 21.6% and 19.2% of participants, respectively. Regarding the use of other medications, 60% of participants did not take any additional drugs, while 24% used acetaminophen, 13.6% used β-blockers, and 11.2% used proton pump inhibitors.
Breast cancer was the most common diagnosis, affecting 32.8% of participants, followed by gastrointestinal cancer (21.6%), malignant lymphoma (20.8%), leukemia (16.0%), and lung cancer (13.6%). Additionally, a significant majority (92.0%) of participants reported not receiving counseling from health care professionals, with a small proportion receiving counseling from a nurse (9.6%), a pharmacist (6.4%), or a physician (2.4%). These findings provide valuable insights into the clinical characteristics, treatment history, and support systems of cancer patients in the study population.
Use of CAM, Avoidance of Food and Preferred Information Source
Use of CAM, Avoidance of Food, and Preferred Information Source.

Regarding food avoidance, the majority (64.0%) of participants did not avoid any specific foods. Among those who did avoid foods, sugar was the most avoided (29.6%), followed by fatty foods (16.8%), spicy foods (6.4%), and fast food (2.4%). A small group (8.0%) reported avoiding other types of food.
When it comes to the preferred source of health information, most participants (90.4%) preferred to receive information from their doctor. The internet was the second most common source (11.2%), followed by general searches (4.8%), Google (3.2%), and other sources (6.4%). These findings highlight the diverse practices and preferences regarding CAM use, dietary restrictions, and the sources from which patients seek health information.
Awareness of Contraindications
Figure 1 illustrates participants’ awareness regarding various aspects of their cancer treatment, including contraindications related to body temperature, the usefulness of exercise, food avoidance, the use of complementary and alternative medicine (CAM), vitamins, and drug use. Awareness of the use of contraindicated drugs, food, exercise, body temperature, and use of CAM.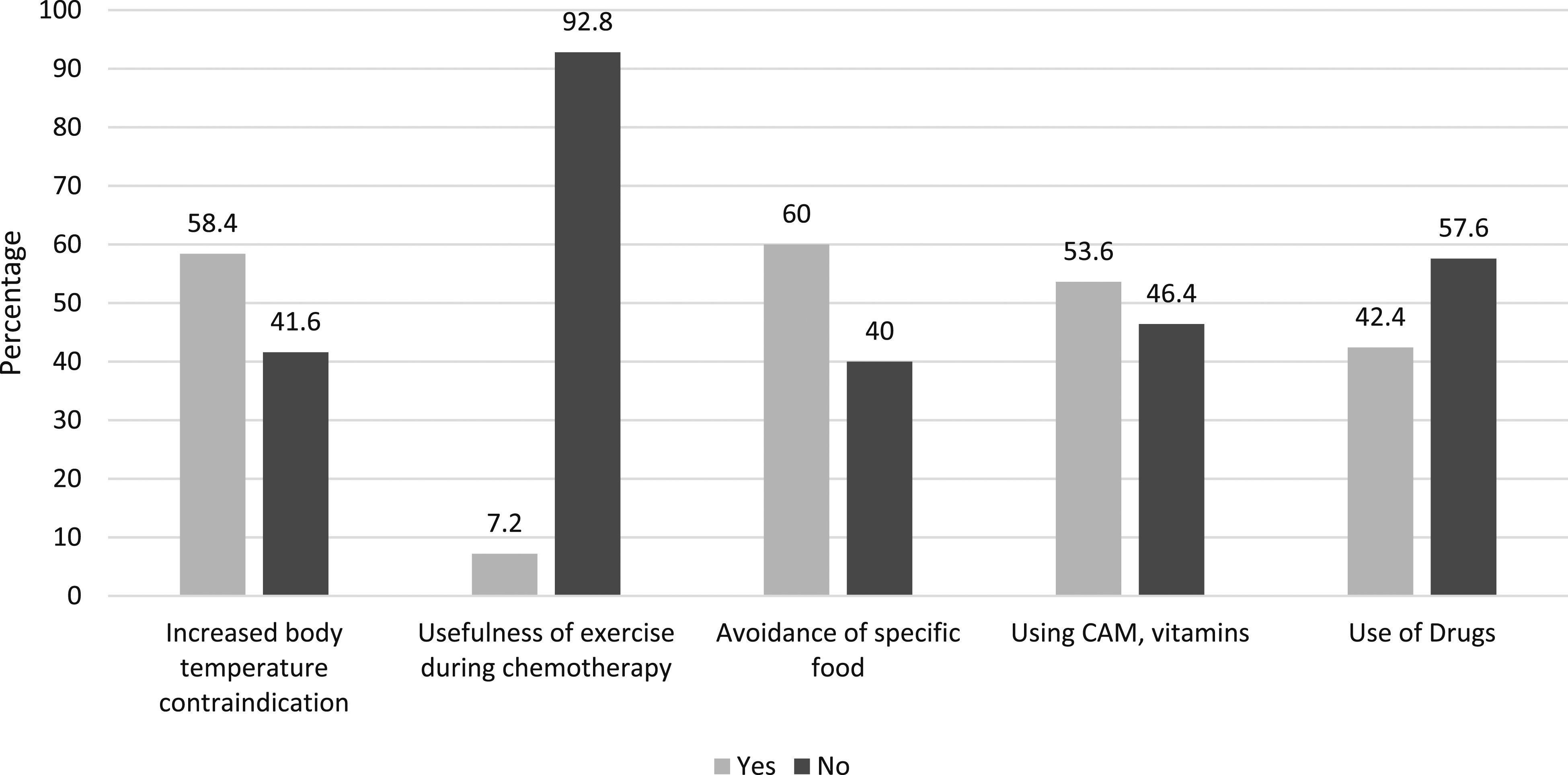
The data shows that 58.4% of participants were aware of the contraindication related to increased body temperature, while 41.6% were not. Regarding the usefulness of exercise during chemotherapy, only 7.2% of participants believed exercise to be useful, while a substantial 92.8% did not. In terms of food avoidance, 60.0% of participants were aware of the need to avoid specific foods, while 40.0% were not. Regarding CAM and vitamin use, 53.6% of participants were aware of their potential benefits, while 46.4% were not. Finally, about drug use, 42.4% of participants were aware of the importance of avoiding certain drugs, while 57.6% were not.
These findings highlight varying levels of awareness among patients about key aspects of their cancer treatment and self-care, particularly concerning contraindications, exercise, and the use of CAM and other supplements.
Comparison of the Awareness Status of the Participants with Their Sociodemographic Characteristics
Comparison of Awareness of Contraindicated Drugs and Food With Patients’ Characteristics.
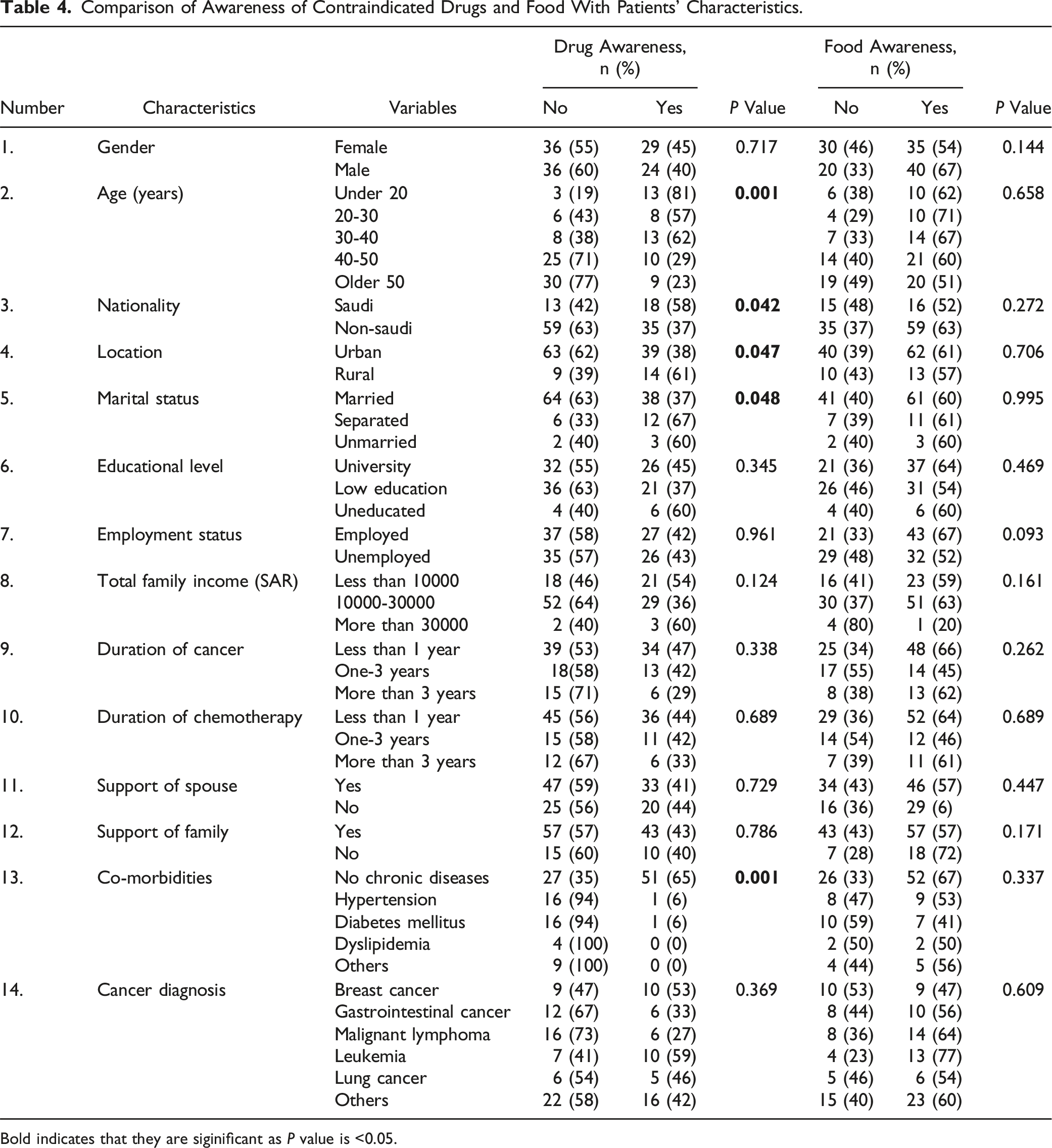
Bold indicates that they are siginificant as P value is <0.05.
Participants’ awareness of contraindicated foods was compared across various demographic and clinical characteristics, as shown in Table 4. The analysis revealed that factors such as gender, age, nationality, and marital status did not have statistically significant associations with awareness levels. For instance, although more males (67%) were aware of contraindicated foods compared to females (54%), this difference was not statistically significant (P = 0.144). Similarly, non-Saudi participants had slightly higher awareness (63%) than Saudi participants (52%) (P = 0.272), but this difference was also not significant.
Further analysis indicated no significant differences in awareness based on location, educational level, employment status, or support from family or spouse (P > 0.05). However, participants without chronic diseases demonstrated higher awareness (67%) compared to those with hypertension, diabetes, or other conditions (P = 0.337). Cancer diagnosis also did not significantly impact awareness, though those diagnosed with leukemia (77%) or malignant lymphoma (64%) showed higher awareness of contraindicated foods. These findings suggest that while there are some trends, most demographic and clinical factors did not show statistically significant differences in awareness of contraindicated foods.
Comparison of Body Temperature and Exercise Awareness With Patients’ Characteristics.

Bold indicates that they are siginificant as P value is <0.05.
Comparison of Awareness of the Use of CAM With Patients’ Characteristics.
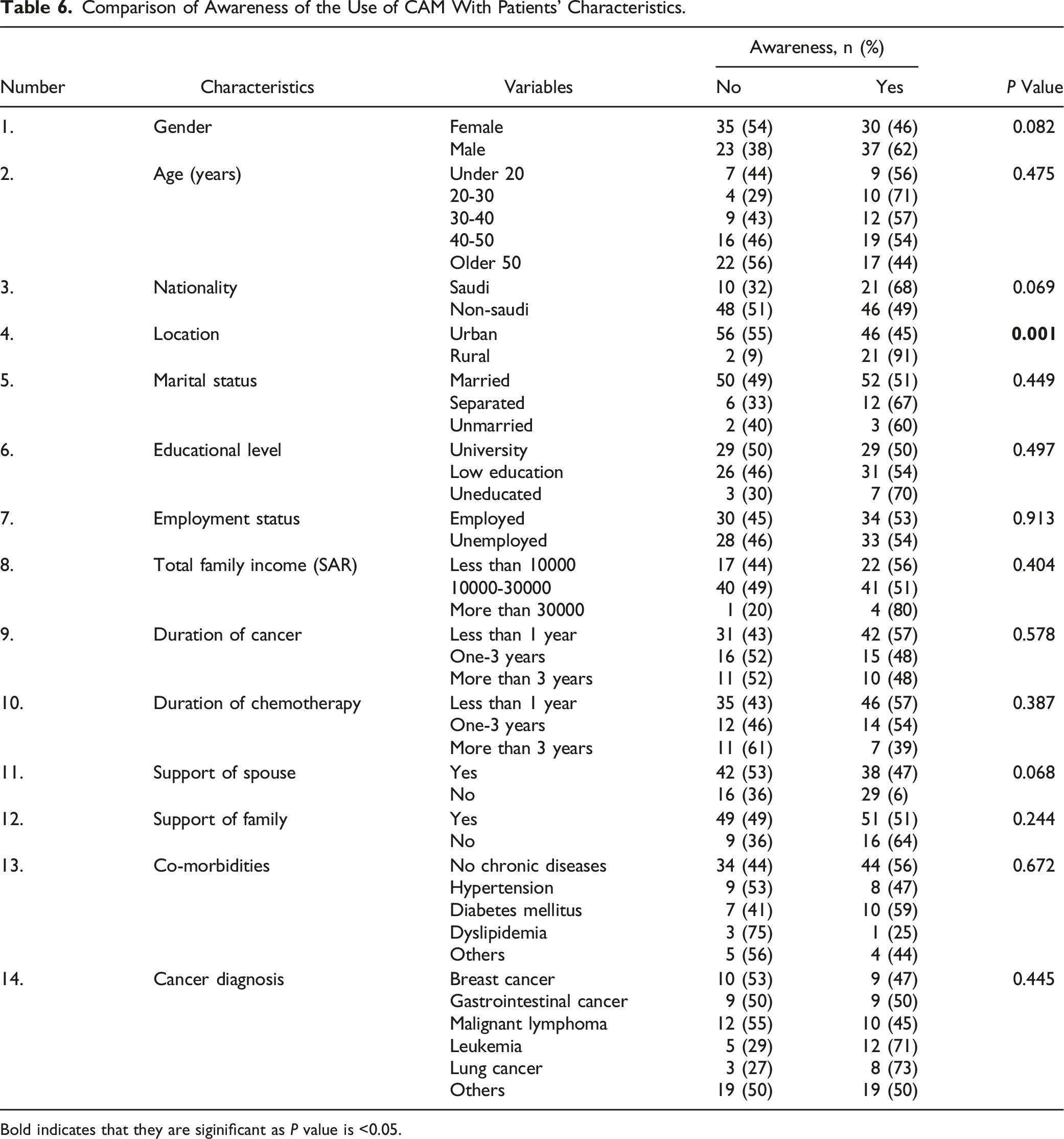
Bold indicates that they are siginificant as P value is <0.05.
Multinomial Regression Analysis to Determine Factors Influencing Outcome Variables
Factors Influencing the Awareness of Contraindicated Drugs and Food.

aDependent Variable: Awareness of contraindicated drugs.
bDependent Variable: Awareness of contraindicated food.
Bold indicates that they are siginificant as P value is <0.05.
For awareness of contraindicated drugs, nationality was a significant predictor (P = 0.010), with non-Saudi participants showing a significantly higher likelihood of awareness (Exp(B) = 8.913, 95% CI: 1.697-46.810). Additionally, co-morbidities had a strong association with awareness (P = 0.000), with participants without chronic diseases being 15 times more likely to be aware of contraindicated drugs (Exp(B) = 15.076, 95% CI: 3.442-66.042). The duration of cancer was also significant (P = 0.022), with those having been diagnosed for a longer period (Exp(B) = 9.398, 95% CI: 1.381-63.962) showing increased awareness.
For awareness of contraindicated foods, gender was a notable factor, with males showing a higher likelihood of awareness, although the result was not statistically significant (P = 0.607). Cancer diagnosis showed a significant relationship (P = 0.033), suggesting that certain cancer types may influence food awareness. Duration of cancer was also a significant factor for food awareness (P = 0.022), indicating that patients diagnosed for longer periods were more likely to be aware of contraindicated foods.
Other variables, such as age, location, education level, employment status, family support, and chemotherapy duration, did not significantly influence awareness of either contraindicated drugs or foods (P > 0.05). These findings underscore that specific demographic and clinical factors, such as nationality, co-morbidities, and the duration of cancer, play a significant role in patients’ awareness of contraindicated drugs and foods.
Factors Influencing the Awareness of CAM, Exercise, and Body Temperature.

aDependent Variable: Body Temperature Awareness.
bDependent Variable: Exercise Awareness.
cDependent Variable:CAM Awareness.
Bold indicates that they are siginificant as P value is <0.05.
For body temperature awareness, none of the demographic or clinical factors were statistically significant (P > 0.05), indicating that variables such as gender, age, nationality, and marital status did not significantly influence awareness of body temperature management. Similarly, exercise awareness showed no significant predictors, although a trend towards significance was noted for location (P = 0.064), with urban dwellers potentially having higher awareness. For CAM awareness, location was a significant factor (P = 0.001), with rural participants demonstrating significantly higher awareness of CAM (Exp(B) = 0.047, 95% CI: 0.008-0.286), suggesting that geographical location might play a role in access to or knowledge about CAM practices.
Other factors, including educational level, employment status, family support, co-morbidities, cancer diagnosis, and the duration of cancer or chemotherapy, did not show significant associations with awareness of body temperature, exercise, or CAM (P > 0.05). The results suggest that while some individual factors like location may influence awareness of CAM, overall, demographic and clinical characteristics have limited impact on awareness of body temperature and exercise management during chemotherapy.
Discussion
This study provides critical insights into the sociodemographic characteristics, co-morbidities, medication use, cancer types, professional counseling, complementary and alternative medicine (CAM) use, contraindications, and the awareness of cancer patients regarding the management of their disease. Through an in-depth analysis of these factors, we aim to highlight key drivers of cancer patients’ knowledge about their condition, particularly concerning contraindications related to both medications and foods. The findings are instrumental in understanding the gaps in patient education and suggest strategies for improving cancer care through targeted educational interventions.
The study’s demographic profile revealed a nearly equal distribution of male and female participants, with more than half of the respondents being over 40 years old. The majority (75.2%) were non-Saudis, reflecting the demographic diversity seen in urban cancer centers due to immigration. This pattern mirrors trends observed in other regions where aging, urbanization, and diverse populations correlate with higher cancer prevalence.31-33 Participants with higher education levels and moderate incomes were more frequently represented, aligning with previous research that indicates that educated patients are more likely to seek medical advice and actively participate in managing their health.34,35
Interestingly, sociodemographic factors such as education, income, and employment did not significantly affect the awareness of cancer contraindications in this study. This suggests that other factors, such as exposure to health care services, the duration of illness, and the type of cancer, may play a more prominent role in determining a patient’s awareness level. The role of family support was also a significant consideration in this study. More than 80% of participants reported receiving family support, with 64% indicating spousal support. This aligns with a growing body of literature highlighting the crucial role of family in enhancing cancer patients’ treatment adherence and overall well-being. 36 However, despite the high level of support, there was no statistically significant correlation between family support and awareness of contraindications. This finding suggests that while emotional and practical support is crucial, it does not necessarily translate into greater awareness of the complexities of cancer treatment. This gap highlights the need for more targeted educational interventions aimed at both patients and their families, particularly around contraindications and the management of cancer treatment.
The presence of co-morbidities such as diabetes (19.2%) and hypertension (21.6%) among participants underscores the challenges of managing multiple health conditions simultaneously. Cancer treatments often interact with medications used for chronic conditions, requiring careful management to avoid adverse drug interactions. 37 Additionally, mental health issues, such as depression, are common among cancer patients, which complicates their ability to manage medications and adhere to treatment protocols. 38 Addressing both the physical and psychological aspects of cancer care through integrated services can improve patients’ ability to manage contraindications and enhance their overall quality of life.
Medication use among participants revealed that acetaminophen (24%) was the most frequently used drug, a reflection of the need for cancer patients to manage pain and treatment-related symptoms. 39 Other commonly used medications include β-blockers and proton pump inhibitors, which are employed to manage co-morbid conditions or alleviate side effects of chemotherapy. 37 Interestingly, only 20.8% of participants reported using multiple medications, suggesting a cautious approach to polypharmacy. This finding highlights the importance of detailed records and open communication between patients and health care providers to prevent harmful drug interactions. For example, drugs like erlotinib, used for non-small cell lung cancer, can alter the metabolism of acetaminophen, indicating the necessity for careful monitoring and patient education. 40
Despite the high demand for cancer education, 90% of our participants did not receive any form of professional counseling. Limited professional counseling, especially from physicians, suggests that there may be barriers, such as time constraints, high patient loads, or lack of specific training among health care providers, which limit effective communication on contraindications and disease management. Studies show that health care providers who deliver comprehensive counseling improve cancer patients’ adherence to treatment and reduce their use of contraindicated substances.41,42 Furthermore, our findings reveal that approximately half of the participants did not use any complementary or alternative medicine (CAM), while a notable fraction consumed vitamins, especially vitamins B12 and D. The literature indicates mixed opinions on CAM use in cancer treatment, as some studies suggest potential benefits, while others highlight risks associated with drug-CAM interactions.33,43
The multinomial regression analysis conducted in this study reveals the significant factors influencing awareness of contraindicated drugs and foods among cancer patients. For contraindicated drugs, nationality, co-morbidities, and duration of cancer were the most significant predictors. Nationality was a strong determinant, with Saudi patients being significantly more likely to be aware of contraindicated drugs (P = 0.010). This could reflect differences in health care access, patient education, or cultural factors that influence how people from different nationalities approach their cancer treatment. 34 The presence of co-morbidities had a powerful association with awareness of contraindicated drugs. Participants without chronic diseases were found to be 15 times more likely to be aware of contraindicated medications (Exp(B) = 15.076, 95% CI: 3.442-66.042). This finding suggests that patients managing multiple health conditions may be overwhelmed with their treatment regimens, reducing their focus on the specific contraindications of drugs. 37 Duration of cancer also played a critical role in awareness of drug contraindications. Patients diagnosed for longer periods were significantly more aware of drugs to avoid, indicating that prolonged exposure to the health care system enhances knowledge of potential risks and interactions. 40
For contraindicated foods, gender, cancer diagnosis, and duration of cancer emerged as important factors. Gender was noted as a factor, with males showing a slightly higher likelihood of being aware of food contraindications, although the result was not statistically significant (P = 0.607). Cancer diagnosis showed a significant relationship (P = 0.033), suggesting that the type of cancer may influence food awareness. For example, patients with gastrointestinal cancers or those undergoing chemotherapy for digestive system-related cancers may have more knowledge about dietary restrictions due to the direct impact of their treatments on digestion and nutrition. 44 Duration of cancer was again a significant factor, with patients who had been diagnosed for longer periods showing better awareness of food contraindications (P = 0.022). This finding aligns with the notion that the more exposure patients have to the health care system and treatment regimens, the more likely they are to accumulate essential knowledge. 45
Interestingly, age, location, education level, employment status, family support, and chemotherapy duration did not significantly influence awareness of contraindicated drugs or foods (P > 0.05). This suggests that demographic and psychosocial variables might influence other aspects of cancer care but do not directly correlate with awareness of contraindications. The lack of significance for family support is noteworthy, as it challenges the assumption that a supportive family network automatically translates into improved patient knowledge, particularly regarding treatment and dietary restrictions.
The study also identified some concerning gaps in cancer patients’ understanding of contraindications. Dietary misconceptions were prevalent, with 60% of participants believing that avoiding sugar would enhance their treatment effectiveness. This reflects a widespread but incorrect belief among cancer patients about the role of diet in cancer management. While patients need to maintain a balanced diet, there is no scientific evidence to support the idea that sugar directly influences cancer progression or treatment outcomes. 33 Another significant knowledge gap was observed regarding the importance of controlling body temperature during chemotherapy. Over 58% of patients were unaware of the need to regulate body temperature during treatment, which can lead to complications if not managed properly. These gaps in understanding underscore the need for more comprehensive educational efforts targeting the nuances of chemotherapy side effects and their management. 46
Limitations and Recommendations
One limitation of this study is its cross-sectional design, which restricts the ability to draw causal inferences about the factors influencing awareness of contraindications. Additionally, the reliance on self-reported data may introduce response bias, particularly regarding sensitive topics such as dietary habits and medication use. Patients may underreport or overreport their behaviors due to social desirability bias or recall errors. Future research should focus on longitudinal studies to explore causal relationships and the long-term impact of educational interventions on patient knowledge and health outcomes. Additionally, exploring family-centered educational programs could provide a more holistic approach to cancer care, ensuring that both patients and their support systems are informed about the complexities of treatment management.
Practice Implications
This study emphasizes the importance of improving cancer patient education, particularly regarding contraindications related to drugs and foods. Health care providers should take a proactive approach to educate patients about these critical aspects of treatment management. Education efforts should be tailored to individual patient needs, with special attention given to those with specific risk factors such as nationality, co-morbidities, and the duration of cancer treatment. Multidisciplinary teams, including oncologists, pharmacists, dietitians, and nurses, should collaborate to offer comprehensive education on both drug interactions and dietary restrictions. These interventions should be introduced early in the treatment process, especially for newly diagnosed patients, and reinforced throughout their care journey. Furthermore, educating family members about contraindications and proper care practices should be a key component of cancer care, as their support plays a critical role in patients’ overall treatment adherence and well-being.
Conclusion
This study highlights the critical need to enhance cancer patients’ awareness of contraindications, particularly regarding medications and foods, which can significantly impact treatment efficacy and safety. The factors influencing awareness include nationality, co-morbidities, and duration of cancer, with gender and cancer diagnosis also playing a role in food-related awareness. Although family support is beneficial, it does not necessarily improve patients' knowledge of contraindications, indicating the need for targeted educational interventions for both patients and their families. By improving patient education and incorporating multidisciplinary care models, health care providers can reduce risks, enhance patient outcomes, and ultimately improve the quality of life for cancer patients.
Footnotes
Acknowledgments
The authors would like to acknowledge the Researchers Supporting Project number (RSP2025R115), King Saud University, Riyadh, Saudi Arabia, for extending financial support to do this research project. The authors are also thankful to AlMaarefa University for supporting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to express gratitude to King Saud University, Riyadh, Saudi Arabia, for extending financial support to do this research project through the Researchers Supporting Project number (RSP2025R115).