
Abstract
Introduction
EGFR and KRAS mutations are frequently detected in lung adenocarcinoma (LUAD). Tumor mutational signature (TMS) determination is an approach to identify somatic mutational patterns associated with pathogenic factors. In this study, through the analysis of TMS, the underlying pathogenic factors of LUAD with EGFR and KRAS mutations were traced.
Methods
This was a retrospective study. TMS of LUAD with KRAS and EGFR mutations from the TCGA, OncoSG, and MSK datasets was determined by two bioinformatics tools, namely the “MutationalPatterns” and “FitMS” packages. Elevated microsatellite alterations at selected tetranucleotide repeats (EMAST) of LUAD clinical specimens was analyzed using capillary electrophoresis.
Results
In LUAD with KRAS mutations, TMS analysis indicated that the smoking-related SBS4 signature was enriched. For LUAD with EGFR L858R mutation, the smoking-related SBS4 signature was enriched in the Western population from the TCGA database; however, the smoking-related SBS4 signature was not obvious in Asian LUAD patients. LUAD with EGFR exon19 deletion (19Del) exhibited stronger SBS15 signature, which was related to defective DNA mismatch repair. Capillary electrophoresis analysis showed that an EMAST locus was frequently instable in LUAD with EGFR 19Del. Different from the Western population, Asian LUAD patients with EGFR mutations exhibited the enrichment of SBS1, SBS2, and SBS13 signatures, which were associated with the endogenous mutation process of cytidine deamination.
Conclusions
TMS analysis reveals that smoking is associated with LUAD with KRAS mutations. Defective DNA mismatch repair and endogenous cytidine deamination are associated with LUAD with EGFR mutations, especially for the EGFR 19Del. The endogenous mutational process is stronger in Asian LUAD patients than Western LUAD patients.
Introduction
Cancer is presently the second most significant cause of mortality globally and places a considerable economic burden on public health systems. 1 Of these, lung cancer is the most common and most deadly cancer in the world. Lung cancer ranks first in terms of the number of new cases and deaths of cancer in China in 2020. 2 There are two subtypes of lung cancer: small cell lung cancer (SCLC) (15%) and non-small cell lung cancer (NSCLC) (85%). The World Health Organization has categorized NSCLC into three primary types, namely squamous cell carcinoma, adenocarcinoma and large cell carcinoma. 3 Lung adenocarcinoma (LUAD) is the most common subtype of NSCLC. Two-thirds of LUAD are characterized by the presence of activated oncogenes, such as KRAS, EGFR, translocated ALK, ROS1, or RET. EGFR and KRAS mutations are the most common oncogenic driver events in LUAD. 4 Among them, EGFR mutations are the most frequently detected oncogenic driver in east Asians, occurring at a rate of ∼50%, while in Westerners with LUADs, the incidence ranges from 10% to 15%. 5 In addition, KRAS mutations are present in nearly 30% of lung cancer cases. 4 The epidermal growth factor receptor (EGFR) belongs to the ErbB family of receptor tyrosine kinases, which plays a very critical role in the physiological process of epithelial cells, and it links extracellular signaling to the control of cell growth, survival, differentiation and proliferation. 6 Mutations of EGFR in the tyrosine kinase domain (18, 19, 20 and 21 exons) lead to constitutive EGFR activation and oncogenic signaling. 7 The L858R point mutation and exon 19 deletions (19Del) comprise the vast majority of EGFR mutations (approximately 85%). Other rare mutations include point mutations, insertions and deletions within exons 18 to 21 of the EGFR gene, which account for about 15% of the EGFR mutations in NSCLC. 8 KRAS encodes a membrane-bound guanosine triphosphatase. Nonsynonymous mutations frequently occur in codons 12, 13 and 61 in KRAS gene, and smoking has been closely associated with KRAS mutations in lung cancer. 9 Mutant forms of KRAS can lead to increased cellular proliferation and have oncogenic effects. 10
Smoking is the leading cause of lung cancer and is responsible for more than 80% of lung cancer cases. 11 While all major histologic subtypes of NSCLC, as well as SCLC, are associated with smoking, lung squamous cell carcinoma and SCLC are more strongly associated than LUAD, which is the most common histologic type among non-smokers. 11 Lung cancer from non-smokers is more common in Asian women and may be associated with environmental exposures such as secondhand smoke, occupational carcinogens, cooking oil vapors, and indoor coal combustion, as well as genetic susceptibility, but the exact cause is not known. 12 In the study, we hypothesized that besides smoking, other pathogenic factors (such as endogenous mutational process) were causative factors of LUAD, especially for the non-smoking patients.
Tumor mutational signature (TMS) determination is an emerging approach that integrates the somatic mutational landscape into individual tumors to identify mutational patterns associated with different pathogenic factors. 13 The main types of somatic mutations are single base substitutions (SBS) signatures, doublet base substitutions (DBS) signatures and small insertions and deletions (ID) signatures. Each mutational signature may be associated with the exogenous or endogenous mutagen exposures, intrinsic slight infidelity of the DNA replication machinery, enzymatic modification of DNA and defective DNA repair. 14 And different mutational processes usually produce unique combinations of mutational types on the basis of which the main pathogenic factors can be analyzed. At present, TMS has been widely used to reveal the molecular mutation processes and causative factors of specific cancers.15,16 Data mining by bioinformatics-based workflow has been broadly used to identify the potential biomarkers of cancer pathogenesis, treatment resistance and prognosis.17-20 Here, we focused on the study of LUAD using a TMS analysis to determine the major causative factor of EGFR mutations or KRAS mutations.
Methods
Data Acquisition
This was a retrospective study. Somatic mutation data of LUAD patients in TCGA database were acquired from here: https://xena.ucsc.edu/ (Dataset ID: TCGA-LUAD.mutect2_snv.tsv; Version: 07-20-2019). 58 LUAD patients with EGFR mutations (in exons 18, 19, 20 and 21) and 146 LUAD patients with KRAS mutations (at codons 12, 13 and 61) were collected in the study. Using TCGA criteria, “never smokers” is identified as non-smokers and “ever smokers” is identified as smokers. Somatic mutations and clinical data of 171 LUAD patients from Singapore were collected in OncoSG (https://src.gisapps.org/OncoSG/) under dataset “Lung Adenocarcinoma (GIS, 2019)”. 21 Somatic mutations and clinical data of 197 LUAD patients from MSK dataset were collected in cBioPortal (https://www.cbioportal.org/study/summary?id=nsclc_ctdx_msk_2022). 22 The OncoPrint for EGFR and KRAS mutations were drawn using “maftools” package in R (version 4.1.3).
Mutational Signature Analysis
Somatic mutation data of TCGA LUAD samples were aligned to the human reference genome (GRCh38), while somatic mutation data from Asian LUAD samples were aligned to the human reference genome (GRCh37). Based on the six substitution classes (T>A, T>C, T>G, C>A, C>G, C>T) and the bases immediately 5′ and 3′ to the mutated base, the signature of 96 possible mutation subtypes were produced. The mutation signature of each sample was compared with 79 known COSMIC mutational signatures (https://cancer.sanger.ac.uk/cosmic/signatures; Database version 3.3, June 2022), and the contribution of different mutation signatures of each sample was determined and scored. The analysis was performed using the “MutationalPatterns” package 23 and “FitMS” package 24 in R (version 4.1.3).
DNA Extraction
Formalin-fixed paraffin-embedded (FFPE) LUADs tissues (tumor tissues and normal adjacent tissues) were obtained from Hefei Cancer Hospital, Chinese Academy of Sciences. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Hefei Cancer Hospital, Chinese Academy of Sciences (approval number: SL-KY2023-081). All patients agreed to the use of their FFPE samples for the study by providing written informed consent. All details information identifying the patients have been removed. Genomic DNA was extracted from 10 to 15 FFPE sections using the GeneRead DNA FFPE Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. The concentration of the extracted DNA was quantified using Qubit 4.0 fluorometer (Thermo Fisher Scientific, MA, USA).
The Analysis of Elevated Microsatellite Alterations at Selected Tetranucleotide Repeats (EMAST)
EMAST analysis was performed using a tetranucleotide locus D20S85. The primers of the nest PCR for the site D20S85 were shown as follow: outer primer (forward primer: 5′-GACTCTCAGAATGGGTCAG-3′, reverse primer: 5′-CTGTGTATGGCAATGCAC-3′) and inner primer (forward primer: 5′-GACTTGATGGGAGTATCCAGAGAG-3′, reverse primer: 5′-CATGAATTACAGTGTGAGACC-3′).
Amplification reactions (10 μL) were prepared subjected to two round PCR amplification using the nest primers with an initial incubation at 94°C for 4 minutes; 39 cycles of denaturation at 94°C for 50 seconds, annealing at 55°C for 40 seconds, and extension at 72°C for 35 seconds; and final extension at 72°C for 5 minutes. PCR products were analyzed on the capillary electrophoresis (Qsep1, Bioptic, Taiwan).
Statistical Analysis
All analyses were performed with R version 4.1.3 and corresponding packages. Wilcoxon test and t test were used to compare the difference. P < 0.05 was considered to be significant.
Results
LUAD Tumors with KRAS Mutation Exhibit Stronger Smoking-Related Mutation Signature Than LUAD Tumors with EGFR Mutation
The flowchart of this study was shown in Figure 1. The reporting of this study conforms to STROBE guidelines.
25
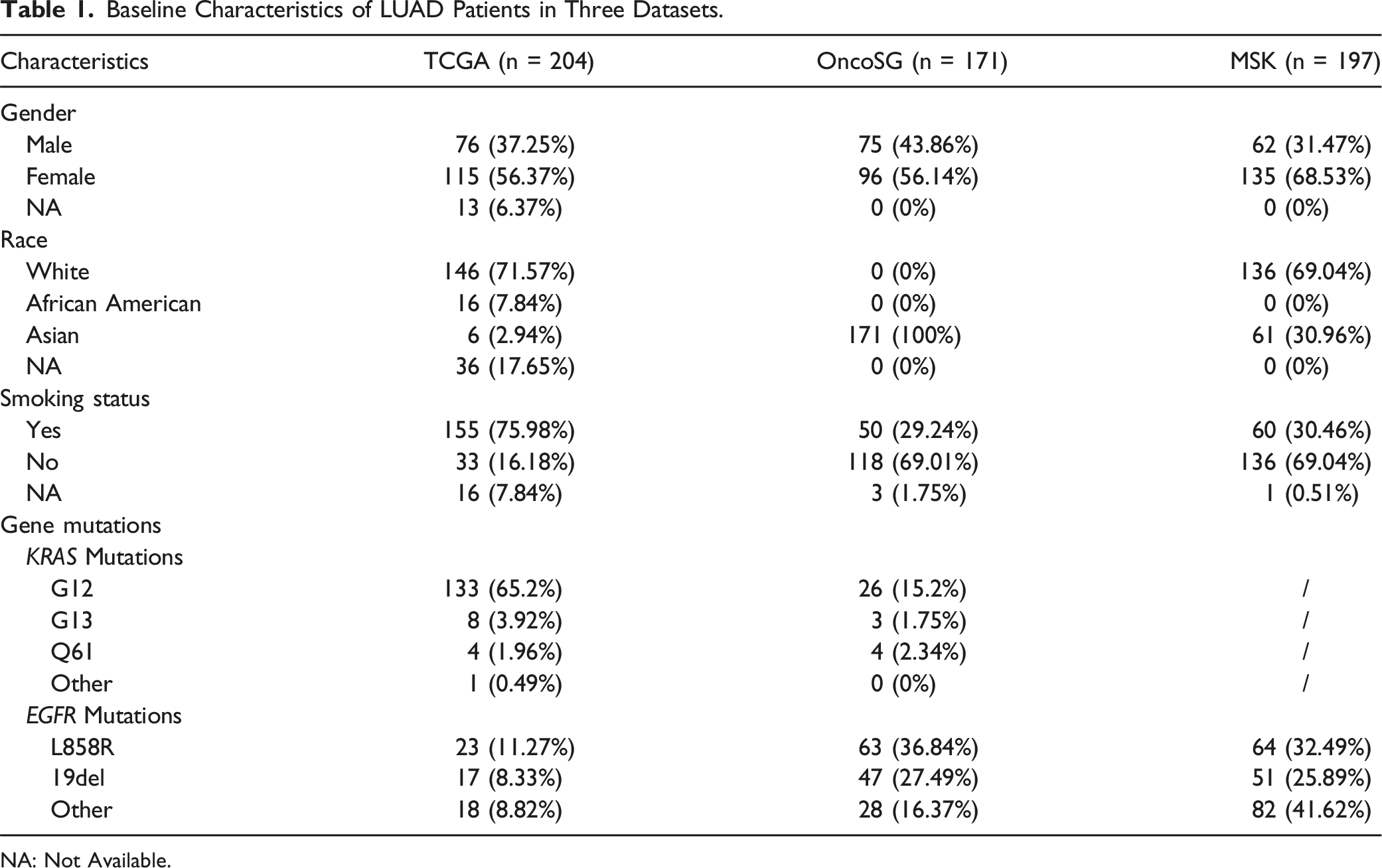
We downloaded somatic mutation data of LUAD tumors from TCGA database (Table 1 and Supplemental Table 1). Among these LUAD tumors, 26% of samples harbored KRAS mutations, and 10% of samples harbored EGFR mutations. KRAS mutations were mainly missense variants, and EGFR mutations were mainly missense and inframe-deletion variants. Mutations in EGFR and KRAS genes have a strongly mutually exclusive distribution (Figure 2(A)). Since smoking is associated with a high tumor mutation burden (TMB), we compared the TMB between LUADs with EGFR mutations and KRAS mutations. The TMB level of LUADs with KRAS mutations was significantly higher than that of LUADs with EGFR mutations (Figure 2(B)). Next, we extracted TMS, including SBS signatures and ID signatures, in LUAD samples with EGFR mutations and KRAS mutations, respectively (Supplemental Table 2). The proportion of each mutation signature for each sample was shown in Figure 2(C) (SBS signature) and Figure 2(D) (ID signature). The flowchart of this study. Baseline Characteristics of LUAD Patients in Three Datasets. NA: Not Available. The extraction of mutational signatures for LUAD with EGFR and KRAS mutations in TCGA dataset. (A) OncoPrint showing the LUAD samples with EGFR and KRAS mutations in the TCGA dataset. The smoking status and gender are shown. (B) Boxplot showing the level of TMB of LUAD samples with EGFR and KRAS mutations. (C) TMS profiles derived from SBS signatures for each patient with EGFR and KRAS mutations. The x-axis represents different patients, while the y-axis represents the proportion of different SBS signatures. (D) TMS profiles derived from ID signatures for each patient with EGFR and KRAS mutations. The x-axis represents different patients, while the y-axis represents the proportion of different ID signatures.

Based on the proportion of mutation signatures in each patient, the mean contributed proportions of each SBS and indels ID signatures were calculated for LUAD samples with EGFR mutations and KRAS mutations, respectively (Supplemental Table 3). Furthermore, we selected out the mutation signatures with a mean contributed proportions more than 0.02 in either group and compared the difference between the two groups (Figure 3(A) and (B)). In LUAD with KRAS mutations, the major contributed mutation signature was identified SBS4, a signature caused by tobacco carcinogens such as benzo[a]pyrene exposure. However, the SBS4 signature was much weaker in LUAD with EGFR mutations. The major contributed mutation signature was identified SBS1 and SBS15 in LUAD with EGFR mutations (Figure 3(A)). The SBS1 signature is an endogenous and spontaneous mutational process of 5-methylcytosine deamination. The SBS15 signature is associated with defective DNA mismatch repair.
26
For ID signature, ID8 was the major contributed mutation signature in both groups with EGFR and KRAS mutations. The proportion of ID8 in LUAD with EGFR mutation was higher than that in LUAD with KRAS mutation (Figure 3(B)). The causative factor for ID8 signature is largely unknown.
14
The SBS signatures were also displayed using the 96-substitution classification. C-to-T transitions frequently occurred in LUAD with EGFR mutations, while C-to-A transversions frequently occurred in LUAD with KRAS mutations (Figure 3(C) and (D)). Therefore, TMS analysis indicates that LUAD tumors with KRAS mutation exhibit stronger smoking-related mutation signature than LUAD tumors with EGFR mutation. The comparison of TMS between EGFR and KRAS mutated LUAD tumors. (A) The heatmap showing the mean contributed value of each SBS signature in LUAD tumors with EGFR and KRAS mutations. The boxplot showing the contributed proportions of SBS signatures with the significant difference between the two groups. Only the mean contributed proportions (>0.02) in either group are selected out. (B) The heatmap showing the mean contributed value of each ID signature in LUAD tumors with EGFR and KRAS mutations. The boxplot showing the contributed proportions of ID signatures with the significant difference between the two groups. Only the mean contributed proportions (>0.02) in either group are selected out. (C) Number of each single-nucleotide substitution for LUAD samples with EGFR and KRAS mutations. X axis displays the 96 substitutions classification defined by the substitution type and sequence context immediately 5′ and 3′ to the mutated base. Y axis displays the relative quantity of each classification. (D) Relative contribution of each single-nucleotide substitution in LUAD samples with EGFR mutations and KRAS mutations. X axis displays the six main types of single-base substitutions. Y axis displays the relative contribution.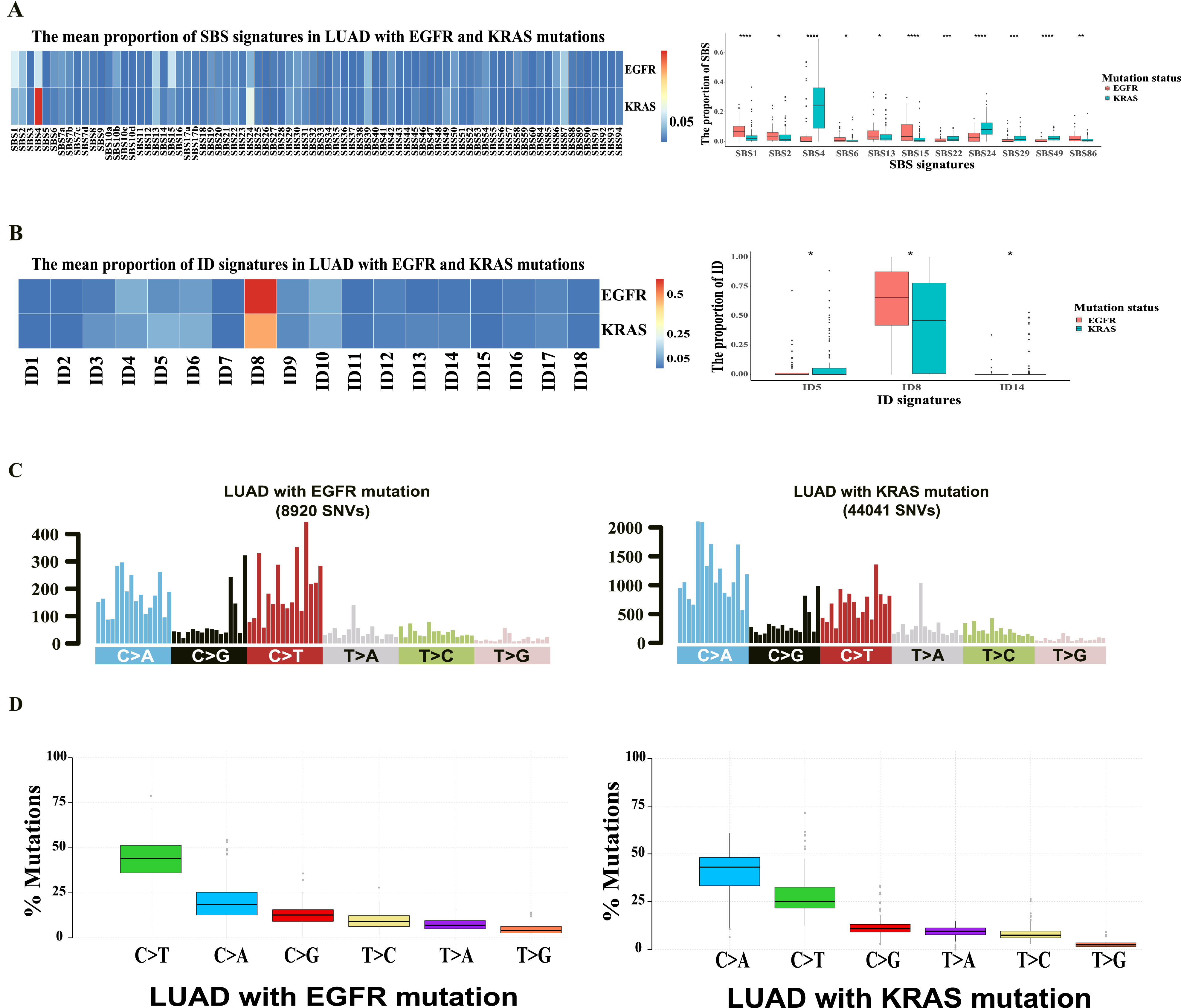
Non-smoking LUAD patients with EGFR mutation exhibit stronger SBS15 mutation signature than smoking LUAD patients with EGFR mutation
In order to explore the causative factors of EGFR mutation in LUAD patients, we further performed mutation signatures analysis in LUAD patients with EGFR mutations. Firstly, we divided the LUAD patients with EGFR mutations into two groups based on smoking status (Supplemental Table 3). The proportion of SBS4 signature in smoking patients was significantly higher than those in non-smoking patients, while SBS15 signature in non-smoking patients was significantly higher than those in smoking patients (Figure 4(A)). Furthermore, we divided LUAD patients with EGFR mutations into four groups: male smoking, male non-smoking, female smoking and female non-smoking (Supplemental Table 3). The signature SBS15 was significantly higher in female non-smoking patients compared with female smoking patients. The signature SBS4 was significantly higher in female smoking patients compared with female non-smoking patients (Figure 4(B)). But the comparisons did not reach the statistical significance in male (Figure 4(B)). Moreover, we compared the contribution of mutation signatures among the four groups. The contribution of SBS4 signature was enriched in male and female smoking patients, while SBS15 signature was enriched in male and female non-smoking patients (Figure 4(C)). Therefore, in LUAD patients with EGFR mutation, smokers exhibited stronger SBS4 mutational signature, while non-smokers exhibited stronger SBS15 mutational signature. The TMS signature of LUAD with EGFR mutations in TCGA dataset. (A) The heatmap showing the mean contributed value of each SBS signature in LUAD samples with EGFR mutations based on the smoking status. The boxplot showing the contributed proportions of SBS signatures with the significant difference between the smokers and non-smokers. Only the mean contributed proportions (>0.02) in either group are selected out. (B) The heatmap showing the mean value of each SBS signature in LUAD samples with EGFR mutations based on gender and smoking status. The boxplot showing the contributed proportions of SBS signatures with the significant difference between the groups. Only the mean contributed proportions (>0.02) in either group are selected out. (C) Similarity comparison of SBS signatures with the COSMIC signatures in LUAD samples with EGFR mutations among the four groups.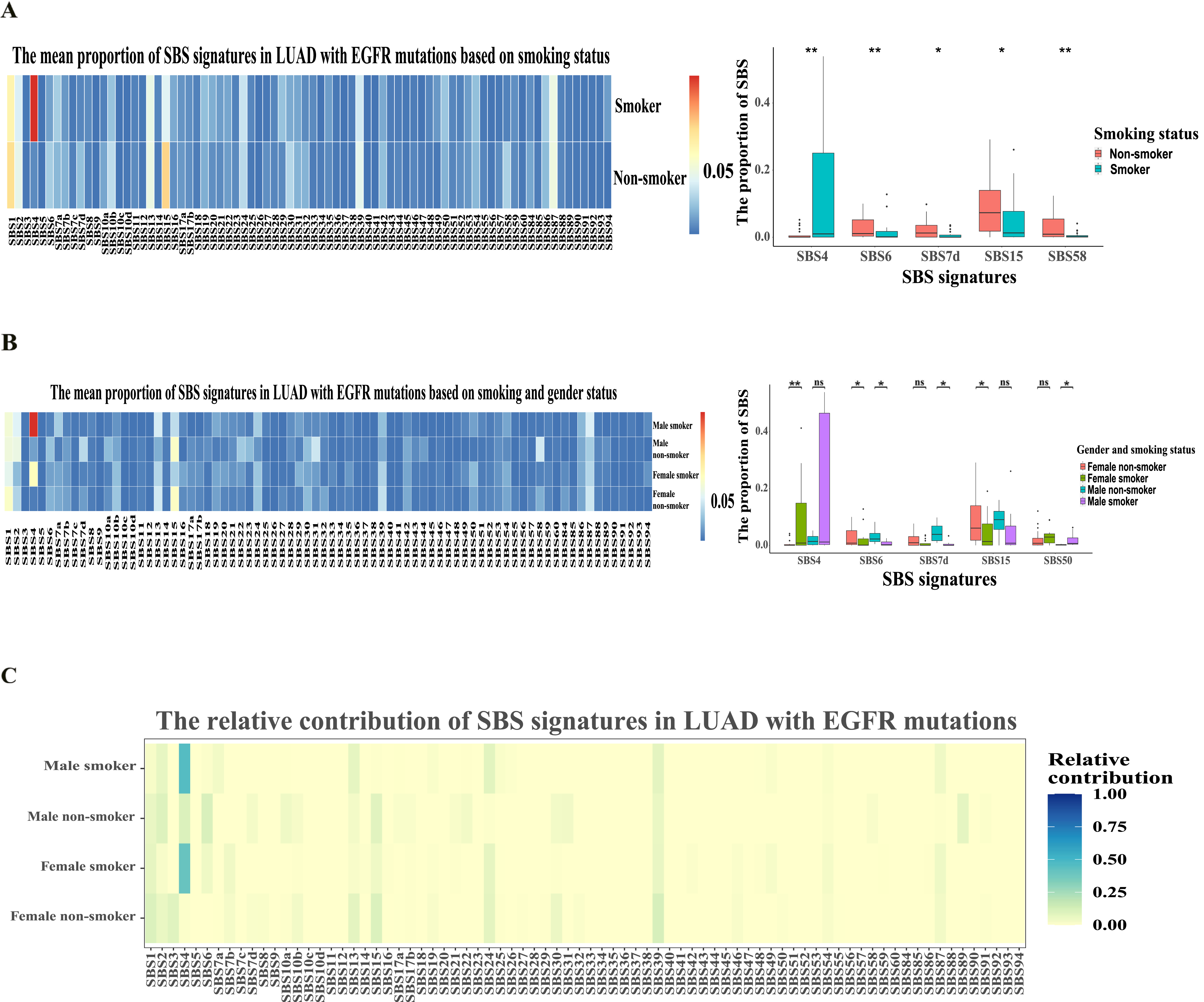
LUAD tumors with EGFR 19Del mutation exhibit stronger SBS15 mutation signature than LUAD tumors with EGFR L858R mutation
In LUAD, L858R point mutation and 19Del are two main subtypes of EGFR mutation. We compared the mutation signatures in LUAD with EGFR mutations between L858R mutation and 19Del (Supplemental Table 3). We found that SBS4 signature was significantly enriched in the L858R mutation group, while SBS15 signature was significantly enriched in 19Del group (Figure 5(A)). The proportion of SBS15 signature in EGFR 19Del LUADs were significantly higher than those in EGFR L858R mutated LUADs (Figure 5(B)). EGFR 19Del mutations were frequently detected in female non-smoking patients, whereas EGFR L858R mutations were frequently detected in female smoking patients (Figure 5(C)). This suggests that EGFR L858R mutation tends to be associated with smoking, whereas EGFR exon 19 deletion tends to be associated with defective DNA mismatch repair. Defective DNA mismatch repair is associated with microsatellite instability (MSI). However, previous studies have indicated that MSI occurred in a few of LUAD tumors, while studies have reported that a distinct form of MSI, which was called elevated microsatellite alterations at selected tetranucleotide repeats (EMAST) often occurred in LUAD.
27
Thus, we collected the LUAD specimens with EGFR 19Del and L858R mutations to determine EMAST (Figure 5(D)). In 21 LUAD samples with EGFR 19Del, we detected 18 samples (85.7%) with EMAST at D20S85 loci, while in 21 LUAD samples with EGFR L858R, we detected 11 samples (52.4%) with EMAST at D20S85 loci (Figure 5(E)). Therefore, our study suggests that LUAD tumors with EGFR 19Del exhibit stronger defective DNA mismatch repair than LUAD tumors with EGFR L858R mutation. The TMS signature of LUAD with EGFR L858R and 19Del mutations in TCGA dataset. (A) The heatmap showing the mean value of each SBS signature in LUAD samples with EGFR L858R and 19Del mutations. (B) The boxplot showing the contributed proportions of SBS signatures with the significant difference between the two groups. Only the mean contributed proportions (>0.02) in either group are selected out. (C) Distribution of the number of LUAD patients with EGFR L858R and 19Del mutations. EGFR 19Del mutations frequently occurred in female non-smoking LUAD patients. (D) The representative map of capillary electrophoresis for the detection of EMAST marker (D20S85 site). The EMAST (D20S85 site) is instable in the tumor tissue of a LUAD sample with EGFR 19Del mutation. The EMAST (D20S85 site) is stable in the tumor tissue of a LUAD sample with EGFR L858R mutation. (E) EMAST frequently occurred in LUAD with EGFR 19Del mutations.
The feature of TMS in Asian LAUD Patients with KRAS and EGFR Mutations
Previous study has indicated that EGFR mutations were often detected in east Asians. However, most of patients in TCGA were Westerners. Therefore, we collected somatic mutations and clinical data of 302 LUAD patients from Singapore in a previous study. 21 In this Asian cohort, 46% of LUAD samples harbored EGFR mutations, and 11% of samples harbored KRAS mutations (Table 1, Supplemental Figure 1A and Supplemental Table 1). Similarly, mutations in EGFR and KRAS genes have a strongly mutually exclusive distribution, and the TMB level of LUADs with KRAS mutations was significantly higher than that of LUADs with EGFR mutations (Supplemental Figure 1A and 1B). We extracted SBS signatures and ID signatures in these LUAD samples (Supplemental Figure 1C and 1D, Supplemental Table 2).
Likewise, in Asian LUAD with KRAS mutations, the major contributed mutation signature was SBS4 (Figure 6(A) and Supplemental Table 3). For ID signature, ID8 was the major contributed mutation signature in both groups with EGFR and KRAS mutations. The proportion of ID8 in LUAD tumors with EGFR mutation was higher than that in LUAD tumors with KRAS mutation (Figure 6(B) and Supplemental Table 3). Next, we divided the LUAD patients with EGFR mutations into two groups based on smoking status. Different from TCGA samples of Westerners, SBS4 signature in Asian smoking LUAD patients with EGFR mutations was not obvious. The main contributed mutation signatures were SBS1, SBS2, SBS13, SBS15 and SBS87 in LUAD patients with EGFR mutations. Among these signatures, the proportion of SBS1 signature in non-smoking patients was significantly higher than those in smoking patients (Figure 6(C) and Supplemental Table 3). The TMS signature of LUAD with EGFR and KRAS mutations in Asian dataset. (A) The heatmap showing the mean value of each SBS signature in LUAD samples with EGFR and KRAS mutations. (B) The heatmap showing the mean value of each ID signature in LUAD samples with EGFR and KRAS mutations. (C) The heatmap showing the mean value of each SBS signature in LUAD samples with EGFR mutations based on smoking status. (D) The heatmap showing the mean value of each SBS signature in LUAD samples with EGFR L858R and 19Del mutations. (E) The boxplot showing the contributed proportions of SBS signatures with the significant difference between the two groups. Only the mean contributed proportions (>0.02) in either group are selected out. (F) The distribution of the number of LUAD patients with EGFR L858R and 19Del mutations.
Finally, we compared the mutation signatures in Asian LUAD patients with EGFR mutations between L858R mutation and exon 19 deletion. We also found that the proportion of SBS15 signature was significantly higher in LUAD patients with EGFR 19Del, compared with LUAD patients with EGFR L858R (Figure 6(D) and (E), Supplemental Table 3). Same with TCGA LUAD samples, EGFR 19Del mutations were frequently detected in Asian female non-smoking LAUD patients. But different from TCGA LUAD samples, EGFR L858R mutations were frequently detected in female non-smoking patients (Figure 6(F)). Therefore, these data indicate that smoking-related SBS4 signature is the main contributed mutation signature in Asian LUAD patients with KRAS mutation, while Asian LUAD patients with EGFR mutations exhibited stronger SBS1, SBS2 and SBS13 mutational signatures, regardless of smoking status.
Asian LUAD patients with EGFR mutation exhibit stronger endogenous SBS1 mutational signature than Western LUAD patients with EGFR mutation
Finally, we used another bioinformatics tool “FitMS”
24
to determine the TMS in Western and Asian LUADs. We divided LUAD patients with EGFR mutations into two groups: smoking and non-smoking. In the TCGA cohort, smoking LUAD patients had the highest SBS4 signature (Figure 7(A)), and the SBS1 signature was relatively high in the non-smoking groups (Figure 7(A)). However, in the Asian LUAD patients, the SBS1 feature was highest in the all two groups, while the SBS4 feature was relatively weak even in smoker LUAD patients (Figure 7(B)). Furthermore, we used an additional dataset, MSK cohort including both Western and Asian LUAD patients (Table 1 and Supplemental Table 1). Similarly, smoking LUAD with EGFR mutations had the highest SBS4 signature and non-smoking LUAD had relatively higher SBS1 signature in Western population (Figure 7(C)). In Asian population, SBS4 signature was very weak in smoking LUAD with EGFR mutations, while SBS1 signature was highest in both smoking and non-smoking LUAD with EGFR mutations (Figure 7(D)). The data suggest that the endogenous SBS1 mutational signature is stronger in Asian LUAD patients with EGFR mutation, compared with Western LUAD patients with EGFR mutation. Mutation signature determination and contribution was conducted utilizing another tool (FitMS). (A) The map indicating the contribution of the SBS mutational signatures in smoking and non-smoking LUAD with EGFR Mutations in the TCGA database. (B) The map indicating the contribution of the SBS mutational signatures in smoking and non-smoking LUAD with EGFR mutations in the Asian database. (C) The map indicating the contribution of the SBS mutational signatures in smoking and non-smoking LUAD with EGFR mutations in the Western population of MSK dataset. (D) The map indicating the contribution of the SBS mutational signatures in smoking and non-smoking LUAD with EGFR mutations in the Asian population of MSK dataset.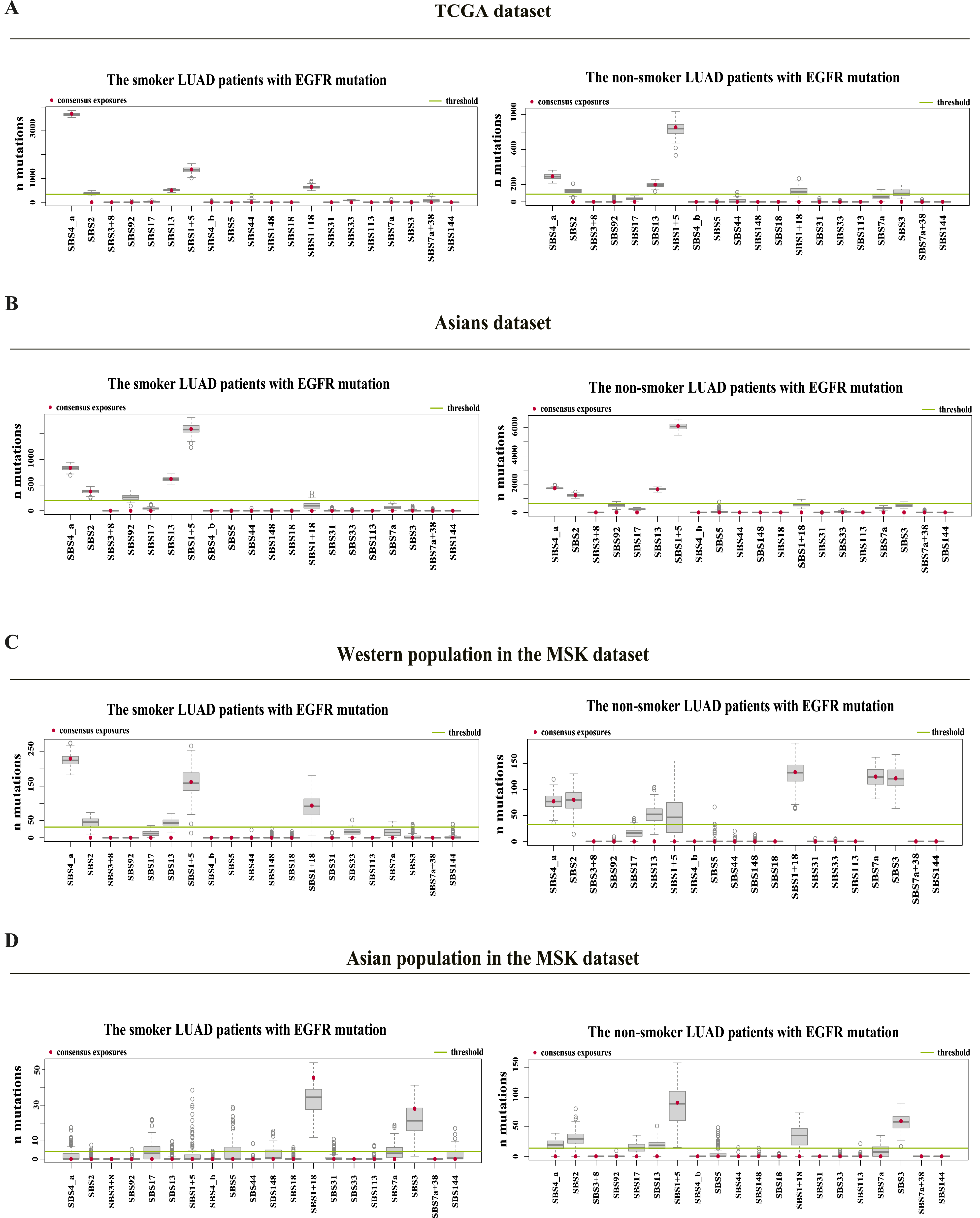
Discussion
A majority of lung cancer cases are closely associated with the pernicious habit of smoking. Previous study has demonstrated that smoking-related SBS4 signature was frequently found in LUAD. 28 The emissions generated by smoking give rise to the accumulation of driver mutations, ultimately culminating in the development of lung cancer. 29 In this study, we further explored the primary etiological factors behind KRAS and EGFR mutations in LUAD, by using the analysis of mutational signature.
Firstly, our study found a significant enrichment of SBS4 mutation signature in LUAD patients with KRAS mutations. This is consistent with a previous study, which reported that smoking-related SBS4 signature was frequently observed in KRAS-mutated LUAD. 30 96-substitution classification revealed that C-to-A transversions frequently occurred in LUAD with KRAS mutations. Previous study has indicated the higher prevalence of C>A mutations was associated with the formation of adducts on guanine by tobacco carcinogens. 14 Furthermore, we found that TMB was higher in LUAD with KRAS mutations. A previous study has reported that NSCLC harboring SBS4 signature had a higher median TMB than NSCLC with other signatures. 31 High TMB is a predictive biomarker for the response of immune checkpoint blockade-based therapy. 32 Therefore, KRAS mutation-associated SBS4 signature may be used as biomarkers for the response to immunotherapy.
We found that smoking-related SBS4 signature was also present in smoking LUAD patients with EGFR mutation in TCGA Western population. Particularly, smoking-related SBS4 signature was associated with EGFR L858R mutation, rather than EGFR exon19 deletion. However, in Asian population, SBS4 signature was very weak in smoking LUAD with EGFR mutations. A recent publication reported that in a Chinese LUAD cohort, the SBS4 signature was not associated with smoking status, but SBS4 activity was higher in Chinese male LUAD patients than female patients. 33 The recent study is consistent with our study that indicated that SBS4 signature was not enriched in Asian smoking LUAD with EGFR mutations, because EGFR mutations mostly occurred in Asian female LUAD patients. We think that it may be because of higher rates of smoking among Chinese males compared to Chinese females. Although some Chinese female LUAD patients smoke, they may smoke lightly. Therefore, SBS4 signature was not enriched in Asian smoking LUAD with EGFR mutation.
For non-smoking patients with EGFR mutations, we have observed a marked enrichment of the SBS15 mutation signature. Further analysis of the two major mutations (L858R and 19Del) in EGFR gene has revealed a significant enrichment of SBS15 in LUAD patients with 19Del mutations. SBS15 is a signature which is associated with defective DNA mismatch repair and microsatellite instability. 26 Using the collected LUAD samples with EGFR mutations, we observed that an EMAST locus (D20S85) was frequently instable in LUAD samples with EGFR 19Del. Previous studies have reported that EMAST often occurred in approximately 32%∼64.5% of lung cancers. 34 Jiang et al have reported that high inflammation response index was associated with EGFR 19Del mutation. 35 Tumors with EMAST have been found to be also associated with chronic inflammation. Inflammation might have an impact on the function of MSH3. The inflammatory tumor microenvironment contains free oxygen radicals from oxidative stress and pro-inflammatory cytokines, which might be the main drivers of loss of nuclear MSH3. In vitro studies have revealed that IL-6 and oxidative stress in the form of hydrogen peroxide, can trigger the translocation of MSH3 from nucleus to the cytosol, thereby inducing instability at EMAST loci. 36 Munakata et al. reported a reduced nuclear expression of MSH3 by the increased IL-6 expression in the non-neoplastic epithelium of patients with ulcerative colitis. 37 Therefore, inflammation results in EMAST, which might be associated with EGFR 19Del. Our and these previous data imply that LUAD with EGFR 19Del may be associated with inflammation.
Our study demonstrated the differences of TMS in LUAD tumors with EGFR mutations between Asian and Western population. EGFR mutation frequently occurred in Asian female non-smoking patients. 38 In Asian LUAD patients with EGFR mutations, the main contributed mutation signatures were SBS1, SBS2 and SBS13. SBS1 is an endogenous mutational process initiated by spontaneous deamination of 5-methylcytosine. SBS2 and SBS13 have been proposed that activation of AID/APOBEC cytidine deaminases may be due to previous viral infection, retrotransposon jumping, or tissue inflammation. 39 Previous studies have demonstrated that age-associated signature (SBS1) and APOBEC-associated signatures (SBS2 and SBS3) contributed to endogenous mutational processes in LUAD.26,40 Therefore, infection and inflammation may be the susceptibility factors in Asian LUAD with EGFR mutations. Our data further suggest that endogenous mutational process may be stronger in Asian population than that in Western population. That may be due to genetic factors that result in the decreased ability of cells to repair DNA damage in Asian population.
However, our study has some limitations. Firstly, the number of samples is limited. The results found by TMS analysis need to been validated in larger LUAD population. Secondly, SBS1, SBS2 and SBS13 enriched in Asian LUAD with EGFR mutations may be associated with genetic factor, infection and inflammation. It remains speculative. Further studies need to investigate the history of inflammation and viral infections in Asian LUAD patients with EGFR mutations. In addition, the genetic variants that affect DNA damage repair need to be studied in Asian LUAD patients with EGFR mutations. Thirdly, in the MSK cohort, some LUAD patients were subjected to the prior treatment. which may affect the result of TMB analysis. Some confounding factors, such as inflammation or infection, may influence the results of TMS analysis.
Conclusion
Through TMS signature analysis, the study reveals that LUAD tumors with KRAS mutation display markedly increased smoking-related SBS4 signature. In Western population, LUAD tumors with EGFR L858R mutation also exhibit the strong enrichment of SBS4 signature, but SBS4 signature is not enriched in Asian LUAD with EGFR L858R mutation. LUAD tumors with EGFR 19Del exhibit notably enhanced SBS15 signature, which is associated with DNA mismatch repair deficiency and microsatellite instability. Additionally, Asian LUAD patients carrying EGFR mutation show stronger endogenous cytidine deamination-related mutation processes (SBS1, SBS2 and SBS13 signatures), regardless of smoking status. In summary, our study has identified a significant association between smoking and KRAS mutation, further emphasizing smoking as a risk factor for LUAD. Our study finds that defective DNA mismatch repair and endogenous cytidine deamination are associated with LUAD with EGFR mutations, which provides a direction for the future study to explore molecular mechanisms of pathogenesis in non-smoking LUAD patients with EGFR mutations.
Supplemental Material
Supplemental Material - Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation
Supplemental Material for Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation by Jialiang Wang, Chang Guo, Jiexiao Wang, Xiaopeng Zhang, Jian Qi, Xiang Huang, Zongtao Hu, Hongzhi Wang, and Bo Hong in Cancer Control.
Supplemental Material
Supplemental Material - Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation
Supplemental Material for Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation by Jialiang Wang, Chang Guo, Jiexiao Wang, Xiaopeng Zhang, Jian Qi, Xiang Huang, Zongtao Hu, Hongzhi Wang, and Bo Hong in Cancer Control.
Supplemental Material
Supplemental Material - Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation
Supplemental Material for Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation by Jialiang Wang, Chang Guo, Jiexiao Wang, Xiaopeng Zhang, Jian Qi, Xiang Huang, Zongtao Hu, Hongzhi Wang, and Bo Hong in Cancer Control.
Supplemental Material
Supplemental Material - Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation
Supplemental Material for Tumor Mutation Signature Reveals the Risk Factors of Lung Adenocarcinoma with EGFR or KRAS Mutation by Jialiang Wang, Chang Guo, Jiexiao Wang, Xiaopeng Zhang, Jian Qi, Xiang Huang, Zongtao Hu, Hongzhi Wang, and Bo Hong in Cancer Control.
Footnotes
Authors’ Contributions
B. H. and H. W. designed the study. J. W. (Jialiang Wang), X. Z., X. H. and Z. H. collected the samples and performed the EMAST analysis. J. W. (Jialiang Wang), J. W. (Jiexiao Wang), C. G. and J. Q. performed the bioinformatic analysis. J. W. (Jialiang Wang) wrote the first draft of the manuscript. B. H. and H. W. revised the manuscript. All authors reviewed the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (81872438), the Program of Research and Development of Key Common Technologies and Engineering of Major Scientific and Technological Achievements in Hefei (2021YL007), the Collaborative Innovation Program of Hefei Science Center, CAS (2022HSC-CIP015), and the Program of Clinical Medical Translational Research in Anhui Province (Grant Numbers: 202304295107020092).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.