
Abstract
Objective
This study explored the relationship between perceptions of health mis/disinformation on social media and belief that progress has been made in curing cancer.
Methods
We analyzed cross-sectional, retrospective data collected from 4246 adult social media users in the 2022 Health Information National Trends Survey (HINTS 6). The outcome variable was the belief in whether progress has been made in curing cancer. The primary predictor variable was the perception of health mis/disinformation on social media, categorized as ‘Substantial’ and ‘< Substantial’. We also examined whether the relationship varied by health care system trust, frequency of social media use, and education. The analysis controlled for demographic, socioeconomic, and health-related factors.
Results
Perception of substantial social media health mis- and disinformation was associated with a lower likelihood of believing progress has been made in curing cancer (odds ratios = 0.74, 95% CI = 0.59-0.94). Persons who perceived substantial social media health mis-and disinformation and had low trust in the health care system were less likely to believe progress has been made in curing cancer: 36% (95% CI: 28-45%). Persons who perceived substantial social media health mis-and disinformation and used social media less than daily were less likely to believe progress has been made in curing cancer: 44% (95% CI: 36-52%). Persons without a college degree who perceived substantial social media health mis-and disinformation were less likely to agree that progress has been made in curing cancer: 44% (95% CI: 39-50%).
Conclusion
Exposure to misinformation on social media may be associated with negative attitudes about advances in curing cancer, particularly among social media users with low trust in the health care system trust, less frequent social media users, or those without a college degree.
Keywords
Introduction
Social media has revolutionized the field of health communication, acting as a channel for both reliable and deceptive health-related information. 1 Social media platforms serve as a crucial source of health information for many individuals and play a vital role in public health communication.2-4 Nevertheless, the unrestricted and unregulated nature of these platforms has also enabled the widespread dissemination of health misinformation and disinformation.5,6 Misinformation refers to false or misleading information shared unintentionally, while disinformation denotes the deliberate creation and dissemination of false information. 7 The consequences of such misinformation and disinformation are far-reaching, potentially leading to harmful health behaviors, decreased vaccination rates, and the undermining of public trust in health institutions.8,9
The dynamics of information seeking and belief formation can be explored through the lens of the Health Belief Model (HBM). 10 The HBM posits that individuals’ perceptions of susceptibility to cancer and the severity of the disease can influence their motivation to seek information. In this context, we can examine if exposure to perceived health misinformation on social media shapes individual perceptions of cancer curability, potentially lowering their perceived susceptibility or severity. 11 This could then indirectly influence their belief in advancements made in cancer treatment.
Cancer is a critical area of focus because it remains one of the leading causes of death worldwide. 12 Beliefs about progress in curing cancer can significantly impact public support for research funding, participation in clinical trials, and adherence to preventive measures and treatments.13-15 Examining these beliefs in the context of misinformation and disinformation is essential because skewed perceptions can hinder efforts to improve cancer outcomes.
Beliefs about cancer can be shaped by education, as suggested by the HBM. 10 Individuals with higher educational attainment might be better equipped to critically evaluate information, potentially leading to a lower perception of susceptibility to misinformation and a more nuanced understanding of the disease’s severity. 16 Recent research supports this notion, suggesting that education enhances critical thinking skills and source verification when evaluating online health information.17,18
Additionally, trust in the health care system can act as a filter for information credibility. 19 In this study, “trust in the health care system” is defined as the confidence individuals have in the competence, reliability, and integrity of health care providers and institutions. 20 People with high trust are more likely to view information from established medical sources as credible, while low trust can make individuals more susceptible to misinformation.21,22 Studies have shown a link between trust in health care providers and adherence to treatment plans, highlighting the influence of trust on how individuals interpret and act upon health information.23-26 By incorporating the moderating effects of both education and trust, this study can offer a richer understanding of how misinformation disrupts the information-seeking process and shapes health beliefs. 27
Our research explores the interplay between the perception of health misinformation and disinformation on social media and the belief in the progress made in curing cancer. The guiding research questions are: What is the relationship between perceptions of health misinformation and disinformation on social media and the belief in advancements in cancer treatment? And how does this relationship vary by trust in the health care system, frequency of social media use, and educational attainment? Understanding these dynamics is vital for devising public health strategies and communication campaigns to counter misinformation and enhance public awareness of medical progress. By pinpointing the factors influencing beliefs about medical advancements, findings from this study can help inform tailored interventions to enhance public perceptions and foster trust in health care innovations.
The research questions drive several hypotheses. The first hypothesis posits that individuals perceiving substantial health misinformation and disinformation on social media are less likely to believe in significant progress in curing cancer. This is premised on the idea that misinformation and disinformation can skew public perceptions of scientific progress and erode trust in medical advancements. While it is conceptually possible that trust in medical advancements might influence perceptions of misinformation, this study focuses on the more direct pathway where misinformation impacts trust. The second hypothesis suggests that those with low trust in the health care system, compounded by negative perceptions, are least likely to acknowledge progress in cancer treatment. This recognizes that trust in the health care system is instrumental in shaping health beliefs and attitudes, and that misinformation and disinformation can further undermine this trust. The third hypothesis suggests that the frequency of social media use will moderate the relationship between perceived health misinformation and beliefs about cancer progress. Specifically, less frequent social media users that perceive substantial misinformation are hypothesized to be more vulnerable to its negative effects, making them significantly less likely to believe in progress in curing cancer compared to persons that do not perceive substantial misinformation. This hypothesis highlights the potential compounding effect of both misinformation and lower frequency of engagement with social media on public health perceptions. 11 The fourth hypothesis proposes that individuals with lower educational attainment, particularly those without a college degree, are less likely to believe in advancements when they perceive high levels of misinformation and disinformation. This acknowledges the role of education in fostering critical thinking skills necessary to distinguish credible information from misinformation and disinformation.
Methods
Data
This retrospective, cross-sectional study utilized nationally representative data from the Health Information National Trends Survey 6 (HINTS 6). HINTS 6 surveys non-institutionalized adults (18 years and older) in the United States (US) about health communication and cancer prevention attitudes and behaviors. The data were collected via mail and online surveys from March to November 2022, achieving a response rate of 28.1%. Detailed survey methodology is available from the National Cancer Institute. 28 Participants who reported not using social media in the survey item that asked about perceptions of social media information were excluded (N = 1211). In addition, we used listwise deletion for missing information on any of the variables used in the study (N = 713), resulting in a final, nationally representative sample of 4246 adult social media users. We conducted post-hoc power calculations to ensure the adequacy of our sample size. Given the effect sizes observed in the analysis, our sample size of 4246 respondents provided over 80% power to detect significant associations at a 0.05 significance level, particularly for the primary predictor variable (perception of health mis/disinformation on social media).
Measures
The outcome measure was derived from respondents’ answers to the question, “How much progress has been made in curing cancer?” This measure has been used to investigate cancer fear, worry, and perceived risk.26,29-31 Response options included: “almost none,” “a little,” “don’t know,” “some,” and “a lot.” Following a recent study, this measure was dichotomized into “progress” (“some” or “a lot”) vs “no progress” (“almost none,” “a little,” or “don’t know”). 26
The primary predictor variable assessed perceptions of health misinformation and disinformation on social media with the question, “How much of the health information that you see on social media do you think is false or misleading?” Responses were dichotomized as “substantial” (“a lot”) versus “less than substantial” (“none,” “a little,” or “some”), consistent with past studies.7,22,25
We tested mechanisms based on the theoretical framework: trust in the health care system, social media use, and education level. Trust in the health care system was measured by asking, “How much do you trust the health care system (for example, hospitals, pharmacies, and other organizations involved in health care)?” Responses were dichotomized as high (“very” and “somewhat”) vs low (“not at all” and “a little”), based on prior literature.32,33 Social media use was categorized as daily vs less than daily (including “never,” “weekly,” “monthly”). Education level was categorized as not having a college degree vs having a college degree or higher.
Control variables included demographic characteristics, health-related factors, and social media utilization. Demographic variables included age (18-49, 50-64, or 65+), sex (male or female), marital status (married/cohabiting, formerly married, or never married), self-reported race and ethnicity (non-Latino White, non-Latino Black, non-Latino Other, or Latino), education level (college degree or higher vs less than a college degree), residence (metropolitan or nonmetropolitan), full-time employment status, and household income perceptions (very/difficult on present income, getting by on present income, and living comfortably on present income). Health-related factors included health insurance status (insured or uninsured), unmet need for medical care (defined as delaying or not receiving medically necessary care), self-rated overall health status (excellent/very good/good or fair/poor), and personal and family history of cancer.
Statistical Analysis
Descriptive statistics were calculated as survey-weighted percentages. Bivariable relationships between the outcome and predictor variables were assessed using cell percentages and design-based Pearson Chi-Square tests. Multivariable logistic regression was conducted to examine the main effect of perceptions of misinformation/disinformation on beliefs about progress in curing cancer. Sensitivity analyses using ordered logit regression assessed whether results varied when using the ordinal version of the outcome variable.
Interaction effects between the primary predictor and secondary predictor variables were calculated to estimate the theorized pathways linking social media misinformation/disinformation, education level, health care system trust, frequency of social media use, and beliefs about cancer treatment progress. Predicted probabilities were derived from interaction results using the margins command in Stata for ease of interpretation. All analyses were conducted with StataNow/MP 18.5 and accounted for survey weights and design using jackknife replicate weights for variance estimation. Statistical significance was set at an alpha level of 0.05. We followed the STROBE guidelines for cross-sectional studies. 34
Ethical Considerations
These publicly available, de-identified data did not require institutional review board approval, as determined by the University of Texas Southwestern Medical Center human research protection program.
Results
Sample Size and Survey Weighted Percentages, HINTS 6, 2022, N = 4246.
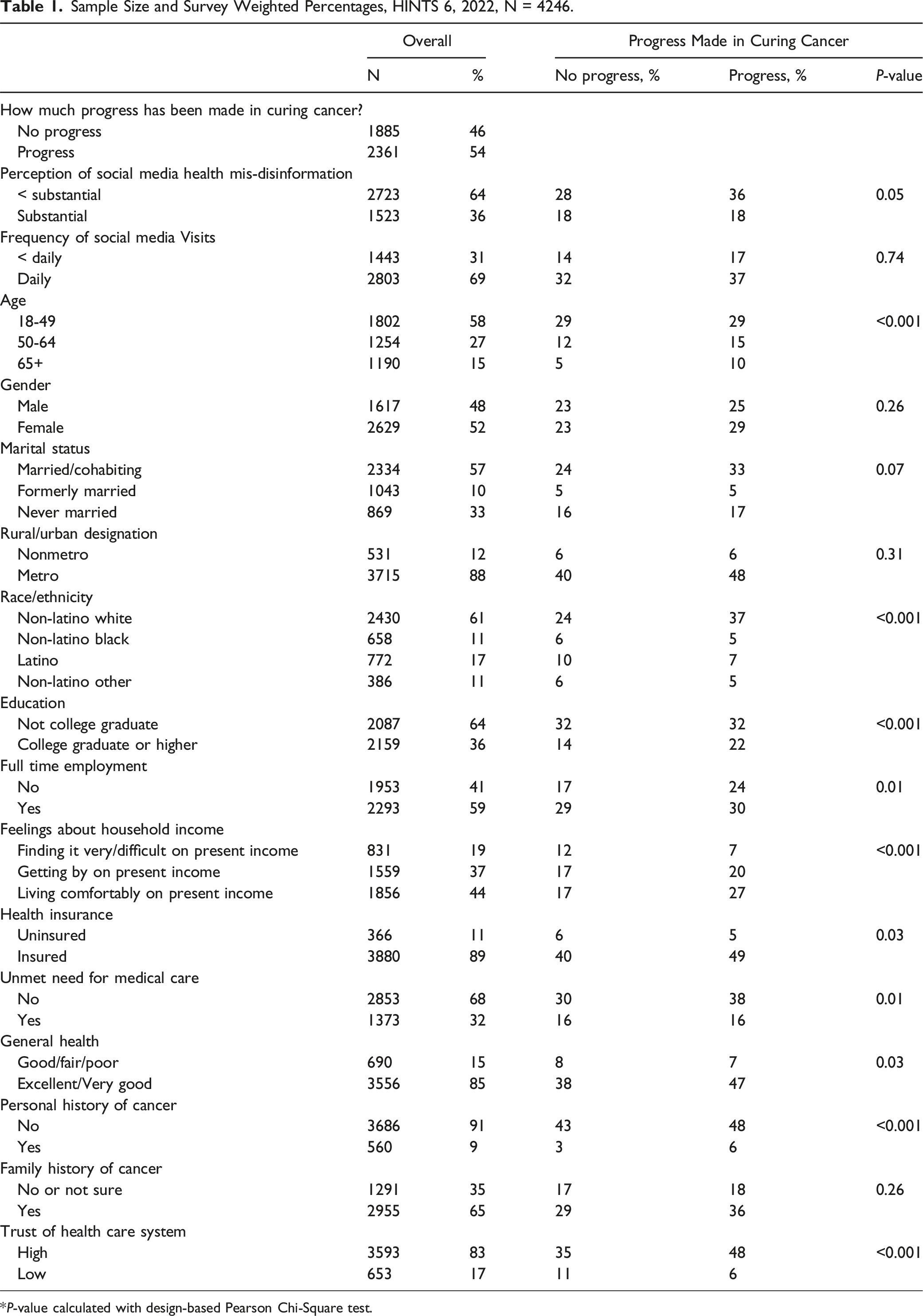
*P-value calculated with design-based Pearson Chi-Square test.
Socially disadvantaged populations are less likely to report perceptions of progress in cancer treatment than socially advantaged populations. Younger respondents (aged 18-49) demonstrate a stronger belief in progress, with 29% expressing this view, in contrast to 15% of those aged 50-64 and 10% of those aged 65 and above. Both males and females show similar perceptions, with 25% of males and 29% of females believing in progress. Married or cohabiting individuals are more likely to believe in progress (33%) compared to formerly married individuals (5%) and those never married (17%). There is a notable difference in belief in progress between respondents in metropolitan (48%) and nonmetropolitan areas (6%). Non-Latino Whites are more inclined to believe in progress (37%) compared to Non-Latino Blacks (5%), Latinos (7%), and Non-Latino Others (5%). Educational attainment influences perceptions, with 32% of individuals without a college degree believing in progress, compared to 22% of those with a college degree or higher. Full-time employment correlates with a higher belief in progress (30%) compared to those not employed full-time (24%). Financial stability also plays a role, with 27% of those living comfortably believing in progress, vs 7% of those struggling financially.
Insurance status significantly impacts belief in progress, with 49% of insured individuals holding this view, compared to 5% of uninsured individuals. Those without unmet medical needs are more likely to believe in progress (38%) compared to those with unmet needs (16%). Good physical health correlates strongly with belief in progress, with 47% of those in excellent or very good health endorsing this view, compared to 7% of those in fair or poor health. Personal and family history of cancer also influenced perceptions. Individuals without a personal history of cancer are more likely to believe in progress (48%) compared to those with a history of cancer (6%). Those with a family history of cancer are more inclined to believe in advancements (36%) compared to those without or unsure of their family history (18%). Trust in the health care system is a significant factor, with 48% of those with high trust in the system believing in progress, compared to 6% of those with low trust.
Multivariable Logistic Regression, HINTS 6, 2022, N = 4246.

The results presented in Appendix Table 1 illustrate the findings from sensitivity analyses using multivariable ordered logit regression to assess the perception of social media health misinformation. The table is divided into two main outcomes: a 3-category outcome and a 5-category outcome. For the 3-category outcome, the coefficient for the perception of substantial health misinformation is −0.27 with a P-value of 0.01, indicating a statistically significant negative association. This means that as the perception of substantial misinformation increases, the likelihood of respondents categorizing their perception as “some & a lot” decreases compared to “almost none & a little” and “don’t know.” Similarly, for the 5-category outcome, the coefficient for substantial misinformation is −0.21 with a P-value of 0.04, also indicating a statistically significant negative association. This implies that higher perceptions of substantial misinformation are associated with a lower likelihood of respondents categorizing their perception as “some” or “a lot” compared to “almost none,” “a little,” and “don’t know.”
Marginal Effects of Belief That Progress has Been Made in Curing Cancer Estimated From Multivariable Logistic Regression for the Interaction Effect Between Perception of Mis/Disinformation and Health care System Trust and Education, HINTS 6, 2022, N = 4246.

In addition to exploring the moderating role of trust in the health care system, we examined how the frequency of social media use interacted with perceptions of health mis/disinformation on beliefs about progress in curing cancer. Among respondents who perceived less than substantial misinformation, those who used social media less than daily had a 62% (95% CI: 56-68%) probability of believing that progress has been made in curing cancer. This probability was slightly lower at 55% (95% CI: 51-58%) for daily social media users with the same perception. On the other hand, respondents who perceived substantial misinformation and used social media less than daily had a 44% (95% CI: 36-52%) probability of believing in progress, whereas daily users with the same perception had a higher probability of 53% (95% CI: 48-58%). These findings demonstrate the statistically significant difference between adults that use social media less frequently and perceive substantial misinformation compared to those who use social media less frequently and perceive less than substantial misinformation.
The interaction between educational level and perceived mis/disinformation demonstrated varied impacts on beliefs about cancer progress. Among non-college graduates, the predicted probability of believing progress has been made in curing cancer was 55% (95% CI: 51-59%) among those who perceived less than substantial misinformation/disinformation. Among non-college graduate social media users who perceived substantial misinformation/disinformation, the probability dropped to 44% (95% CI: 39-50%). For college graduates or individuals with higher levels of education, the predicted probability was 60% (95% CI: 55-65%) when they perceived less than substantial misinformation/disinformation, and it remained relatively stable at 59% (95% CI: 54-65%) when they perceived substantial misinformation/disinformation. These results suggest that college graduates maintain a relatively high belief in progress irrespective of their perception of misinformation/disinformation, whereas non-college graduates show a more pronounced low belief in progress when they perceive substantial misinformation/disinformation.
Discussion
Principal Results
This study examined the relationship between attitudes about progress in curing cancer and social media health misinformation and disinformation. We found that adults perceiving substantial health mis/disinformation on social media were significantly less likely to believe that significant progress has been made in curing cancer. This research makes a unique contribution to the literature by being among the first to specifically examine the relationship between perceptions of health misinformation/disinformation on social media and belief in progress in curing cancer. While previous studies have explored the general impact of misinformation on health attitudes, our study introduces the critical moderating effects of trust and education.5,6 This nuanced approach helps to clarify how these factors influence individual susceptibility to misinformation and shape health beliefs.
The study further delved into the moderating roles of trust in the health care system, frequency of social media use, and educational attainment in the relationship between exposure to health misinformation/disinformation on social media and beliefs about progress in curing cancer. Our findings reveal that high trust in the health care system and higher educational attainment can mitigate the adverse effects of substantial misinformation/disinformation. Notably, higher education levels demonstrate particularly strong resilience against misinformation. The mechanisms through which trust and education impact health beliefs can be multifaceted. High trust in the health care system likely enhances the credibility of information from established medical sources, promoting a more accurate understanding of medical advancements. 19 Trust may lead individuals to seek out reputable sources and adhere to medical advice, reducing the influence of misinformation.21,22 Education, on the other hand, equips individuals with critical thinking skills and the ability to verify sources, fostering a more nuanced understanding of health information. 16 Educated individuals may be more adept at distinguishing credible information from falsehoods, thereby maintaining informed and optimistic beliefs about medical progress despite exposure to misinformation.17,18 Finally, individuals who perceived substantial misinformation and used social media less than daily were significantly less likely to believe that progress has been made in curing cancer compared to their counterparts who perceived less substantial misinformation and also used social media less than daily. This result suggests that less frequent social media users might be more susceptible to the negative effects of misinformation, potentially due to a lower overall engagement with and critical consumption of health-related content on these platforms. Daily users, while exposed to substantial misinformation, might also encounter a greater volume of corrective or authoritative health information, which could mitigate the negative impact of misinformation. Alternatively, it could reflect a desensitization effect, where daily users are less swayed by individual pieces of misinformation due to their higher overall exposure to varied content. 11
Limitations and Future Research Directions
Despite its strengths, including a nationally representative sample and a comprehensive consideration of variables, we acknowledge certain limitations, including the potential for Neyman bias, also known as incidence-prevalence bias. This bias can occur in cross-sectional studies, where the timing of data collection may affect the representation of individuals with varying degrees of exposure to misinformation. For example, individuals with recent exposure to substantial misinformation may be overrepresented, while those whose views have stabilized over time may be underrepresented. This limitation suggests that our findings may not fully capture the dynamic nature of beliefs and misinformation exposure over time. Future longitudinal research is needed to address this concern by tracking changes in beliefs and misinformation exposure across different time points, thereby providing a more comprehensive understanding of the long-term effects of health misinformation. Moreover, the reliance on self-reported data may introduce recall or social desirability biases, and the dichotomization of certain variables may oversimplify complex constructs although we conducted sensitivity analyses for the outcome variable. Finally, the model did not control for other sources of obtaining health information such as print media or television. Future research should conduct longitudinal studies to track changes in beliefs over time, explore the mechanisms through which trust in the health care system mitigates the impact of mis/disinformation, and identify specific aspects of educational curricula that bolster resilience to health misinformation.
Implications for Practice and Policy
Social media health mis- and disinformation may make it more likely that the public does not believe in public health innovations, such as progress being made in curing cancer. Our findings underscore the importance of cultivating trust in health care institutions and promoting education as strategies to counteract the influence of health misinformation on social media. Public health strategies should prioritize transparency and credibility in health communication, offering regular updates on medical advancements, debunking myths, and clarifying misconceptions. 35 This could involve health care systems in local communities providing regular updates about advancements in cancer treatment, debunking common myths, and clarifying misconceptions.6,36 Promoting education is also essential to mitigate the detrimental impacts of health misinformation.16,17 Integrating health literacy into educational curricula and offering accessible and comprehensible health information to the public are key strategies.37,38 Finally, interventions may need to attend to the frequency of social media use with less frequent users potentially more susceptible to social media misinformation.
Conclusion
In conclusion, perception of substantial social media health mis- and disinformation was associated with a lower likelihood of believing progress has been made in curing cancer. Persons that perceived substantial social media health mis-and disinformation and had low trust of the health care system, used social media less frequently, and lacked a college degree were the least likely to believe progress has been made in curing cancer. This study highlights the necessity for a multifaceted approach to counter the influence of health misinformation on social media that includes direct fact-checking and debunking efforts, alongside strategies aimed at enhancing public trust in health care systems and promoting higher education. These findings offer insights for developing tailored interventions to improve public perceptions and foster trust in health care innovations.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Data analysis was performed by JPS. The first draft of the manuscript was written by JPS. All authors contributed to subsequent drafts of the manuscript. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JPS was supported by the National Institute on Minority Health and Health Disparities (NIMHD) at the National Institutes of Health (NIH) under award number R01MD018727. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIMHD. The funders had no role in study design, data analysis, decision to publish, or preparation of the manuscript.
Ethical Statement
Data Availability Statement
Appendix
Sensitivity Analyses. Multivariable Ordered Logit Regression. a3 category outcome: “almost none & a little” = 0, “don’t know” = 1, “some & a lot” = 2. b5 category outcome: “almost none” = 0, “a little” = 1, “don’t know” = 2, “some” = 3, “a lot” = 4.
3 Category Outcome
a
5 Category Outcome
b
Coefficient
P-value
Coefficient
P-value
Perception of social media health mis-disinformation
<substantial
Substantial
−0.27
0.01
−0.21
0.04