
Abstract
Background
Circulating tumor markers with satisfactory sensitivity and specificity play crucial roles in cancer diagnosis and therapy. This prospective study aimed to evaluate the potential of circulating lncRNAs as biomarkers for hepatocellular carcinoma (HCC).
Methods
A total of 74 patients with HCC and 94 healthy controls were enrolled. The expression levels of candidate genes in serum were detected by qRT-PCR. Receiver operating characteristic (ROC) curve analysis and logistic regression were employed to investigate the diagnostic capacity of lncRNAs. The analysis of 3-year overall survival (OS) was conducted using the Kaplan-Meier method and log-rank test.
Results
Of the 9 candidate genes, 6 lncRNAs could be stably detected in serum. The expression levels of circulating MALAT1 and HOTTIP in HCC patients were significantly higher than those in controls (P < 0.001). ROC analysis showed that MALAT1 and HOTTIP were more effective than alpha-fetoprotein (AFP) (P < 0.010) in the diagnosis of HCC, with AUCs of 0.896 and 0.899, respectively. Additionally, a panel consisting of MALAT1, HOTTIP, and AFP was constructed to obtain an AUC of 0.968 with a sensitivity of 87.8% and specificity of 94.7% in HCC diagnosis. Moreover, the upregulation of MALAT1 was not only related to multiple tumor lesions, HCV infection, AST level, and AFP level, but also suggested shorter OS. A high expression level of HOTTIP was associated with metastasis.
Conclusion
Serum MALAT1 and HOTTIP play indicative roles as non-invasive biomarkers for HCC.
Introduction
Hepatocellular carcinoma (HCC) is one of the most fatal malignant tumors, ranking fifth in incidence and third in tumor-related deaths worldwide. The annual new cases of and deaths due to HCC in China account for approximately 51% of the world total. 1 Due to the insidious progression and insufficient typical early clinical symptoms of primary hepatic cancer, most patients lose the opportunity for radical treatment when they seek medical consultation, resulting in a 5-year survival rate of less than 20%. 2 Therefore, improving the screening and diagnosis of HCC plays a particularly important role in improving patient prognosis. Alpha-fetoprotein (AFP), a serum tumor marker for HCC, has been widely used clinically. However, it is still challenging to diagnose HCC at an early stage with a sensitivity limited to 65% and of <40% for preclinical prediction. 3 PIVKA-II, an immature form of prothrombin, has recently been proposed as an effective serum HCC marker. However, the level of PIVKA-II could be influenced by various factors, such as vitamin K deficiency, coagulation disorders, and liver diseases. 4 Therefore, finding novel biomarkers with higher specificity and sensitivity is necessary for HCC screening and diagnosis.
Long noncoding RNAs (lncRNAs) are a group of nucleic acid sequences with lengths of more than 200 nucleotides and no protein coding ability. 5 Recently, an increasing number of lncRNAs have been examined and identified, and some of them have been reported to play critical roles in modulating cancer epigenetics and regulating important biological processes.6-8 Previous studies have shown that several lncRNAs in HCC tissues have significantly higher expression levels than those in adjacent liver tissues.9-11 In addition, lncRNAs have been confirmed to have satisfactory stability in plasma. 12 Hence, finding appropriate lncRNAs in blood circulation to serve as markers represents a promising clinical research direction.
Although circulating lncRNAs have been reported as biomarkers for HCC, different researchers yielded inconsistent results. Therefore, more experiments will help promote the progress in this field. We conducted the present study to identify appropriate lncRNAs as circulating HCC markers. Furthermore, their diagnostic efficacy and predictive value as noninvasive markers for HCC were also evaluated.
Materials and Methods
Patients
A total of 168 patients were enrolled in this study, namely, 74 consecutive patients diagnose with HCC at our institution from October 2018 to August 2019, and 94 healthy controls. All patients in the HCC group were confirmed by pathological examination or clinical diagnosis according to the World Health Organization (WHO) criteria, and patients who had received chemotherapy or radiotherapy were excluded. Data were collected prospectively on all patients from the medical records and personal interviews, including demographics, tumor features, laboratory data, and follow-up. Tumor features included number, size and vascular invasion. Laboratory data included levels of albumin (ALB), alanine transaminase (ALT), aspartic transaminase (AST), total bilirubin (TBIL), prothrombin time (PT), hepatitis B surface antigen (HBsAg), anti-hepatitis C virus (anti-HCV), and AFP. Patients from HCC group received ablation or chemoembolization treatment, which were chosen based on the Barcelona Clinic Liver Cancer (BCLC) approach. The follow-up time in HCC group ranged from 4 to 36 months (median 16 months). The research protocol was approved by the Ethics Committee of The First Hospital of China Medical University (2018-215-2). Written informed consent was obtained from every participant and all patient details have been de-identified. The reporting of this study conforms to REMARK guidelines. 13
Plasma Samples
Whole-blood samples obtained with ethylene diamine tetraacetic acid (EDTA) anticoagulation were centrifuged at 3000 r/min for 10 min at 4°C to separate the blood cells. The supernatants were collected and centrifuged at 12,000 r/min for 10 min at 4°C to completely remove cellular components. Then, plasma was collected and stored at −80°C for further use.
RNA Extraction
Total RNA was extracted from 400 μL of cell-free plasma using a mirVana PARIS Kit (Ambion, Austin, TX, USA) and eluted with 100 μL of preheated (95°C) elution solution according to the manufacturer’s protocol as described previously. 14 RNA samples were stored at −80°C until further analysis.
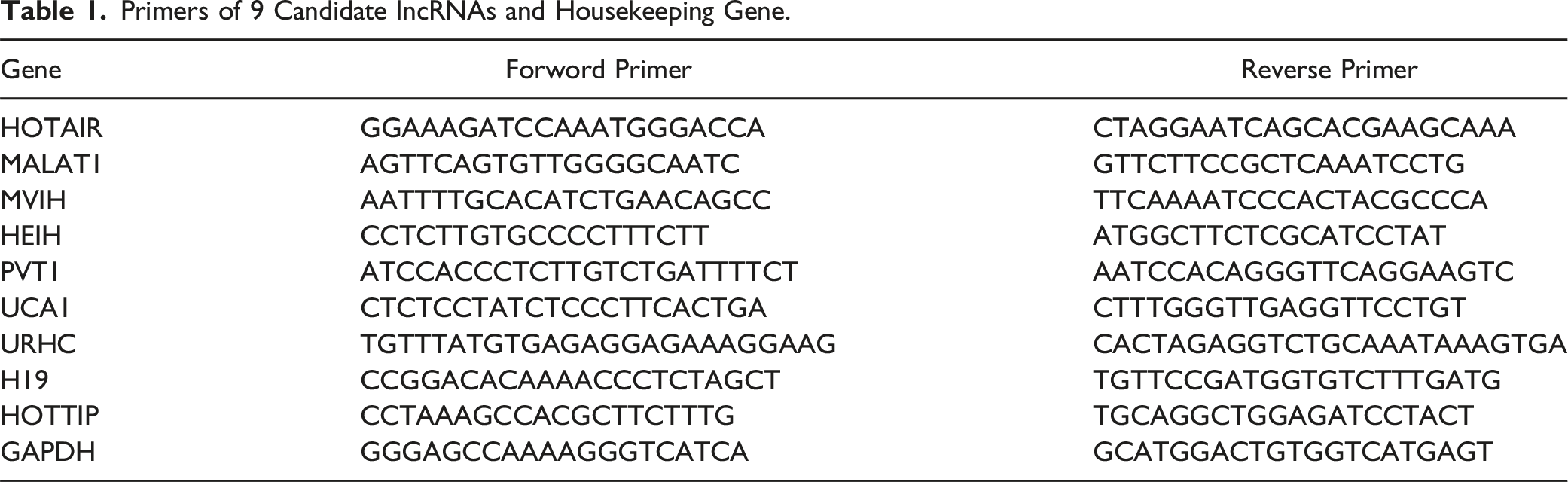
Quantitative Real-Time PCR (qRT‒PCR)
Primers of 9 Candidate lncRNAs and Housekeeping Gene.
Public Data Collection
Public databases were used to compare and validate the expression differences of candidate genes in hepatocellular carcinoma and normal tissue samples. Transcriptome expression data of HCC patients were obtained from the TCGA-LIHC (https://portal.gdc.cancer.gov/) database. To compensate the deficiency of normal samples, normal liver tissue samples in the GTEx database (https://xenabrowser.net/datapages/) were used. In addition, the clinical as well as prognostic information was obtained from the same website.
Statistical Analysis
Continuous variables are expressed as the means ± SDs, and categorical variables are expressed as a number. The differences were compared using t test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. If lncRNAs were found to be significant, receiver operating characteristic (ROC) curve analysis was conducted to obtain the cutoff value, sensitivity and specificity. Combined ROC analysis was conducted on the basis of a logistic regression model. Pearson’s correlation analysis was used to reveal the correlation between the serum lncRNA levels and biochemical parameters. Three-year overall survival (OS) was calculated using the Kaplan-Meier method, and the differences were compared using the log-rank test. The sample size justification of validation set was performed using an online simple size calculator (https://www.trialdesign.org/) with alpha value of 0.05 and power of 90%. The expression levels from TCGA and GTEx datasets between two groups were calculated by the Wilcoxon’s test using R software (https://www.r-project.org/). Statistical analysis was performed using SPSS Statistics 26.0 (IBM SPSS, Shanghai, China) and GraphPad Prism 9.0 (GraphPad Software, LLC., Boston, MA, USA). A two-sided P value of <0.050 was considered statistically significant.
Results
Patient Characteristics
Baseline Characteristics of Patients in the HCC Group and the Control Group.

aIndicates statistically significant, P < 0.050.
Screening of lncRNAs Related to HCC in the Training Set
Baseline Characteristics of the Training and Validation Sets.


Heatmap of lncRNAs expression levels in plasma samples from 20 HCC patients and 20 healthy controls in the training set.
The 2−ΔCt Values of 6 Stably Detected lncRNAs in Serum Samples.

aIndicates statistical significance, P < 0.050.

Relative expression levels of 6 stably detected lncRNAs in serum. The expression levels of MALAT1 (C) and HOTTIP (E) were significantly upregulated in HCC patients compared with healthy controls. There was no significant difference in the expression levels of the other 4 lncRNAs (A, B, D and F). Data on the relative expression of serum lncRNAs are presented after log10 transformation. *** indicates P < 0.001, **** indicates P < 0.0001.
Confirmation of the Selected lncRNAs by the Validation Set
The sample size justification for validation set was based on results from training set. The recommended minimum sample size for MALAT1 and HOTTIP were 73 and 69, respectively. The sample size of the validation set in this study was considered sufficient to reflect the differences in the selected genes. To validate the accuracy and specificity of MALAT1 and HOTTIP as HCC biomarkers, we next examined the expression level of two selected lncRNAs in the validation set composed of the 128 remaining samples. As shown in Figure 3, the relative expression levels of MALAT1 and HOTTIP in the plasma of HCC patients were significantly higher than those in healthy controls, and the results were consistent with those in the training set. Finally, we merged the total samples for further analysis. Comparison of the selected lncRNA expression levels in the validation set. The serum expression levels of MALAT1 (A) and HOTTIP (B) in the HCC group were significantly higher than those in the control group. Data on the relative expression levels of serum lncRNAs are presented after log10 transformation. **** indicates P < 0.0001.
Relationship Between the Expression Levels of Plasma lncRNAs and Clinical Variables
Clinicopathological Relevance Analysis of MALAT1 and HOTTIP Expression in HCC Patients.

aIndicates statistically significant, P < 0.050.

Correlation between serum MALAT1 and biochemical parameters in HCC patients. The expression level of MALAT1 in plasma was positively correlated with the levels of AFP (A) and AST (D). No significant relationships were found between MALAT1 and other biochemical variables (B, C, E and F).

Relevance analysis of plasma HOTTIP with biochemical parameters in HCC patients. No significant relationships were found between HOTTIP and biochemical variables, including AFP (A), ALB (B), ALT (C), AST (D), PT (E), and TBIL (F).
Diagnostic Value of MALAT1 and HOTTIP in HCC Detection
ROC curve analysis was conducted to evaluate the efficacy of the serum lncRNAs MALAT1 and HOTTIP as diagnostic indicators for HCC detection. As shown in Figure 6, when HCC patients were tested against healthy controls, the AUC for MALAT1 was 0.896 (95% CI: 0.848-0.945), with a sensitivity of 75.7% and specificity of 92.6% at the cutoff value of 0.0449. The AUC of plasma HOTTIP for distinguishing HCC patients from healthy controls was 0.899 (95% CI: 0.854-0.944) at the cutoff value of 0.0191 with optimal sensitivity and specificity values of 94.6% and 73.4%, respectively. AFP, as a commonly used biomarker for HCC screening, was also evaluated as the control. The AUC of AFP was 0.763 (95% CI: 0.685-0.842), with a sensitivity and specificity of 63.5% and 88.3%, respectively. The diagnostic efficacy comparison revealed that MALAT1 and HOTTIP were more effective than AFP (P < 0.010). Moreover, the combination of each lncRNA with AFP obtained a higher predictive power than AFP alone, and the merged AUC was 0.924 (95% CI: 0.881-0.967) for MALAT1 with AFP (Y = −2.403 + 22.256× MALAT1 + 0.02 × AFP) and 0.942 (95% CI: 0.909-0.976) for HOTTIP with AFP (Y = −2.37 + 17.333× HOTTIP +0.02 × AFP). In addition, the merged AUC of MALAT1 and HOTTIP increased to 0.955 (95% CI: 0.928-0.981) after analysis with the following formula: Y = −2.909 + 29.473× MALAT1 + 12.629 × HOTTIP, indicating a significantly better diagnostic efficiency than AFP alone (P < 0.001). The highest accuracy for HCC discrimination was obtained with a diagnostic panel consisting of serum MALAT1, HOTTIP, and AFP, yielding an AUC of 0.968 (95% CI: 0.945-0.991) with a sensitivity of 87.8% and specificity of 94.7% (Y = −3.6 + 22.275× MALAT1 + 13.941 × HOTTIP +0.022 × AFP). However, the panel including MALAT1, HOTTIP, and AFP did not show a significant difference compared with the combination of MALAT1 and HOTTIP (P = 0.142). ROC analysis of single lncRNAs and merged factors for diagnosing HCC. (A) ROC analysis of MALAT1, HOTTIP, and AFP for predicting HCC (MALAT1 vs HOTTIP P = 0.934, MALAT1 vs AFP P = 0.002, HOTTIP vs AFP P = 0.003). (B) Diagnostic efficacy of the combinations of serum lncRNAs and AFP to discriminate HCC patients from healthy controls. The diagnostic panel was established with serum MALAT1, HOTTIP, and AFP (MALAT1&HOTTIP vs MALAT1&AFP P = 0.144, MALAT1&HOTTIP vs HOTTIP&AFP P = 0.407, MALAT1&AFP vs HOTTIP&AFP P = 0.456 Panel vs MALAT1&AFP P = 0.016, Panel vs HOTTIP&AFP P = 0.029, Panel vs MALAT1&HOTTIP P = 0.142).
Prognostic Implication of Plasma MALAT1 and HOTTIP Expression in Overall Survival
OS was defined as the time from diagnosis until death or the last follow-up time, which largely represents prognosis. To investigate the predictive value of serum MALAT1 and HOTTIP, a 3-year OS analysis was conducted on 74 HCC patients by using Kaplan-Meier analysis and log-rank tests. High- and low-expression groups were divided according to the median expression levels of lncRNAs in plasma. Patients with HCC in the high serum MALAT1 expression group had significantly shorter OS (Figure 7A, P = 0.002). No significant difference in prognosis between patients with high and low expression levels of HOTTIP was observed (Figure 7B, P = 0.284). Cumulative survival rate according to different serum lncRNA expression levels in 74 HCC patients. (A) High serum MALAT1 expression levels result in shorter patient survival. (B) No statistically significant difference was found between the high and low serum HOTTIP expression groups.
Validation of the Predictive Role of MALAT1 and HOTTIP in Hepatocellular Carcinoma
To further explore the diagnostic and prognostic effects of MALAT1 and HOTTIP, the mRNA expression of tumor tissues from patients with hepatocellular carcinoma in TCGA (n = 152) and normal liver tissues in the GTEx dataset (n = 152) were collected as external validation. The expression levels of MALAT1 and HOTTIP were significantly higher in hepatocellular carcinoma tissues than in normal liver tissues (Figure 8A–B). Consistently, patients with hepatocellular carcinoma exhibiting high expression of MATLAT1 had significantly shorter OS, and patients exhibiting high expression of HOTTIP also had a trend towards poor prognosis, which further suggested the reliability of these two lncRNAs as screening and prognostic predictors (Figure 8C–D). Validation of the predictive role of MALAT1 and HOTTIP in TCGA-LIHC cohorts. (A-B) Boxplot shows the expression difference of MALAT1 and HOTTIP between HCC and adjacent normal liver tissues. (C) High expression of MALAT1 is correlated with shorter OS in HCC patients. (D) Patients with high HOTTIP expression tend to have a shorter OS.
Discussion
HCC is a common, life-threatening clinical disease with high morbidity and mortality. 22 Currently, AFP and PIVKA-II are biomarkers for HCC screening and diagnosis. However, the sensitivity and specificity are not perfect in clinic applications, particularly for early-stage HCC, resulting in only 20% of HCC patients receiving curative treatment through surgical resection, ablation treatment, or liver transplantation. 3 Therefore, it is important to find promising biomarkers for HCC to improve patient prognosis. Several lncRNAs have been reported to be highly expressed in HCC tissue, and some of them can be detected in serum. 23 However, the results from different studies are not exactly consistent. For example, significantly high levels of serum HULC, MALAT1, UCA1 and H19 in HCC patients with a comparison of healthy controls were reported by several literatures.24-27 While Li et al. reported the relative expression levels of 8 HCC-associated lncRNAs, the authors noted that high expression level of HULC was observed, low expression level of UCA1 in HCC patients was identified and no significance was demonstrated for MALAT1 in HCC patients in contrast to controls. 28 Luo et al also reported the expression level of H19 with a result of no difference between HCC and controls. 29 Therefore, identifying appropriate lncRNAs and employing them to screen and diagnose HCC still need further investigation. The present study revealed that the lncRNAs MALAT1 and HOTTIP were significantly over-expressed in the serum of HCC patients, and both of them showed a higher diagnostic value than AFP. Additionally, the combination of MALAT1, HOTTIP and AFP demonstrated the best predictive power. At present, the detection kit based on 7 microRNA combinations has been used for early diagnosis of HCC. 30 MALAT1 and HOTTIP, which are also non-coding RNAs, are expected to constitute a lncRNA panel for HCC diagnosis and prognosis in the future.
This study compared the serum lncRNA expression between patients with HCC and healthy controls, resulting in the identification of two lncRNAs as candidate biomarkers for HCC diagnosis. As a common clinical biomarker in HCC diagnosis, AFP was used as the control. The AUC of AFP in our study was similar to those in previous studies.29,31,32 Importantly, both MALAT1 and HOTTIP showed increased discriminatory power for distinguishing HCC patients from non-HCC patients, with AUCs of 0.896 and 0.899, respectively (MALAT1 vs AFP P = 0.002, HOTTIP vs AFP P = 0.003). The results indicate that MALAT1 and HOTTIP are more effective than AFP with satisfactory potential as novel biomarkers for HCC diagnosis. Moreover, we further explored the combined application of MALAT1, HOTTIP and AFP to improve the diagnostic efficacy of HCC. The panel combining MALAT1, HOTTIP and AFP achieved the best discrimination power (AUC: 0.968, 95% CI: 0.945-0.991) for HCC. Therefore, combining serum lncRNAs, including MALAT1 and HOTTIP, with AFP is of great significance for improving the identification of HCC. It is important to point out that although the AUC of the panel is larger than the AUC of the combination of MALAT1 and HOTTIP, there is no significant difference between the two formulas (Panel vs MALAT1&HOTTIP P = 0.142). After analyzing the regression coefficients of the three markers in the formula of the panel (Y = −3.6 + 22.275× MALAT1 + 13.941 × HOTTIP +0.022 × AFP), the coefficient of AFP was lower than the two lncRNAs by a large margin, indicating its limited role in the diagnosis of HCC. The regression coefficient is a parameter that represents the influence magnitude of the independent variable X on the dependent variable Y. Thus, despite the addition of the marker AFP, there was no statistical difference between the panel and the combination of MALAT1 and HOTTIP.
MALAT1, also known as metastasis-associated lung adenocarcinoma transcript 1, has a length of more than 8000 nt, is located on chromosome 11q13 and is highly conserved in multiple species. 33 Tritaphy et al showed that MALAT1 can affect the phosphorylation of the serine/arginine (SR) protein at the cellular level, thereby regulating the splicing process of pre-mRNA and playing an important role in a variety of tumor biological behaviors. 34 Here, we revealed that serum MALAT1 was significantly upregulated in HCC patients, which was consistent with previous studies.14,25 Moreover, we investigated the correlation between circulating MALAT1 and clinicopathological features of HCC patients. The high level of MALAT1 expression in plasma was positively correlated with multiple tumors and hepatitis C virus infection. Moreover, a significant association between serum MALAT1 and AFP as well as AST was observed in patients with HCC. MALAT1, one of the first lncRNAs identified, has been reported to act as an important metastasis-relevant oncogene. 35 Meta-analysis and multiomics analyses have demonstrated the upregulation of MALAT1 in HCC tissues and indicated that the overexpression of MALAT1 is significantly related to tumor number and AFP.25,36,37 However, there are few studies on the expression of MALAT1 in the plasma of patients with HCC, and the conclusions are inconsistent. Konishi et al confirmed that plasma MALAT1 levels were progressively and significantly elevated in hepatic disease as well as HCC patients and were associated with liver damage but not related to AFP. The researchers concluded that plasma MALAT1 might be derived from not only HCC tissues but also damaged hepatocytes due to hepatitis viral infection, steatosis, and other hepatic diseases. 14 Toraih et al reported that serum MALAT1 overexpression in HCV-related HCC had an AUC of 0.79 to distinguish cancer patients from healthy controls. Correlation analysis showed a positive correlation of MALAT1 with TBIL and AST. 25 Huang et al. demonstrated a significantly higher level of MALAT1 in HCC patients than in healthy controls, whereas there was no association between serum MALAT1 levels and clinicopathological characteristics. 24 Our study not only demonstrated the upregulation of serum MALAT1 in HCC patients but also confirmed the association between serum MALAT1 and clinicopathological features, including tumor number, HCV infection, AST level, and AFP level, highlighting the clinical significance of MALAT1 as a biomarker. MALAT1 could enhance cellular proliferation and inhibit apoptosis via modulating PI3K/AKT and JAK/STAT signaling pathways, upregulating LTBP3 gene, and inhibiting caspase3/7 activity. 25 The putative mechanism for MALAT1 up-regulation could be the transcriptional activation of MALAT1 via the TF specificity protein Sp1/3 in HCC cells. Zhou et al reported that MALAT1 could promote HCC metastasis through the peripheral vascular infiltration by inhibiting the level of miRNA-613, which may be the reason for a significant association of MALAT1 with multi-tumor number and elevation in AFP reported by several studies.11,36 Hepatitis C virus infection not only causes liver cell damage and elevated transaminase levels, but also is related to the occurrence of HCC. Toraih et al reported serum MALAT1 profile was positively correlated with hepatic failure scores and confirmed MALAT1 oncogenic role in HCV-induced HCC in subsequent meta-analysis. 25 Assal et al. reported MALAT1 could target CD-155/TIGIT and PD-1/PD-L1 axes, facilitating HCV-related HCC development by evading immune surveillance. 38 Shao et al indicated that MALAT1 was most likely involved in regulating HCV-related HCC processes by acting as ceRNA regulation in the hsa-miR-193a-3p/BUB1 axis and confirmed in further in vitro experiment. 39 Furthermore, the overall survival analysis with the Kaplan-Meier method showed that patients with HCC in the high serum lncRNA MALAT1 expression group had significantly shorter OS. Although the high expression levels of MALAT1 in HCC tissues have been demonstrated to be associated with poor prognosis, to the best of our knowledge, the current study is the first to report the potential of serum MALAT1 for predicting the prognosis of patients with HCC.
HOTTIP (HOXA transcript at the distal tip), known as HOXA distal tip, is a long noncoding RNA located at the 5′ end of the HOXA gene. HOTTIP can directly control the expression of the HOXA gene by interacting with the WDR5/MLL complex and is associated with metastasis formation and poor patient survival in HCC. 40 Previous studies have shown that HOTTIP, an oncogene, is highly expressed in liver cancer tissues, 20 and several studies have shown that HOTTIP is abnormally expressed in the serum of patients with various tumors, including pancreatic, esophageal, gastric, and colorectal cancer.41-44 However, the serum expression of HOTTIP in HCC is rarely reported. In the present study, we identified that the serum expression of HOTTIP in HCC patients was significantly higher than that in healthy controls and had a better diagnostic efficacy than AFP. Clinicopathological feature analysis showed that abnormal expression of HOTTIP was positively associated with distant metastasis in HCC patients, which was consistent with previous studies.20,40 Tsang et al concluded that HOTTIP could be a novel oncogenic lncRNA, which negatively regulated by miR-125b and might cis-regulate the expression of its neighboring genes residing in the HOXA cluster in HCC and thereby contribute to hepatocarcinogenesis. In addition, knock-down of HOTTIP also inhibited migratory ability of HCC cells and significantly abrogated lung metastasis in orthotopic implantation model in nude mice. This may be a potential mechanism for the association between lncRNA HOTTIP expression and clinical variables. 20 The high expression level of HOTTIP in HCC tissues has been also reported as a candidate biomarker for predicting poor prognosis in HCC patients.40,45 However, we did not observe any associations between serum HOTTIP and biochemical parameters or overall survival. The possible reasons may be the lower expression level of HOTTIP in serum than that in HCC tissues and the short follow-up period in the present study.
There are several limitations to the current study. First, the experiment contains a relatively limited sample size and is a single-center study. The sample size of this study is composed of consecutively collected cases, rather than sample size calculation. However, we conducted a sample size justification in the validation set, using the results of the training set. On the other hand, HCC is a heterogeneous disease, and the expression level of the same gene may be variable in different populations. Thus, large-scale and multicenter studies are recommended to evaluate the diagnostic and prognostic potential of lncRNAs in further investigations. Second, apart from AFP, PIVKA-II is also a common clinical biomarker for HCC. The comparison of the diagnostic value of lncRNAs with PIVKA-II warrants further research. Third, no HCC tissue or adjacent noncancerous liver tissue samples were obtained. A comprehensive transcriptome analysis of tissue and serum from HCC patients showed a correlation in ncRNAs between serum and tissue samples, suggesting that noncoding RNA export from tumors. 46 Although the majority of studies have reported that MALAT111,34,47-49 and HOTTIP20,40,45,50,51 are highly expressed in HCC tissues and validated by public databases, the expression levels of the target genes in tissues were not verified in the present study. In addition, since the GAPDH expression level is usually not affected under experimental or physiological conditions, 52 GAPDH is widely used as an internal control in numerous similar studies. 53 However, it is worth noting that there is no “one-size-fits-all” gene that can be used for the normalization of gene expression data. Therefore, some scholars proposed that gene expression analysis should be related to several housekeepers in parallel. 54 Finally, we paid more attention to lncRNAs acting as novel biomarkers of HCC in this study, and in vivo and in vitro experiments are recommended to explore the functional role of MALAT1 and HOTTIP in HCC development in the future.
Conclusion
In summary, we identified that the serum lncRNAs MALAT1 and HOTTIP were significantly highly expressed in patients with HCC and exhibited a better diagnostic value for HCC than the traditional biomarker AFP. High levels of lncRNA expression were associated with clinical features and poor prognosis of HCC patients, showing potential as noninvasive biomarkers for the diagnosis and prognosis of HCC. Additionally, the combination of MALAT1, HOTTIP and AFP could provide a better diagnostic accuracy, and MALAT1 and HOTTIP play a major role in the diagnostic panel.
Footnotes
Acknowledgments
Authors’ Contributions
HB performed the experiments and drafted the manuscript. YTJ and NW analyzed and interpreted the data. HYS conceived and designed the project. XJH revised the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Funds for Science and Technology Innovation of Shenyang (Grant no. F15-199-1-43), and the National Natural Science Foundation of China (Grant no. 81901846).
Ethical Statement
Data Availability Statement
The datasets generated and/or analyzed during this current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author upon reasonable request.