
Abstract
Skin cancer comprises one-third of all diagnosed cancer cases and remains a major health concern. Genetic and environmental parameters serve as the two main risk factors associated with the development of skin cancer, with ultraviolet radiation being the most common environmental risk factor. Studies have also found fair complexion, arsenic toxicity, indoor tanning, and family history among the prevailing causes of skin cancer. Prevention and early diagnosis play a crucial role in reducing the frequency and ensuring effective management of skin cancer. Recent studies have focused on exploring minimally invasive or non-invasive diagnostic technologies along with artificial intelligence to facilitate rapid and accurate diagnosis. The treatment of skin cancer ranges from traditional surgical excision to various advanced methods such as phototherapy, radiotherapy, immunotherapy, targeted therapy, and combination therapy. Recent studies have focused on immunotherapy, with the introduction of new checkpoint inhibitors and personalized immunotherapy enhancing treatment efficacy. Advancements in multi-omics, nanotechnology, and artificial intelligence have further deepened the understanding of the mechanisms underlying tumoral growth and their interaction with therapeutic effects, which has paved the way for precision oncology. This review aims to highlight the recent advancements in the understanding and management of skin cancer, and provide an overview of existing and emerging diagnostic, prognostic, and therapeutic modalities, while highlighting areas that require further research to bridge the existing knowledge gaps.
Keywords
Introduction
Cancer has been one of the leading causes of mortality for the last two decades. It can be either benign or malignant, depending upon the seriousness of the infection and the ongoing stage. 1 According to the studies of World Health Organization, skin cancer makes a total of one third of all the diagnosed cases globally, with its incidence continuously increasing. 2 The prevalence of various types of skin cancer is linked with several factors. Among the risk factors of skin cancer, age and sex are the main contributing factors. In combination, these two risk factors determine the occurrence of cancer in a population. In addition to this, skin cancer is found to be more frequent in white community than others. Prevention holds a greater importance for combating skin cancer, having both primary and secondary prevention options present, along with tertiary prevention strategies. 3 Various diagnostic and treatment methods have been described in the following manuscript, ranging from traditional to advanced ones. The type of treatment employed depends on several factors including stage and type of skin cancer, the area of tumor, and patient dependent factors such as age, comorbidities, and treatment preferences. Advanced treatment options such as immunotherapy and targeted therapy offer more promising results in management and treatment of skin cancer.
Types
The type of skin cancer is dependent upon the initial point of cancer. Skin cancer is categorized into cutaneous melanoma and non-melanoma skin cancer (NMSC). 4 NMSC includes the cancers that develop from the epithelial cells of the skin but not include melanocytes. NMSC includes basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) or cutaneous squamous cell carcinoma (CSCC). Among these three types, BCC is the most common skin cancer, globally forming almost 75% of all skin cancers. 5 It largely affects light skinned population of the world. 6 BCC is a basaloid differentiated, gradually developing, harmful, and locally invasive epithelium tumor. Without a prior cancerous injury, it originates from the stem cells within the hair follicle and/or the interfollicular dermis. 7 Various stem cell divisions may be attacked and eventually give rise to BCC, according on the carcinogenic substance engaged. 5 BCC has extremely low rates of dissemination and death. But BCC can cause serious complications because of its disruptive development. 8 It can also induce localized invasion. After receiving inadequate or no treatment at all, the BCC may lead to the point where an interdisciplinary treatment plan is required after several years.
SCC accounts for the second greatest number of cutaneous malignancy, and the occurrence of this type of cancer is also on rise. 9 20% of cutaneous tumors and over 75% of all skin cancer-related deaths—aside from melanoma—are caused by CSCC. The advancing years of people and increased emphasis on skin cancer monitoring are the key reasons for its ongoing increase in occurrence. 10 The incidence of CSCC has been risen from 50% to 300% in the last three decades and it is estimated that by 2030, the occurrence of SCC will become twice particularly in European countries than the current level. 11 The unregulated growth of abnormal epidermal keratinocytes is the source of CSCC, which is most likely the outcome of a protracted intraepidermal dysplasia process. 12 The growth of tumors is recognized to occur over time, with multiple histologically and clinically defined phases during its tumor progression, ranging from actinic keratosis to invasive SCC or melanoma. 13
Melanoma accounts for the most dangerous type of skin cancer and although it represents only 1% of skin cancer, it accounts for 80% of causalities resulting from skin cancer.2,14 The incidence of melanoma is higher in white populations due to certain risk factors including long time exposure to ultraviolet (UV) radiations of sun for tanning and tanning facilities combined with genetic factors such as light skin having less melanoma, light hair and some other factors such as large number of moles, family history and age. The frequency of cases of melanoma is 25 new cases per 100 000 individuals in Europe, 30 cases per 100 000 in USA, and 60 cases per 100 000 cases in Australia and New Zealand. 15 With 106 000 projected new cases in 2021, or 5.6% of all cancer diagnoses, melanoma is the fifth most common cancer diagnosis in the US, excluding nonmelanoma skin cancers, according to the most recent SEER data. 14 Melanoma is the malignancy of cells that are responsible for producing melanin pigment. These cells are in the basal layer of epidermis, and they develop from group of embryonic cells i.e., neural crest. Hence, they demonstrate a variety of variables and signaling compounds that facilitate movement and metastasis following malignant transformation. One of the cytological characteristics of malignant melanoma is the presence of visible nucleoli and an improperly wide nuclear membrane. 16
Methods
A comprehensive literature search was carried out using the PubMed, Scopus, Web of Science, and Google Scholar databases for relevant published studies up to January’2024, with the major focus towards studies published within past 5 years. The search terms used for the literature research include “melanoma”, “melanoma diagnosis,” “non-invasive diagnostic techniques” “biopsy”, “imaging techniques,” “diagnostic biomarkers”, “artificial intelligence”, “hybrid models”, “surgical treatment”, “immunotherapy”, “radiotherapy”, “checkpoint inhibitors”, “melanoma prevention”, “primary prevention”, “secondary prevention”, “tertiary prevention”, “melanoma risk factors” “targeted therapies,” “BRAF inhibitors,” “vemurafenib,” “dabrafenib,” “MEK inhibitors,” “oncolytic virus therapy,” “adoptive cell therapy”, “radiotherapy”, “combination therapy”, “Next-generation sequencing”, “chemotherapy”, “nanotechnology” and “precision oncology”. The quality of the selected articles was thoroughly assessed by multiple reviewers independently. The publications were refined by reviewing abstracts and full texts and relevant data was extracted. The references of the selected studies were also examined to figure out any additional relevant articles that might have been missed in the initial search. The examined articles included research papers, clinical trials, literature reviews and systematic reviews containing information about prevention, diagnosis and therapy of melanoma in English language only. Articles covering invasive diagnostic methods were excluded. Disagreements among reviewers were resolved through consensus discussions.
Causative Agents/Risk Factors
The risk factors of skin cancer are several including environmental and genetic. It has the chances to occur by the complex interaction between certain environmental factors (extrinsic) and person’s genotype and phenotype (intrinsic factors). 17 The common risk factors among these for the three types are exposure of UV radiation, light skin (Fitzpatrick I & II), increasing age i.e., >60 years, extended immunosuppression, individual or family background of the disease, and Geno dermatoses.5,18
Environmental and Extrinsic Factors
UV Radiations
UV radiations are one of the main extrinsic risk factors for all types of skin cancer, and they particularly affect areas that are more frequently exposed to the sun such as head and neck, contributing almost 80% of the reported cases. However, about one fourth of the cases are reported in anatomical parts of the body that are not frequently directly exposed to the sun, and it highlights that discontinuous exposure to sun light whether it is intense or for a longer period of time also contributes towards the formation of tumor. 19
DNA photosensitive compounds, primarily thymidine-dimers, are known to be produced by UV light. If nucleotide excision repair (NER) is not used to repair these photoproducts, DNA replication errors, resulting alterations in cell-mediated communication molecules, and ultimately carcinogenesis, can occur. Individuals who have xeroderma pigmentosum, a genetic NER defect, are at a 20 000-fold higher risk of developing skin cancer. 20 The genotoxicity of UVB light (wavelength: 280-320 nm) is thought to be 1000 times greater per photon than that of UVA light (320-400 nm); however, the environmental exposure to UVA light can vary by 20-40 times based on factors such as elevation, longitude, and time of day. 21 Additionally, sunbeds and windowpanes expose people to more UVA radiation, and most non-broad spectrum sun blocks do not filter UVA as well as UVB. It is estimated that the mutagenic effect of UVR causes more than 75% of cutaneous melanomas in White populations. 22
Indoor Tanning
The International Agency for Research on Cancer (IARC) classified tanning bed rays as a carcinogen due to greater quantities of UVA and UVB exposure than that of the daily sun (for most locations), even though an estimated 7.8 million women and 1.9 million men use tanning beds annually. 23 There is evidence linking the number of times utilized in tanning beds, the number of sessions of therapy, or the duration of use to the risk of skin cancer in a dose dependent manner.
Arsenic Toxicity and Ionizing Radiations
Less common extrinsic risk factor in addition to UV rays is the chronic exposure to arsenic as well as ionizing radiations. 17 Skin is prone to arsenic buildup. Hyperkeratosis and skin hyperpigmentation have long been recognized as the primary indicators of prolonged arsenic (As) contact. These dermatological wounds have a strong correlation with a higher likelihood of skin cancer. The effect of oxidative stress is one of arsenic’s toxicity methods. According to research, oxidative stress caused by arsenic causes chromosomal instability, telomere destruction, destruction of DNA, and the death of cells. 24 According to research, oxidative stress caused by arsenic causes chromosomal instability, telomere destruction, destruction of DNA, and the death of cells. 24
Ionizing radiation is a known infective agent that may lead to skin cancer; the direct DNA injury is seen as one major point here. 25 This form of radiation for instance X-rays and gamma rays has enough energy to strip off electrons which are tightly bound to atoms, and therefore results ions formation. The oxidative lesions that occur due to ionizing radiation can lead to mutations if not fixed and this can bring about the malignant changes of skin cells. Such procedures also contribute to radiation exposure; hence, protective and precautionary measures as well as avoiding exposing oneself unnecessarily to X-rays and similar procedures.
Genetic and Personal Factors
Age
Advanced age is an important contributor to risk of skin cancer. 26 As the average lifespan has increased, more skin cancers are anticipated unless greater efforts are made to detect and prevent them early on. Older people are more susceptible to risk factors of skin cancer, particularly because of the combined impact of extended and intense sun exposure and a less effective immune system and a diminished capacity for DNA repair. 27 Age-related increase in melanoma incidence and mortality rate are also observed, with individuals over 75 years of age typically receiving new diagnoses. 28
Personal or Family History
Personal or family history of any type of skin cancer occurs as one of the major risk factors. About 10% of melanoma patients have relatives with a record of the disease; however, only a limited number of congenital syndromes, including mutations and nevi, have been identified. While rare in random instances, mutations in the CDKN2A gene have been linked to up to 30% of genetic melanomas. 14
Genes and Hereditary Disorders
Based on the established facts, melanoma is increasingly influenced by genetic and hereditary aspects. Previously known risk factors included aberrations in the genes such as CDKN2A, CDK4, and BAP1. Of those genes, for instance, CDKN2A mutations interfere with the cell cycle and are identified in a significant portion of familial melanoma, thus requiring thorough genetic analysis. 29 Furthermore, persons with hereditary syndromes including FAMMM syndrome, which is a phenotype that has multiple atypical mole and family history of melanoma, greatly have higher probabilities. 30 The presence of these alteration makes many to get affected by melanoma and several primary melanomas in a lifetime. Also, difference in genes such as melanocortin-1 receptor (MC1R), which is involved in skin coloration, would make an individual more vulnerable to DNA damage caused by UV radiation, thus, heightening melanoma risk.
Fair Complexion
Melanoma originates from individual vulnerability, connected to the skin’s melanin content and its ability to turn brown in response to UV light exposure. Among white people, the Fitzpatrick skin type is a reliable indicator of the relative risk of skin cancer. 31 Because melanin has a defensive function, darker skin is better shielded from the harmful effects of UV radiation from sunlight. 32 Compared to phaeomelanin, which is more prevalent in people with lighter complexions and red hair, eumelanin, which is synthesized in greater amounts in people with darker complexions, provides greater protection against UV radiation. Although eumelanin scatters UV rays to protect DNA, it also reduces the production of cutaneous vitamin D3. 21
Prevention
Diagnosis at an early stage as well as treatment play a crucial role in improving the outcomes of the disease, however, prevention plays a critical role in decreasing the frequency of the disease and early prediction of cancer. Prevention of skin cancer has been categorized into primary prevention, secondary prevention, and tertiary prevention.
Primary Prevention
According to the IARC, primary prevention can be described as any kind of prevention that decrease the possibility of development of cancer in humans, and this is further sub-categorized into collective and individual level. 33 Instead of being limited to the private sector, primary prevention could be a part of an overall approach that also includes the implementation of regulations, guidelines, and prevention-related campaigns, as well as organizational, administration, and community proactive measures and programs. 34
Primary prevention includes the avoidance of excessive UV radiations, which have the chances to reduce genetic and epigenetic risk factors described above. The promotion of sun-safe behaviors is the main assistance in avoiding the harmful effects caused by UV radiations. These include wearing protective clothes and wide-spectrum sunscreens with an SPF of at least thirty.
35
Applying sunscreen on a regular basis has been demonstrated to have long-lasting, sustained impacts on the frequency of primary melanomas (HR = 0/50, Cl 95% = 0.24-1.02, P = 0.05) for up to 10 years, and using it in childhood also lowers the risk of developing one in adulthood.
36
The American Cancer Society (ACS) suggests preventing exposure to the sun between the hours of 10
It is generally agreed upon that areas subjected to the sun should be covered with a broad-spectrum, water-resistant sunscreen with an SPF of 15 to 30 or higher. 37 , 38 The sunscreen should be reapplied once every two hours or after diving, perspiring, and toweling off. Additionally, the International Commission on Non-Ionizing Radiation Protection advises installing sunscreen dispensers at workplaces. Sunscreens with SPF 85 or 100 are more effective at preventing sunburns than those with SPF 50, even though there is no direct linear relationship between the value of the SPF and effectiveness (level II evidence). 39 Furthermore, higher SPF sunscreens may be better at compensating for insufficient application because sunscreen users typically apply less than 2 mg/cm2, the density used for testing by the US Food and Drug Administration and other organizations. 40 The American Cancer Society 41 also suggests completely avoiding artificial UV exposure, including tanning facilities. Tanning facilities mainly utilize artificial UV radiation to develop a tan and have been proven to raise the risk of skin cancer. Exposure to tanning beds is in a concentrated form, and it is proven that the UV light alters the DNA skin cells and makes them mutate, hence cancerous. 42 Also, regular tanning bed usage has cosmetic effects including skin aging, eye harm, and immune system dysfunction.
When paired with sunscreen and/or UV-protective clothing, other externally chemo preventive options have been described as providing additional protection. These options include retinoids, antioxidants (such as nicotinamide and green tea polyphenols), cyclooxygenase-2 inhibitors, and DNA repair enzymes like T4 endonuclease, photolyase, or 8-oxoguanine glycosylase.43,44 Because reactive oxygen species (ROS) and oxidative stress are major factors in the adverse consequences of UV exposure, antioxidants may mitigate these effects by inhibiting the production of ROS, which may also stop protective enzymes from being inactivated and DNA damage from being induced. As a result, systemic antioxidant administration has been suggested as a different or extra UV radiation protection strategy. 45
Secondary Prevention
According to the IARC, early identification and screening are the two main elements of secondary prevention, which will ultimately lead to the early detection of tumors or malignancies in their early stages. 33 Secondary prevention of skin cancer includes interventions that help detect the cancer in an early stage and treat it, to avoid deterioration and formation of new sites. Self-skin checks as well as professional skin checkups are vital to check for early signs of any skin lesions. Methods including dermoscopy and digital surveillance of moles, can also increase the efficiency of early-stage melanoma and other skin malignancies identification. 46 Another approach of secondary prevention includes creating awareness on the need to detect the diseases as early as possible, and creating awareness on signs to watch out for in skin cancer is equally essential. The option of mobile health technologies has enhanced the accessibility of early diagnostic services where teledermatology has also been deemed to have added a positive value propelling the unprecedented results. 47
Adults with light complexions, a familial background of sun exposure, a genetic vulnerability, relevant previous medical history, or other factors are recommended to undergo routine screenings. 14 Programs for screening for skin cancer are clinically beneficial, according to a 2017 meta-analysis of 15 studies. 48 Through intended screening, UV biomarkers can assist in identifying patients at greater risk for secondary prevention. As has been observed with other cancer types like breast and prostate cancers, categorization of risk can help to prevent screening of low-risk populations, which may lead to raised expenses for therapy and little death gain through the excessive diagnosis of melanoma and skin cancer. 49 Experts advise screening populations that are deemed high risk due to the previously mentioned factors. A limited patient population screening program may encourage early melanoma diagnosis, enhancing patient quality of life and lowering treatment expenses. 35
Tertiary Prevention
Intervention techniques used after negative effects have already manifested are referred to as tertiary prevention. Tertiary preventive measures include medical and occupational rehabilitation for skin cancers related to UVR after treatment, with the ultimate goals of providing a secure transition to employment, healing from the disease, and an excellent standard of life. Tertiary skin cancer prevention focuses on decreasing disease consequences with better patients’ quality of life being a main goal. 50 This comprises extensive caring approaches for dealing with the likelihood of the cancer returning, for handling new spreading of the cancer, and handling complications of treatment. After treatment follow-up aims at seeing whether there is recurrence of the same disease/condition or even formation of new primary skin cancers where the patient will be required to go for periodic dermatological examinations, imaging and sometimes lab investigations.
Moreover, tertiary prevention includes other modalities such as counseling and any other necessary support for the patients. 51 Some of them even suffer from pressures resulting from having a disease or undergoing a certain treatment, which requires their interaction with other healers, such as psychologists. Other intervention procedures that are helpful include outpatient educational programs for enhancing the patient’s knowledge on skin cancer, ways by which risk factors may be prevented, and support groups. All enumerated care approaches aim at ensuring that the patients are well managed with the disease and other aspects of their wellbeing.
Diagnosis of Skin Cancer
Accurate and rapid diagnosis of skin cancer serves to be the most vital step in combating the challenge of skin cancer spread and exacerbation. It significantly influences the prognosis and treatment of skin cancer. Melanoma skin cancers have a very high-tendency of gradually spreading out to the whole body which makes the treatment process extremely difficult and can ultimately led to fatality. 52 Thus, early intervention can result in a more efficient and successful recovery process.
The recent trends show shift of focus towards minimally invasive or non-invasive diagnostic technologies coupled with Artificial Intelligence and automated characterization. Using non-invasive imaging technologies significantly reduces the number of unnecessary biopsies and excisions. Information obtained from non-invasive diagnostic tools can be processed by deep learning and machine algorithms to accurately and rapidly characterize and detect the skin cancer.53,54 Moreover, recent studies also reflect the fact that efficacy of combination of multiple diagnostic techniques outpaces the efficacy of a separately used technique. The main aim of emerging techniques is to ensure rapid diagnosis with high accuracy, sensitivity, specificity, comfort, least labor and less financial burden. The following sections explore different types of diagnostic techniques, highlight recent trends and identify research gaps that are necessary to fill to ensure early diagnosis of skin cancer.
Non-invasive methods
Application of Non-invasive Methods for Diagnosis and Characterization of Skin Cancer.

Abbreviations: RCM: reflectance confocal microscopy; OCT: optical coherence tomography; FF-OCT: Full-field optical coherence tomography; NNB: numbers needed to be biopsied; EIS: electrochemical impedance spectroscopy.
Optical Coherence Tomography
Optical Coherence Tomography (OCT) utilizes a low coherence light to generate cross-sectional images of skin tissues on the basis of interferometry. It finds its application in early diagnosis of skin cancer but is not widely used for detection of melanocytic lesions. 54 It exhibits high sensitivity and sensitivity. However, its low resolution, limited penetration depth and requirement of complex setup serve as a limiting factor for its use in clinical practices. A survey conducted among 29 plastic surgeons of different European countries showed that only 20.9% of them employed OCT for skin cancer diagnosis in their clinics. 68 Several research studies have been carried out to modify the conventional OCT model in order to combat these shortcomings. Previous literature studies focused more towards exploration of application of modified OCT models such as LC-OCT (Line-field Confocal Spectroscopy) and HD-OCT (high-definition OCT) and MSS-OCT (multi-beam Swept Source OCT). 54 Recently, FF-OCT (Full-field OCT) has gained more attention due to its clear visualization for skin lesions and comparatively easy setup. They have a charge-coupled device (CCD) or complementary metal-oxide-semiconductor (CMOS) camera as output detector in addition to low coherence interferometer.61,69 Another recent approach is Ns-OCT (Nanosensitive OCT) that works on the principle of spectral encoding of spatial frequencies and possesses nanoscale sensitivity to structural alterations. Thus, it aids in creation of high-resolution real-time images of skin lesions to detect skin cancer, monitor the disease prognosis and study impact of treatment of skin cancer. 70 NsOCT can also be used in combination with the broad bandwidth high-resolution SD-OCT (Spectral Domain OCT) to further improve the resolution of structural imaging. 71 These all modifications have notably enhanced the performance of OCT but need for improvement persists in order to ensure early diagnosis of skin cancer with high accuracy.
Liquid Biopsy
Liquid biopsy is categorized as non or minimally invasive diagnostic and prognostic technique which rely upon screening of biomarkers, such as circulating tumor DNA (ctDNA), circulating gene transcripts (cfRNA), circulating tumor microRNA, exosomes and circulating tumor cells (CTC), present in body fluids in order to detect genetic or molecular modifications.72,73 They not only help in diagnosis of cancer but also determine patient’s response to therapy, evolution of tumor and disease progression. It indicates the real-time condition of tumor which paves the way for targeted or personalized therapy. However, due to its low specificity and sensitivity, it is not used widely used for early diagnosis of skin cancer. 72 None of the stage-specific biomarkers are clinically validated. 74 Recent research studies are exploring the methods to overcome such shortcomings of liquid biopsy. Such efforts include profiling of ctDNA through Next Generation Sequencing based liquid biopsy, combining liquid biopsy with label-of-chip approach and other strategies like microfluidics, electrochemical methods and dielectrophoresis.72,75-77 NGS-based liquid biopsy is a promising approach for accurately profiling ctDNA, even with a low representation, and flourishes precision oncology. However, in order allows to distinguish the clinically relevant mutations, it is necessary to pair it up with bioinformatics tools and artificial intelligence.75,76
Reflectance Confocal Microscopy
Reflectance confocal microscopy (RCM) illuminates a specific area of skin through a near-infrared laser that emits monochromatic coherent light. The reflected light passes through a pinhole and reaches the detector which creates a high-resolution grayscale image. 78 Varying refractive indices result in formation of distinguishable features. Light reflected from a surface of high refractive index appear brighter in the images. Due to this reason, melanin and keratin appear brightest and are easily distinguishable through RCM. 54 It provides high sensitivity and specificity highlights its potential as a useful tool for detailed skin analysis in both research and clinical settings. However, its visualization depth is limited and requires expensive equipment and trained personnel.
Adhesive Patch Biopsy
It is a genetic-based diagnostic and prognostic technique that involves obtaining dispersed mRNA of melanocytes from the outermost layer of epidermis, stratum corneum, by applying an adhesive patch. The cells stick to adhesive tape and are analyzed. 54 Presence of specific biomarkers indicate the occurrence of skin cancer. A 17-gene biomarker classification system was initially proposed that accurately detected melanoma with sensitivity and specificity of 100% and 88% respectively. 79 Later, a 2-gene pigmented lesion assay (LINC00518 and PRAME) was introduced that showed a sensitivity and specificity of 91% and 69% respectively and reduced its operating cost. 80 A pooled analysis of 2-gene PLA-based five studies showed a sensitivity and specificity of 86.9% and 82.4% respectively. 57 Apart from these, more complex assays have also been developed for obtaining specific information. 54
This technique exhibits high sensitivity and specificity and can play a role in advancing precision oncology. Its minimally invasive nature influences comfort of the patient. 54 The skin samples obtained through adhesive patch are easy to transport and store as well in a cost-effective manner. 81 However, this method is unsuitable for detecting ulcerated or scarred lesions or lesions present on nails, soles, palms and mucosal membranes.80,82 Inadequacy of mRNA in the collected sample might necessitate repeated sampling. 83
Electrical Impedance Spectroscopy
The cancerous cells or tissues exhibit unique electrical properties due to their cellular characteristics that distinguishes them from the normal tissues. The changes in tissue properties can be detected through their altered response to electric current. It measures impedance at different frequencies and gives a score depending upon the severity. 54 Lesions yielding a score between 3-6 are suspected to be malignant and are required to be continuously monitored, whereas a score exceeding 6 indicates a high likelihood of malignancy and necessitate the biopsy. 84
It has been thoroughly researched for the detection of melanoma. A safe amount of current voltage is applied on the skin lesions to measure, analyze and digitize the impedance recorded. The integration of EIS in the skin screening process allows early diagnosis and aids in monitoring the progression. A study reported that incorporation of EIS scores reduced NNB (numbers needed to be biopsied) from 6.3 to 5.3. 62 It is a comparatively straightforward and rapid method. However, it is reported that it has lower accuracy. 85 The screening of small lesions (less than 2 mm diameter) or lesions characterized by low cellularity may give false-negative results whereas seborrheic keratosis may sometimes generate false-positive results.86,87 Another limitation of this methodology is its inability to properly and readily screen inflamed, scarred and ulcerated lesions and some specific regions of the skin including soft areas, bony and curved areas, palms, and soles. It exhibits higher sensitivity; however, its specificity is lower.87,88
Raman Spectroscopy
Raman spectroscopy relies upon recording and analyzing the Raman spectra. 89 When light passes through a cell or tissue, some of the photons experience change in energy due to the vibrations of molecular bonds of the cell or tissue, thus causing inelastic or Raman scattering of photons. This change in energy is dependent upon the molecular nature of cells or tissues which is altered in case of cancer. Thus, it allows to differentiate between normal tissues, benign or malignant lesions. 85
In RS-based diagnostic models, a near-infrared laser radiation emitting probe serves as a proton source and the change in energy is recorded by a spectrometer in order to predict the nature of lesion.89,90 It is reported to reduce the number needed to be treated from 8.6 to 4.1 which demonstrates its potential for reducing the unnecessary biopsies. 55 Its high sensitivity contributes to the accuracy of its results. However, it requires long acquisition time and expensive apparatus which limits its clinical utility. 88 Apart from diagnosis, Raman spectroscopy has also been utilized in treatment. It can assess the tumor margins and assist the skin cancer surgery. 91
Role of Artificial Intelligence in Diagnosis of Skin Cancer
Keeping in view the need to speed up and improve the accuracy of the diagnostic process, artificial intelligence has found its way in the diagnosis of skin cancer. The images captured by aforementioned imaging techniques can be accurately analyzed by utilizing artificial intelligence. Recent studies demonstrate increased interest in exploration of machine learning and deep learning techniques for assisting the diagnosis of skin cancer, with greater focus towards deep learning. Deep learning is a subgroup of machine learning that requires comparatively less human intervention and extracts the features automatically.92,93
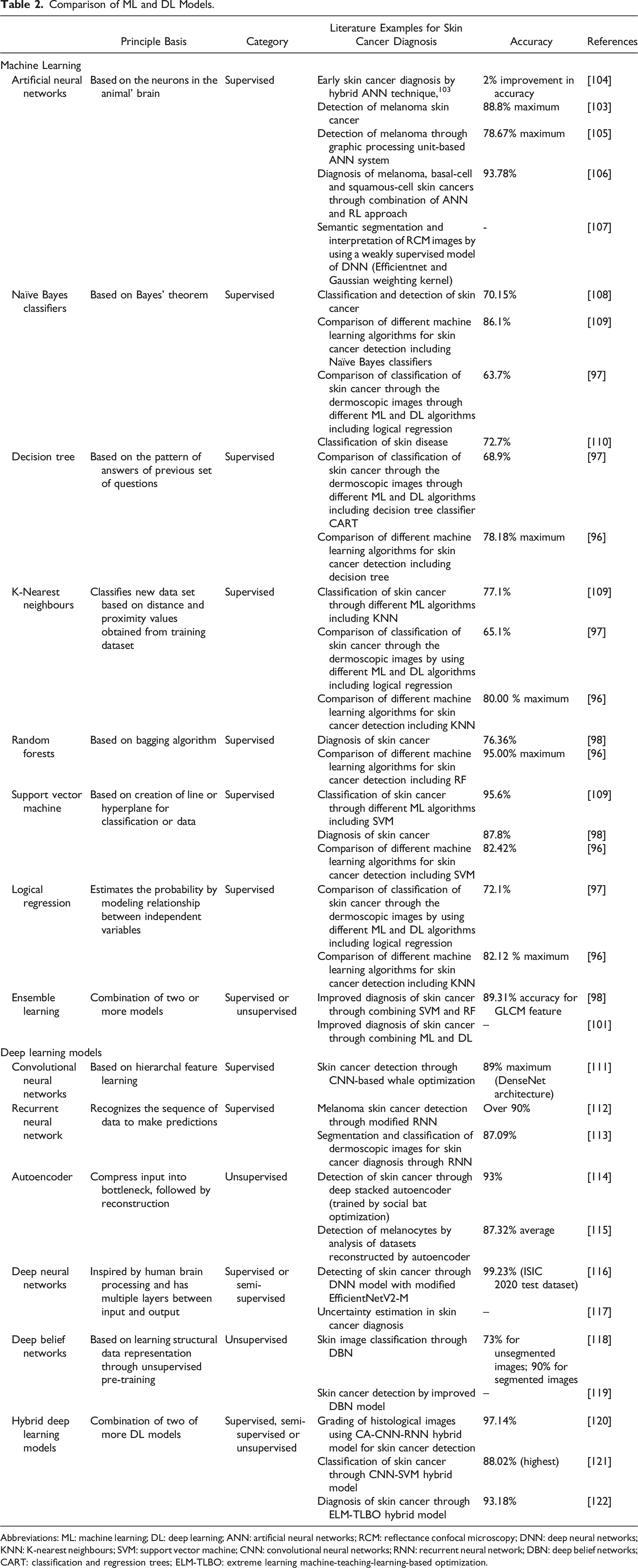
The training time of deep learning techniques is usually longer than the machine learning algorithms. Due to this reason, the pre-trained models have recently grabbed more attention. Transfer learning can be utilized to re-use the information obtained from previously performed task.94,95 The research trends of Artificial Intelligence for diagnosis of skin cancer are also visualized in Figure 1. A study was conducted on a comparison of machine learning algorithms for detection of skin cancers and concluded that random forest algorithm gave overall best performance with maximum accuracy of 95.00% and recall of 86.36%. Even when compared with some deep learning algorithms including Convolutional Neural Networks (CNN), it yielded best results with comparatively lesser training time.
96
However, another study reported that performance of deep learning algorithms (maximum accuracy of 88%) outpaces the machine learning algorithms (maximum accuracy of 72%). Among machine learning algorithms, they evaluated Gaussian Naïve Bayes, K-Nearest Neighbor, Decision tree classifier, Linear Discriminant Analysis and Logistic Regression algorithms. They found LR to be the most optimal ML model as it effectively classifies the data in two distinct classes, malignant or benign. They concluded that use of deep learning models, especially pre-trained models like VGG16, is a fruitful methodology for diagnosis and classification of skin cancers from dermoscopic images. The accuracy of ML models was improved to the level of 75% by employing ensemble learning.
97
There are several other examples from literature that support superiority of ensemble models over any individual model. A study showed that an ensemble model of support vector machin (SVM) and radio frequency (RF) (89.31% accuracy, 88.56% sensitivity, 87.81% specificity) outperformed individual SVM (87.8% accuracy, 85.72% sensitivity, 83.64% specificity) and RF (76.36% accuracy, 74. 28% sensitivity, 72.2% specificity) models.
98
Table 2 gives a comparison of commonly studied ML and DL algorithms for assisting skin cancer diagnosis. Another review emphasized on the increasing trend of integration of deep learning algorithms in the diagnostic approaches.
92
CNN algorithms are one of most researched deep learning models for assisting diagnosis of skin cancer. A study utilized an ensemble of pre-trained CNN model and voting strategy along with a patching approach to automate the classification of dermoscopic images.
99
In another study, classification of skin cancer from dermoscopic images by employing patch-based local deep feature extraction using pre-trained CNN models improved the accuracy and automated the diagnostic process.
100
Similarly, several other deep learning models have been exploited for image classification to speed up the diagnostic process. Research Trends in use of AI models for skin cancer classification. Comparison of ML and DL Models. Abbreviations: ML: machine learning; DL: deep learning; ANN: artificial neural networks; RCM: reflectance confocal microscopy; DNN: deep neural networks; KNN: K-nearest neighbours; SVM: support vector machine; CNN: convolutional neural networks; RNN: recurrent neural network; DBN: deep belief networks; CART: classification and regression trees; ELM-TLBO: extreme learning machine-teaching-learning-based optimization.
The contradictory implications of the recent comparative studies highlight the need of more research. In order to integrate artificial intelligence, there is a need to remove the hurdle between medical professionals and AI. Secondly, accuracy of AI algorithms, especially deep learning algorithms is directly dependent upon available datasets for training and low diversity of available datasets may also lead to biased predictions. It is necessary to standardize the AI algorithms to improve their clinical utility. 92
Development of ensemble models by strategically combining such AI algorithms which complement each other by analyzing the inherent limitations of individual models appears as a promising strategy for improving their efficiency. According to a study, ensemble of machine learning and deep learning algorithms resulted in a greater efficiency and accuracy. 101 It is important to notice that even if artificial intelligence continues to grow stronger, importance of human involvement cannot be denied. A research study conducted showed that the diagnostic model performed better and had greater accuracy when the artificial intelligence was paired up with the human assistance. 102
Treatment
Treatment for skin cancer comprises of a range of modalities which depends on the specific type and the extent of spread of skin cancer, and the method of diagnosis as well. Several types of treatment regimens are present. Below, Figure 2 provides an overview of several types of treatment regimens discussed in this article. Overview of treatment methods.
Surgery
Surgery is employed for localized skin cancers. 123 It includes a combined utilization of chemotherapeutics and excisional removal of tissues. Traditional method of surgery includes the employment of a scalpel to a certain depth. Effective adjuvant and neoadjuvant therapy are decreasing the requirement for invasive surgical procedures, but the importance of surgery for accurate disease staging, early-stage melanoma detection, and palliative care in more advanced instances cannot be denied. It was found that surgical treatments in melanoma may attain a high rate of local control with low chances of recurrence most often in the localized stage of the disease. The main types of surgical methods employed for treatment of skin cancers includes:
Excisional Biopsy
In this treatment method, the afflicted skin area, or the tumor, is surgically removed from the body alongside a portion of the normal cells, and the incision site is then stitched back together. The cut tissues by a dermatopathologist are sent to the laboratory. This is done for the confirmation of the removal of whole tumor from the body. Fusiform shape mark is preferred for the prevention of excess skin during ablation. 124 In melanoma, excisional biopsy is done where the biopsy is also therapeutic and involves the removal of the tumor completely. 125 It affords total excision with disease-free margins, thus, decreasing the potential of tumor reappearance.
Mohs Micrographic Surgery
Contrary to the excisional biopsy, this surgical method is precision based that spares the healthy tissues. It is usually employed for the recurrent type of skin cancer, and preferred when conservation of skin is required. This type of surgery is ambulatory which is often preferred for large area tumors, and it combines the elimination of the tumorous tissue from body with microscopic examination during surgery. The removal of the tumor also affects the small areas of damaged skin, as determined by categorized form evaluation of the skin. 126 Additionally, the region is examined to determine whether any more tumor cells or tissues exist where the tumor was removed. Next, a thin section of the tissue underneath is removed, and its histology is examined using a preserved subsection to determine whether there are any tumors present. In case of detection that tumor is still present, the process is repeated until no detection appears. The person stays in hospital during this period. 127
\The primary advantage of Mohs surgery is its ability to precisely control the entire tumor margin at the microscopic level while optimizing the maintenance of healthy tissue. 97% of primary tumors are cured after 5 years, and 90% of recurrences are cured after 5 years, according to retrospective studies. In comparison, alternative methods result in 77% of recurrences and 92% of primary tumors.128,129 This technique is suitable for early melanoma where the cancer is limited to the surface layer of the skin; melanoma in situ and thin melanomas (<0.8 mm Breslow depth) in cosmetically or functionally sensitive areas, and it has very high cure rates without removing much tissue while the doctor is gradually shaving off layer of skin and looking at it under a microscope to ensure there are no cancer cells left.130,131
Photodynamic Therapy
This method involves applying a deactivated topical medication to the region that is affected, and then exposing the area to a specific light wavelength to further activate the area. Photodynamic therapy (PDT) relies on three essential components: photosensitizer, light, and oxygen. They initiate a photochemical reaction that produces several free radicals and singlet oxygen, a highly reactive material. 132 Through significant alterations in the structure and function of the cellular membrane as well as internal processes, they trigger the cytotoxic activity that impairs major cellular functions and eventually causes cancer cell death. 133
Because PDT is non-invasive and has few side effects, it may be an alternative beneficial treatment for patients with advanced melanoma. According to Baldea et al, PDT on human and mouse melanoma cells using different techniques greatly enhanced necrosis, apoptosis, tumor growth arrest, and extended life of animals utilized in experimental settings; however, complete recovery was infrequent and was followed by complications and adverse effects. 134
Radiotherapy
Radiotherapy serves as one of most common treatment methods of skin cancer. 135 Older people and co-morbid patients, when surgery is not an option, with limited capacity for function can benefit from relatively brief hypo-fractionated radiation therapy. In radiation therapy, the tumorous area’s outer skin surface is the only area that receives radiation. Radiotherapy uses low energy x-rays (superficial radiation therapy) or electrons (electron beam radiation), neither of which penetrates the skin more deeply. 136 It provides synergistic effect when used in combination with immunotherapy. 137
In melanoma, radiotherapy is employed as an adjuvant therapy to irradiate any left-out disease after surgery in addition to a mode of treatment for tumors that cannot be removed surgically. Kin 13 suppresses the production of nuclear factor NFkB. It contributes to cancer cell death by directly damaging the DNA and by production of cytokines and reactive oxygen species that cause oxidative stress and damage to cellular components. 138 Dosages include better control of localized recurrence and possible gain in the survival rate, but it is likely to cause side effects, for example, skin alterations and formation of second cancers.
One of the factors impacting the efficacy of radiotherapy is the radioresistance of melanomas, mainly due to the overexpression of DNA repair genes and the regulation of multiple biochemical repair pathways. A recent study highlights the potential of Microbeam radiation therapy (MRT) to overcome these limitations by delivering high-dose, spatially fractionated radiation. This can contribute to improvement in tumor control while reducing normal tissue toxicity through selective damage. Utilizing MRT in combination with immunotherapy appears to be a promising approach for melanoma management.139,140
Chemotherapy
Chemotherapy might be considered in specifically developed or spread skin cancer cases when surgery is not an option or when the cancer has spread to other body parts. 16 Chemotherapy drugs can be administered orally or intravenously in these circumstances to target cancer cells throughout the body. They disrupt the critical cellular processes such as cross-linking of DNA, blocking activity of topoisomerase, interfering with the nucleic acid synthesis, disrupting DNA replication, thus leading to the cancer cell death. 141 Chemotherapy in melanoma has overall fewer response rates than other more innovative treatments, although it is utilized occasionally in complexes with other treatments. 56
Topical Chemotherapy
To treat precancerous skin conditions that have not penetrated the deep layers of skin or spread to other organs, topical chemotherapy medications, such as 5-flurouracil (5-FU) in cream form, can be employed directly to the skin’s surface. 123 This kind of chemotherapy can minimize contact with normal tissue and its possible side effects because it is localized. Imiquimod, for instance, which is applied at the surface of the skin, causes an immunological reaction against melanoma cells for the treatment of superficial melanomas. 142
Systemic Chemotherapy
Dacarbazine is among the alkylating agents which have been used in the past in the treatment of melanoma but has been replaced by more effective targeted and immunotherapies. 143 However, it may still be used as the last resort in cases of metastatic diseases. It causes cross-linking of DNA through addition of alkyl groups which prevents its replication, ultimately leading to cell death. 141
Immunotherapy
Antigen-antibody interactions are the basis of immunotherapy, a novel approach to cancer treatment. By attaching to target cell receptors, interferon plays a significant part in immunotherapy in treating cancer. For cancer cells, interferons have antiproliferative properties through growth factor inhibition, pro-apoptotic gene activation, and promotion of antiangiogenic activity. They also help the immune system combat agents that cause cancer. 144
Ignacio et al investigated the impact of cancer immunotherapeutic administered intratumorally on tumor cells. The study’s findings showed that administering the iontophoretic entity directly to the tumor alters the immunotherapeutic agent’s toxicity profile significantly and increases its efficacy or therapeutic index by avoiding systemic exposure. 145
Skin Cancer Immunotherapy Types
Checkpoint Inhibitors
By obstructing specific proteins that impede the body’s defenses, these medications improve the ability of immune cells to identify and combat cancer cells. Treatment for skin cancer frequently involves the use of checkpoint inhibitors such as PD-1 (programmed cell death protein 1) and CTLA-4 (cytotoxic T-lymphocyte-associated protein 4) inhibitors. 127 Anti-PD-1 (pembrolizumab, nivolumab) and anti-CTLA-4 (ipilimumab) antibodies inhibit the negative signals given by the tumor to the T-cells increasing their activity against melanoma cells. 146 Ipilimumab influences the T cell activity by blocking CTLA-4, a protein that suppresses immune system reactions. Its effectiveness in preventing disease recurrence and combination use with PD-1 inhibitors are being studied. When used as monotherapies, anti-PD-1 medications have shown 40-60% response rates. 147
Cytokine Therapy
The immune system is controlled by signaling molecules called cytokines. Interferons and interleukins are two examples of cytokines used in skin cancer immunotherapy to boost the immune system’s defense against cancer cells. 127 Agents such as IL-2 enhance the immune response but have cytotoxic effects therefore are restricted. 148
CAR-T Cell Therapy
The goal of chimeric antigen receptor (CAR) T-cell therapy is to genetically alter a patient’s T cells so that they express receptors that recognize antigens unique to cancer. 127 The generation of CAR specific for melanoma-associated antigens from engineered T cells can be considered a successful concept; however, the clinical application of the concept is not very advanced.
Oncolytic Virus Therapy
Oncolytic virus therapy has been exploited to treat melanoma skin cancer that has spread to soft tissue, lymph nodes, or other areas of the skin and is no longer treatable. As a targeted therapy, T-VEC reduces lesions in the skin and lymph nodes while also eradicating melanoma cells. The exact way in which T-VEC functions within the immune system is still unknown. However, in addition to killing cells directly, antigens, which trigger an immune response, and GM-CSF, a molecule that fortifies the immune system, are believed to be additional ways that the virus may trigger an immune response that fights melanoma.149,150
Cancer Vaccines
Cancer-fighting vaccines, like the MAGE-A3 vaccine, enhance the immune system’s defense against the disease by specifically targeting antigens that are expressed by cancer cells. Trials are still underway to determine how well they work to boost immune responses in the fight against melanoma.151,152 According to research from Oregon State University College of Pharmacy, a vaccination that boosts the production of a protein essential to the skin’s antioxidant system may help people strengthen their defenses against skin cancer. 153 An mRNA vaccine has demonstrated promise in treating stage 3 and stage 4 melanoma in clinical trials. When combined with immunotherapy treatments, the Moderna vaccination was found to have a 44% reduced risk for mortality and complications from melanoma in stages three and four than when used alone. 154 The treatment efficacy of the personalized vaccines that target tumor-specific neoantigens is evident from multiple clinical trial results.155,156
New Checkpoint Inhibitors
According to research, suppressing or blocking LAG-3 can improve T cells’ capacity to eliminate tumors, lessen their influence over immune responses, and increase their cytotoxic activity. Apart from CTLA-4 and PD-1/PD-L1, LAG-3 has emerged as a new target for immunotherapy against tumors and a prognostic indicator for them.157,158
Personalized Immunotherapy
Using the patient’s immune system to combat tumor cells, personalized immunotherapy is a form of highly customized cancer treatment. For patients whose cancers do not respond to conventional treatment, the discovery of uncommon anti-tumor lymphocytes that can infiltrate and aid in the removal of metastatic solid epithelial tumors may promote the development and efficacy of specialized cancer immunotherapies. 159 Studies are being conducted to evaluate the efficacy and safety of CAR-T cells that have been designed to target antigens that have been identified. The first phase I trial in Europe to treat melanoma with CD20 CAR-transduced T cells was scheduled for March 2019 (NCT03893019). The trial’s justification stems from the discovery that CD20 is expressed by melanoma cancer cells and that eradicating CD20+ cells in preclinical models has potent anticancer effects. 127 Immunotherapies have significantly altered the prognosis of melanoma and resulted in durable survivals as well as responses to treatment however immune-related side effects are not uncommon.
Combination Therapy
Every treatment methodology has certain drawbacks. However, combining multiple methodologies can reduce such shortcomings and improve the efficacy of the treatment. The efficacy of combination therapy outpaces monotherapy. Multiple therapies interact synergistically to give optimal performance. 160
Nanotechnology in Treatment
Nanotechnology exhibits great potential for obtaining optimal results from the skin cancer treatment methodologies due to their ability to enhance selectivity, epithelial permeability and strength while reducing the risk of unintended harm to nonmalignant cells and drug resistance. 161
Advancements in nanotechnology have significantly influenced precision oncology. The nanoparticles can be modified to meet specific therapeutic demands and surpass the heterogenous biological barriers. For instance, iCluster is an example of smartly designed nanoparticles that is initially bigger in size which facilitates its transport in blood. Later, its size is shrunk which allows better penetration.162,163 They may be organic, inorganic or hybrid. They can easily pass through the barriers of tissue and can be directed towards specific sites for targeted drug delivery.
164
According to a study, nano-based targeted delivery systems for mRNA therapeutic vaccines not only improved the drug delivery but also prevented mRNA from degradation.
165
They have been explored to assist immunotherapy by protecting antigens from degradation, enhancing their presentation, augmenting their bioavailability, assisting their delivery pathway and improving their efficiency.
155
They reduce the risk of off-target delivery in genome editing therapies.
163
They are also reported to improve efficiency and specific targeting of photodynamic therapy through nano-based targeted delivery and nano-modulation of photosensitizers.
166
For instance, chitosan-coated liposomes improved efficiency and stability of indocyanine green for PDT.
167
Another study highlighted that copper-cysteamine (Cu–Cy) nanoparticles assisted PDT simultaneously induced immunotherapeutic and oxidative effects as well on melanomas, thus significantly enhancing the treatment efficiency.
168
5-Fluorouracin possesses anti-cancerous properties and showed cytotoxic effects on tumor’s MCF-7 cells when delivered through a topical gel containing aptamer-functionalized polymeric nanocapsules.
169
In chemotherapy, the main concern is low bioavailability and permeability of chemotherapeutics which hampers its therapeutic efficiency. However, nanoparticles have emerged as a potential tool to address these limitations. Chitosan based nanoparticles improved the penetrability, bioavailability and inhibitory action of a chemotherapeutic agent,10-Hydroxycamptothecin (HCPT).
170
Another study showed that combination of cisplatin and
Despite all these benefits, there still exists a barrier between scientific literature and commercial implementation. 172 Non-availability of commercialized nano-based therapeutic technologies highlights the need to further explore the characteristics of nano-based technologies and their possible toxicity. It is necessary to investigate the underlying mechanisms of the toxic aggregation and degradation of nanoparticles and the ways of preventing it. 173 The capping agents and ligands are proven to be efficacious in this regard, however, more investigations are still needed in order to develop a commercially available nano-formulation as a reliable therapeutic agent for skin cancer. 174 Such efforts are crucial to find the suitable nano-formulations that can be widely implemented in clinical settings and would pave the way for commercial-scale adoption of nanotechnology-based therapeutic approaches for treating skin cancer.
Precision Oncology
Precision oncology is a personalized approach that takes individual’s unique characteristics into account that influence the cancer, including biomarker analysis, genetic and epigenetic profile, to tailor the treatment and monitoring strategies in order to ensure optimal treatment efficiency while minimizing the toxic effects. Advancements in multi-omics have enabled in-depth evaluation of responsible factors and underlying mechanisms of cancer proliferation and has allowed to customize the management strategies accordingly. 175 Precision oncology doesn’t only encompass treatment but also prevention, diagnosis, prognosis and treatment response monitoring.
It begins with precision prevention which requires personalized risk assessment to opt for tailored monitoring approaches. 176 A randomized clinical trial was carried out to check efficacy of precision skin cancer prevention in Hispanics by testing for susceptibility gene, MC1R. It resulted in enhanced preventive behavior in more susceptible population. 177 Early detection can be done by next-generation 3D imaging of whole body to determine the precise anatomical position of lesions throughout the body, analysis of predictive biomarkers, sequencing of genomics, analysis of exact locations of genetic mutations and implementation of AI-algorithms for classification of lesions. 178 Many diagnostic biomarkers have been introduced so far and are under study to validate their accuracy. Such examples include 40 CpG methylation profile 179 and miRNAs for melanoma diagnosis, 180 overexpression of amino acid transporter for BCC diagnosis 181 and tumor‐cell‐derived C1r and C1s 182 and deletion of inositol polyphosphate-5-phosphatase A for SCC diagnosis. 183
Resistance and response to a particular treatment methodology may vary at individual level. Thus, a personalized treatment approach can be identified using multi-omics analysis, during or immediately after diagnosis. One of the most highlighted personalized treatment-predicting methodology is targeted-gene panel. It analyzes the cancer-related genes specific to an individual by using Next Generation Sequencing to figure out the most suitable treatment methodology.
184
NGS has paved the way for more detailed analysis including whole genome analysis and epigenetic analysis by making sequencing faster and cost-effective.185,186 Machine learning and deep learning algorithms are employed to rapidly analyze and make predictions according to the data obtained through sequencing. It also provides information regarding post-treatment response and survival rate. Pairing up genome sequencing with AI holds a great potential in improving utility of precision oncology.184,187 The role of AI in prediction of personalized treatment is also depicted in Figure 3. Artificial intelligence for prediction of personalized therapy.
Precision therapy has also enabled treatment of rare type of skin cancers. Such therapies are tailored according to the specific characteristics of neoplasms, keeping in view the underlying mechanisms of tumoral growth, treatment response, racial and age disparities.
Specific biomarkers and genomic signatures can also give information regarding disease prognosis and determine treatment efficacy by indicating the response. Tumor mutation burden (TMB), miRNAs and ctDNAs have been exploited to predict the therapy response.188,189 However, in patients with lower or medium burden, TMB might not be enough to predict therapy response. In such patients, UV mutational signature enrichment score is reported to be a fruitful predictor or treatment efficacy. 190 Another study suggested that pathway-based genomic signatures from on-treatment melanoma specimens have great potential to accurately predict response to immune-checkpoint blockade (ICB) therapies. 191 Soluble CTLA-4 192 and soluble CD73 189 have also been reported to predict the response of metastatic melanomas to ipilimumab and nivolumab-based targeted therapy respectively. Based on the data obtained from genetic and biomarker testing, AI has also been exploited to predict post-treatment response and the recurrence risk. According to the level of risk, appropriate monitoring strategies can be employed to eliminate the risk of recurrence. 193
Underlying Mechanisms and Their Association with Therapeutic Effects in Precision Oncology
Underlying Mechanisms of Tumoral Growth in Melanoma
Genetic Mutations and Oncogenes
Melanoma is often associated with the genetic mutations in the oncogenes that includes BRAF, NRAS and c-KIT. Thus, BRAF V600E, the most prevalent mutation, results in the constitutive activation of the MAPK/ERK pathway, which in turn boosts cell proliferation. 194 Understanding of these mutations has translated into the availability of targeted therapies such as BRAF inhibitors, including vemurafenib, and MEK inhibitors such as trametinib, which have high effectiveness in the treatment of BRAF mutated melanoma. 195
Tumor Microenvironment
There are also non-cancerous cells within the melanoma tumor microenvironment (TME) and these comprises of fibroblast cells, immune cells, and endothelial cells. The TME can modulate the tumor size, spread to other areas and its sensitivity to treatments. For example, cells of the immune system that locate themselves within the TME can either inhibit or promote new tumor formation. 196
Underlying Mechanisms of Immune Response in Melanoma
Immune Evasion by Tumors Immune Evasion by Tumors
Melanoma cells secrete PD L-1 and this interact with PD-1 receptors on T-cells and rendered them inactive. This Immune checkpoint pathway is actively being targeted by the therapies like; pembrolizumab and nivolumab which is an anti-PD-1 and atezolizumab against PD-L1 and this pathway makes the T cell responsive and enhance the survival rate from the melanoma patients. 197 The resistance promoting factors, such as complex cellular interactions due to T-lymphocytes or different biomolecules like cytokines, vary at the individual level and can be tackled through personalized immunotherapy. 198 The adoptive cell therapy targeting specific somatic mutations through chimeric antigens expressing-T cells and mRNA-based vaccines stimulating T-cell responses specific to patient’s tumor also appear as promising approaches for personalized immunotherapy. 155
Tumor-Associated Macrophages (TAMs)
In the case of melanoma, it was also demonstrated that TAMs may enhance tumor growth via stimulation of angiogenesis and disruption of anti-tumor immunity, as well as help in metastasis formation.199,200 Techniques are being developed to exhaust or reeducate TAMs to improve the outcomes associated with immunotherapies and other treatments.
Microbiome-Mediated Pathways
The activation RIG-I pathway enhances the effectiveness of ICB by improving tumor antigen presentation, promoting immune cell infiltration and creating an immune-supportive microenvironment. It activates the downstream signaling pathways that produce type I interferons and other inflammatory cytokines upon recognizing the pathogen. However, its activation is impacted by the microbiome surrounding the tumor. The diverse unique microbiome of mucosal melanoma causes loss of intra-tumoral RIG-I signaling which may contribute to poor anti-tumor immunity and immunotherapy resistance in mucosal melanoma. 201 Comprehending such mechanisms that are mediated by the microenvironment of the tumor have broadened the precision oncology.
Biological Aspects of Metastasis/Progression in Melanoma
Epithelial-Mesenchymal Transition (EMT)
EMT is a process in melanoma metastasis, where melanoma cells gain mesenchymal property thereby increasing it mobility and invasive nature. This process is partly responsible for spreading cancer cells and poor responsiveness to treatment. This suggests that a strategy of targeting pathways, associated with EMT including TGF-β signaling, could be effective in melanoma. 202
Circulating Tumor Cells
CTCs are melanoma cells that have left the primary tumor and migrate in the blood stream and thus spread. 203 CTCs can be used in understanding metastatic process and to evaluate the efficiency of therapy. Measures directed at CTCs are being trialed with a view of halting metastasis.
Main Aspects of the DNA Repair Mechanism in the Framework of Melanoma
Features of DNA Damage Response (DDR) pathways
Melanoma cells tend to have some defects in the DNA repair mechanisms including homologous recombination and NER. These defects make melanoma cells more sensitive to DNA damaging agents such as PARP inhibitors. 204 Several strategies could be advised to increase the likelihood of success of the treatments through disruption of DDR pathways and the possible resistance.
Disparities in Melanoma Treatment
Racial and Regional Disparities
There are documented disparities among racial demographics in both incidence rates as well as melanoma mortality, while white patients have higher rates of melanoma incidence, non- white patients, including African, American or Hispanic patients, have comparatively poorer survival rates. 205 This gap in survival rate is due to late-stage diagnosis in non-white patients. 206 Its root causes are attributed to the variations in genetic mutations, types of tumors, and care-seeking behavior. A study compared the genetic profile of Chinese melanoma patients with western patients through NGS and revealed significant differences in their genetic profiles. 207 Advancements in genome sequencing is facilitating the determination of race-specific genetic alterations that is essential for precision therapy. Formerly, it was reported that 40% of Chinese melanoma patients could be treated with drugs. However, a new study identified potentially actionable targets through DNA-NGS which increased the percentage of druggable Chinese melanoma patients to 75%. RNA-NGS further increased this percentage to 78%. 208
Age Disparities
The problem of older melanoma patients means that these patients have more developed several diseases and may have concomitant illnesses that affect the choice of therapy. 209 Approaches, that are modified with reference to the patient’s age, are required, for instance, changes in doses and type of used chemotherapy agents, or less invasive surgeries due to potentially lesser effectiveness but higher quality of life.
Gender Disparities
It is a fact that hormonal factors and genetic differences between male and female affect the prognosis of melanoma. Female patients seem to have a better prognosis than male patients because most patients who died were male and tumor characteristics between male and female seem to differ. 210 Gender specific research can help in offering style treatment methods.
Future Prospects and Conclusion
The field of melanoma has advanced significantly leading to breakthroughs in diagnostic technologies and treatment technologies. Despite extensive research efforts, melanoma continues to arise as one of the major health concerns. One of the major contributing factors is the gap between scientific literature and its practical implementation. The inadequate dissemination of research findings to the health care providers, policymakers and public lowers the clinical utility of concepts and methodologies. In addition, more research is needed to be done for standardization of introduced technologies, like artificial intelligence, to promote their utility. 211 To bridge the gap between practical and theory, the inter-disciplinary communication should be promoted. Diluiso et al suggested creation of Skin Cancer Units for this purpose. 68 Another factor that prevents incorporation of innovative research findings into clinical practices is unavailability of adequate evidence and controversial research implications. There is a need to include diverse and extensive class of patients for clinical trials to ensure the safety and clinical relevance of the devised methodologies. A recent study contradicted the diagnostic accuracy of pigmented lesion assay testing, which is known for its high sensitivity and specificity. 212 Thus, more and broad clinical trials are required to validate the accuracy before widely incorporating such controversial research findings in the clinical settings. It would significantly promote consumer and health care trust in innovative approaches.
Nanotechnology, multi-omics and artificial intelligence have an immense potential to revolutionize precision oncology which holds the key to success in cancer management. Thus, more research studies should be carried out to identify and minimize the risks associated with them. In regards to artificial intelligence, further studies are required to address the privacy concerns and the possibility of generation of biased results due to limited and less diverse available datasets. 68 A greater focus should be made towards prevention and early diagnosis to lessen the time and financial burden. Combination of techniques have been reported to outpace the efficiency of mono-techniques across various domains, including diagnostic techniques, therapies and AI algorithms. Thus, future studies should explore and validate strategic combination of multiple techniques to find the most optimal one.99,101,171 Furthermore, future studies should aim to reduce the operating cost of the proposed methodologies and developing accessible and user-friendly technologies based on them such as wearable biosensors. 213 Considering the rapid pace of advancements in the field of skin cancer and our deepening comprehension of underlying molecular mechanisms behind cancer proliferation and drug resistance, it is reasonable to predict that skin cancer management would become more effective and better understood in near future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data will be available upon request.