
Abstract
Background
Acral lentiginous melanoma is associated with worse survival than other subtypes of melanoma. Understanding prognostic factors for survival and recurrence can help better inform follow-up care.
Objectives
To analyze the clinicopathologic features, melanoma-specific survival, and recurrence-free survival by substage in a large, multi-institutional cohort of primary acral lentiginous melanoma patients.
Methods
Retrospective review of the United States Melanoma Consortium database, a multi-center prospectively collected database of acral lentiginous melanoma patients treated between January 2000 and December 2017.
Results
Of the 433 primary acral lentiginous melanoma patients identified (median [range] age: 66 [8–97] years; 53% female, 83% white), 66% presented with stage 0–2 disease and the median time of follow-up for the 392 patients included in the survival analysis was 32.5 months (range: 0–259). The 5-year melanoma-specific survivals by stage were 0 = 100%, I = 93.8%, II = 76.2%, III = 63.4%, IIIA = 80.8%, and IV = 0%. Thicker Breslow depth ((HR) = 1.13; 95% CI = 1.05–1.21; P < .001)) and positive nodal status ((HR) = 1.79; 95% CI = 1.00–3.22; P = .050)) were independent prognostic factors for melanoma-specific survival. Breslow depth ((HR = 1.13; 95% CI = 1.07–1.20; P < .001), and positive nodal status (HR = 2.12; 95% CI = 1.38–3.80; P = .001) were also prognostic factors for recurrence-free survival.
Conclusion
In this cohort of patients, acral lentiginous melanoma was associated with poor outcomes even in early stage disease, consistent with prior reports. Stage IIB and IIC disease were associated with particularly low melanoma-specific and recurrence-free survival. This suggests that studies investigating adjuvant therapies in stage II patients may be especially valuable in acral lentiginous melanoma patients.
Introduction
Acral lentiginous melanoma (ALM) is a subtype of melanoma predominantly occurring on palmar, plantar, and subungual skin. Though only accounting for 2–3% of all melanomas, ALM disproportionately affects African American, Hispanic, and Asian populations.1,2 It is the most common subtype in those with darker skin types and needs to remain a significant diagnostic consideration in these individuals.1,3
The prognosis of patients with ALM is worse compared to patients with non-acral melanoma. 1 It has been suggested that decreased survival may be due to a delay in diagnosis, leading to increased tumor thickness and advanced stage at presentation.1,3-12 The later stage at diagnosis may be due to initial misdiagnosis, atypical location compared to superficial spreading melanoma, unusual presentation, or delay in seeking care.1,3 However, recent studies have suggested that ALM patients may not necessarily present at a later stage than non-ALM patients. 13 Additional possibilities for survival disparities include genomic differences between ALM (likely non-ultraviolet (UV)-induced) and cutaneous melanoma (UV-induced). 14 The exact cause of the poor prognosis associated with ALM therefore remains unknown.
A thorough description of the diagnostic, management, and recurrence patterns may uncover key features that help explain the poor survival associated with ALM. Unfortunately, many previous studies examining ALM prognosis have been limited by small sample sizes and/or ethnically homogenous populations (i.e., exclusively in Japanese or Caucasian patients) in single-institution cohorts,3,7-12 and the few larger cohort studies have not examined recurrence patterns.1,5,6 In this study, we used a large, multi-institutional melanoma database to not only characterize the presenting clinicopathologic features and recurrence patterns of ALM, but also analyze melanoma-specific survival (MSS) and recurrence-free survival (RFS) by pathologic American Joint Cancer Committee (AJCC) eighth ed. stage and substage, which highlights important prognostic features when caring for patients with ALM.
Methods
The United States Melanoma Consortium database, a prospectively collected database from six institutions (New York University Langone Health, Moffitt Cancer Center, Emory University, Oregon Health and Science University, University of Alabama Birmingham, and Duke University), was used to perform a retrospective study of 433 patients with primary ALM managed surgically at one of the above institutions between January 2000 and December 2017. Patients who presented with recurrent ALM were excluded. All institutions received approval for this study and waiver of consent from their respective institutional review boards (Emory IRB#00101435)
Data collected included demographics, comorbidities, clinical characteristics, diagnostic work-up, histopathology of final excision specimen, postoperative outcomes, systemic treatment/radiotherapy, disease recurrence and survival data. All tumors underwent wide local excision with margins based on National Comprehensive Cancer Network (NCCN) guidelines. 15 Pathologic TNM stage was used to reclassify patients based on AJCC eighth edition staging. 16 Survival time was calculated as months between date of surgery and date of last follow-up or death. Follow-up included clinical exams with the surgeon, oncologist, and/or dermatologist and surveillance imaging at the discretion of the treating physician. Forty-one patients with inadequate details on pathologic stage or date of surgery were excluded from survival analyses. Of the patients included, substage could not be determined for two of the stage II patients.
Clinical characteristics analyzed included age, sex, patient-reported race, and location of lesion. Race was included to determine whether or not it is a prognostic factor for survival. Histopathologic characteristics analyzed included AJCC eighth edition stage, Breslow thickness of final specimen, presence of ulceration, presence of mitoses, and lymph node status. Five-year MSS and RFS rates and curves were generated using the Kaplan–Meier method. Melanoma-related deaths were determined based on review of death certificates, inquiry to patient’s treating physicians, known stage IV disease resulting in multisystem organ failure, or documentation of hospice care for advanced melanoma. Recurrence was defined as detection of disease in patients whom had no residual disease following intervention. For stage III disease, patients who had undergone completion lymph node dissection (CLND) were considered to be without residual disease; those who had not undergone CLND were assumed to have no residual disease after sentinel lymph node biopsy (SLNB) unless otherwise documented, as data shows that only 11.5% of these patients have residual disease. 17 Stage IV patients were excluded from RFS analysis. Univariate Cox regression model was used to determine if any of the clinicopathologic characteristics were associated with MSS or RFS. Proportional hazards assumption was tested using Kaplan–Meier curves and time-dependent covariate Cox regression models Characteristics significant (P value <.05) on univariate analysis were included in the multivariable Cox proportional hazards model to identify prognostic factors. Data analysis was performed using SPSS software (IBM Inc. Armonk, NY).
Results
Clinicopathologic Characteristics
Clinical and Histopathologic Characteristic.

aUlceration status was not required to stage 30 patients; substage could not be determined for two patients; ulceration status from biopsy was used to stage the remaining ten patients.
Melanoma-Specific Survival by Stage
The median time to follow up for the 392 patients included was 32 months (range 0–259) Overall 5-year MSS was 78.1% (Figure 1) and by stage were stage 0 = 100%, stage I = 93.8%, IA = 94.2%, IB = 93.4%, II = 76.2%, IIA = 96.8%, IIB = 73.2%, IIC = 63.2%, III = 63.4%, IIIA = 80.8%, IIIB = 79.5%, IIIC = 56.5%, IIID = 44.4%, and IV = 0% (Table 2). The percent of melanoma-related deaths that occurred within 3 years after surgery were 9.1% for stage IIB, 40% for IIC, 25% for IIIA, 66.7% for IIIB, and 89.5% for IIIC. All but 2 stage IIB and IIC patients had sentinel lymph node biopsies performed. Kaplan–meier curves for 5-year melanoma-specific survival stratified by pathologic AJCC eighth edition stage (A) and substage (B) and for 5-year recurrence-free survival stratified by stage (C) and substage (D). Melanoma-Specific Survival and Recurrence-Free Survival Rates by AJCC Eighth Edition Stage and Substage. aSubstage could not be determined for two stage II patients; Abbreviations: MSS—Melanoma-Specific Survival, CM—Cutaneous Melanoma, RFS—Recurrence-Free Survival.

Recurrence-Free Survival by Stage
Eight additional patients were excluded due to unknown date of recurrence (n = 1) or because they had residual disease following intervention (n = 7). Overall 5-year RFS rate for the 384 included patients was 62.8% (Figure 1) with a median time to recurrence of 23 months (range: 0–54 months). For patients with recurrence who experienced death, median time to recurrence was 15 months (range: 0–71 months) and median time between detection of recurrence and death was 16 months (range: 1–142 months). The 5-year RFS was stage 0 = 100%, stage I = 90.3%, IA = 90.7%, IB = 89.7%, II = 50.1%, IIA = 67.8%, IIB = 45.0%, IIC = 38.3%, III = 38.2%, IIIA = 55.7%, IIIB = 50.2%, IIIC = 33.4%, IIID = .0% (Table 2).
Site of First Recurrence by AJCC Eighth Edition Substage.

Cox Proportional Hazards Survival Analysis
Cox Proportional Hazards Model for Melanoma-Specific Survival and Recurrence-Free Survival (Univariate Analysis).

aIncludes patients who had sentinel lymph node biopsy performed or had clinically palpable lymph nodes (n = 314).
bContinuous variable.
Cox Proportional Hazards Model for Melanoma-Specific Survival and Recurrence-Free Survival (Multivariate Analysis)a.
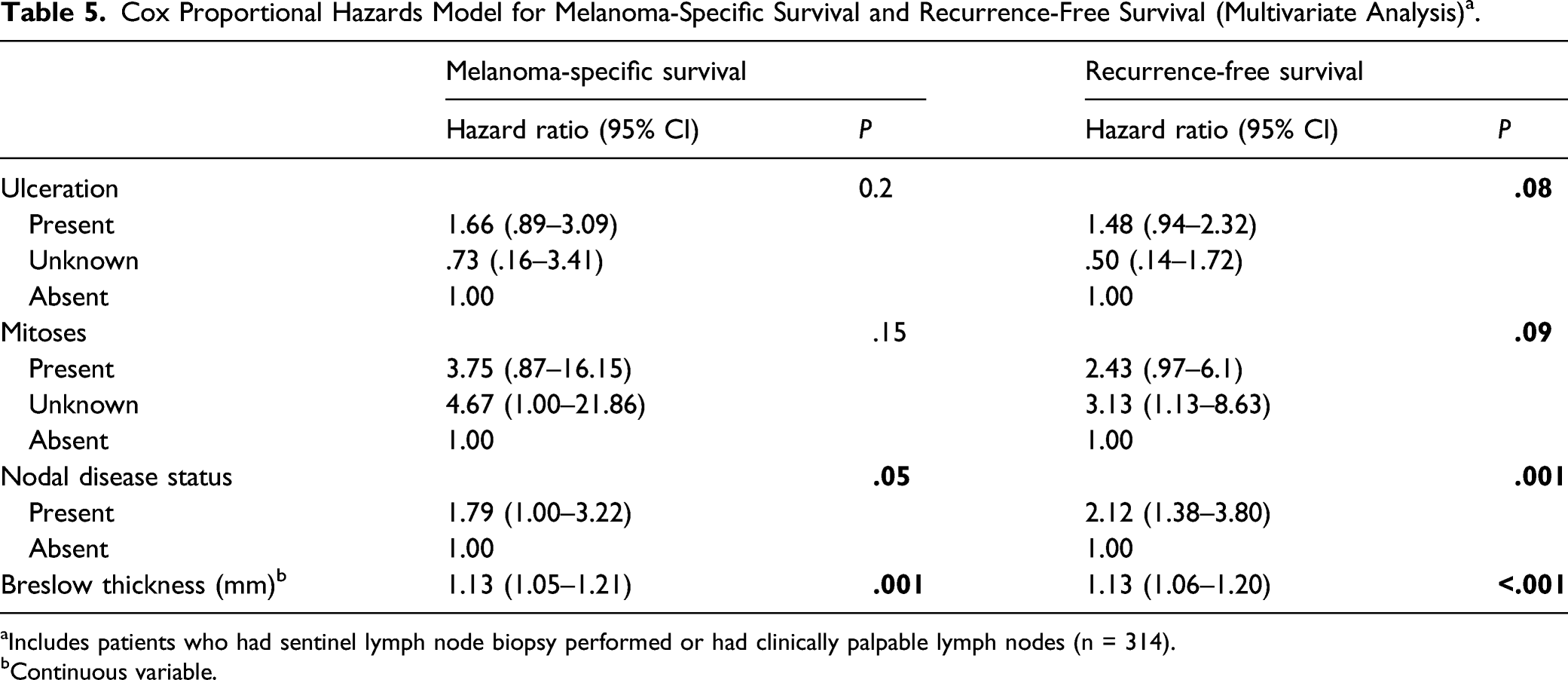
aIncludes patients who had sentinel lymph node biopsy performed or had clinically palpable lymph nodes (n = 314).
bContinuous variable.
Discussion
Acral lentiginous melanoma is a rare subtype of melanoma, and survival outcomes are significantly worse when compared to other cutaneous melanomas. 1 To date, most studies characterizing ALM have been limited in sample size and ethnic diversity.3,7-12 In this study, we utilized a large, multi-institutional database to perform an in-depth analysis of ALM diagnosis, management, recurrence patterns, and survival characteristics, which highlights unique ALM stage and substage features that have the potential to identify patients at risk for recurrence and improve outcomes.
Similar to other studies, our study highlights that ALM is associated with advanced age and plantar location.3,6,7,11,13 Most primary tumors were >1.0 mm (74%) and had mitoses present (61.0%). Histologic ulceration was present in 35.1 and 26.5% had at least one positive node. Tumor thickness was an independent prognostic factor for MSS, which is consistent with prior ALM series.6,13,18 A majority (72%) of our cohort presented with localized (AJCC eighth edition stage 0 to II) disease. In two recent single-institution cohort studies, Bello et al. 13 reported that 71% of patients with non-acral melanoma on the extremities presented with localized disease, and Wada et al. 7 reported this proportion to be 63%, suggesting that ALM patients may not necessarily present at a later stage than non-ALM patients.
In contrast to the survival patterns in overall cutaneous melanoma, 16 stage I disease in our cohort was associated with excellent outcomes while stage II was not, suggesting that early stage disease may not necessarily be associated with good prognosis. The trends in our 5-year MSS by stage are consistent with prior reports of ALM patients (Table 2).1,13,16 In Bradford et al. 1 ’s population-based analysis of the Surveillance, Epidemiology, and End Results (SEER) registry, they additionally found that after controlling for AJCC stage, survival rates for ALM patients were lower compared to non-ALM patients in stage II and III patients. This suggests that the poorer survival of ALM compared to non-ALM is independent of stage, and further highlights that the worse prognosis in ALM may not be entirely due to advanced disease at presentation. It has been hypothesized that distinct genetic alterations as well as socioeconomic disparities may also contribute to survival differences. 5 ALM is genetically distinct in that BRAF mutations have been reported less frequently compared to melanoma that occurs on sun-exposed skin.19,20 ALM also has a lower mutation burden compared to melanoma on UV-exposed skin, and thus, fewer actionable targets. 21 Studies have also found that ALM more frequently has KIT mutations than non-acral cutaneous melanomas (36 vs 28%, respectively). 22 However, the relationship between these variations in molecular pathways and prognosis remains poorly understood. Because patients with darker skin comprise a greater proportion of ALM cases compared to non-acral cases, socioeconomic disparities may also play a role. 23 In a more recent analysis of the SEER database, Huang et al. 5 found that non-Hispanic Whites had the highest survival and Blacks had the lowest. After stratifying by stage, this difference in survival remained significant in stage I and stage III patients. In our cohort, the majority of patients were white (83%), which is consistent with the racial distribution of the SEER database. Although race was not a prognostic factor for MSS in our cohort, understanding the underlying socioeconomic factors of such health disparities warrants further investigation.
In overall cutaneous melanoma, stage IIB and IIC MSS is better than or similar to stage IIIB MSS. 16 In contrast, stage IIB/IIC patients had worse 5-year MSS and RFS compared to IIIB patients in our cohort. In addition, our 5-year RFS for stage IIB (45%) and IIC (38%) were lower than the rates reported by Lee et al. 24 in a survival analysis of stage II cutaneous melanoma (62 and 53%, respectively). Although we found that many of the first sites of recurrence were in transit/satellite in stage IIB (21%) and IIC (46%) patients, we do not have data on subsequent sites of tumor spread, and it is likely that many of these patients initially presented with locoregional recurrences and later developed distant metastases, contributing to poor survival rates. This underscores that, in the absence of nodal disease, higher T category is associated with worse outcomes in ALM, especially given that Breslow thickness was found to be a prognostic factor on the multivariable model. Due to the aforementioned unique molecular and genetic characteristics of ALM, it has been postulated that these tumors may present with more aggressive vertical growth phases,3,13 as supported by the high median tumor thickness of 1.7 mm in this cohort. Thus, stage IIB and IIC may have locally invasive tumors with high metastatic potential.
These recurrence patterns should be considered when tailoring surveillance strategies for ALM, particularly for patients who are stage IIB and higher. Current recommendations for melanoma follow-up are limited by a lack of prospective, randomized trials, resulting in surveillance strategies that vary widely. 25 Guidelines for ALM-specific surveillance strategies are further limited by the low prevalence of this melanoma subtype. The NCCN guidelines for stages IIB-IV cutaneous melanoma recommend a history and physical exam with emphasis on the skin and lymph nodes every 3–6 months for 2 years, then every 3–12 months for 3 years, then annually. 15 In one of the few prospective studies on melanoma surveillance, Garbe found that almost 50% of stage II and III recurrences were detected by clinical exam. 26 Given that the most common first site of recurrence for stage IIC (48%), IIIB (78%), and IIIC (33%) patients in our cohort was satellite/in-transit, our findings further support the importance of the clinical exam in stage II and III ALM patients. The NCCN guidelines also recommend considering imaging for up to 5 years to screen for recurrence and metastases for patients with stage IIB-IV cutaneous melanoma. 15 For stage IIB ALM patients, examination and imaging of the lymph nodes may be particularly important given that 53% of patients with recurrence presented with regional nodal metastasis in our cohort. In addition, a majority of recurrences in stage IIB and higher occurred within 5 years (95% for stage IIB, 100% for stage IIC, and 95% for stage III), suggesting that the timeline recommended by the NCCN for radiologic follow-up of cutaneous melanoma patients is appropriate for ALM as well.
These recurrence and survival patterns should also be taken into account when determining the need for adjuvant therapy. Immunotherapy has been shown to improve progression-free survival and overall survival in patients with metastatic melanoma.27,28 While 41% of all patients in our cohort were treated prior to availability of currently utilized immunotherapies, many of the stage III and IV patients would be considered for immunotherapy if treated in the present. However, these therapies would not be indicated for stage II patients even if they were treated today. Given the worse 5-year MSS and RFS in stage IIB/IIC patients compared to stage IIIB, ALM patients may especially benefit from current clinical trials investigating the survival benefit of immunotherapy and targeted therapy in stage II disease (KEYNOTE-716). 28 Furthermore, given that ALM patients are often underrepresented in clinical trials and may respond to immunotherapy differently than other cutaneous melanomas, it is important that they be included in current and future trials. 29
Because this study is a retrospective review of prospectively collected data, it is limited by not having full data on other variables that may impact recurrence and survival, such as socioeconomic factors, time between lesion onset and presentation, and date of diagnosis. We also did not have full data on the frequency and types of surveillance imaging utilized, which could help further inform surveillance strategies. In addition, 47.8% of patients were lost to follow-up prior to the date of final data collection, resulting in a median time to follow up of only 32 months, and thus, our Kaplan–Meier estimates may underestimate the long-term risk of recurrence and death. In addition, the majority of our cohort was white, which may limit the applicability of these findings in non-white patients. Finally, because we are comparing our survival data to the much larger AJCC dataset, there is a chance of type I error; however, given the rarity of this subtype, it is unavoidable.
Conclusion
We present a large multi-center substage survival analysis of primary ALM patients. Patients with early stage disease (i.e., stage II patients) were associated with poor outcomes, consistent with prior cohort studies. The particularly low RFS and MSS rates in stage IIB/IIC patients compared to stage IIIB disease suggests that increased thickness is associated with worse outcomes, even in the absence of nodal metastases, and highlights that studies investigating adjuvant therapies in stage II cutaneous melanoma patients may be particularly valuable for ALM. Furthermore, the timing and sites of recurrence support the utilization of current cutaneous melanoma surveillance strategies for ALM patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The NYU Langone Health melanoma database is supported in part by a Melanoma SPORE grant (P50 CA225450). The authors otherwise received no other financial support for the research, authorship, and/or publication of this article.
Ethical approval
This Study and waiver of consent were Approved by the respective institutional review boards of All collaborating institutions (NYU Langone, Moffitt Cancer Center, Emory University, Oregon Health & Science University, University of Alabama Birmingham, and Duke University, Emory IRB#00101435).