
Abstract
Introduction
Ovarian cancer (OC) poses significant challenges due to its high mortality rate, particularly in advanced stages where symptoms may not be evident. DNA repair mechanisms, including nucleotide excision repair (NER), are crucial in maintaining genomic stability and preventing cancer. This study focuses on exploring the role of two NER-related genes, Xeroderma Pigmentosum Complementation Group C (XPC) and DNA Damage Binding Protein 2 (DDB2), in OC susceptibility.
Objectives
This study aims to investigate the association between variations in two NER-related genes, XPC rs2228001 and DDB2 rs830083, among a cohort of Turkish individuals with OC and control subjects.
Methods
Genotyping of XPC rs2228001 and DDB2 rs830083 was performed on 103 OC patients and 104 control subjects from the Turkish population using the Fast Real-Time 7500 PCR platform from Applied Biosystems.
Results
Individuals with the homozygous AA genotype of XPC rs2228001 exhibited a reduced likelihood of developing OC (OR 0.511; 95% CI 0.261 - 1.003; P-value 0.049), whereas those with the CC variant faced an elevated risk (OR = 2.32, 95% CI = 1.75-3.08; P-value 0.035). The presence of the A allele was associated with decreased OC occurrence (P-value = 0.035). Similarly, for DDB2 rs830083, individuals with the homozygous CG genotype had a diminished risk of OC (P-value 0.036), compared to those with the GG polymorphism (OR 1.895; 95% CI 1.033 - 3.476; P-value 0.038). Furthermore, the presence of the C allele was associated with a 1.89-fold decrease in the likelihood of OC.
Conclusion
These findings shed light on the genetic factors influencing OC susceptibility, emphasizing the importance of DNA repair systems in disease. Further research in larger and more diverse populations is warranted to validate these findings, facilitating precise risk assessment, and potentially guiding tailored treatment strategies for OC patients.
Plain Language Summary
Ovarian cancer is a serious disease with a high mortality rate, especially in its advanced stages when symptoms are often not obvious. Our cells have mechanisms to repair DNA damage and maintain stability in our genetic material. Two genes involved in one of these repair mechanisms, called nucleotide excision repair (NER), are Xeroderma Pigmentosum Complementation Group C (XPC) and DNA Damage Binding Protein 2 (DDB2). This study investigates how variations in these genes may influence the risk of developing ovarian cancer. Understanding these genetic factors could lead to improved methods for diagnosing and treating this challenging disease.
Keywords
Introduction and Purpose
Cancer is the most prevalent cause of death in many regions of the world.1,2 Among reproductive cancers affecting women, ovarian cancer (OC) has the highest fatality rate. 3 As a result, it ranks fifth as a leading cause of death among women in general. 4 Due to its minimal symptoms, OC is frequently known as the “silent killer” 5 for that 75% of females with OC have advanced disease with stages III and IV, and 25% of these patients can survive for 5 years. 6 Factors such as increased estrogen exposure, inflammatory diseases, hormone replacement therapy, smoking, metabolic abnormalities, and obesity can all elevate the risk of ovarian cancer.7-9 Additionally, genetic mutations and a family history of the disease are among the most significant risk factors for its development. 9
Nucleotide excision repair (NER) has the capacity to identify and repair different types of DNA damage caused by factors such as radiation, as well as bulky DNA adducts generated by exposure to environmental mutagens or chemotherapy treatments. 10 NER consists of two sub-routes, which are global genomic repair (GGR) and transcription-coupled repair (TCR).10,11 GGR contains different types of genes, such as xeroderma pigmentosum (XPC) and DNA damage binding protein 2 (DDB2). 12 XPC plays a crucial role in global genome repair (GGR) by recognizing DNA damage and initiating the repair mechanism.12,13 Additionally, DDB2, a significant component of the DNA repair process, is recruited to the damaged site. These genes interact with other GGR components to initiate the repair process, such as correcting damage caused by ultraviolet radiation (UV), thus preventing the accumulation of mutations and the onset of cancer.12,14
The XPC rs2228001 variant causes a missense mutation, leading to the substitution of Lysine (Lys) with Glutamine (Gln) this alteration may potentially impact the structure, function, or stability of the XPC protein, which could in turn influence various cellular processes or disease susceptibility such as OC. 15 While the DDB2 rs830083 variant is located in an intron, potentially affecting gene expression through mechanisms such as splicing efficiency, mRNA stability, and gene regulation. 16 Despite the potential importance, the exact molecular mechanism responsible for the effects of DDB2 rs830083 remains unknown. Further investigation, particularly in the realm of OC, is required to better comprehend its functional implications. Currently, there is a lack of research on the association between these two SNPs and OC susceptibility. Therefore, the present study aimed to investigate the relationship between polymorphisms of rs2228001 and rs830083 in XPC and DDB2 the susceptibility to OC in the Turkish population.
Materials and Methods
The nature of the study involved utilizing a case-control design to explore the relationship between variations in two nucleotide excision repair (NER)-related genes, namely Xeroderma Pigmentosum Complementation Group C (XPC) rs2228001 and DNA Damage Binding Protein 2 (DDB2) rs830083, and the susceptibility to ovarian cancer (OC). This marks the initial investigation into the correlation between DDB2 rs830083 and OC.
Study Subjects
Slovin’s, Krejcie’s, and Margon’s formulas were utilized to determine the sample size for the study. The sample size was collected as a hospital-based study. Both the patient and control groups consisted entirely of individuals of Turkish descent (Caucasians) from the same geographical region in Turkey. The patient group comprised 103 participants diagnosed with OC by Obstetrics and Gynecology specialists at Yeditepe University Hospital in Istanbul, while the control group included 104 healthy individuals. All participants were aged 18 and above. During the interview process, each participant completed a structured questionnaire covering demographic information, cancer history, menopausal status, and reproductive history. Subsequently, approximately 5 mL tubes containing EDTA of venous blood were collected from each participant. These samples were then stored in a refrigerator at 4°C until DNA isolation was initiated, typically within a timeframe ranging from 3 to 7 days. The study received approval from the Ethics Committee of Yeditepe University, with a registration number of 2426 for the Clinical Research Ethics Committee (KAEK) application file. The study underwent examination by the Ethics Committee during a meeting on 08.06.2022, where it was determined to be both ethically and scientifically appropriate to conduct (KAEK Decision No: 1621).
DNA Isolation From Blood
Genomic DNA was extracted from a 350 μL blood using the iPrep PureLink gDNA blood kit and the iPrep purification instrument (Thermo Fisher Scientific – SA). This instrument utilizes magnetic bead isolation principles, where positively charged magnetic beads form an ionic bond with the negatively charged DNA backbone at low pH values. Consequently, proteins and other impurities remain unbound and are eliminated by a liquid wash buffer.
DNA Quantitation and Purification
The DNA concentration and quality were evaluated utilizing a Nanodrop spectrophotometer (ThermoScientific, United States). Measurements were conducted at wavelengths of 260 nm and 280 nm, with the optical density (OD) ratio (A260/A280) automatically calculated. A standard purity threshold of 1.8-2.0 for the OD ratio was employed. Ratios below 1.8 indicated protein contamination, while ratios exceeding 2.0 suggested contamination by chloroform, phenol, or other organic compounds.
SNP Genotyping
The Applied Biosystems TaqMan SNP Genotyping Assay Sets are composed of predetermined selections of pre-designed and customized TaqMan SNP Genotyping Assays sourced from publicly available databases and scientific literature.
The Primer and Probe Sequences for TaqMan Assay.

The Mixtures of Real-Time PCR Reaction.

Statistical Analysis
Statistical analyses were performed using SPSS software, version 27, a t-test was employed to compare the mean age between cases and controls. The genotype frequencies for individual markers were compared between patients and control subjects using the Chi-square test. Odds ratios (OR) were estimated along with their corresponding 95% confidence intervals (95% CI), and statistical significance was defined as P < 0.05.
Results
Demographic Characteristics
Demographics of Ovarian Cancer Patients and Healthy Participants.

(n: number of samples
There was a significant difference in the distributions of smoking (P < 0.0001) and alcohol consumption (P < 0.0005). However, there were no statistical differences in the distributions of age and family history of cancer between the OC patients and controls (P = 0.582 and 0.412, respectively). Nevertheless, there were more postmenopausal (79.5% vs 17.4%), number of parities more than one (72.7% vs 43.5%), and number of pregnancies more than one (77.3% vs 43.5%) in the OC patients than that in the controls.
Clinical and Treatment Characteristics of Patients.

n: number of samples,
Associations Between DDB2 and XPC Genotypes and OC Risk
DDB2 Genotype and Allele Distribution in Patient and Control Groups.

XPC Genotype and Allele Distribution in Patient and Control Groups.

Statistical Evaluation of Real-Time PCR Results
The allelic discriminations in our study were automatically assessed using the software of the 7500 Fast-Real-Time PCR Instrument. The fluorescence irradiation readings and interpretations were based on the dyes present in the probes. Specifically, the FAM dye appeared as blue in both figures, while the VIC dye exhibited a red color. While the green dots represent markers showing heterozygous genotypes. The ROX dye serves as a reference color in the instrument’s software. Its primary function is to facilitate background removal, which is essential for ensuring the accurate operation of the instrument during allelic discrimination analysis. However, it is important to note that for certain samples, discrimination between alleles could not be achieved. In such cases, the Thermo Fisher Cloud platform was utilized to determine the undetermined samples. Our experiment was conducted multiple times for both patient and control samples. Figures 1 and 2 illustrate some of the analyses of allelic discrimination through the examination and interpretation of radiance curves. Allelic discrimination analysis of DDB2 genotypes (GG, CG, and CC). Allelic discrimination analysis of XPC genotypes (AA, CA, and CC).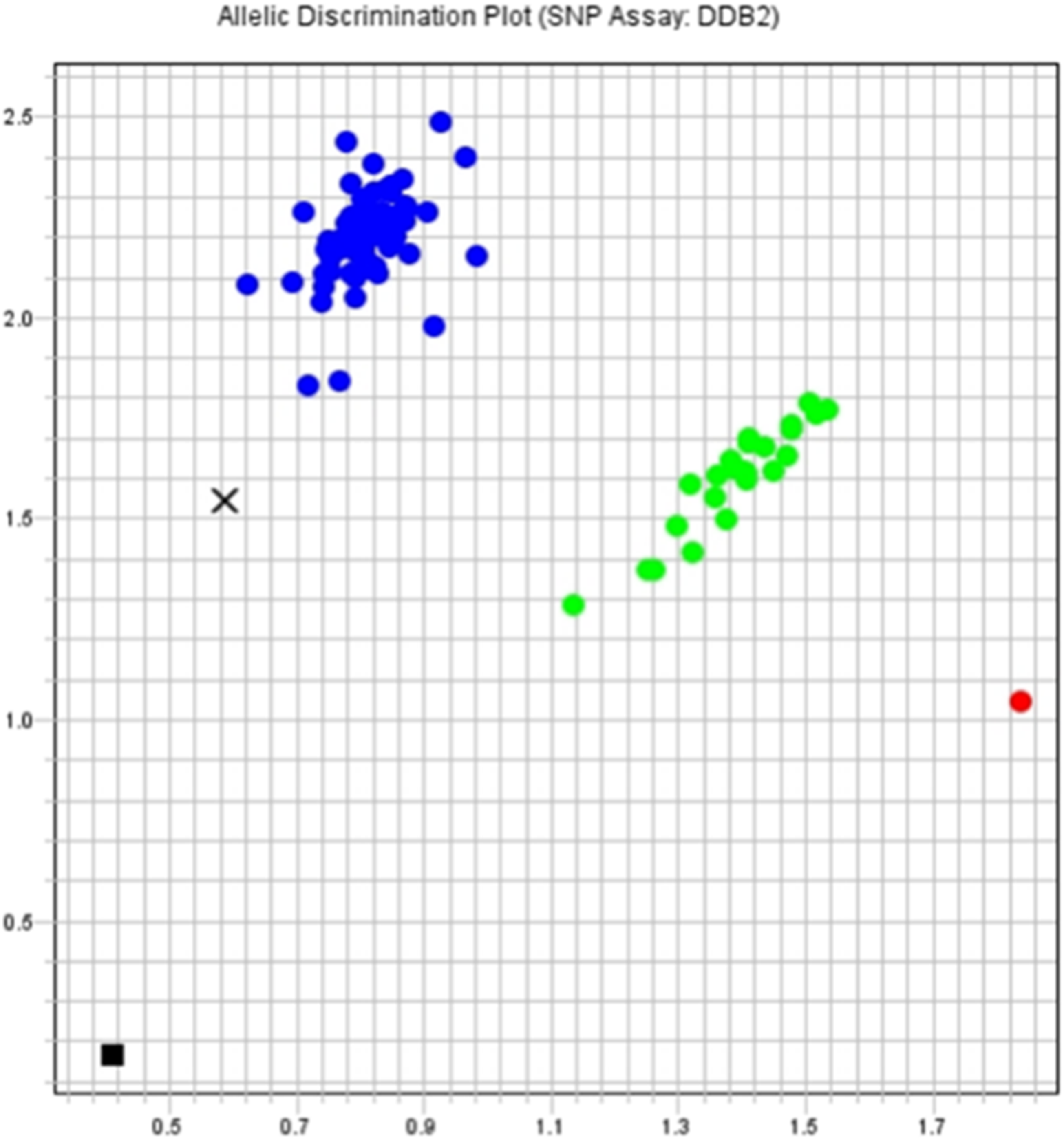

Discussion
In the context of our investigation into the association between variations in two nucleotide NER related genes and OC susceptibility among Turkish individuals, it is essential to recognize the limitations inherent to the case-control study design. Given the retrospective nature of our study, potential biases such as selection bias and recall bias may have influenced our results. Selection bias arises from the non-random selection of cases and controls, potentially leading to a lack of representativeness and affecting the validity of our findings. Similarly, recall bias, stemming from differential recall of past exposures or experiences between cases and controls, may introduce systematic errors and impact the accuracy of the reported data. Moreover, while our study provides insights into the genetic factors influencing OC susceptibility in the Turkish population, the generalizability of these findings to broader populations may be limited. Therefore, future research endeavors should address these limitations by conducting studies in larger, more diverse populations to ensure the validity and applicability of the findings. Additionally, our study encountered unbalanced sample sizes, with 103 patients compared to 104 controls. This disparity arose due to limitations in the number of ovarian cancer patients willing to share their data through our questionnaire. Furthermore, the collection of our samples as subgroups was challenging due to differences among participants, such as age and other factors, which presented logistical limitations. Lastly, our study would benefit from investigating family history of colorectal cancer, endometrial cancer, HNPCC, and breast cancer, as these are closely related to ovarian cancer development. By acknowledging and addressing these limitations, researchers can advance our understanding of OC etiology and pave the way for the development of more effective treatment strategies tailored to specific populations.
OC is the eighth most fatal disease among women and is considered one of the deadliest forms of cancer affecting women.17-19 Epithelial OC is the most lethal cancer affecting the female reproductive system, particularly highly serous tumors. 20 Our study revealed that (90%) of OC had epithelial tumors. Our findings are consistent with previous research, as (54.8%) of OC patients in our study were diagnosed at advanced stages (III or IV), largely due to the nonspecific nature of OC symptoms that are often mistaken for common female discomforts. 21 Several factors contribute to the development of OC, with smoking identified as a statistically significant risk factor in our research. Among OC patients, smoking was more prevalent (82.2%) compared to the healthy group (55.3%). 22 Additionally, a significant association was observed between OC development and individuals with a familial history of the disease. In our study, most patients (64.2%) had no cancer history in their family, while (35.8%) had a history of cancer in their family. Despite the increased risk associated with a family history of OC, a substantial proportion of OC cases occur in individuals without such a history, possibly due to the limited number of participants in our study. 23 Furthermore, elevated levels of circulating androgens and menopausal hormonal therapy may increase OC risk, as evidenced by the majority of our participants (79.5%) being in the postmenopausal phase. 24
Our study aimed to examine the genetic correlation between OC susceptibility and two SNPs found in genes associated with the NER pathway, namely XPC and DDB2.
XPC rs2228001 (Lys939Gln) at exon 16, which has been implicated in various cancer types. Our study represents the first attempt to explore the potential link between XPC rs2228001 and OC within the Turkish population. The analysis revealed that individuals carrying the homozygous AA genotype at the XPC gene exhibited a reduced OC risk (OR 0.511; 95% CI 0.261 - 1.003), while those with the CC polymorphism had an elevated OC risk (OR 1.980; 95% CI 1.044 - 3.754) with a significant (P-value = 0.035). Additionally, the A allele was significantly associated with a reduced OC risk (P-value = 0.035), potentially reducing the risk by 1.9 times. Our findings align with previous research, particularly a study by Zhiguang Zhao in the Chinese population, which indicated that individuals with the rs2228001 CC/AC variant genotype had an increased OC risk compared to those with the AA variant genotype (adjusted OR = 1.72, 95% CI = 1.02-2.92, P-value = 0.043). 25 Several studies have linked the XPC rs2228001 intron 11 splice acceptor site polymorphisms to increased exon 12 skipping and decreased DNA repair capacity in the context of colorectal cancer. 26 Additionally, this polymorphism leads to a missense variant at position 939, specifically involving a lysine to glutamine substitution. 27 Emerging evidence suggests that the XPC 939 alteration is associated with a higher frequency of p53 mutations in breast cancer. 28 Future investigations delving into the XPC rs2228001 intron and its influence on gene expression in the context of OC may yield valuable insights for further studies and clinical outcomes.
In contrast, the DDB2 rs830083 variant, considered an intron variant with associations in various cancer types, was explored for its potential link to OC within the Turkish population, marking the first investigation of its kind. Notably, no prior studies have proposed a direct relationship between DDB2 rs830083 variants and OC risk. The individuals carrying the homozygous CG genotype at the DDB2 gene exhibited a reduced OC risk (OR 0.521; 95% CI 0.282 - 0.961). Conversely, those with the GG polymorphism at the DDB2 gene faced an increased OC risk (OR 1.895; 95% CI 1.033 - 3.476) with (P-value of 0.038. Additionally, the presence of the C allele was significantly associated with a decreased OC risk (P-value = 0.038), potentially reducing the risk by 1.89 times.
In a prior study, it was observed that individuals with the DDB2 rs830083 GG genotype had a significantly higher risk of gastric cancer compared to those with the wild-type CC genotype (OR = 2.32, 95% CI = 1.75-3.08). 29 Another study focusing on DDB2 rs830083 and lung cancer found that the CG and GG genotypes were associated with a substantially increased risk of lung cancer compared to the rs830083 CC genotype. 30 These findings suggest that the DDB2 rs830083 variation may influence alternative splicing patterns, impacting gene transcription regulation and, in turn, affecting the activity of certain proteins involved in the NER pathway. 31 Altered NER capacity could affect the frequency of DNA mutations resulting from unrepaired damaged DNA. Some studies propose that specific DDB2 variations, including rs830083, may influence the function of p53, potentially affecting DNA repair pathways. 32 Additionally, DDB2 rs830083 has been identified as a potential biomarker in various investigations, indicating a potential haplotype inheritance with neighboring variants. 30 Despite its potential significance, the precise molecular mechanism behind the actions of DDB2 rs830083 remains unclear. Further research, especially in the context of OC, is needed to gain a better understanding of its functional implications.
Conclusion
In discussing the clinical implications of our study findings, it is essential to consider the potential implications for the diagnosis, treatment, and management of OC among Turkish individuals. Our investigation into the association between variations in two NER-related genes, XPC rs2228001 and DDB2 rs830083, has provided valuable insights into the genetic factors influencing OC susceptibility within this population. Specifically, our results indicate that individuals with certain genotypes, such as the homozygous AA genotype of XPC rs2228001 and the homozygous CG genotype of DDB2 rs830083, exhibit a reduced risk of developing OC. These findings underscore the importance of DNA repair mechanisms, particularly NER, in maintaining genomic stability and preventing cancer development. In a clinical setting, identifying individuals with these genetic variants may aid in risk assessment and potentially guide personalized treatment strategies for OC patients. Furthermore, our study highlights the need for further research in larger and more diverse populations to validate these findings and enhance our understanding of OC etiology, ultimately contributing to improved patient outcomes and healthcare practices. By elucidating the clinical implications of our study, we aim to bridge the gap between research and clinical practice, ultimately benefiting individuals affected by OC in the Turkish population.
Footnotes
Acknowledgments
I want to thank everyone who contributed to making this project a reality. First and foremost, I would want to express my gratitude to my co-authors for their tremendous contributions and teamwork throughout the research process. Their knowledge, ideas, and enthusiasm have significantly improved the quality and impact of this work. I am really grateful to Yeditepe University for supplying the necessary resources, facilities, and assistance to enable this research. The institutional infrastructure and academic environment were crucial in the design and implementation of this inquiry. I’d like to express my gratitude to everyone who provided me with advice, insight, and critical comments during the manuscript preparation and revision process. Their thoughtful comments and recommendations significantly improved this study. Also, I would like to acknowledge the valuable support of artificial intelligence tools used for rewriting and enhancing the writing throughout the research.
Author Contributions
Rukset Attar: Recruitment of study participants and clinical investigation, data collection. Assoc. Prof. Seda and Turgay İsbir: Contributed to the design and implementation of the research. Dorcas, Fatma Tuba Akdeniz, Betül Çapar Goralı: Performed the experiments. Sara: Contributed to the design and implementation of the research, performed the experiments and statistical analysis. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data generated in the present study may be requested from the corresponding author or Assoc. Prof. Seda Yılmaz.