
Abstract
The objective of this research was to determine if the engagement/participation in health promotion activities of cancer survivors in the United States (US) changed between 2006 and 2015. We pooled two independent cross-sectional data of cancer survivors using Medical Expenditure Panel Surveys from 2006 (N = 791; weighted N = 9,532,674) and 2015 (N = 1067; weighted N = 15,744,959). Health promoting activities consisted of past year influenza immunization, routine physical examination, and dental visit. Self-care included maintaining normal weight, not smoking, and engagement in recommended vigorous physical activity. We conducted unadjusted and adjusted logistic regression analyses to examine the change in engagement in health promoting activities over time. We found rates of annual influenza immunization (66.8% vs 70.3%), dental visit (71.8% vs 70.3%), and normal weight (33.9% vs 33.5%) did not change from 2006 to 2015. The percent with physical examination (90.8% vs 93.8%; P = .03) and non-smokers increased (87.9% vs 91.2; P = .04). Between 2006 and 2015, despite guidelines and recommendations for personalized cancer survivorship health plans, health promoting activities among cancer survivors did not change significantly.
Background
There is a positive trend in cancer survivorship in the United States (US): 10 million in 2006; 1 15.5 million in 2015; 2 and 16.9 million currently. It is expected that by 2030, there will be 22.1 million Americans who will have survived cancer. 3 While improvements in cancer treatment have increased the number of survivors, and guidelines for prevention, active monitoring, and management plans should be in place for their future care, little is known about the difference over time of survivors’ actual healthcare engagement in health promotion activities post-cancer treatment. 4
The emphasis to have healthcare engagement post-cancer treatment has been built upon the groundbreaking report From Cancer Patient to Cancer Survivors: Lost in Transition. 5 It helped to create a movement for preventive care for cancer survivors similar to health promotion activities (eg, exercise, smoking, alcohol, diet) that have been associated with prevention of noncommunicable diseases such as diabetes. 5
The importance of such ongoing health promoting activities and preventive care has resulted in several national guideline-setting organizations (such as the American Cancer Society (1), American Society of Clinical Oncology, and the National Accreditation Program for Breast Centers) to release guidelines for cancer survivorship. These contemporary guidelines address the unique physical, psychosocial, and spiritual issues of active treatment phase, post-treatment phase (ie, long-term effects), and late effects that may occur months or years after treatment ends. 6 They provide evidence-based recommendations that were not previously available.
Long-term cancer survivorship care involves providing specific health promotion activities for individuals in the heterogeneous survivorship population in terms of any on-going cancer treatment, post-cancer care, and managing co-existing comorbidities.7,8 In particular, the specialists are to focus upon preventive screenings, management of effects of cancer therapies, 9 and management of co-morbidities.
Additionally, within the previous decade, access to the long-term cancer survivorship care was extended through the Affordable Care Act (ACA) in 2010 where health insurance was available to millions who previously did not have access. With the access, it was possible to develop long-term cancer survivorship care programs that supported coordinated, patient-centered, cost-effective cancer care. 10
Also, since 2010, improvements in access to information, psychosocial support groups, and other resources have surged through the evolution of the internet and the use of web pages and applications (apps) for cell phones. Fox 11 and Brenner noted that 79% of caregivers had access to the internet, and of those, 88% looked online for health information. The expansion of the internet and social media offer several health promotion and disease prevention programs for cancer survivors such as e-EXCELS, a tool to support the needs of survivors to promote their health, 12 a cell phone app to promote exercise among older cancer survivors, 13 and an internet-based way to complete cancer survivorship plans. 14 There are many additional information resources available such as the National Cancer Institute (NCI) with its literature and downloadable information, the National Coalition for Cancer Survivorship (NCCS)’s Cancer Survival Toolbox, and the Lance Armstrong Foundation (LIVESTRONG) which offers a wide variety of information about cancer survivorship on its webpage and through printed materials. All of these resources have emerged over the past decade or so to support health and improve healthcare navigation of the people who have survived cancer.
With the improvements in clinical therapies, clinical guidelines, communication, and resources, it is important to determine if there has been a change in engagement in health promotion activities among people who have survived cancer. It would be expected that such advances as identified above would lead to increased preventive service utilization. Therefore, our primary objective was to assess the change of engagement/participation in health promotion activities among adults who have survived cancer in the US using data from a nationally representative survey of non-institutionalized civilian household members to examine changes in health care practices over time.
Methods and Design
Study Design
We used a cross-sectional cohort study design for this research. We pooled 2 independent cross-sections (2006 and 2015) of a nationally representative survey of non-institutionalized civilian population to analyze the change between the 2 periods of time with respect to engagement in health promotion activities among cancer survivors. This study was reviewed and approved as non-human subjects by the West Virginia University institutional review board # 2006045826.
Data Source
Data for this paper were retrieved from the Medical Expenditure Panel Survey (MEPS), a nationally representative survey of the US non-institutionalized civilian population. 15 MEPS has a household and an insurance component comprised of responses to large-scale surveys of families and individuals, their medical providers (eg, doctors, hospitals, pharmacies, etc.), and employers. The dataset has data on the specific health services use, frequency of that use, the cost of services, and how they are paid for, as well as data on the scope, and breadth of health insurance held by the individual respondents. MEPS data are used for evaluation of health care utilization, payment sources, demographics, and information about minority health.
Analytical Sample
We restricted our analytical sample to: (1) adults (age ≥21 years); (2) with cancer; (3) alive during the observation period; and (4) did not have any missing values on any of the health promotion activities measures. We additionally excluded 3 individuals who did not have any preventive care during the observation period. The final sample size consisted of 791 (2006) and 1067 (2015) adult cancer survivors.
Identification of Cancer Survivors
We defined cancer survivors as those who reported ever having been diagnosed with cancer of any type by a physician or other health professional using the survey question within MEPS. The MEPS respondents can report a medical condition as part of their healthcare utilization, disability days, or experiencing the condition. These conditions are recorded “verbatim” and converted to clinical classification codes (CCS) via the International Classification of Diseases, 9th Edition (ICD9). We used the CCS codes from 11 through 43 to identify cancer survivors.
Dependent Variables
The key dependent variables addressing health promotion activities included health practices related to seeking access to the healthcare system. The participants were queried as to if they had received an influenza immunization, dental examination, and medical examination within the past year. We classified these as health promotion activities and dichotomized them into categorical “yes, no” responses.
The key dependent variables addressing preventive, self-management practices were also dichotomized into categorical “yes, no” variables. These included maintaining a normal weight; not smoking; and recommendations for being physically active with vigorous exercise. Also, an additive, continuous variable was created for the cumulative number of preventive activities for the participant.
It should be noted that there was a change in the definition of physical activity used by MEPS researchers between 2006 and 2015. The cut-point for being physically active was endorsing at least 3 vigorous periods of physical activity per week in 2006. The cut-point for being physically active was endorsing at least 5 vigorous periods of physical activity in 2015. Although the results are reported, they should be used with caution. This is recognized as a study limitation and is addressed in the discussion section.
Key Independent Variable: MEPS Year 2006 Versus 2015
The key independent variable was time. Data from MEPS, Year 2006 was compared with data from MEPS 2015 to analyze changes over the 10-year period. This time period was selected as a previously published study analyzed trends in preventive care among cancer survivors during the period between 2000 and 2004. 16 The current report is an update that analyzed changes in preventive care between 2006 and 2015; year 2005 was not selected because MEPS follows individuals for a total period of 2 years. As we are interested in 10-year change, we focused on the period between 2006 and 2015. Additionally, although later years (2016, 2017, and 2018) are available, these years do not contain information on all the variables that we used (eg, BMI, dental check, flu shot). 17 The interview year MEPS 2006 was used as the reference year for the analyses.
Other Independent Variables
Other factors are known to influence engagement in health promotion activities in patients with cancer based upon the Krieger 18 Ecosocial Theory. In the model, individuals are the embodiment of their biological, societal, and lived experiences with multiple interplays of exposure, susceptibility and resistance based upon age, sex/gender inequality, race/ethnicity inequality, class inequality, household/group/area influences, and individual factors. Additional variables were based upon published literature. The independent variables included age (21–34 years; 35–44 years; 45–54 years; 55–64 years; 65–74 years; 75 years and older), sex (women/men), race/ethnicity (non-Hispanic white/African Americans/Hispanics/other racial minorities), marital status (married/widowed/separated and divorced/never married), education (less than high school/high school/some college/college), poverty status, health insurance coverage (private/public/uninsured), multimorbidity (2 or more conditions from a list of 17 conditions excluding cancer—Goodman framework 19 ), pain interference with normal activities (little/none/moderate/severe/extreme) perceived physical (excellent and very good/good/fair and poor) and mental health status (excellent and very good/good/fair and poor) and region (northeast, Midwest, south, West). Additionally, other chronic conditions are known to change the dynamics of health and health care; therefore, the Goodman framework was used to address these aspects of analysis. In the Goodman model, changes in the dynamics of health care, disease distribution, population growth patterns and similar risk factors are involved in chronic conditions. The Goodman conceptual model applies a standard classification scheme for chronic conditions to 5 national-level data systems 19 where the coding system for chronic conditions and data systems intersect are 20 conditions. Therefore, multimorbidity (2 or more of the Goodman conditions, excluding cancer) was included as an independent variable.
Additional variables were based upon published literature and epidemiological significance. The independent variables included: age (21–34 years, 35–44 years, 45–54 years, 55–64 years, 65–74 years, 75 years and older); sex (women, men); race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanics, other racial minorities); marital status (married, widowed, separated/divorced, never married); education (less than high school, high school graduate, some college, college degree and above); poverty status (poor, near poor, middle income, high income); health insurance coverage (private, public, uninsured); perceived physical (excellent/very good, good/fair, poor); mental health status (excellent/very good, good/fair, poor); level of pain interference in normal activities (none, little, moderate, severe, extreme); and, region (Northeast, Midwest, South, West).
Statistical Analyses
As MEPS involve complex survey design with clustering, strata and weights, all statistical analyses were conducted with SAS survey procedures. We conducted used Rao-Scott chi-square tests to examine the subgroup differences between 2006 and 2015 by not only patient characteristics but also health promotion activities. Further, we conducted separate multivariable logistic regressions for each of the binary dependent variables including normal weight; being physically active; not smoking; influenza immunization within the past year, routine physical examination within the past year, and dental visit within the past year. In these regressions, we controlled for age, sex, race/ethnicity, marital status, education, poverty status, health insurance coverage, multimorbidity, perceived physical and mental health, pain interference with normal activities and region. In regression models of health promotion activities (influenza immunization, physical examination and dental visit), we also included (body mass index categories (underweight or normal/overweight/obese), physical activity (3x or 5 times a week/other), and current smoking (yes/no) as independent variables.
Results
Profile of Adult (≥21years) Cancer Survivors in 2006 and 2015 Medical Expenditure Panel Survey, 2006 and 2015.
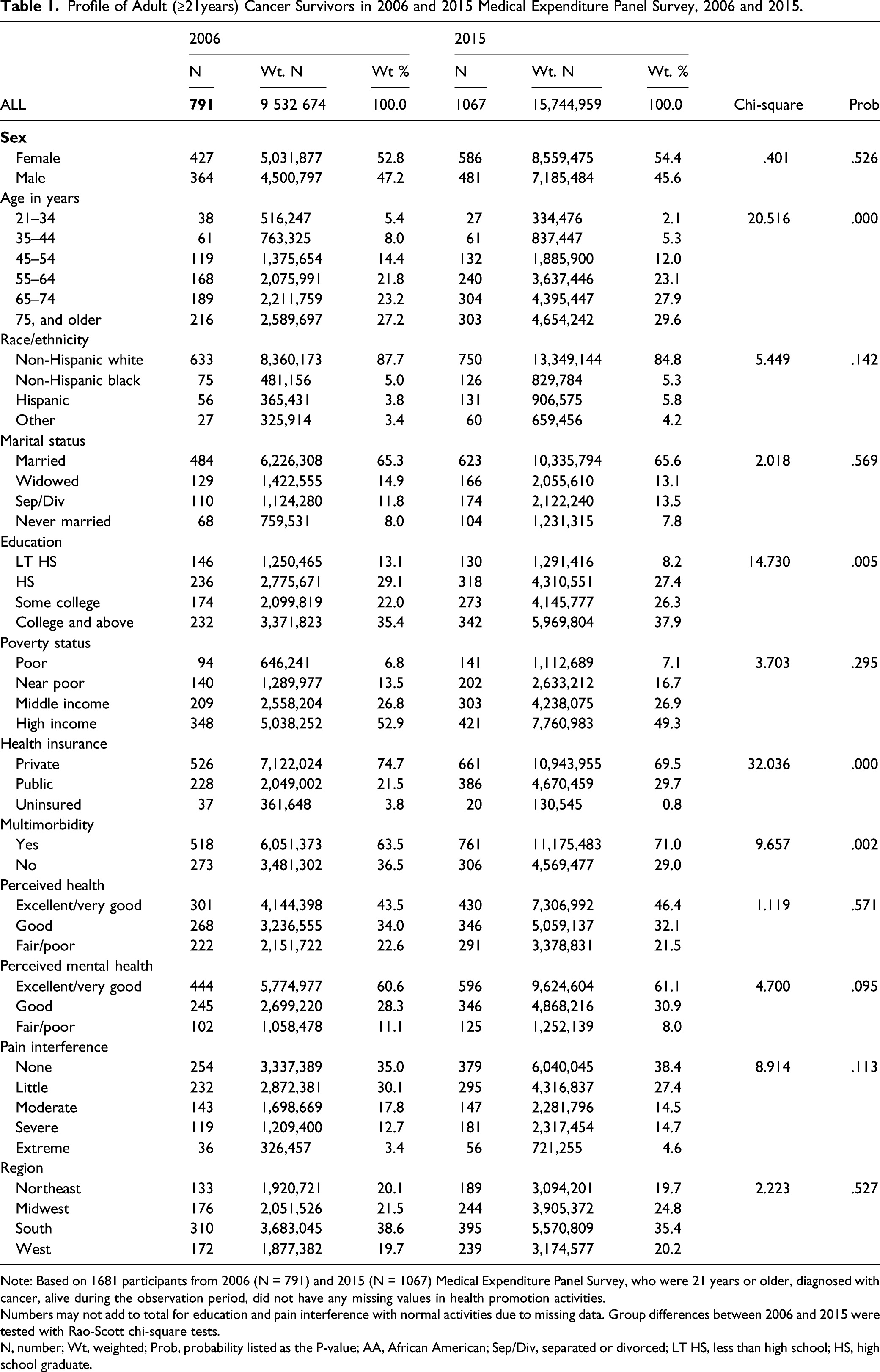
Note: Based on 1681 participants from 2006 (N = 791) and 2015 (N = 1067) Medical Expenditure Panel Survey, who were 21 years or older, diagnosed with cancer, alive during the observation period, did not have any missing values in health promotion activities.
Numbers may not add to total for education and pain interference with normal activities due to missing data. Group differences between 2006 and 2015 were tested with Rao-Scott chi-square tests.
N, number; Wt, weighted; Prob, probability listed as the P-value; AA, African American; Sep/Div, separated or divorced; LT HS, less than high school; HS, high school graduate.
Unadjusted Analyses: Health Promotion Activities Engagement/Participation
Health Promotion Activities in 2006 and 2015 Adult (age >21 years) Cancer Survivors Medical Expenditure Panel Survey, 2006 and 2015.

Note: Based on 1681 participants from 2006 (N = 791) and 2015 (N = 1067) Medical Expenditure Panel Survey, who were 21 years or older, diagnosed with cancer, alive during the observation period, did not have any missing values in health promotion activities. Numbers may not add to total for education and pain interference with normal activities due to missing data. Differences in health promotion activities between 2006 and 2015 were tested with Rao-Scott chi-square tests.
Recommended Vigorous Exercise was defined as 3 or more times per week in data to 2006, and was defined as 5 or more times per week after 2006.
Abbreviations: N, number; Wt, weighted; Prob, probability listed as the P-value.
Unadjusted (UOR) and Adjusted Odds Ratios (AOR) of Observation Year from Separate Logistic Regressions on Health Promotion Activities Adult (age ≥21 years) Cancer Survivors Medical Expenditure Panel Survey, 2006 and 2015.

Note: Based on 1681 participants from 2006 (N = 791) and 2015 (N = 1067) Medical Expenditure Panel Survey, who were 21 years or older, diagnosed with cancer, alive during the observation period, did not have any missing values in health promotion activities. Fully adjusted models controlled for sex, age, race/ethnicity, marital status, education, poverty status, health insurance coverage, multimorbidity, perceived physical and mental health, pain interference with normal activities, and region. In health promotion activities (influenza immunization, physical examination and dental visit) we additionally included self-management practices as independent variables.
Recommended Vigorous Exercise was defined as 3 or more times per week in data to 2006, and was defined as 5 or more times per week after 2010.
Abbreviations: UOR, unadjusted odds ratio; AOR, adjusted odds ratio; CI, confidence interval; Prob, probability listed as the P-value.
Adjusted Analyses: Health Promotion Engagement Over Time
In fully adjusted logistic regression models (Table 3), cancer survivors in 2015 were significantly less likely to report physical activity (AOR = .68; 95% CI = .54, .86 P = .0012). None of the other health promotion activity engagement/participation were significantly different between the two years.
Discussion
There have been many advancements in cancer care between 2006 and 2015, including the roll-out of the Affordable Care Act. It was hoped that this major advancement in healthcare access in particular, and post-cancer plans would have resulted in positive changes on the engagement/participation in health promotion activities. Using data from a nationally representative data set, MEPS, we found that the engagement/participation in health promotion activities remained relatively stable over the 10-year period. Although there was a reported decline and, in fact, physical activity rates declined.
Having an influenza immunization changed from 66.8% in 2006 to 70.3% in 2015. Healthy People 2020 set a goal of 38.1% of noninstitutionalized adults 18 years and older to receive the vaccine. 20 Having nearly double the goal percentage in both years indicates the importance that healthcare providers have in increasing the influenza vaccination rates for cancer survivors.21,22 One access advancement for the vaccinations is the availability of the vaccines from community pharmacists. 23 This benefit is particularly important for those at risk for severe illness and/or complications from the flu, including cancer survivors. 24 In light of the number of US residents who report being anti-vaccination (approximately 9-10%), and the number who have eschewed the life-saving COVID-19 vaccinations despite ongoing public service announcements (approximately 30%), having a near 70% of cancer survivors with influenza vaccination level in both years is remarkable. Nevertheless, some may have thought that with the implementation of the ACA and the related Medicaid expansions which pay for the influenza vaccination that there would have been greater use. 25 It has been found that the individual needs to have continuous coverage to see the benefits (ie, preventive care and cancer screening) of having insurance under the ACA. 26
The 2006 IOM report 27 sets forth recommendation to help survivors face the late and long-term effects of treatment and to guide them on the necessary preventive and follow-up care, including survivorship care plans (SCPs). 28 However, researchers have found that primary care providers had limited knowledge of cancer sequalae to develop these plans with their patients. 29 In fact, less than 25% of cancer programs even use SCPs. 30 A recent meta-analysis and systematic review of SCPs concluded that they do not improve patient outcomes. 31 We do not know if persons in our study had SCPs, but even if they did, the results would tend to the null (not have impacted outcomes). This may be a factor in not having greater engagement/participation in health promotion activities or self-management behaviors in our study.
Other reasons for the lack of engagement/participation in health promotion activities may include the lack of health policies for preventive care to support wellness. Only 10% of increased survival is attributable to medical care, while 40% is due to behavioral changes. 32 The lack of health policies is problematic on the individual level as well as the population level. Nearly 95% of the trillion dollars the US spends on health is for medical care services, while only 5% is for population-based strategies to support preventive health. 32 As our study shows, more attention is needed to support preventive health (ie, health promotion activities) and address the whole health model.
Consistent with a prior study, 33 we observed that as of 2015, 52.9% of cancer survivors did not engage in physical activity 5 times a week for 30 minutes. There was a hope that messaging about the importance of exercising for cancer survivors would have resulted in greater participation. 34 The results of the study, a decline in physical activity, should be considered with caution as there was a change in the definitions and recommendations for physical activity between 2006 and 2015. In 2006, MEPS investigators defined physical activity as engaging in physical activity 3 times a week for 30 minutes, but in 2008 the guidelines changed to recommend vigorous physical activity 5 times a week for 30 minutes. 35
Nevertheless, our findings suggest that cancer survivors are not engaging in physical activity at the recommended levels. This is despite the implementation of SCPs and the abundance of national health messaging about the importance of exercise. 33 In all these programs, policies, and messages, the focus has always been on the individual. Based on intervention studies, we speculate that perhaps system changes need to occur for the cancer survivors to change their life-style activities. Clarke et al suggest that, particularly for those of racial and ethnic minorities, interventions that focus not only on the individual but also the systems encourage preventive behavior. 36 Systems-based approaches can include green spaces to walk, walking-friendly communities, and community-based activities (eg, events in which people come together to make exercise more regular throughout the year), in addition to a systems approach to support caregivers to guide appropriate physical exercise. 37
We also note the increased presence of multimorbidity of the cancer survivors in 2015 compared to 2006. These differences are partially explained by changes in the ways of capturing chronic conditions (eg, arthritis). Additionally, multimorbidity creates a situation of competing demands, and often the focus is on conditions that are dominant.38,39 Until recently, and in just one study, 40 the majority of current clinical guidelines focus on individuals with a single disease such as diabetes or cancer, not on those with multimorbidities.40,41 Even today, clinical guidelines are needed for cancer survivors with multimorbidities. The system needs to shift from a “disease-specific” oriented system to “whole-person” system.
Consistent with other studies, we also found an increase in the overall age of the cancer survivor. Researchers indicate that there have been improvements in early diagnosis and treatment of cancer and therefore an increase in age of cancer survivors. This is an important finding as it emphasizes the need to provide care for the older cancer survivor to ensure they engage in health promotion activities. One hopeful note is that older cancer survivors are more likely to engage in these activities than other older adults. 21
Our findings do seem provide indirect evidence of a “gateway hypothesis.” In the gateway hypothesis, engaging in one healthful behavior is more likely to lead to engagement of another healthful behavior—if a person is physically active, he or she may be more likely to eat more healthfully 42 which may lead to maintaining normal weight, etc. In our study, few of the cancer survivors had at least one health promotion activity, which we identify as a gateway problem. This suggests that it important to understand what is preventing an individual from doing one behavior, to give opportunity for other behavioral interventions to become more likely to succeed.
Limitations
There are several limitations to this study that need to be noted. First, the study was cross-sectional using self-reported data. Because of the way the question was asked about having cancer, we were not able to distinguish between cancer survivors in treatment and in remission. We also have the limitation of the change of definition of physical activity/exercise between 2006 and 2015.
Despite these limitations, we did use a large nationally representative dataset, MEPS, and considered a comprehensive list of services as well as factors associated with health promotion activities. Our study shows cancer survivors are still not adequately engaging in health promotion activities. It would be important for providers to continue to emphasize messages around health promotion activities, including the benefits of physical activity for cancer survivors.
Clinical Implications
We found there remains a need to improve engagement/participation of cancer survivors in health promotion activities. There was little change in these important aspects of improving the quality of life.
Footnotes
Author Contributions
Concept: PF and US.Analysis: US and PF.Manuscript draft: US and PF.Revisions: All authors.Final approval: all authors.
Declaration of Conflicting Interests
All authors declare no competing interests.
Funding
There is no funding to declare for this work.
Ethical approval
The West Virginia University Institutional Review Board has determined that protocol 2008089719 does not meet the definition of human subjects research, as provided in 45 CFR 46.