
Abstract
Objectives
We examined the extent to which funded satellite clinics could sustain the California Colon Cancer Control Program (C4P) strategies implemented in health systems to increase uptake of the fecal immunochemical test (FIT) or immunochemical fecal occult blood test (iFOBT) for colorectal cancer (CRC) screening in the absence of future C4P funds.
Introduction
Seven health systems consisting of 38 satellite clinics participated in C4P to examine the sustainability of the program in the absence future Centers for Disease Control and Prevention (CDC) funding.
Methods
Quantitative and qualitative methods with a close and open-ended survey approach, and a prospective cohort design were used to examine the sustainability of the C4P in health systems.
Results
A total of 61% of satellite clinics could not sustain funding stability. Only 26% could sustain funding stability. About, 71%, 26%, and 21% of the satellite clinics could sustain the small media platform, patient navigation services, and community health workers (CHWs), respectively. All the satellite clinics sustained the provider reminder system and professional development. Roughly, 71% and 42% of funded satellite clinics could not sustain the patient navigators and CHWs, respectively. The satellite clinics that could sustain funding stability, sustained patient navigation services and CHWs. Health systems that could not sustain funding stability, could not sustain patient navigation services and CHWs. Qualitatively, the need to support uninsured priority populations, health educators, patient navigators, care coordination activities, outreach services, and provision of enhanced services emerged. The need to support enhanced quality measures, expansion of funding, Medi-Cal Public Hospital Redesign and Incentive coverage, health plan, community linkages, resource sharing, and best practices specifically on CRC screening emerged. Themes such as automated reminder, limited personalized care delivery and capacity, transportation barriers, staff salary, expansion of care through patient navigation, and culturally appropriate media campaign also emerged.
Conclusion
Overall, to address sustainability barriers, funding stability should be maintained in the health systems.
Keywords
Introduction
Colorectal cancer (CRC) remained the second leading cause of cancer-related deaths and the third most common type of cancer in the United States (US) in men and women combined.1,2,3 More than 149,000 new cases are diagnosed and over 52,000 people die from CRC in the US each year.1,2 In California, CRC is also the second leading cause of cancer-related deaths and over 5,300 Californians die each year from CRC. 1
High uptake of CRC screening is necessary to delay and prevent CRC. The US Preventive Services Task Force (USPSTF) recommends the use of Fecal Immunochemical Test (FIT) or Immunochemical Fecal Occult Blood Test (iFOBT) for CRC screening.2,4-8 FIT/iFOBT is a noninvasive, an affordable, and population-based CRC screening test compared to colonoscopy or other CRC screening modalities.5,9-12 Yet, the uptake of CRC screening is suboptimal in the US.13,14,15 FIT is a stool-based screening test most commonly used worldwide to detect polyps or cancer in the colon or rectum.4,9,10,16,17 It has higher sensitivity and can detect advanced adenomas or colorectal adenocarcinomas compared with the RIDASCREEN (R-Biopharm AG, Darmstadt, Germany).5,9,18 FIT is the second most common test used for CRC screening in the US. 9
FIT/iFOBT uptake contributed to the decline in the CRC incidence and mortality, 9 and about 65% of age-eligible adults in the US are up to date with CRC screenings.7,19 Though, FIT CRC screening rates may vary by programs and clinical settings, the overall adherence to FIT-based CRC screening is low. 9 High adherence requires adoption of evidence-based interventions (EBIs) and supporting activities known to increase uptake of FIT/iFOBT CRC screening. 9
To maintain high uptake of CRC screening strategies, health systems must maintain the capacity to sustain implemented EBIs and supporting activities in the absence of Centers for Disease Control and Prevention (CDC) or California Colon Cancer Control Program (C4P) funds. Often, sustainability requires a program champion and organizational support. 13 Organizational support can include strategic planning and integration, funding, and enhanced policies and procedures to engage organizational commitment to program investments and outcomes. 13 In this study, we examined the extent to which funded health systems and their satellite clinics could sustain C4P strategies that were implemented to increase uptake of FIT/iFOBT CRC screening rates in the absence of future C4P funds.
Program Strategies and Activities
From 2015 to 2020, the C4P promoted and implemented the following six strategies and activities, partnerships and program coordination, priority EBIs, community-clinical linkages, professional development training, health information technology (HIT), and program monitoring and evaluation to increase uptake of FIT/iFOBT CRC screening in seven health systems consisting of 38 satellite clinics.
Partnerships and Program Coordination
C4P identified health systems partners and implemented EBIs and supporting activities to increase CRC screening and ensure quality care among patients ages 50-75 years old. The major component of the partnership and coordination included assessment of the health system or partners’ organizational data, current infrastructure, processes, procedures, and other relevant data framework to inform the intervention plan (for example, a patient reminder system exists but is not used by all staff) to increase and improve CRC screening within the health system. C4P developed an implementation plan that includes evaluation measures and data sources, and monitored and evaluated project progress. Also, C4P provided a plan to formally evaluate the processes and outcomes of partnerships and partnership activities.
Priority EBIs
C4P promoted and worked with the health systems and their satellite clinics to implement EBIs included in the Community Guide-recommended interventions to increase CRC screening. The EBIs and supporting activities implemented included provider assessment and feedback, provider reminders, patient/client reminders (letter, postcard, e-mail or telephone messages including automated messages) designed to advise people that they are due for CRC screening. C4P promoted and implemented small media, patient navigations, and reduction of structural barriers activities (for example, structural barriers are non-economic burdens or obstacles such as inconvenient clinic hours that make it difficult for people to access CRC screening) in the health systems and their satellite clinics.
Community-Clinical Linkages
C4P promoted and facilitated collaboration between health systems and community-based organizations that serve the target population. For example, we promoted the utilization of community health workers (CHWs) for community outreach to reach priority populations and provided CRC screening education and support to link patients to primary health care for CRC services. We also facilitated a formal partnership with the health systems to work with community leaders and local stakeholders to engage in community activities such as talking circles to improve community trust. C4P worked with health systems to promote integration of the strategies and activities into their organizational strategic planning and policy that encourages CRC screening among priority populations to remove structural barriers that may prevent or delay CRC screening. Further, we integrated CRC screening as part of a community-based program such as, but not limited to, a Flu-FIT/Flu-FOBT program.
Professional Development Training
C4P promoted adherence to USPSTF guidelines for CRC screening and the US multisociety task force surveillance guidelines for CRC. We also promoted CRC screening quality assurance and quality improvement best practices.
HIT
C4P promoted electronic health records (EHR) or HIT optimization to collect and report relevant data (for example, baseline and post-intervention CRC screening numbers). We promoted and implement enhanced EHR or HIT optimization to reduce missed opportunities and ensure that patients received adequate CRC screening. We encouraged health systems to monitor quality (timeliness) and clinical outcomes and enhance its clinical decision support, EHR/IT and financial management systems to identify, screen, and follow up on persons due for CRC screening in the health systems. We used program data to routinely conduct quality improvement activities.
Throughout the duration of the program, we provided feedback on the progress attained and challenges encountered toward the project goals. C4P assisted health systems in adopting strategies to improve the exchange of electronic data across organizational and jurisdictional boundaries and worked together to address the legal, ethical, security, and confidentiality issues related to data sharing by ensuring that only de-identified and aggregate patient data was shared with the CDC.
Program Monitoring and Evaluation
C4P monitored and evaluated the program to track progress and measure outcomes of the program efforts. We conducted process evaluations to monitor implementation of all program activities. We evaluated the achievement of the program workplan outcomes such as increased high quality screening among defined patient populations, increased adherence to timely diagnostic colonoscopy, and increased re-screening among defined patient populations such as those who had incomplete test results. Further, we obtained baseline data for the outcomes from all the seven health systems and their satellite clinics (38 satellite clinics) prior to implementation of the C4P activities described in the program workplan. Annually, we collected data for all the strategies and activities to assess outcomes.
Core Sustainability Components
CDC Colorectal Cancer Control Program (CRCCP) Operationalization of EBIs and Supporting Activities.

Core component source: Strategies recommended by guide to community preventive services for increasing CRC screening by FIT/FOBT apply to all core component areas. https://www.thecommunityguide.org/cancer/
PSAT source: Luke, D. A., Calhoun, A., Robichaux, C, B., Elliott, M, B., Moreland-Russell, S (2014). The program sustainability assessment tool: A new instrument for public health programs. Prevention Chronic Disease, 11: E12. doi: 10.5888/pcd11.130184
The C4P promoted strategies, EBIs, and supporting activities to increase uptake of FIT/iFOBT CRC screening in health systems to reduce the incidence, mortality, and health disparities of CRC in underserved populations. The EBIs and supporting activities are part of the CRC intervention recommended by the Guide to Community Preventive Services to increase CRC screening.21,22,23 For this sustainability assessment, the award received by C4P from the CDC’s Colorectal Cancer Control Program (CRCCP) began on June 30, 2015 and ended on June 29, 2020. In this study, we examined the sustainability of C4P strategies, EBIs, and supporting activities in three core areas: Core capacity, EBIs, and supporting activity components. The three core component definitions were operationalized, Table 1.
C4P Target Population
Core Capacity Sustainability Responses.

Methodology
A close and open-ended survey was used to collect both quantitative and qualitative data from funded health systems and their satellite clinics for each PSAT component comprising of core capacity, EBIs, and supporting activity of the sustainability assessment. The sustainability survey was administered to seven funded health systems consisting of 38 satellite clinics in Year 4 (2019) of the C4P grant cycle. At the time the sustainability survey was administered, 38 satellite clinics were participating in C4P intervention. In Year 4 of the C4P grant cycle, the health systems had stabilized the EBIs and supporting activities they implemented for the uptake of FIT/iFOBT CRC screening.
The sustainability survey included, one quantitative and one qualitative question for each core sustainability area. The quantitative question asked for each core component was: “without additional funding from the CDC, which of these core sustainable areas can or cannot be sustained by your health center/clinics?” The nominal response options for this question were ‘yes’, ‘no’, ‘don’t know’, and ‘not applicable’. For these options, only one response could be selected by the respondents. The quantitative question was followed by a probing qualitative question, where we asked respondents to briefly describe the reason or rationale for the response option they selected.
Data Collection
Both the quantitative and qualitative data for the sustainability capacity were collected from seven funded health systems consisting of the 38 satellite clinics to understand the quantitative and subjective views of the core sustainability areas in the absence of future funding support from C4P for FIT/iFOBT CRC screening. The responses provided by the funded health systems represented 38 participating satellite clinics. The sustainability survey was sent to the funded health systems through an email platform which included a hard copy attachment of the survey. The program director and coordinator responsible for the C4P in each health system worked with their respective satellite clinical staff and management team to complete the survey. Therefore, to ensure reliability of the responses for each question, we allowed the clinical staff responsible for the C4P in each health system to coordinate the survey responses because the team knows the appropriate staff responsible for the program activities. Each health system compiled their responses to the survey from their satellite clinics as a unit. All the completed responses were submitted to the CDPH-C4P team through email.
Statistical Analysis
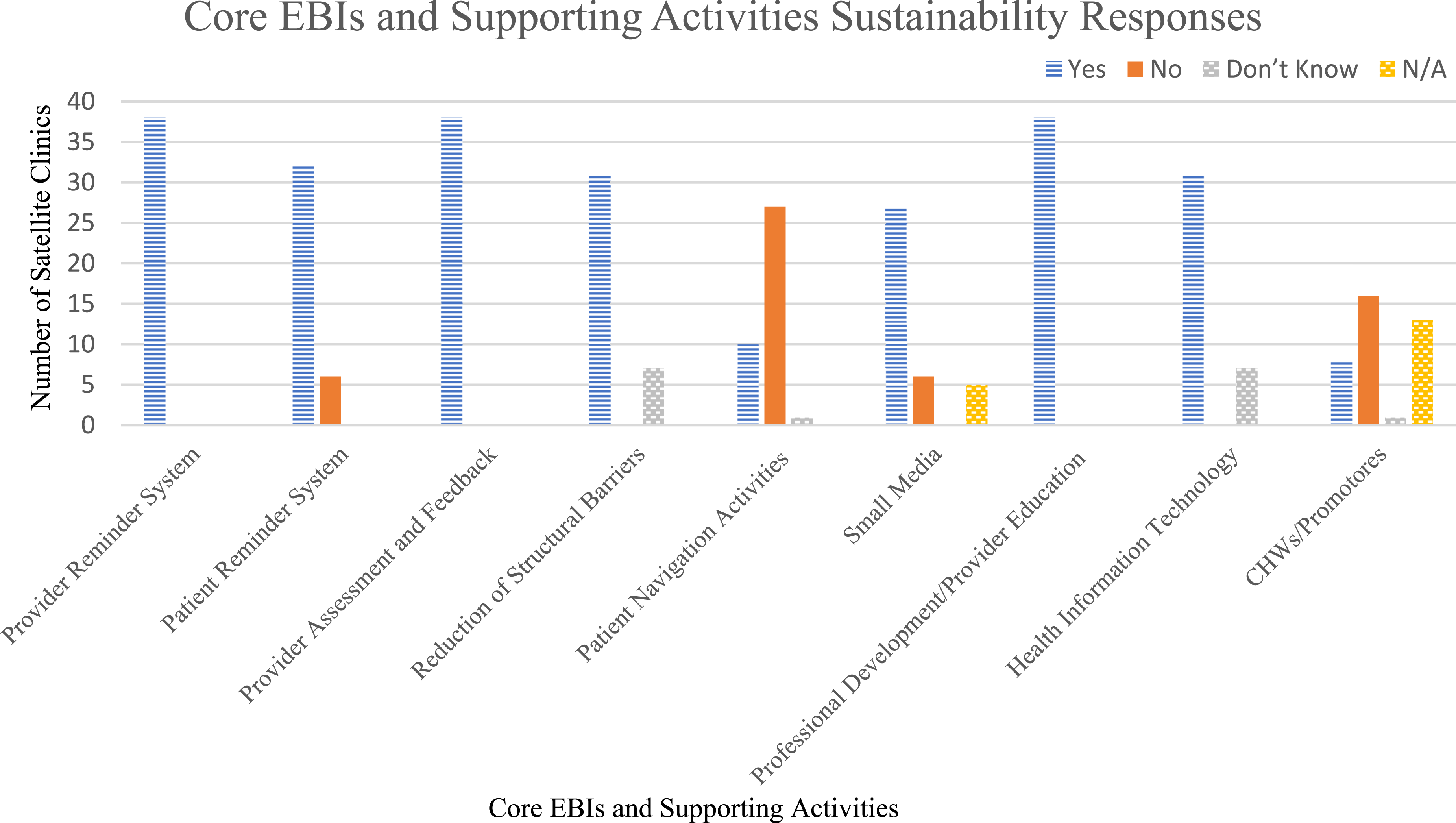
Core EBIs and Supporting Activities Sustainability Responses.

N/A = Not Applicable.

Core capacity sustainability assessment.
Core EBIs and supporting activities sustainability assessment.
The open-ended responses were used for the qualitative thematic analysis. The thematic analysis was conducted by reviewing the narrative responses and identifying the key themes of the narrative reported by the health systems for each question. Thematic analysis was used to identify common subjective themes to inform sustainability successes and challenges described in this study. For each core sustainability component category, the health systems provided a brief narrative after selecting an option from the nominal response category that described their rationale for the selection. We reviewed each of the narrative and identified the key themes that emerged. The themes identified were the foundation of the qualitative findings described in this study. The sustainability survey had three core components; the core capacity, EBIs, and supporting activity (Table 1), but in the analysis (Table 2 and Figure 2), the EBIs and supporting activity components were combined.
Results
C4P funded seven health systems and their satellite clinics. A combined total of 40 satellite clinics from the seven health systems participated in C4P. Of the 40 satellite clinics, 38 (95%) were actively participating in C4P in Year 4 (2019) when the sustainability survey was administered. For the 2 satellite clinics that were excluded, 1 (2.5%) was closed in 2018 and the other started C4P strategies after the sustainability survey was fielded in 2019.
All seven funded health systems and their satellite clinics, 38 in total, adopted and implemented C4P strategies to improve uptake of FIT/iFOBT CRC screening among eligible patients. In this study, all seven funded health systems and their 38 satellite clinics participated in the sustainability survey assessment. In the absence of future C4P funding support, all 38 satellite clinics (100%) can sustain the partnership and strategic plan developed during the implementation phase of C4P strategies for uptake of FIT/iFOBT CRC screening. Approximately, 90% of the satellite clinics will continue to sustain the environmental support and program adaptation strategies. About, 74% of the satellite clinics will continue to sustain the program evaluation and program adoption strategies. Seventy one percent of satellite clinics that participated in the C4P intervention will continue to sustain the organizational capacity and communication infrastructures and infostructures. Only, 26% of the satellite clinics can sustain funding stability to continue to support strategies and activities for uptake of FIT/iFOBT CRC screening implemented in the health systems and their satellite clinics in the absence of future C4P funding support (Table 2 and Figure 1). Of the 38 satellite clinics, 23 (61%) satellite clinics do not have funding stability to sustain uptake of FIT/iFOBT CRC screening while five satellite clinics do not know if they have the funding stability to sustain the C4P activities. Only 10 satellite clinics have funding stability to sustain C4P strategies (Figure 1). Approximately, 26% cannot sustain program adoption strategies. Furthermore, 16% and 10% cannot sustain organizational capacity and environmental support or program evaluation respectively, in the absence of future C4P funding support (Table 2 and Figure 1).
For the core EBIs and supporting activity sustainability components, in the absence of future C4P funding support, all 38 satellite clinics (100%) can sustain the provider reminder system, provider assessment and feedback, and professional development/provider education strategies developed during the C4P implementation phase. About 84% of satellite clinics can sustain the patient reminder system. Approximately, 82% of the satellite clinics can sustain infrastructures put in place to reduce structural barriers and maintain HIT. In the absence of future C4P funding support, 71%, 26%, and 21% of the funded satellite clinics can sustain the small media platform, patient navigation, and CHWs, respectively. Roughly, 71% and 42% of satellite clinics cannot sustain the patient navigators and CHWs, respectively. The health systems and satellite clinics that can sustain funding stability can also sustain patient navigation and CHWs. The health systems that cannot sustain funding stability cannot sustain patient navigation and CHWs. Only 16% of the satellite clinics cannot sustain the patient reminder system or small media in the absence of future C4P funding support (Table 3 and Figure 2).
Core Capacity Themes
Several themes emerged from the qualitative or subjective narrative responses provided by the health systems’ staff for each core capacity assessment component question. The common themes that emerged were support for uninsured priority populations, provision of enhanced services, health educators, patient navigators, care coordination activities, and outreach services. Themes such as standard quality measure requirements including Healthcare Effectiveness Data and Information Set (HEDIS), limited funding, Medi-Cal Public Hospital Redesign and Incentives coverage, health plan, community linkages, resource sharing, and best practices also emerged. These themes were the justifications provided by the health systems to support the quantitative responses they selected for the core capacity components.
The 10 satellite clinics that indicated that they had funding stability to support C4P strategies in the absence of future C4P funding support also stated that the C4P funds were primarily used to support the needs of their uninsured patient population in the health system. Therefore, in the absence of C4P funding support, they indicated that the C4P activities would continue with the insured patients while the uninsured patients would not receive enhanced services supported by the C4P strategies. The 23 satellite clinics that did not have funding stability to sustain uptake of FIT/iFOBT CRC screening primarily used the C4P funds to support health educators, patient navigators, care coordination activities, and outreach services for CRC screening. They further stated that CRC screening was not an incentivized HEDIS measure through health plans. Thus, the C4P strategies and activities cannot be sustained in the absence of future C4P funding. On the other hand, the five satellite clinics that reported that they “Don’t Know” the funding stability status for sustaining C4P strategies indicated that there was limited funding towards CRC programming through the California Medi-Cal Public Hospital Redesign and Incentives, and that they may not be able to support the program activities in the absence of future C4P funding.
Most importantly, 38 satellite clinics will sustain their partnership/collaboration efforts to continue CRC screening. Their existing partnerships and collaboration with other community organizations such as the American Cancer Society (ACS), local health agencies, and CDPH will continue. Partners provide educational resources and best practices' materials to improve staff, providers, and patient education on CRC screening. Some of the local agencies operate volunteer-based health advocacy to provide community linkages and connect patients with outside organizations for resources and social services. All the seven health systems and their 38 satellite clinics stated that C4P activities would be incorporated into their system-wide strategic planning to continue to improve CRC intervention approaches and FIT-based population-driven CRC screening. They will continue to implement CRC interventions and share best practices on CRC screening with stakeholders.
Core EBIs and Supporting Activity Themes
Several themes emerged from the brief qualitative narrative responses provided by the health systems for each of the core EBIs and supporting activity question. For the core EBIs and supporting activity components, the emerged themes include automated EHR-based alert reminder systems, limited personalized care, limited capacity, transportation barriers, staff salary, expansion of care through patient navigation, and culturally appropriate media campaign. The stated themes were provided by the health systems to support the quantitative narrative responses for the core EBIs and supporting activity components.
The health systems’ 38 satellite clinics can sustain the automated EHR-based provider reminder system, provider assessment and feedback, and professional development/provider education system-wide to continue to improve FIT-based CRC screening. A total of 32 satellite clinics can sustain the patient reminder system. In the absence of future C4P funding support, the satellite clinics’ capacity including availability and access to patient navigation activities and personalized care or services implemented to increase the uptake of FIT-based CRC screening will be compromised.
Transportation and community linkage barriers were the primary structural barriers addressed by health systems through the assistance programs such as financial, housing, social support, and Social Work and Health Advocates Programs. With limited travel options or funding capacity to continue to provide transportation vouchers to eligible patients, the underserved priority populations will experience difficulties maintaining their scheduled appointments.
Of the 38 funded satellite clinics, only 10 satellite clinics can sustain the patient navigation activities. A total of 27 satellite clinics cannot sustain the patient navigation activities and one does not know if they can or cannot sustain patient navigation in the absence of future C4P funding. The C4P funding was the primary source through which the patient navigator and health educator’s salaries were funded. Therefore, in the absence of the C4P funding, the patient navigation and health educator’s positions will be dissolved. Furthermore, some aspects of CRC screening outreach performed by the patient navigators and/or health educators could be absorbed by other clinic staff, but the outreach would not be nearly as robust as that of patient navigators or health educators, as clinics have competing priorities and staffing limitations. The health systems that did not know the sustainability status of patient navigation suggested that the patient navigation activity needs further expansion in terms of their operational constructs and roles.
Of the 38 funded satellite clinics, six (16%) satellite clinics cannot sustain and will not continue the small media campaign for CRC screening in the absence of future C4P funding for lack of capacity to support dynamic and culturally appropriate media campaigns around CRC screening. Thirty one (82%) satellite clinics that will sustain optimized HIT or EHR system-wide mentioned they will do so to continue to improve FIT-based CRC screening and support the day-to-day service and care delivery processes. Seven satellite clinics did not know if they can sustain the optimized HIT or EHR system adopted during the C4P implementation phase as they could not determine the extent to which C4P strategies could be maintained without adequate funding.
Of the 38 satellite clinics, only eight satellite clinics can sustain the CHWs system-wide to continue to improve FIT-based CRC screening and support the day-to-day activities of a patient care team. A total of 16 satellite clinics do not currently use CHWs and cannot sustain the supporting activity component due to limited funding. One satellite clinic does not know if they can sustain CHWs and does not know of other alternative funding for CHW activities. Thirteen satellite clinics did not provide any response on CHWs sustainability status (Figure 2).
Discussion
All seven funded health systems and their 38 respective satellite clinics can sustain some of the C4P strategies designed to improve FIT/iFOBT-based CRC screening. Some of the strategies cannot be sustained in the absence of future C4P funding support. In this study, funding stability was the most important determining factor that affected core areas of the sustainability assessment components (core capacity, EBIs, and supporting activities). Funding stability, affected health systems’ sustainability decisions around the core capacity components such as organizational capacity, program evaluation, program adaptation, and communication (Figure 1). In addition, funding stability heavily affected health systems’ sustainability decisions around the core EBIs and supporting activity components such as patient navigation and CHWs activities. There is a slight or minimal impact of funding stability on patient reminder system, reduction of structural barriers, small media use, and HIT optimization (Figure 2).
Around the core capacity assessment components, the common themes that emerged included support for uninsured priority populations, health educators, patient navigators, care coordination activities, outreach services, and provision of enhanced services. The need for support of enhanced quality measures, expansion of funding, Medi-Cal Public Hospital Redesign and Incentives coverage, health plan, community linkages, resource sharing, and best practices on CRC screening also emerged in this study.
For the core EBIs and supporting activity components, automated EHR-based alert reminder systems, limited personalized care delivery and capacity, transportation barriers, staff salary, expansion of care through patient navigation, and culturally appropriate media campaign themes emerged. To mitigate the issues around these themes effectively and efficiently, funding stability should be maintained and sustained in the health systems.
According to many experts, average effect sizes had greater impacts with additional adoption of other EBI components, provider incentives, patient navigation, and access to free or low-cost testing.24,25 Similarly, CRC screening rates are higher with inclusion of more and sustainable EBIs.24,25 Patient navigation improves adherence to colonoscopy follow-up. According to Coronado et al, 26 76% of patients who received patient navigation completed a colonoscopy while 65% with usual care completed a colonoscopy, HR = 1.35; 95% CI, 1.07-1.72; P = .027. In this study, in the absence of future CDC funds, funding stability, patient navigation, and CHWs cannot be sustained in most of the 38 funded satellite clinics. Patient navigation and CHWs play critical roles in patient care and continuity of service including appointment reminders and high uptake of FIT to reduce structural barriers, promote adherence, reinforce healthy behavior, and improve patient quality of life.27-30 Modifiable behaviors and best practices including lifestyle factors such as physical activity, body mass index, alcoholic drinks, red meat, processed meat, dietary fiber, dietary calcium and cigarette smoking are risk factors of CRC.31,32 Patient with familial history are at higher risk of CRC, thus, early screening for CRC might be considered for first degree relatives of patients with polyps. 32 Patient navigators and CHWs are essential in navigating patients through the CRC screening processes. In this study, patient navigators and CHWs cannot be sustained in the absence of future CDC funds because the patient navigators’ salaries were funded exclusively from the C4P fund.
The major limitations of the study include the structure of the program evaluation, once the C4P funding support ends for the health systems and their satellite clinics, the C4P team cannot prospectively monitor the progress of the seven health systems and their 38 satellite clinics to assess the core component areas they sustained or did not sustain. More importantly, the C4P funding support provided to the seven health systems and their 38 satellite clinics was exclusively from the CDC’s CRCCP grant award. In this study, the health systems and their satellite clinics that participated in the C4P were funded by C4P through the CDC’s CRCCP funds. In the absence of the CDC funds,, CDPH could not continue to fund the C4P activities and intervention in California.
Conclusion
In this study, funding stability, patient navigation, and CHWs cannot be sustained in the majority of the 38 funded satellite clinics in the absence of future C4P funding support. Patient navigation plays a substantive role in clinical and community settings in linking patients with resources and services to promote healthier behavior and improve patient quality of life. Patient navigators and CHWs have access to community linkages and resources. C4P strategies encourage and promote patient navigation activities both at the clinical and community settings to increase awareness about CRC. Further studies are needed to examine alternative strategies to support funding stability in health systems to provide EBIs in the absence of future C4P funding support to ensure sustainability of FIT/iFOBT-based CRC screening.
Implication to Public Health Policy, Clinical Best Practices, and Future Research
Seven health systems consisting of 38 respective satellite clinics were funded by C4P between 2015 to 2020 to improve uptake of FIT/iFOBT-based CRC screening capacity to maintain, manage, and sustain existing CRC screening processes and best practices in core sustainability component areas. However, funding stability cannot be sustained in many health systems in the absence of future C4P funding support. The findings provide an opportunity for CDPH and many health systems’ management to re-assess and explore other alternative funding opportunities to support C4P strategies in the absence of CDC’s CRCCP funding support. It is also necessary for CDPH to invest in a multi-agency grant opportunity approach to create stronger sustainability strategies for programs such as the C4P, California Well-Integrated Screening and Evaluation for Women Across the Nation, Prevention Forward (the diabetes and cardiovascular disease program), and other state and local programs. At the clinical level, in the absence of future C4P funding support, health systems should integrate the C4P strategies into their system-wide operational plan in ways that would not compromise the CRC screening efforts, progress, and processes. Therefore, we suggest that health systems management team should integrate effective public health and medical interventions shown to increase uptake of CRC screening such as the FIT/iFOBT-population-based CRC screening best practices into their system-wide strategic planning to ensure sustainability in the absence of external funding.
Footnotes
Acknowledgments
We thank the CDC for providing a five-year (2015 to 2020) award to CDPH to support the C4P population-based colorectal cancer screening efforts. The CDC’s CRCCP grant award supported CDPH public health efforts and allowed us to provide over 91,000 CRC screenings in California through the C4P. We also acknowledge all seven funded health centers and their respective 40 satellite clinics, clinical staff, management team, and stakeholders who participated, supported, and implemented the C4P strategies and activities in the health systems. Many thanks to other partners and stakeholders, including the ACS and California Colorectal Cancer Coalition for supporting and sharing of resources that informed CRC best practices throughout the five-year period of the program’s implementation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The most recent CDC’s CRCCP five-year grant award to Centers for Disease Control and Prevention (CDC) and California Department of Public Health (CDPH) (NU58DP006095) was from 2015 through 2020 for CRC screening project.