
Abstract
Background
The goal of this study was to evaluate the global burden of malignant skin melanoma (MSM) from 1990 to 2019 using MSM-related data from the Global Burden of Disease study.
Methods
The incidences’ relationships with the social-demographic index (SDI) and human developmental index (HDI) were investigated. To determine significant changes in incidence trends, the joinpoint regression model was used. To demonstrate trends in MSM mortality rates, an Age-Period-Cohort framework was conducted. For the projection of new cases and the age-standardized incidence rate (ASR) of MSM incidence to 2034, the Nordpred method was used.
Results
In 2019, the ASR incidence per 100, 000 people for MSM was 3.6 (95% UI, 2.6–4.2). MSM prevalence increased in most countries between 1990 and 2019 (average annual percentage change >0). HDI and annual percentage change (APC) (ρ = .63, P < .001), as well as SDI and ASR, had a positive correlation. The total MSM mortality rate declined globally, with an APC of −.61%. Likewise, the mortality rate for the age group of people with ages <77.5 years declined. Predictive analysis demonstrated a declining trend in ASR incidence and a growing number of MSM.
Conclusion
There are significant differences in ASR incidence among regions and countries. Despite decreases in ASR incidence and fatality, MSM remains one of the leading sources of cancer mortality and morbidity globally. MSM necessitates more primary prevention measures and screening in high-risk areas.
Keywords
Introduction
Melanoma is a melanocyte-derived malignancy. Melanoma accounts for only 10% of all skin cancers yet accounts for 80% of skin cancer-related deaths. 1 The majority of melanomas are malignant skin melanoma (MSM), with mucosal and uveal melanoma each accounting for 4%. 2 Patients with melanoma gained better therapeutic outcomes with complicated reconstructive procedures and precision medication after decades of research.3,4 Despite the fact that the 5-year cancer-specific death rate for melanoma is already as low as 8.2%, another significant issue is the growing disease burden. 5 One-fifth of melanoma patients develop lymph node metastatic relapse after the first surgical resection, necessitating further surgical treatment as well as sophisticated targeted therapy and immunotherapy. 6 Melanoma therapy was estimated to cost US$3.3 billion a year in the United States between 2007 and 2011. 7 There were 308,684 melanoma incidences worldwide in 2017, with a 161.3% increase from 1990 to 2017. 8
MSM epidemiology and illness burden are linked to race, sociocultural development, demographic trends, and risk factors. 9 MSM is significantly more common in fair-skinned people than in dark-skinned people, with regional and socioeconomic differences, with Australia bearing the greatest burden, followed by high-income North America and Europe. 10 Furthermore, differences in sun exposure are attributed to the incidence patterns of MSM. The main environmental risk factor for MSM is ultraviolet (UV) radiation, specifically the UV-B spectrum found in sunlight which might help to partially explain why melanoma is so common in Australasia. 11 The worldwide prevalence of MSM has been increasing very rapidly each year compared to other malignancies, in 2012, the prevalence of MSM was ranked 15th in the world. 12 Therefore, in order to develop and implement policies for regional and global MSM prevention, it is necessary to estimate the spatiotemporal variation in the MSM burden.
The GBD 2019 dataset provides estimates for incidence, prevalence, mortality, years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life-years (DALYs) related to 369 diseases and injuries. These estimates cover both genders and encompass data for 204 countries and territories. The dataset is publicly available and overseen by the Institute for Health Metrics and Evaluation (IHME). The GBD estimation process involves identifying numerous data sources for diseases and injuries, including censuses, surveys, vital statistics, registries, health care utilization, pollution monitors, satellite imagery, and notifications. These data sources are gathered through systematic reviews, government/international websites, reports, and primary sources like Demographic and Health Surveys. A total of 86,249 sources were utilized, covering deaths, incidence, prevalence, and other metrics. Each source is assigned a unique identifier and cataloged in the Global Health Data Exchange (GHDx). 13
Understanding the disease burden of MSM allows resources and health care services to be allocated more effectively in order to reduce MSM incidence, prevalence, and mortality. Although regional and global trends in the incidence and mortality of skin diseases have been identified, there are few detailed epidemiologic studies on global MSM. There have been no published correlation studies between sociological indicators (socio-demographic index (SDI), human development index (HDI)) and MSM trends, or predictions of MSM disease burden in the future. In this study, several global trends in MSM through the GBD were highlighted from 1990 to 2019 in 204 countries, moreover, correlations between sociological indicators and MSM trends were also elucidated. Furthermore, based on GBD 2019, we forecast the global burden of MSM over the next 10 years. The current study provided evidence-based strategies for coordinated actions to promote resource allocation for health care and prevention.
Materials and Methods
Study Data
This study used a data review from GBD instead of human or animal subjects. The Global Health Data Exchange (GHDx) query tool (https://ghdx.healthdata.org/gbd-results-tool) was used to extract the following variables from the database: the number and age-standardized rates (ASRs) of incident cases, prevalent cases, at the global, regional, and national levels. 14 These variables can help us analyze the disease burden across different regions and countries. Geographically, the 204 GBD countries and territories were divided into 22 regions. The data for this study were analyzed from May 1, 2022 to May 31, 2022. The original data extracted from GBD (Supplementary Tables 1 and 2) and related world populations of all age groups were included in the supplementary tables (Supplementary Table 3).
Trend Analysis
Annual data of incident numbers of different metrics quantifying the burden of MSM were extracted from the GBD database for 204 countries and territories spanning the years 1990 to 2019. These estimates were accompanied by their respective 95% uncertainty intervals (UIs). The ASR were determined through a calculation process involving the summation of products of age-specific rates (denoted as “ai,” where “i” represents the ith age category) and the corresponding number of individuals (or weights, “wi”) within each age subgroup “i” from the chosen reference standard population. This summation was followed by the division of the resulting sum by the sum of the weights of the standard population. This method allows for a standardized comparison of rates across different populations or time periods, accounting for variations in age distributions. The Estimated Average Percentage Change (EAPC) was calculated to represent the secular trend in Age-Standardized Rates (ASRs) of MSM burden. This was accomplished by employing a regression model that involved fitting the natural logarithm of ASR against the calendar year. 15 The correlation between EAPCs and ASRs was investigated to identify the influencing factors for EAPCs (1990). The countries or territories were then divided into four categories based on their temporal trends in MSM ASR incidence and mortality rates, using a hierarchical cluster analysis.
Sociological Indicators
Nations were categorized based on the 2019 United Nations Human Development Index (HDI) classification system into either developed (high/very high HDI) or developing (low/medium HDI) groups (https://hdr.undp.org/data-center/human-development-index#/indicies/HDI). The current study investigates the relationship between EAPCs and HDI (2019). The SDI is a score ranging from 0 · 0 to 1 · 0, derived from the geometric mean of three adjusted components: total fertility under the age of 25 years (TFU25), income per capita distributed with a lag (LDI), and mean educational attainment for individuals aged 15 years and older. 16 To ascertain the relationship between a country’s or region’s socioeconomic development status and the ASR for MSM, the SDI was used. The SDI data was procured from the Institute for Health Metrics and Evaluation (IHME) (https://ghdx.healthdata.org/record/ihme-data/gbd-2019-socio-demographic-index-sdi-1950-2019).
Joinpoint Regression Analysis
Joinpoint regression analysis was conducted to calculate the annual percentage change (APC), average annual percent change (AAPC), and corresponding 95% confidence intervals to determine long-term trends in the incidence of MSM. 17 The Joinpoint software (version 4.9.1.0) provided by the US National Cancer Institute was used for this analysis.
Age-Period-Cohort Analysis
An Age-Period-Cohort model is a descriptive tool used to distinguish and statistically analyze the distinct effects of age, period, and cohort. 18 It describes trends in cancer incidence and mortality rates using the aforementioned scales.
The present study aimed to estimate age, period, and cohort-specific effects using the Age-Period-Cohort model between 1990 and 2019. The Web Tool for Age-Period-Cohort Analysis was used to analyze the data (Biostatistics Branch, National Cancer Institute, Bethesda, MD https://analysistools.nci.nih.gov/apc/). 19 Data was tabulated into 18 five-year age groups (ranging from 1 to 4 years to 85 years), 6 five-year periods, and 25 overlapping 5-year birth cohorts. The Wald Chi-Square test was used to determine statistical parameters in this model.
Prediction of the Incidence and Number of New Cases to 2034
The R package Nordpred was used to forecast the incidence and new cases of MSM by country to 2034 using a calibrated Age-Period-Cohort model (five-year age group and five-year interval). 20 The rates were forecasted using extrapolations from 3- to 5-year time frames, and the quantity was arrived at using model goodness-of-fit. To extrapolate the most recent 10-year linear trend, we attenuated the slope, as advised by the authors after empirical validation, by 25 and 50% for the second and third prediction periods, and by 75% for the fourth and fifth periods. 20 Applying the anticipated age-specific rates of the corresponding period to the anticipated global population (https://ghdx.healthdata.org/record/ihme-data/gbd-2019-population-estimates-1950-2019) allowed for the prediction of the number of new cases. 20
Statistical Analysis
Statistical analyses were performed with R software (version 4.2.2). A P-value of .05 or less was regarded as statistically significant.
Results
Global MSM Burden
The Age-Standard Rate of MSM, Incident Cases, and Temporal Trends Between 1990 and 2019.

ASR, age-standardized rate; CI, confidence interval; EAPC, estimated annual percentage change; UI, uncertainty interval.
ASR*: ASR per 100,000.

The prevalence of MSM in 204 countries and territories for both sexes. (A) The ASR of MSM incidence in 2019; (B) the change in MSM incident cases relative to 1990 to 2019; and (C) the EAPC of MSM ASR from 1990 to 2019. Annotations were made for nations or areas with an unusually high number of cases. ASR, age-standardized rate; EAPC, estimated annual percentage change; MSM, malignant skin melanoma.
The Influential Factors for ASR and EAPC Incidence
EAPC, ASR (in 1990), and HDI (in 2019) were found to have a significant relationship. MSM ASR in 1990 is a measure of the disease reservoir at the time, whereas HDI in 2019 measures the level of health care provided in each country. When the ASR was less than 10 per 100,000, it was positively correlated with EAPCs (ρ = .30, P .001) (Figure 2(A)). Furthermore, a significant positive relationship was found between HDIs and EAPCs (ρ = .63, P .001), indicating a faster increase in MSM ASR for countries with higher HDIs from 1990 to 2019 (Figure 2(B)). As for SDI, high SDI regions or countries, including those in Western Europe, high-income North America, and Australasia recorded the highest corresponding ASR of MSM incidence, as shown in Figures 2(C) and (D). MSM’s EAPCs at the global, regional, and national levels. The relationship between EAPC and MSM (A) ASR in 1990 and (B) HDI in 2019. The circles represent countries whose HDI data was available. The circle grows in size as the number of MSM cases increases. Statistical analysis was carried out using Pearson correlation analysis. Age-standardized rates of malignant skin melanoma incidence by Socio-demographic Index for 18 GBD regions (C) and 204 countries and territories (D), 1990-2019. ASR, age-standardized rate; EAPC, estimated annual percentage change; HDI, human development index; MSM, malignant skin melanoma.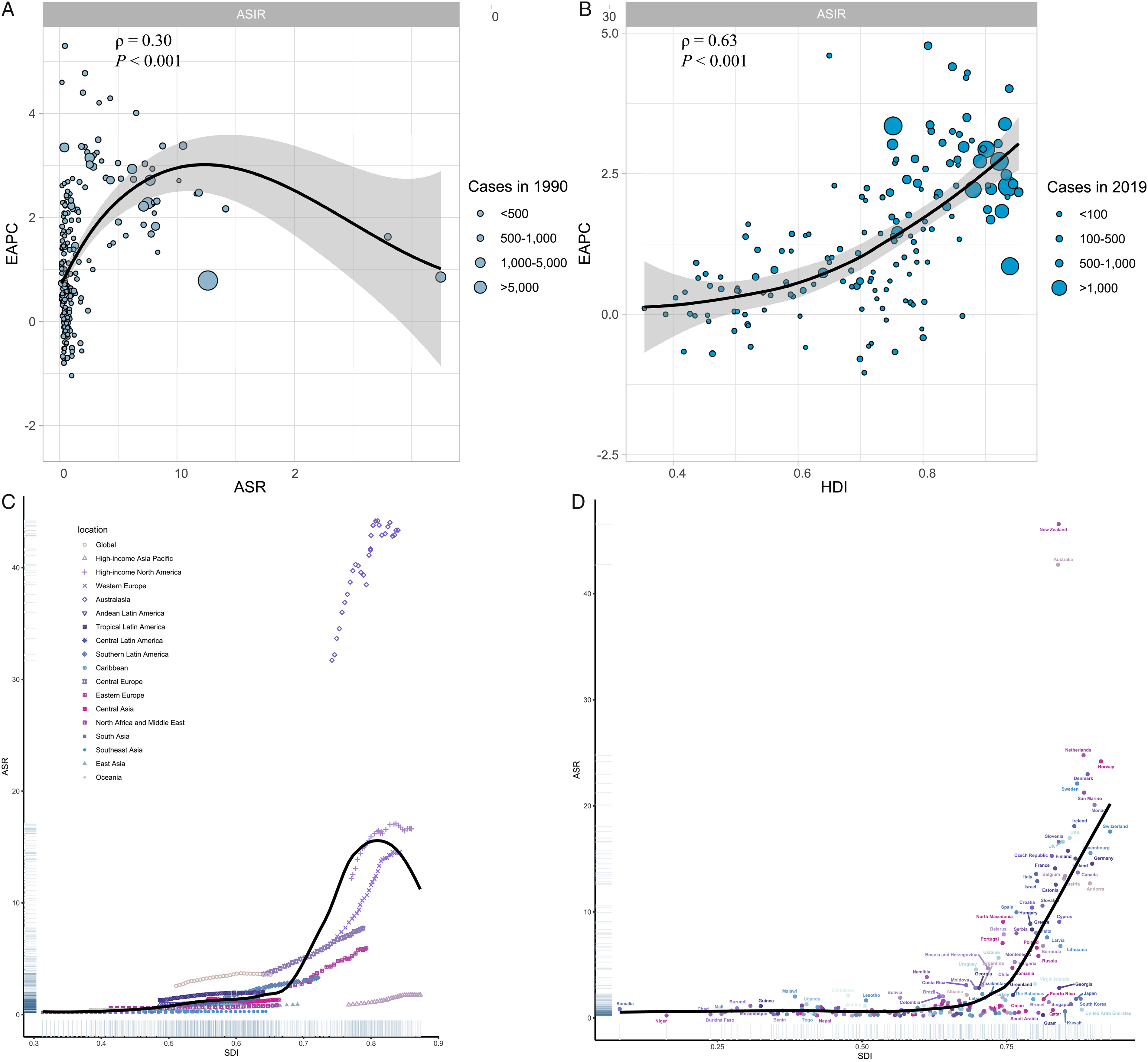
Joinpoint Regression Analysis
According to joinpoint regression, the most significant upward trends in incidence rates were found to be in the Republic of Korea (AAPC = 4.903%, 95% CI 4.596–5.211), Belarus (AAPC = 4.61%, 95% CI 4.41–4.811), and Portugal (AAPC = 4.395%, 95% CI 4.183–4.608), (Supplementary Table 4). Over the entire period, the majority of these countries showed an increasing trend in MSM incidence.
The Age-Period-Cohort Analysis of the Mortality Rate of MSM from 1990 to 2019
The time-trend analysis for the global cohort revealed that the overall MSM mortality rate decreased with a significant annual percentage change (Net Drift) of −.61%. The mortality rates were decreasing for age groups <77.5 years, as shown in Figure 3, with an estimator of the age-specific annual percentage change (Local Drifts) of −.038% (Figure 3(J)), but increasing for age groups of 82.5 or older, with a Local Drifts of .21%. The effect of age on the mortality rate (Figures 3(A), (D), (F), and (G)) showed a tendency of drop-rise-drop. The period effect of the period on the mortality rate of MSM was also investigated (Figures 3(B), (H), and (I)). Prior to the year 2002, there was a higher risk of death during the RRs period, which tended to trend slowly downward from 1990 to 2019 (Figure 3(I)). The cohort RRs showed that the mortality rates for those born before the period of 1950–1960 were higher than those for those born after the period of 1950–1960 and that these mortality rates gradually decreased for those born after the period of 1950–1960 (Figures 3(C) and (E)). Analysis of the Age-Period-Cohort model to determine the long-term trends of mortality from malignant skin melanoma between 1990 and 2019.
Prediction of MSM Incidence and New Cases to 2034
According to the predictive analysis, there will be 1,864,477.14 new cases of MSM worldwide in the years 2030 to 2034 (Figure 4(B)), with people aged 75 to 79 having the highest incident rate (Figure 4(C)). Predicted ASRs for MSM incidence during this time range from 6.95 between 2020 and 2024, 6.93 between 2025 and 2029, and 6.85 between 2030 and 2034. (Figure 4(A)). The age group of 70 to 74 years is expected to have the highest incidence of MSM, with 90,637.56 females and 127,471.44 males (Figure 4C)). Furthermore, in the period 2030–2034, the age group of >85 years will have the highest incidence rates of 20.41 in males and 17.20 in females (Figure 4(D)). Worldwide MSM ASR incidence (A) and incident cases (B) prediction analysis. Age-standardized rate, malignant skin melanoma, and ASR are the same thing. Predictive analysis of MSM incident cases (C) and incidence rates (D) worldwide, broken down by age and sex. 1–4 years to 85+ years, with a 5-year interval between each age group, is the order of age groups for each period from bottom to top. MSM, malignant skin melanoma; ASR, age-standardized rate.
Discussion
Global MSM incidences are noticeably different due to the heterogeneous pattern of risk factors. Generally, between 1990 and 2019, MSM incidence and cancer cases increased globally, but the temporal trends of MSM incidence varied greatly by region and nation. In our study, Australasia was found to have the highest incidence of MSM, with ASR more than 100 times that of Asia. Environmental factors and genetic predisposition are the two principal causes of this disparity. An earlier study found that the spectrum of driver mutations strongly implicated ultraviolet light as a direct mutagen in melanogenesis. 21 According to estimates, 63% of MSM are thought to be born in Australia, where ultraviolet radiation levels are roughly three times higher. 22 Furthermore, a possible direct or indirect relationship between MSM susceptibility genes (CDK4R24C, BAP1 (Y646X), MC1R-PTEN axis) and UV radiation has been suggested.23–25 Furthermore, ethnic differences in MSM susceptibility genes exist, which may explain some of the geographic and ethnic variations in MSM incidence. Therefore, identifying the ethnicity-specific influence of susceptible genes on the MSM risk in various ethnic groups may offer insightful information about the possible root causes of racial MSM as well as personal susceptibility, facilitating the implementation of focused preventive measures.
The HDI and SDI are indicators of human and societal development, respectively. A positive correlation between HDI and EAPC was discovered in this study, indicating that countries with high HDI have a more rapid increase in MSM ASR. At this time, East Asia, which was previously thought of as a low-incidence region, had the highest EAPC of MSM incidence in ASR from a global perspective. This could be primarily attributed to East Asia’s recent rapid development and higher rates of neoplasm detection. Early detection strongly depends on the HDI-people in countries with high HDI who can afford the related primary health care costs. Furthermore, regions with high SDI, such as Australasia, High-Income North America, and Western Europe, also had high ASR of MSM incidence. Australasia, as a high SDI region, is frequently used as a model for discussion. In addition to the sunbathing habit, as a result of their colonial history, the majority of Australasian people trace their ancestry to English, Scottish, or Irish ancestors. Additionally, these populations frequently lack much of the naturally occurring intrinsic photoprotection offered by cutaneous melanin, which could partially account for the high incidence of MSM found in particular geographic areas. 26
Although the incidence of MSM mortality is still increasing globally, the Age-Period-Cohort analysis revealed a lower MSM mortality rate for the global cohort. MSM mortality rates for those over 82.5 years old, on the other hand, are rising. According to this, increased mortality rates among the elderly may be due to the increased prevalence of MSM. Additionally, improvements in the systematic treatment of MSM have marginally increased overall survival, which has led to a delayed recurrence or metastasis. 27 Our predictive results show that, while the global ASR of MSM is slowly decreasing, the global disease rate remains significant. The number of incident cases will reach two million globally between 2030 and 2034, with the age groups of 85 and over and 70 to 74 years having the highest incidence rates and incident numbers, respectively. The burden of MSM disease will increase as the world’s population ages. Additionally, the incidence trend revealed that Asia had the highest rate of MSM occurrence in recent years. This could be attributed to population expansion, population aging, and opportunistic screening.
Global Cancer Observatory (GLOBOCAN) 2020 is a global online cancer database conducted by the International Agency for Research on Cancer’s (IARC) Global Cancer Observatory of the World Health Organization. 28 Sung et al provided age-standardized incidence or mortality rates per 100,000 person-years, utilizing the 1966 Segi-Doll World standard population as a reference. Additionally, they offered the cumulative risk of developing or succumbing to cancer before reaching the age of 75 years, assuming no interference from other causes of death, expressed as a percentage. For the majority of diseases and injuries in the GBD dataset, processed data undergo modeling with standardized methodologies to produce estimates for each relevant parameter, considering factors such as age, gender, geographical location, and year. These estimates are generated using three primary standardized tools: the Cause of Death Ensemble model (CODEm), spatiotemporal Gaussian process regression (ST-GPR), and DisMod-MR.29,30
Incidence trends for skin cancers, including MSM locally or globally, as well as links between MSM and socioeconomic advancement, have also been shown by other studies. The incidence, prevalence, and mortality rates of melanoma and non-melanoma skin cancer in the United States were reported by Aggarwal et al. 31 Laughter et al 32 discovered the significant burden of skin and subcutaneous disease as well as regional differences in MSM disability-adjusted life-years (DALYs) rate trends. Skin cancer incidence, mortality, and disability-adjusted life-years (DALYs) trends over the past few decades were demonstrated by Zhang et al 33 on a global, regional, and national level. The disease burden of MSM in Canada and Asia was also revealed by Bridgman 34 and Urban, 35 respectively. However, our study is the first to concentrate on the overall impact of MSM and to display trends in incidence as well as predictions for the future. Using the GBD 2019 data, we investigate the long-term trends in the incidence of and mortality from MSM between 1990 and 2019 using the Age-Period-Cohort framework. Furthermore, we use the R package Nordpred to forecast the incidence and new cases of MSM by country through 2034 using a calibrated Age-Period-Cohort model. This study revealed that MSM incidence has been on the rise globally over the study period, with the exception of the age group >82.5 years old, where it has been steadily declining. Additional predictive findings show that, despite the MSM ASR gradually declining, the MSM incident number will continue to rise, particularly in the older population. These findings may serve as a guide for governments as they develop targeted interventions, especially those that focus on sun protection, early diagnosis, and public awareness of melanoma.
Conclusion
In summary, melanoma incidence demonstrates substantial variation across regions and nations. Our research and the ensuing discussion underscore the urgent necessity for enhancing melanoma registration, comprehending the diversity of melanoma risk factors in different regions and countries, and conducting an impartial evaluation of the health care systems’ capability to detect, document, and manage melanoma cases. Such investigations are essential for laying the groundwork for comprehensive strategies that encompass health care promotion, education, and cancer control programs, with a particular emphasis on sun protection, early diagnosis, and raising public awareness about melanoma.
Limitations
The most important limitation is the fact that melanoma reporting is often inaccurate, under-reported in some countries, and unpredictable.36,37 There are a few countries whose reporting is considered to be fairly complete such as the US and Switzerland. As for Qatar, the incidence of MSM had a 15-fold increase over a relatively short period of time. It could be concluded that it is primarily a reflection of reporting-low reporting at one earlier point with far improved reporting at a more recent point.
Supplemental Material
Supplemental Material - Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034
Supplemental Material for Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034 by Jin Yuan, Xiaoyang Li, and Shengji Yu in Cancer Control
Supplemental Material
Supplemental Material - Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034
Supplemental Material for Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034 by Jin Yuan, Xiaoyang Li, and Shengji Yu in Cancer Control
Supplemental Material
Supplemental Material - Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034
Supplemental Material for Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034 by Jin Yuan, Xiaoyang Li, and Shengji Yu in Cancer Control
Supplemental Material
Supplemental Material - Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034
Supplemental Material for Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034 by Jin Yuan, Xiaoyang Li, and Shengji Yu in Cancer Control
Supplemental Material
Supplemental Material - Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034
Supplemental Material for Global, Regional, and National Incidence Trend Analysis of Malignant Skin Melanoma Between 1990 and 2019, and Projections Until 2034 by Jin Yuan, Xiaoyang Li, and Shengji Yu in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No.82272964; No.82002848; No.82003397); the CAMS Innovation Fund for Medical Sciences (CIFMS) (2021- I2M-C&T-B-054, 2021-I2M-C&T-B-053), the Capital Characterized Clinical Application Research Fund of Beijing Municipal Science and Technology Commission of China (No. Z171100001017210); the Fundamental Research Funds for the Central Universities (No. 3332021097); the Beijing Hope Run Special Fund of Cancer Foundation of China (No. LC2021A14).
Ethical Statement
Our study did not require an ethical board approval because it did not contain human or animal trials.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.