
Abstract
Background and Objectives
Primary cutaneous leiomyosarcoma (cLMS), a rare, typically intradermal tumor, has previously been reported to exhibit an indolent course of disease with zero-to-low risk of local recurrence or distant metastasis. This study seeks to evaluate recurrence and survival of cLMS patients through study of its clinicopathologic and treatment characteristics.
Methods
All patients included underwent resection of primary cLMS at this institution between 2006 and 2019. A retrospective cohort study analysis of clinicopathologic characteristics, treatment, recurrence, and overall survival was performed. Data was assessed through descriptive statistics and outcome measures assessed by Cox proportional models and log-rank tests.
Results
Eighty-eight patients with cLMS were evaluated. The majority were men (n = 68, 77%) and Caucasian (n = 85, 97%), with median age at diagnosis of 66 years (range 20–96). 65% of tumors were located on the extremities, with a median size of 1.3 cm (range .3–15). Assessment revealed low (n = 41, 47%), intermediate (n = 29, 33%), and high (n = 18, 20%) grade tumors, demonstrating extension into subcutaneous tissue in 38/60 (60%), with 3 patients exhibiting extension into muscle (3%). All underwent resection as primary treatment with median 1 cm margins (range .5–2). With median follow-up of 27.5 months (IQR 8–51; range 1–131), no low-grade cases had recurrence or death while there was a recurrence rate of 19.1% (9/47) and death rate of 8.5% (4/47) in intermediate- to high-grade cases.
Conclusions
Primary tumor resection of cLMS provides excellent local control for low-grade tumors as no low-grade cases experienced recurrence. For patients with intermediate- to high-grade tumors, there is potential for local recurrence, distant metastasis, and death, and therefore surveillance following treatment is encouraged.
Introduction
Cutaneous leiomyosarcoma (cLMS) is a rare mesenchymal neoplasm which develops within the dermis and may ulcerate or extend into the subcutaneous tissue. 1 cLMS accounts for approximately 2% of cutaneous soft tissue sarcomas, occurring more frequently in Caucasian men with no anatomical predilection and increasing incidence with older age. 2 The histologic cell of origin is thought to be from the arrector pili muscle, or areola complex, and tumors are characterized by nodular or diffuse interlacing fascicles of spindle cells. Tumor cells may exhibit a variable mitotic rate and have nuclei which are typically elongated with blunt edges; nuclei may also be enlarged, hyperchromatic, or irregular. 3 Immunohistochemical staining reveals positivity for smooth muscle actin, vimentin, desmin, and h-caldesmon and negativity for S-100. 4 There is no recommended staging system to aid in the prognostication of cLMS as neither system specifies use for soft tissue sarcomas stratified by depth. However, the Federation Nationale des Centres de Lutte Contre Le Cancer (FNCLCC) 5 sarcoma grading system, based on tumor differentiation, mitotic rate, and degree of necrosis, integrates within the American Joint Committee on Cancer (AJCC) 8th edition 6 to provide the classification of soft tissue sarcomas.
The clinical behavior is correlated to the depth of invasion with cLMS demonstrating a more benign tumor biology than leiomyosarcoma (LMS) arising within the subcutaneous tissue. It is therefore critical to evaluate the entire depth of the tumor to assess its origin. 3 In fact, based on the low rate of recurrence and absence of metastases, the name “atypical intradermal smooth muscle neoplasm” was proposed in 2011 for these tumors 7 and is offered as an interchangeable term rather than distinct pathologic entity. 8 First-line treatment is complete surgical excision with negative margins. Definitive recommendations for margin of excision are lacking, with some proponents of 2–5 cm for cLMS and subcutaneous tumors,9,10 while other authors have reported excellent outcomes with a 1 cm margin.11,12 The risk of local recurrence has been reported to range from 0% for 67% for cLMS and 19% to 40% for subcutaneous LMS,9,11-15 with ability to attain clear margins being one of the most important factors in predicting recurrence. 12 Rates of metastasis have been reported in studies to be 0%-14% for cLMS and 27%-63% for subcutaneous LMS,9,11-15 with histologic grade, size, necrosis, and subcutaneous presence increasing the likelihood of metastasis. 3 Currently, there is no consensus as to whether cLMS has metastatic potential or if secondary extension into the subcutaneous tissue confers worse prognosis.3,7,12,13
Deneve et al 11 previously reported a series of 33 consecutive patients, noting no locoregional recurrence, distant metastasis, or deaths over a median follow-up time of 15 months. The present study aims to expand this cohort and utilize these findings, using a 9 year update of the previous dataset to report the recurrence-free survival and secondarily overall survival outcomes of cLMS patients. This study serves as the largest report of the clinical, pathologic, and treatment characteristics of this rare tumor while also describing prognostic value of applying the FNCLCC grading system to this rare diagnosis given that the AJCC 8th edition staging manual for soft tissue sarcoma does not account for cutaneous LMS.
Materials and Methods
FNCLCC Histologic Grading System. 22

FNCLCC: Federation Nationale des Centres de Lutte Contre Le Cancer. HPF: High-powered field, assessed using a 40× objective.
Statistical Analysis
Hazard ratios (HRs) for recurrence-free survival (RFS) were assessed by Cox proportional models and log-rank tests. To build the univariable Cox proportional hazard model, Firth’s penalized maximum likelihood estimation was used. To build the multivariable Cox proportional hazard model, backwards selection was used to eliminate non-significant variables and an alpha level of .2 was chosen. A P-value <.05 was considered statistically significant. All analyses were performed using R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org).
Results
Patient and Tumor Characteristics
Patient Characteristics, Treatment, and Outcomes.

Pathologic assessment revealed low (n = 41, 47%), intermediate (n = 29, 33%), and high (n = 18, 20%) grade tumors. Mitotic count was recorded in 89% (n = 78) of patients. Mitotic count scores were as follows: score of 1, n = 42/78, 54%; score of 2, n = 17/78, 22%; score of 3, n = 19/78, 24%. Tumor differentiation was recorded in 80% (n = 70) of patients. Tumor differentiation scores were as follows: score of 1, n = 34/70, 49%; score of 2, n = 31/70, 44%; score of 3, n = 5/70, 7%. Percentage of tumor necrosis was recorded in 48% (n = 42) of patients. Tumor necrosis scores were as follows: score of 0, n = 33/42, 79%; score of 1, n = 9/42, 21%; score of 2, n = 0/42, 0%.
A total of 41 specimens were eligible for complete FNCLCC grading (all 3 score values reported). Grade 1 was classified in 59% (n = 24/41), grade 2 was classified in 29% (n = 12/41), and grade 3 was classified in 12% (n = 5/41). Of those 41 patients with FNCLCC grading, scoring breakdowns were as follows: mitotic count score of 1, n = 22/41, 54%; score of 2, n = 11/41, 27%; score of 3, n = 8/41, 19%; tumor differentiation score of 1, n = 25/41, 61%; score of 2, n = 15, 37%; score of 3, n = 1/41, 2%; tumor necrosis score of 0, n = 32/41, 78%; score of 1, n = 9/41, 22%; score of 2, 0/41, 0%.
Immunohistochemistry was positive for smooth muscle actin (n = 69/70, 99%) and desmin (n = 60/70, 86%), while negative for S-100 (n = 62/62, 100%). The single tumor negative for smooth muscle actin was positive for desmin, and therefore no tumors were found to be negative for both smooth muscle actin and desmin. Preoperative tumor grading based on the biopsy was discordant with postoperative final pathology in only 6 (7%) patients, of which 5 increased while 1 decreased in grade severity. Tumor was confined to the dermis in 47 patients (53%). Extension from the dermis into the subcutaneous tissue was seen in 38 patients (43%) and extension into the muscle was noted in 3 patients (3%) (Table 2).
Treatment and Outcomes
All patients underwent surgical resection as primary treatment with a median of 1 cm planned surgical margins (range .5–2 cm). The planned surgical margin was not described in 3 patients. Final pathologic margins were R0 in 99% (n = 87) and R1 in 1% (n = 1). Sixty (68%) patients received preoperative imaging of the chest with PET (n = 5, 6%), CT (n = 37, 42%), MRI (n = 2, 2%), or plain film radiography (n = 15, 17%), none of which demonstrated distant metastasis. Preoperative imaging was performed or deferred at the discretion of the attending surgeon of record. One patient received preoperative treatment with a partial regimen of radiation therapy prior to referral to our institution, which was discontinued upon referral. No patient received preoperative systemic therapy. Seven (8%) patients received adjuvant radiation to the primary site with a median dose of 62 Gy (range 60–66 Gy). For the seven patients who received adjuvant radiation, tumor characteristics were as follows: median planned surgical margin of 1 cm (range .1–2 cm); final pathologic margin of R0 in 100% (n = 7/7); tumor grades of low (n = 2/7), intermediate (n = 3/7), and high (n = 2/7); median tumor size of 1.5 cm (range .7–8 cm); with recurrence prior to radiation in 2 of 7 patients. No patients received adjuvant chemotherapy (Table 2).
Over a median follow-up of 27.5 months (IQR 8–51 months), recurrence was identified in 9 patients (10%; local, n = 3; local and regional, n = 1; local and distant, n = 2; distant, n = 3). Overall median time to recurrence was 24 months (range 7–82 months). Median time to local recurrence was 16 months (range 7–82 months), while median time to distant recurrence was 34 months (range 14–62 months). No patients with pathologic low-grade tumors experienced recurrence. All 9 patients with recurrences had intermediate-to high-grade tumors on pathological evaluation. Of those who recurred, the median clinical tumor size was 2 cm (range .3–4 cm) and had preoperative imaging with PET/CT (n = 6), CT chest (n = 1), or none (n = 2). Site of recurrence was evenly distributed across site of primary tumors, divided between the extremity (n = 3), trunk (n = 3), and head/neck (n = 3). Seven (78%) of these patients had tumors that extended into the subcutaneous tissue, 1 (11%) extended into the muscle, and 1 (11%) was strictly intradermal. Extended oncologic resection did not definitively preclude recurrence as 7 (78%) of the 9 patients with recurrence had resection that included at least underlying fascia. Four (4.5%) patients died of disease at median 3.3 years; all of whom at diagnosis had intermediate- to high-grade tumors sized 1.8–3 cm located on the head/neck or trunk and had biopsy-proven recurrent distant disease (Table 2).
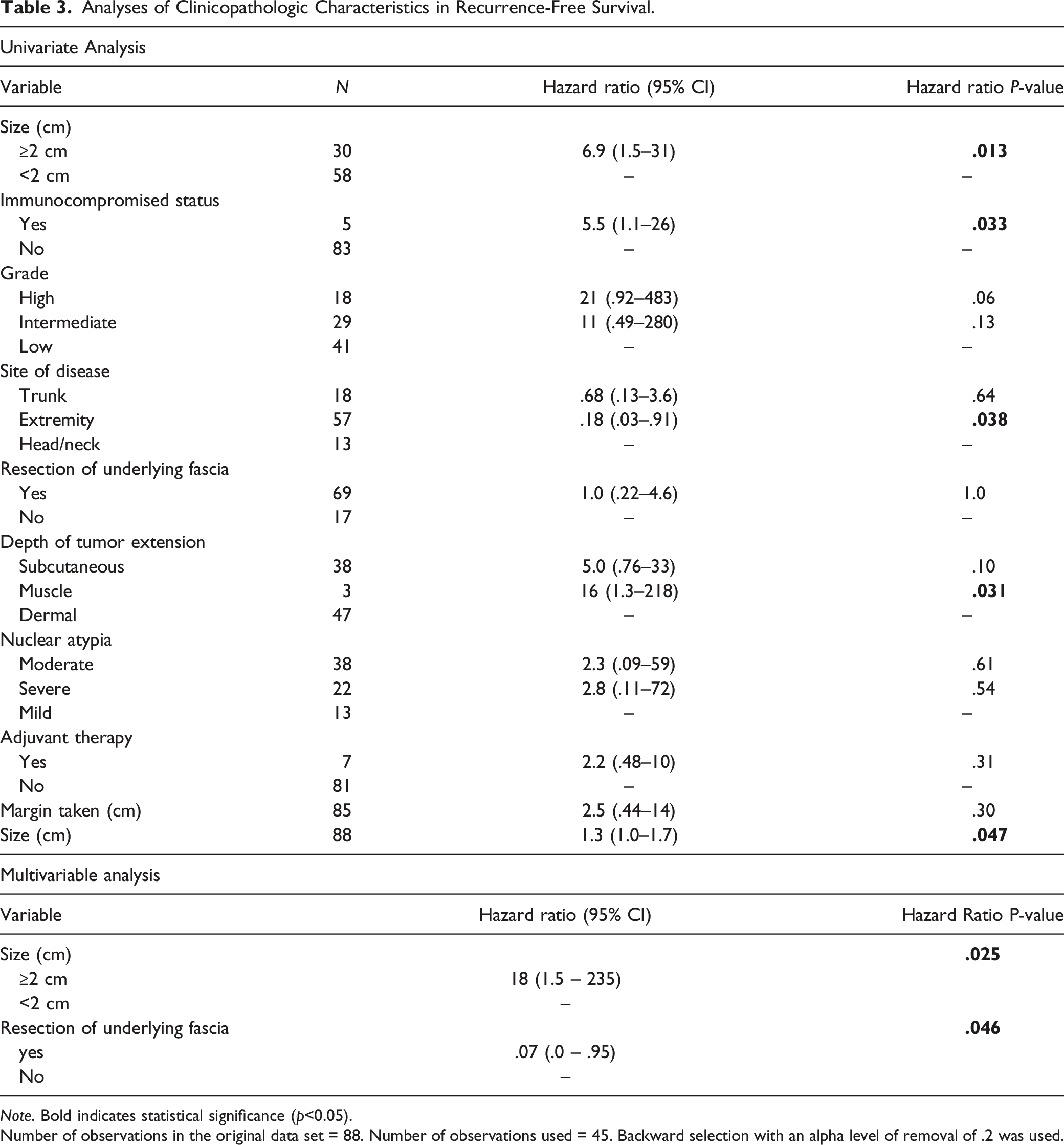
On univariate analysis, patients with intermediate- and high-grade tumors had significantly worse RFS compared to those with low-grade tumors (HR 11 [95% CI .49–280] and HR 21 [95% CI .92–483], respectively, P = .015). Other variables predicting worse RFS included immunocompromised status (HR 5.5 (95% CI 1.1–26), P = .037), primary tumor size ≥ 2 cm (HR 6.9 (95% CI 1.5–31), P = .002), primary tumor location, with those found on extremities (HR .18 (95% CI .03–.91) and trunk (HR .68 (95% CI .13–3.56) having significantly better RFS than that of in the head/neck (P = .049), and invasion beyond the dermis (subcutaneous tissue HR 5.0 (95% CI .76–33 and muscle HR 17 (95% CI 1.29–218), P = .041) (Figure 1). There was no significant difference in RFS among degree of nuclear atypia, surgical margin, resection of underlying fascia, or use of adjuvant radiation (Table 3). On multivariate analysis, tumor size ≥ 2 cm (HR 18 (95% CI 1.5–234), P = .025) and resection of the underlying fascia were significant for risk of recurrence (HR .07 (95% CI .00–.95), P = .046). Tumor grade, depth of extension, location, and resection margin were removed in the backward variable selection step for building the final parsimonious model in the multivariate analysis (Table 3). Recurrence-Free Survival Across Significant Variables. (A) Risk of recurrence by size of primary tumor, < or ≥2 cm. (B) Risk of recurrence by site of primary tumor development, stratified by head and neck, trunk, and extremity tumors. (C) Risk of recurrence by low, intermediate, and high grade as determined by the FNCLCC system. (D) Risk of recurrence by depth of extension, stratified by dermal, subcutaneous, and muscle invasion. Analyses of Clinicopathologic Characteristics in Recurrence-Free Survival. Note. Bold indicates statistical significance (p<0.05). Number of observations in the original data set = 88. Number of observations used = 45. Backward selection with an alpha level of removal of .2 was used.
Discussion
Cutaneous leiomyosarcoma is an exceedingly rare cutaneous tumor, and data are lacking to guide treatment and surveillance for these patients. This report offers this guidance as the largest single cohort of cLMS presented to date with updates from a previously reported single-institution series. 11 Consistent with the previous analysis, preoperative imaging seemed to have little added benefit as evidence of metastasis was not seen in any of the patients with thoracic or full body imaging. With a larger cohort size and longer follow-up, recurrence was identified in 9 patients at a median of 24 months, and metastasis was found in 6 patients at a median of 27 months, of whom 4 died of disease at a median of 40 months.
Although soft tissue LMS has been shown to have worse oncologic outcomes when compared to cLMS, few studies have directly evaluated purely dermal cLMS vs cLMS with subcutaneous extension. In the current study, tumors with subcutaneous extension were found to have significantly higher risk of recurrence than strictly dermal tumors, in line with previous studies investigating depth of invasion.7,17 Yet, cLMS limited to the dermis does have at least a limited capacity to recur and metastasize, as seen in one patient in the current series and previously reported in several others.12,14,18 Previous studies have reported exceptionally low or even zero risk of cLMS recurrence and metastasis to the point of some groups advocating reclassification outside of sarcoma.7,13,15,17,19,20 The current study data do not support the idea that cLMS without subcutaneous extension is benign, as tumors confined to the dermis were shown to have metastatic potential, corroborating studies which have also observed occurrence of distant metastasis and death.12,14,18,21
Applying the FNCLCC grading system to cLMS may aid in the prognostication of these tumors, as severity of grade clearly stratified patients for risk as recurrence was seen only in intermediate- or high-grade tumors. No patient in the current study with low-grade cLMS as categorized by the FNCLCC grading system developed recurrence, metastasis, or death, congruent with other studies stratifying tumors by FNCLCC grade.14,17 Low-grade cLMS has been reported to recur in the literature, but the majority of those recurrences were associated with incomplete excision of the primary. 7 In addition to the FNCLCC histologic grade cLMS, primary tumor size should also be incorporated in treatment algorithms. The tumor diameter categories as currently defined by the AJCC 8th edition for soft tissue sarcoma with a cutoff of 5 cm are reasonable for subfascial LMS but are rare in cLMS. These data demonstrate a higher risk of recurrence in tumors ≥2 cm than tumors with size < 2 cm. This offers an objective data point, in addition to tumor grade, that can be used in treatment algorithms for cLMS.
Due to low incidence of cLMS, standardized treatment approaches have not been presented but the data in this report yields objective endpoints for branch points in a treatment pathway. The determination of clinical risk of cLMS should include histologic grade, size, and location of the primary tumor, and treatment plans should incorporate these features. Pathway. Initial treatment with surgical resection margins of at least 1 cm should be performed with negative margins attained.7,10 There is no need for routine preoperative imaging aside from circumstances with a high clinical suspicion that the cutaneous disease represents a metastasis or with disease presenting with an increased clinical risk as evidenced by factors such as large size (≥2 cm) and intermediate- to high-grade. The benefit of adjuvant treatment with chemotherapy remains unknown and thus should be deferred, with chemotherapy recommended only for distant metastasis. Adjuvant radiation should be administered on an individualized basis after multidisciplinary discussion in the setting of positive postoperative margins with limited ability for further resection or intermediate- to high-grade tumors ≥ 2 cm.4,17 Nomenclature is important, and the distinction on pathologic evaluation between degree of subcutaneous invasion among tumors is standardized in this report. Where other studies may describe cutaneous vs subcutaneous tumors, the current report describes cutaneous vs cutaneous with subcutaneous extension. To ensure consistent reporting of data, future studies should leverage the nomenclature and approach to grading presented in this report to generalize results. The low incidence of cLMS requires this multi-institutional cooperation regarding data reporting and interpretation.
The retrospective nature of this study is a limitation as selection bias certainly exists. Despite this, patients were carefully selected for eligibility and all data was collected and validated in the same manner to minimize bias in reported data. Regarding inclusion criteria, performance of preoperative imaging was not consistently performed and therefore may have influenced the results of regional and distant recurrence outcomes. Due to the low incidence of cLMS, a power calculation for estimation of sample size selected for the study was not done in lieu of reporting all confirmed cases of cLMS at this single institution. Given the fact that the FNCLCC grading criteria is not widely adopted in the United States, this information was not available for all patients in this study, which limits its statistical power. No pathology review was performed to confirm the pathologic data, and half of the cases did not have documentation of all three parameters utilized to determine tumor grade.
Conclusions
Excellent local control with an almost 90% local recurrence-free survival was seen in this large cohort, and no patients with low-grade tumors experienced a recurrence. For patients with intermediate- to high-grade disease, there is potential of recurrence and death, and therefore clinical surveillance following treatment is encouraged, though data are not sufficient for definitive imaging interval assessment. Considering the lack of a specific staging system for cLMS, establishing risk stratification for these patients delineated by FNCLCC grade in conjunction with tumor depth and size may provide a straightforward evaluation for discussion of prognostic risk as well as a framework for future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported in part by the Biostatistics and Bioinformatics Shared Resources at the Moffitt Cancer Center & Research Institute, an NCI-designated Comprehensive Cancer Center (P30-CA076292).