
Abstract
Radiotherapy (RT) is an important component of the treatment of soft tissue sarcomas (STS) and has been traditionally incorporated with a homogenous approach despite the reality that STS displays a known heterogeneity in clinicopathologic features and treatment outcomes. In this article, we explore the principle components of personalized medicine, including genomics, radiomics, and treatment response, along with their impact on the future of radiation therapy for STS. We propose a shift in the treatment paradigm for STS from a one-size-fits-all technique to one that implements the tenets of personalized medicine and includes the framework for a potential clinical trial technique in this heterogeneous disease.
Introduction
Soft tissue sarcoma (STS) is a rare disease representing approximately 1% of the cancer incidence in the United States. 1 Soft tissue sarcoma is a diverse disease consisting of dozens of histologies with substantial heterogeneity, both between patients (intertumor heterogeneity) and within the tumor itself (intratumor heterogeneity). 2 –4 The majority of STS occurs within the trunk and extremities but can occur anywhere, including the head/neck region, retroperitoneum, skin, and visceral organs. This requires proper radiotherapy (RT) technique and careful treatment modification based on the anatomic location. The current standard of care for STS typically incorporates surgical resection and depending on a patient’s clinical risk factors the addition of radiation therapy and chemotherapy. Radiation therapy is commonly delivered with either external beam radiotherapy (EBRT) or internal radiotherapy (brachytherapy). Typically, EBRT is delivered with conventional fractionation to either 4500 to 5000 cGy preoperatively or 6000 to 7000 cGy postoperatively, with little deviation from this formula. 5 Advances made in the field of radiation oncology over the past century have created or expanded upon the use of intensity-modulated radiotherapy (IMRT), image-guided radiotherapy, stereotactic body radiotherapy, particle-based therapy, and brachytherapy. Despite these improvements in treatment techniques, the current approaches continue to result in local recurrences rates approaching 20%, the majority of which occurring within the treatment field, suggesting a degree of inherent radioresistance. 5 –8
Regardless of the vast heterogeneity in STS, the current standard of care is a uniform radiation dose delivered homogenously to the entire tumor, regardless of histology, grade, or obvious radiographic intratumoral heterogeneity. The careful construction and utilization of next-generation disease characterization will aid in building the framework of a personalized treatment approach. In this article, we will explore the core principles of personalized medicine and our group’s efforts to advance the future of radiation oncology.
Genomics
The utilization of genomics-based treatment has a clear and important role in medical oncology, with selection of patients who will benefit from cytotoxic chemotherapy, immunotherapy, and other targeted therapies. 9 –11 In STS, gene expression was utilized to characterize 12 and stratify subtypes based on tumor behavior, such as metastatic propensity. 13 Chromosomal-based heterogeneity has also predicted for STS progression and metastatic dissemination. 14,15
Tumor Heterogeneity
Soft tissue sarcoma is characterized by heterogeneous genomic features and gene expression. 4 Francis et al showed that significant variability in gene expression profiles exist not only among tumors but also within the tumor itself. 12 In STS, there is also evidence of intratumor karyotype and chromosomal heterogeneity. 3 This heterogeneity has made it difficult to accurately identify patients who would most benefit from treatment deintensification and/or intensification, such as modulating radiotherapy dose or considering adjuvant systemic therapies. This variance in treatment response is linked with both intratumoral and intertumoral genomic heterogeneity, with subclonal tumor populations with distinct gene expression profiles that may correspond to their response to various treatment modalities. 4,13,16 –19 These findings provide insight into the potential to improve outcome by applying radiation dose heterogeneously, or “dose painting,” based on the distinct subclonal populations throughout the tumor, rather than the typical homogenous dose distributions that are currently used.
Tumor Radiosensitivity
In an effort to utilize a clinically relevant systems biology model, our group has developed a genome-based radiosensitivity index (RSI) that has been clinically validated in multiple cancer sites, including STS. 20 A low RSI score indicates higher radiosensitivity, whereas a high RSI score correlates with cellular radioresistance. 21 –24 Sarcomas tend to lie in the more radioresistant end of the spectrum. 20 Preliminary RSI data of a small sample of sarcoma patients suggested a nonsignificant association between radioresistance and local failure, with local first failure occuring in 6 of 20 radioresistant lesions compared to failure in only 1 of 12 radiosensitive lesions (P = .21). 25 Although this study was underpowered to show a local control significance, it is intriguing and follows the associations observed in various other cancers tested. 20,26,27
Recently, Torres-Roca et al has utilized the gene expression-based RSI to derive a genomic-adjusted radiation dose (GARD)—a signature developed via multi-institutional collaboration evaluating breast, lung, pancreas, glioblastomas, and STS. The GARD independently predicted for clinical outcome of patients treated with radiotherapy in various disease sites tested. 20 Based on the genomically quantified tumor biology, a high GARD value translates to a higher equivalent radiation dose for the tumor, in turn predicting for a higher therapeutic effect with radiotherapy. In contrast, sarcoma and glioma had the lowest GARD values, which were statistically lower than any other disease site tested (P < .001) 20 This suggests that sarcoma is relatively radioresistant, requiring a higher radiation dose to achieve the same treatment effect as other disease sites. The use of GARD potentially translates into how we could modulate radiation dose in individual patients with sarcoma in an effort to improve outcomes.
Immunogenicity
Exploring the benefits of immunotherapy and RT in cancer treatment has continued to expand as an area of active interest in the current clinical trials. 28 Integrating tumor immunogenicity with radiosensitivity will further enhance the genomic-based prediction of STS outcome. In addition to RSI and GARD, Messina et al and Coppola et al have recently developed a genomic-based predictor of tumor immunogenicity—a 12-chemokine signature (12-CK). This signature is based on 12 chemokine genes (CCL2, CCL3, CCL4, CCL5, CCL8, CCL18, CCL19, CCL21, CXCL9, CXCL10, CXCL1 1, and CXCL13) chosen from a metagene grouping of genes related to immunity and inflammation, which predicted for improved disease outcome in colorectal cancer and metastatic melanoma. 29,30 This marker of immune activation was cross-compared with RSI in an exploratory analysis measuring activity of the immune system and found that low-RSI (radiosensitive) tumors had a significantly higher 12-CK level when compared to high-RSI (radioresistant) tumors. 31 This link was tested in early-stage breast cancer, which showed on multivariate analysis that RSI and 12-CK levels were associated with improved distant metastasis-free survival. 32
Preclinical and in vitro studies of STS cell lines have suggested potential targets for immune-modulating therapy, which include fusion proteins, cancer testis antigens, and specific targetable mutations. 33,34 Given this disease’s rarity and heterogeneity, traditional clinical trials are less than ideal in regard to accrual time and accurately depicting treatment response. To facilitate the advancement of the field in STS, the utilization of genomically based radiosensitivity (eg, GARD) and immunopredictors (eg, 12-CK) offers tools outside the generic clinicopathologic features used today (eg, histology, grade, size, and so on) to empower the clinician to adapt treatment based on the inherent tumor biology, thus optimizing patient outcome.
Radiomics
A variety of imaging studies ranging from computed tomography (CT), magnetic resonance imaging (MRI), and to a lesser extent fluorodeoxyglucose (FDG)-positron emission tomography (PET), are obtained routinely for staging and treatment planning purposes. 35 This acquisition of images has resulted in a plethora of data that have been underutilized to date. With technologic advances, computers can now aid in analyzing radiographic source material in ways the human eye cannot. This active area of cancer research, termed “radiomics,” has gained popularity in the last decade. 36,37 Radiomics refers to the conversion of images to structured and mineable data. 37 The exponential growth of imaging studies along with markedly increased quality has amplified the potential for radiomics in the clinical and research settings, as traditional use of imaging was limited by subjective visual interpretation. In contrast, radiomics allows for deeper interpretation of data not readily visible or quantifiable from visual inspection. In STS, radiomics has been associated with STS grade, 38 treatment response, 6 and outcome. 39
Tumor Heterogeneity
Since STS can occur at any site and is made up of diverse histologies, radiographic images (eg, MRI and CT) can assist in identifying a tumor histology and/or grade. In liposarcoma, it can be possible to distinguish between the well-differentiated and dedifferentiated component of a patient’s tumor on imaging. 11 This is overly simplistic, as we know that even morphologically identical areas within a sarcoma can possess distinct biomolecular intratumoral heterogeneity on mass spectroscopy. 40 Sarcomas can vary by grade, discrimination of which may be aided by PET 41,42 and CT. 38,43
Computed Tomography Radiomics
Imaging with CT is essential for RT treatment planning purposes, which provides an ideal basis for radiomic analyses. In CT radiomics, multiorder features not readily visualized on classic imaging interpretation include the following features: shape (size and geometrical shape), intensity histogram (distribution of voxel intensities), gray-level run length matrix (spatial relationships of voxel intensities), gray-level size zone matrix (characterize regions of similar gray level), neighborhood gray tone difference text (visual properties of texture), fractal dimensions (surface roughness of an image), and first-order wavelets (analyze coarse and fine textures) in a contoured region of interest. 44 The CT-based radiomics has shown promise in lung and head/neck cancers, wherein an imaging biomarker comprised of 4 radiomics features (shape, texture, tumor image intensity, and wavelet decomposition) was a significant prognostic indicator of intratumor heterogeneity. 45
Magnetic Resonance Imaging Radiomics
Local staging for STS is commonly defined based on MRI imaging. Various MRI sequences can help in determining tumor histology, grade, depth, size, and peritumoral edema, which can aid both in surgical and in radiation-based treatment planning. 35 Radiomics for these commonly obtained MRI sequences (eg, T1, contrast-enhanced T1 and T2 STIR images) can be analyzed either independently or in combination. There are data to suggest that radiomic analysis of STS can accurately distinguish intermediate and high-grade lesions, 38 degree of necrosis, 46 and patient outcome. 47
The Federation Nationale des Centres de Luttre Contre le Center (FNCLCC) grading system is most commonly used, which takes into account mitosis rate, degree of necrosis, and tumor differentiation. 48,49 Corino et al evaluated 19 patients with STS analyzing 65 radiomic features and found that intermediate-grade STS had a higher and less disperse apparent diffusion coefficient (ADC) values. Utilizing first-order radiomic features, they showed that high-grade STS can be identified with 90% accuracy and 85% area under the curve (AUC) predictive power. 38 The ability to differentiate tumor grade may have diagnostic and therapeutic implications and offers clinicians the potential for modifying treatment-based difference in grade between patients and potentially within the tumor. Additional MRI radiomic features evaluated includes intensity, gradient, and curvature, which have been used to predict whether disease is primary versus metastatic or predict the degree of necrosis. 46 Preliminary analysis from our institution evaluated the first-order MRI radiomic features in 60 patients with STS treated with neoadjuvant RT. 50 In this study, patients with high entropy and low surface to volume ratio (SVR), such as heterogeneous spherical tumors, had worse distant control (hazard ratio [HR] 1.66, 95% confidence interval [CI] 1.04-2.66, P = .033) and overall survival (OS; HR 1.64, 95%CI 1.07-2.50, P = .023). Tumors with low entropy and high SVR, more asymmetric and infiltrative in nature, had worse local control (HR 3.40, 95%CI 1.03-11.23, P = .045) but improvements in distant control (HR 0.32, 95%CI 0.12-0.89, P = .029) and OS (HR 0.36, 95%CI 0.15-0.88, P = .025) as we would see in morphologies such as myxofibrosarcoma 50 (Figure 1). This suggests that MRI radiomics predict local and distant control, with the opportunity to adapt treatment to the patient. Other preliminary analyses including Spraker et al demonstrated the utility of T1-weighted pretreatment MRIs in STS to create clinical and radiomic models—they created a clinical/radiomic model incorporating 4 radiomic variable classes (tumor volume, dissimilarity, busyness, and large zone/low gray emphasis) with significant predictive capability for OS and progression-free survival (PFS). 51
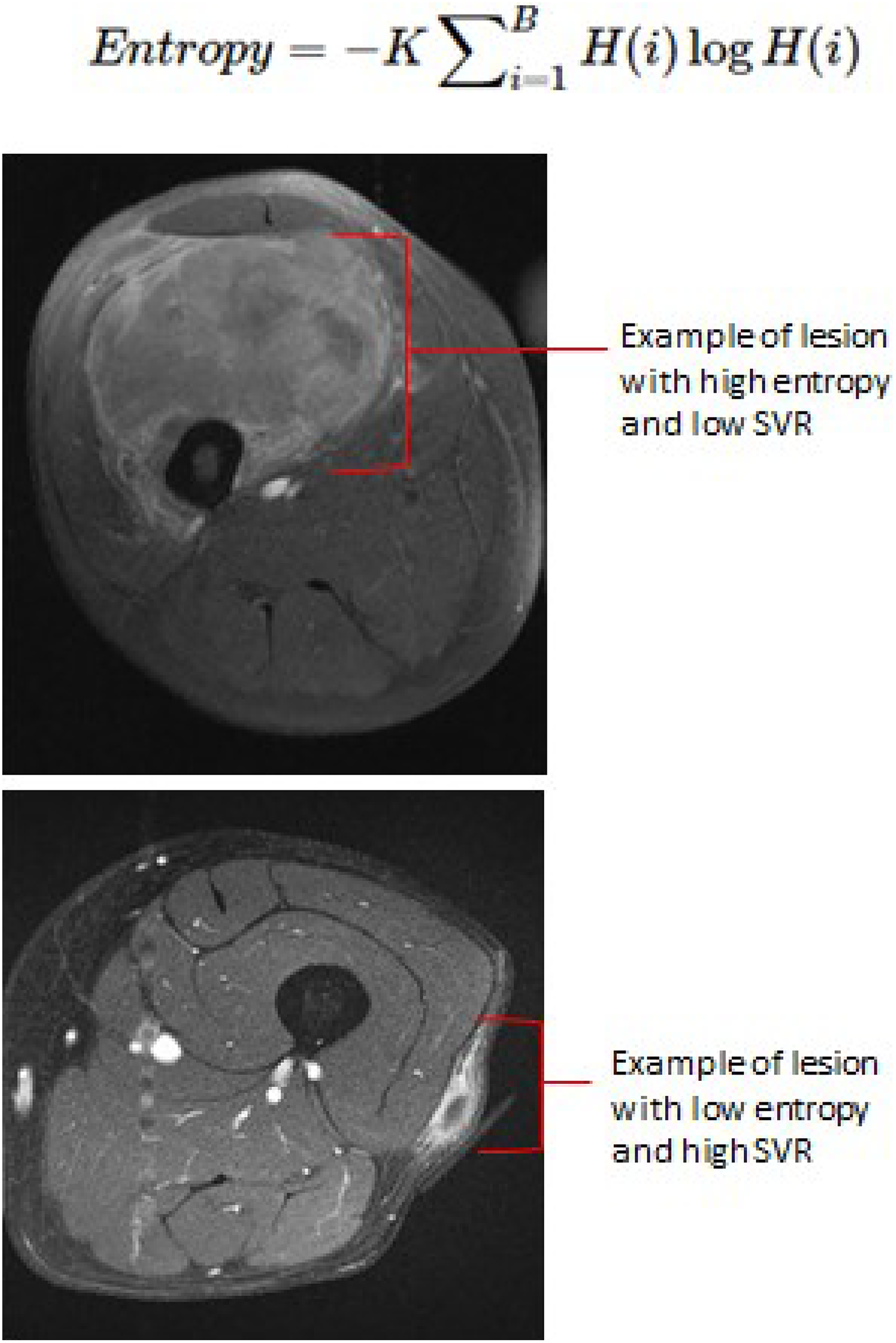
Examples of high-entropy and low- surface to volume ratio (SVR) lesions and low-entropy/high-SVR lesions.
Positron emission tomography Radiomics
The FDG-PET is not commonly used for the treatment of STS but may play a role in delineating STS grade, 52 response to neoadjuvant treatment, 53 and risk of developing distant metastases. 39 Fendler et al found that an SUV peak >2.4 times the mean liver uptake predicted for high-grade STS with a high sensitivity (79%) and specificity (81%). 52 The PET can also be used to assess pathologic treatment response in the setting of neoadjuvant chemotherapy. 53 This additional data, in conjunction with existing radiomics data in the CT and MRI realm, can only improve our resolution in predicting patient outcome. 54 Evaluating textural features in the MRI and PET of a primary STS, or spatial arrangement of pixels of different intensities, can predict for the development of lung metastases with a sensitivity/specificity ranging from 93% to 95%. 39 Although not commonly used for STS staging, PET may offer predictive/prognostic tools that may prove to be beneficial in the management of these patients.
Radiogenomics
The timeline for the field of radiomics and genomics has developed over the past decade, culminating in the incorporation of both into radiogenomics. Radiogenomics is based on the notion that tumor heterogeneity at the molecular and cellular level is intrinsically linked to its radiologic phenotype. The correlation between radiomic features and clinically distinct regions of genomic intratumor heterogeneity has been described in multiple malignancies, such as liver cancer, 55 glioblastoma, 56,57 prostate cancer, 58 and breast cancer. 59,60 Among the first groups to explore this was Segal et al who noted that the level of global gene expression seen in liver cancer was systemically related to imaging features. 55 In glioblastoma multiforme (GBM), Diehn et al described the use of contrast enhancement and mass effect to predict for proliferation and hypoxia gene expression and identified a specific “infiltrative” imaging phenotype that was predictive of patient outcome. 57 Similarly, genomic and radiomic information from The Cancer Genome Atlas and The Cancer Imaging Archive, in conjunction with MRI, were analyzed in invasive breast carcinoma. 60 This study identified genomic features predictive for Estrogen Receptor/Progesterone Receptor (ER/PR) and human epidermal growth factor receptor 2 status, and radiomic features predictive for stage and PR status. An analysis done by Zhu et al revealed that quantitative MRI phenotypes (size, shape, margin, and blood flow kinetics) were associated with corresponding molecular profiles and genetic pathways in breast cancer. 59 Overall, these studies highlight the potential of MRI as a noninvasive surrogate for tumor biology, which may be utilized to predict tumor genetics.
Radiomic Habitats
Radiomics commonly analyze a single imaging sequence for a given cancer, but we know that radiologic phenotypes can be much more complex. Radiomic habitats are created by overlaying various imaging sequences for a tumor to reveal distinct radiographic regions of disease that are not readily evaluable on visual inspection. This represents subpopulations within an image that may correlate with distinct tumor biology. 2,3,46 These radiomic habitats offer a higher resolution with identifying distinct clonal populations (intratumor heterogeneity), predictive/prognostic markers, tumor response, and tumor biology.
Habitat analysis of radiogenomics has been described in GBM and STS. In GBM, various ecologic diversity indices, defined as separate tumor regions of high- and low-blood contrast enhancement and cell density/edema, were utilized to quantify the habitat diversity of tumors, based on T1 postcontrast and T2-fluid-attenuated inversion recovery (FLAIR) with subclassification into high- and low-signal intensity regions corresponding to distinct subregions/habitats. These habitat diversity features predicted for epidermal growth factor receptor (EGFR)-driven GBMs with a high accuracy (79%) and AUC (85%) as well as predicted for OS (74% accuracy). 61 This was done on a larger scale in GBM by Zinn et al with pre- and postcontrast T1-weighted and FLAIR brain MRIs evaluating significant textural differences and radiomic features for TP53, PTEN, and EGFR. This study showed that mutated versus wild-type versions of the genes correlated with distinct radiomic texture features. 62 Similarly designed habitat analyses were performed by Farhidzadeh et al, utilizing T1 pre-/post-contrast and T2 noncontrast-based habitats in 31 patients with STS, demonstrated the proportion of the high T1 postcontrast/low T2 habitat predicted for OS (P = .036) and PFS (P = .05). They were also able to predict tumor necrosis (<90% vs ≥90%; 76% accuracy) and correctly classify whether a tumor was metastatic or nonmetastatic disease with 81% accuracy. 2,3 These findings highlight the possibility that distinct radiologic habitats within a tumor can identify clonal populations, which may aid in predicting tumor behavior/outcome or influence our treatment approach.
Treatment Response
The importance of disease heterogeneity is highlighted in evaluating the response to treatment in sarcoma. Although a homogenous treatment is offered both among patients with sarcoma and within a given tumor, there is vastly different tumor response to neoadjuvant treatment (eg, tumor necrosis), which can correlate to patient outcome. 63 –65 Therefore, identifying radiologic surrogates for evaluating tumor response offers real-time noninvasive measures of treatment response and the opportunity to adapt treatment to optimize patient care.
Tumor response to treatment or pathologic necrosis (≥90%-95%) has been described as a predictor for OS, local recurrence, 63 and distant metastasis. 64,65 Eilber et al evaluated 496 patients with intermediate/high-grade extremity STS treated with neoadjuvant chemoradiotherapy and found that tumors with ≥ 95% necrosis had a 10 year improvement in local control (89% vs 77%, P = .0018) and OS (71% vs 55%, P = .0001) when compared to <95% pathologic necrosis. 63 This is consistent with a similar study done by UC-Davis, but with a smaller cohort (n = 30), the association between pathologic necrosis (≥95%) and 3-year distant recurrence-free survival (100% vs 63%, P = 0.28) was clinically but not statistically significant. 65 MacDermed et al also evaluated the response of locally advanced STS (n = 34) treated with neoadjuvant chemoradiotherapy and found that tumors with a ≥90% response were associated with an improvement in distant metastasis-free survival (85% vs 20%, P = .02) and a trend toward an OS benefit (67% vs 27%, P = .09). 64
The current standard for radiologically evaluating a tumor response to treatment is by the Response Evaluation Criteria In Solid Tumors (RECIST). In STS, there is evidence to suggest that change in tumor size alone (RECIST) does not accurately predict for tumor response to treatment. Integrating the change in tumor attenuation with size (on CT or MRI), referred to as the Choi criteria, 66 better predicts for tumor response to neoadjuvant treatment. 53 When compared to RECIST, the Choi criteria had an improved sensitivity in predicting treatment response, whether it was for good response (residual disease <50%: 88% vs 32%) or very good response (residual disease <10%: 82% vs 41%). 6 Similarly, radiomic habitats utilizing MRI T1 postcontrast and T2 noncontrast have been used to predict for degree of tumor necrosis (≥90% or <90%) with 76% accuracy. 3
Changes in radiomic features, known as delta-radiomics features, are potential prognostic factors that have been previously described in non-small cell lung cancer, 47 colorectal liver metastases, 67 and metastatic renal cell carcinoma 68 in their response to chemotherapy. This concept has been applied in STS, with an initial experience by Tian et al evaluating the response of STS to neoadjuvant bevacizumab with RT. This study utilized mean of positive pixels (MPP) as a texture parameter and tumor blood flow (BF) before and after therapy and correlated it with pathologic response to neoadjuvant treatment. After 2 weeks of therapy, MPP and BF decreased by 10% and 20%, respectively, while tumor size and density were relatively unchanged. This effect was amplified at 8 weeks posttreatment, with MPP and BF (29% and 53%) substantially changed still without a change in size of tumor. Their analysis demonstrated that an MPP change of −35% was the ideal threshold to predict for pathologic response (sensitivity/specificity 85%/71%). 69
Additional MRI sequences that are not commonly obtained in STS, such as ADC, have an association with treatment response in bone sarcoma 70 and may provide additional information in STS moving forward. Although there are radiographic methods of evaluating tumor response, quantifiable measures of response in a clinic meaningful way is still under investigation. This includes correlating commonly used scans in STS (eg, CT, MRI, and FDG-PET) with treatment response as a surrogate predictor of outcome and offers clinically actionable data prior to surgery that may aid in decision-making, such as intensifying or deintensifying treatment.
Personalized Medicine
Personalized medicine is an area that radiation oncology is uniquely poised to lead, with intrinsic principles of personalized care used for all aspects of radiotherapy treatment planning and delivery. Within this framework, radiogenomics represents a novel, noninvasive approach for determining intertumor and intratumor heterogeneity. This utilization of image-driven data that are collected in typical clinical practice and integration with next-generation genomic profiling represents a new frontier in oncology, one that addresses the challenges of disease heterogeneity and offers a personalized medicine solution especially for a rare disease such as STS.
Radiotherapy
A discussion of personalized medicine would be incomplete without mention of the rapid advancement of precision medicine. With the progress in technology, utilization of IMRT helps create conformal RT, with evidence that it significantly improves the local tumor control over conventional 3D-conformal radiation in STS 71 while mitigating normal tissue dose, which has translated to significant improvements in acute and long-term toxicity. 7
The practice of selectively increasing radiation dose to specific regions within a tumor is known as “dose-painting,” most frequently achieved with IMRT or other highly conformal techniques. It has gained traction in the treatment of retroperitoneal STS, which is a particularly challenging clinical scenario, as it frequently presents with bulky disease abutting multiple radiosensitive organs (eg, kidneys, small bowel, stomach, and so on) and has much higher rates of local failure (40%-80%) compared to other STS sites. 72 Surgery is the mainstay for the treatment in retroperitoneal sarcoma and one of the strongest predictors for local control is obtaining a complete resection with clear margins (R0). 73 The addition of preoperative radiation has been associated with higher rates of R0 resection 74 and an improvement in the locoregional control in retrospective series. 75 Therefore, practice has moved toward dose-painting, increasing radiation dose to areas where obtaining clear resection margins is challenging (eg, abutting neurovascular structures, perivertebral, paravertebral, and so on), in hopes of improving tumor response and thereby facilitating an R0 resection. 72,73,76 –79 This rationale for augmenting radiation dose can be expanded to adjust dose based on tumor biology or characteristics (eg, radioresistance, hypoxia, aggressive clonal populations, and so on), such as improving the biologic effective dose (BED) for more radioresistant subclonal populations (low α/β ratio) by hypofractionating those areas, which may help to achieve a pathologic necrosis level (>90%-95%) associated with an outcome benefit.
Brachytherapy or “internal radiotherapy” is another form of precision treatment, especially with the utilization of high-dose rate (HDR) techniques. A key strength of HDR brachytherapy is the ability to adapt the dose based on clinical characteristics, such focally increasing the dose to areas of highest concern of residual disease (eg, close margins) while avoiding excess dose to normal structures (eg, neurovascular structures). 77 Brachytherapy is an effective treatment in STS, with trials highlighting their benefit in improving local control with limb preserving surgery. 80 Current guidelines describe its use in the postoperative and intraoperative setting, using either an interstitial or an intracavitary approach. 74,75,77
The paradigm for recurrent or previously irradiated disease differs significantly from primary treatment and requires a more focal and personalized approach due to intrinsic treatment-resistant properties of recurrent disease and markedly increased likelihood for toxicity. Since brachytherapy delivers radiation from within, the areas receiving the highest radiation dose are the highest risk for microscopic disease (eg, tumor bed), with a rapid dose drop off to the neighboring normal tissue, which is ideal for previously irradiated sarcoma. Sarcomas are generally described as more radioresistant, with an α/β ratio ranging from 2 to 6 (mean ∼4). 81 Local recurrence in sarcoma is primarily within the radiation field, 7 suggesting that clonal populations that persist or recur after radiotherapy are at baseline radioresistant. This difference in α/β ratio compared to other diseases provides an opportunity to hypofractionated RT to increase the BED. Hypofractionated EBRT has been described with success in the preoperative 5,80,82 and postoperative setting. 81 Brachytherapy is also commonly hypofractionated (3-4 Gy twice daily) and allows for an even higher doses near the catheters (eg, tumor bed), delivering upward of >150% of the dose to the microscopic radioresistant cells, facilitating more cell killing. Although the common radiotherapy practice in STS consists primarily of conventional homogenous fractionation, there are advancements that are underutilized (eg, altered fractionation, brachytherapy, dose-painting, and so on) that may provide a personalized approach to treating STS accounting for the tumor biology.
Systemic Therapy
With durable local control in STS, distant control rates can range from 30% to 50%. 83 –86 One of the challenges in treating STS is identifying the patient population at high risk of micrometastatic tumor burden and would most benefit from systemic therapy. Traditional clinical features predictive of distant metastasis include tumor size, tumor depth, disease recurrence, histology, and patient age, 87 –89 but the role of chemotherapy in this population is not clearly defined.
A large meta-analysis of 14 studies noted a 5% OS benefit with the use of chemotherapy in STS but was not able to determine which subpopulation would benefit the most from therapy. 90 Other data in the adjuvant chemotherapy setting have been mixed but usually are underpowered and include heterogeneity of tumors treated and treatments delivered. 91 –93 More recently, EORTC-62931 was a randomized phase III study that evaluated patients with resected grade II to III tumors to either observation or postoperative chemotherapy (ifosfamide, doxorubicin, and lenograstim) and noted no difference in OS at 5 years. 94 At 8 years of follow-up, this study suggested that for patients with the lowest OS, addition of chemotherapy was associated with a disease-free survival benefit (HR 0.46, 95% CI 0.24-0.94, P < .05), which was not detected in patients with high or intermediate OS. 95 Other systemic agents, such as tyrosine kinase inhibitors and small molecule drugs, have been used in the metastatic and recurrent settings, 96 but the role of these therapies as part in the treatment of definitive STS is not established.
In addition to clinical features, incorporation of genomic and radiomic biomarkers will become essential to identifying patients at risk of micrometastatic disease that would most benefit from systemic therapy and will become a critical component in personalizing therapy in STS.
Immune-Modulated Therapy
The interplay between tumor immunogenicity, tumor microenvironment, and current therapeutic strategies has led to several breakthroughs involving immune-modulated treatment strategies. There is some exploration of the role of immunotherapy and STS, with proposed clinical trials utilizing cancer vaccines and immune checkpoint blockades. 33,34,97,98 The current landscape for immunotherapy agents has built upon progress in other solid tumors such as melanoma and nonsmall cell lung cancer. 99 –101 Improved clinical response to ipilimumab in metastatic melanoma has been associated with increased mutational load, neoantigen load, and cytolytic markers. 101 This is thought to be due to the increased mutational burden of these tumor cells leading to increased immune surveillance and response.
With significant heterogeneity in sarcoma, immunotherapy trials are likely to show mixed results, and refining our selection for ideal immunotherapy candidates is required. An example is SARC028, a phase II trial evaluating the role of pembrolizumab (anti-PD-1 antibody) in metastatic or surgically unresectable locally advanced sarcoma previously treated with chemotherapy, which did not meet their primary end point of overall response. 102 In STS, they found an overall response rate of 18% (7 of 40), but histologies with higher mutational burden and T-cell fractions such as undifferentiated pleomorphic sarcoma had a higher response rate of (40%; 4 of 10). 102 In addition to checkpoint inhibitors, other methods of immunomodulators being tested for the treatment of sarcoma include activating tumor-associated macrophages 103 (eg, leiomyosarcoma, 104 myxoid liposarcoma, 105 and Ewing 106 ), chimeric antigen receptor T cells (eg, Ewing and osteosarcoma), 10,107 dendritic cell infusions with EBRT, 108,109 and viral vectors (eg, synovial sarcoma and liposarcoma 79 )
Finally, the role of radiotherapy as an immune modulator is documented in the rare but clinically remarkable abscopal effect, where local treatment of a primary tumor results in long-term control of distant metastatic disease through an immune-mediated response. 110 Efforts to exploit this immune-modulated effect have noted that larger doses of radiation appear to induce greater immune activation in a preclinical setting. 34,110,111,112 In STS, prior studies combining radiation and immunomodulators had suboptimal outcomes, but these studies commonly employed conventional EBRT fractionation (2.0 Gy per fraction) 108,109 which in vitro studies suggest are less than ideal outcomes, since this fractionation is less effective at inducing immunogenic cell death and may hinder the immunogenic response by sterilizing infiltrating lymphocytes. 112 In the long-term follow-up of by Finklestein et al phase I study evaluating the use of dendritic cell vaccines and neoadjuvant radiation (50 Gy in 25 daily fractions) for large (>5 cm) high-grade resectable STS, they found that 61% (11/18) were alive without systemic recurrence. Although this suggests a role for immunomodulation and radiation in STS, consideration for altered radiation fractionation or the addition of other immunogenics may further optimize patient outcomes.
The potential combination of RT as an immune-modulating agent and current checkpoint inhibitors has manifested itself in several currently enrolling clinical trials. The NEXIS trial is an investigation of neoadjuvant durvalumab (a PD-1/PDL-1 and CD80 inhibitor) and tremelimumab (CTLA-4 monoclonal antibody) with conventionally fractionated (50 Gy/1.8-2.0 Gy per fraction) or high-dose (15 Gy/1 fraction) radiotherapy followed by surgical resection (NCT03116529). Similarly designed is NCT03463408, a 2-cohort, open-label nonrandomized study of neoadjuvant nivolumab and ipilimumab with concurrent radiation followed by surgical resection (additional trials in Table 1). Further novel combinations of modern immunotherapy agents such as the checkpoint inhibitors and previously mentioned therapies as well as a more refined focus on radiotherapy as an immunomodulator are necessary to increase the efficacy of these treatment combinations. In addition, using genomics, radiomics, and radiogenomics to properly identify candidates with sarcoma who would most benefit from immunomodulatory therapy would allow us to personalize care for the patient, leading to improvements in their outcome.
Selected Clinical Trials for STS Using RT.
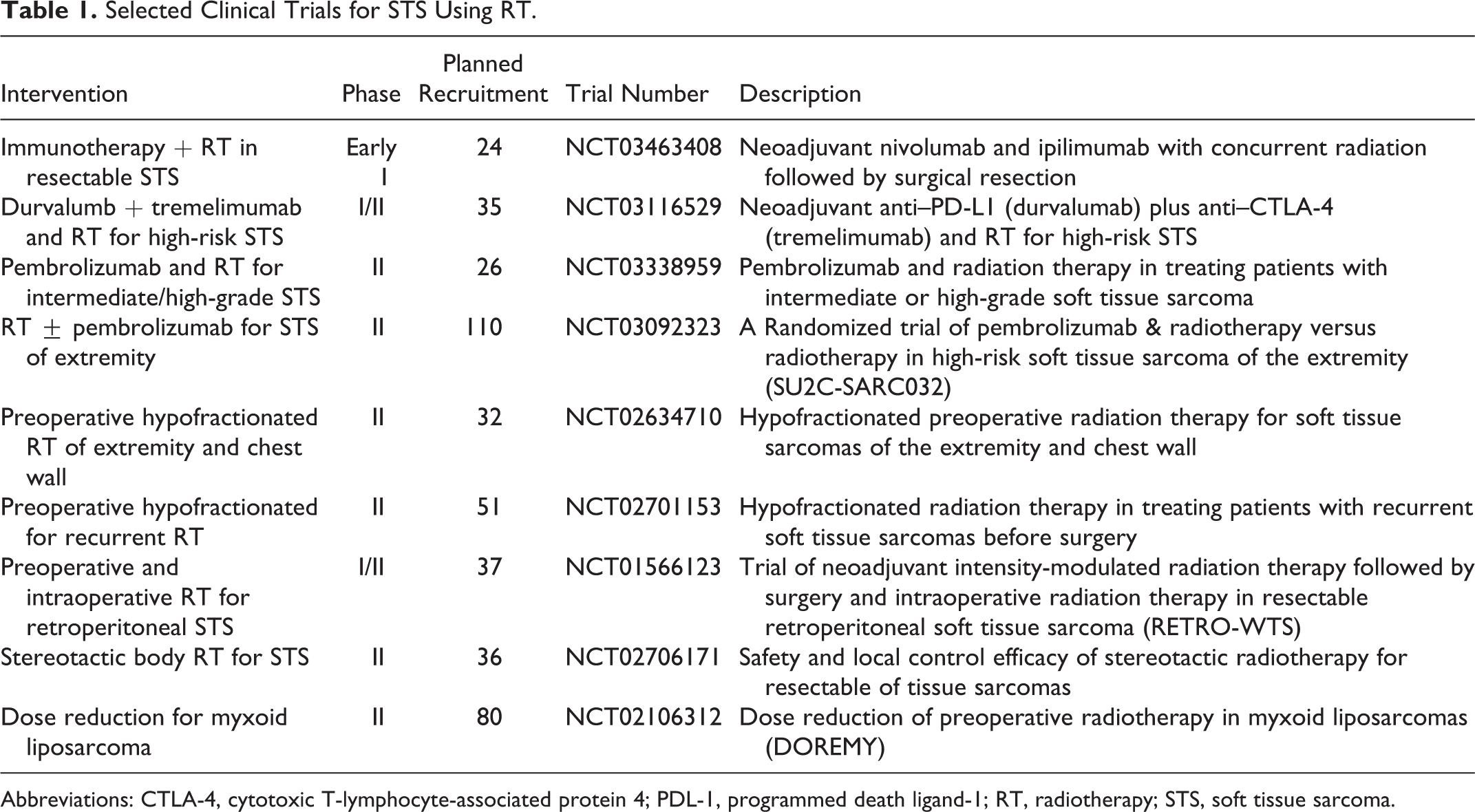
Abbreviations: CTLA-4, cytotoxic T-lymphocyte-associated protein 4; PDL-1, programmed death ligand-1; RT, radiotherapy; STS, soft tissue sarcoma.
Future Directions
Our institution is at the forefront of personalized medicine with a proposed radiogenomic framework to enact change. Given the current landscape toward personalized medicine and the tools available to the treating physician, there is a missing link between the preclinical data, radiogenomic data gleaned from noninvasive studies, and overall patient outcomes. We have therefore proposed a study framework to integrate all of these features with the goal of optimizing outcome in STS (schema in Figure 2).
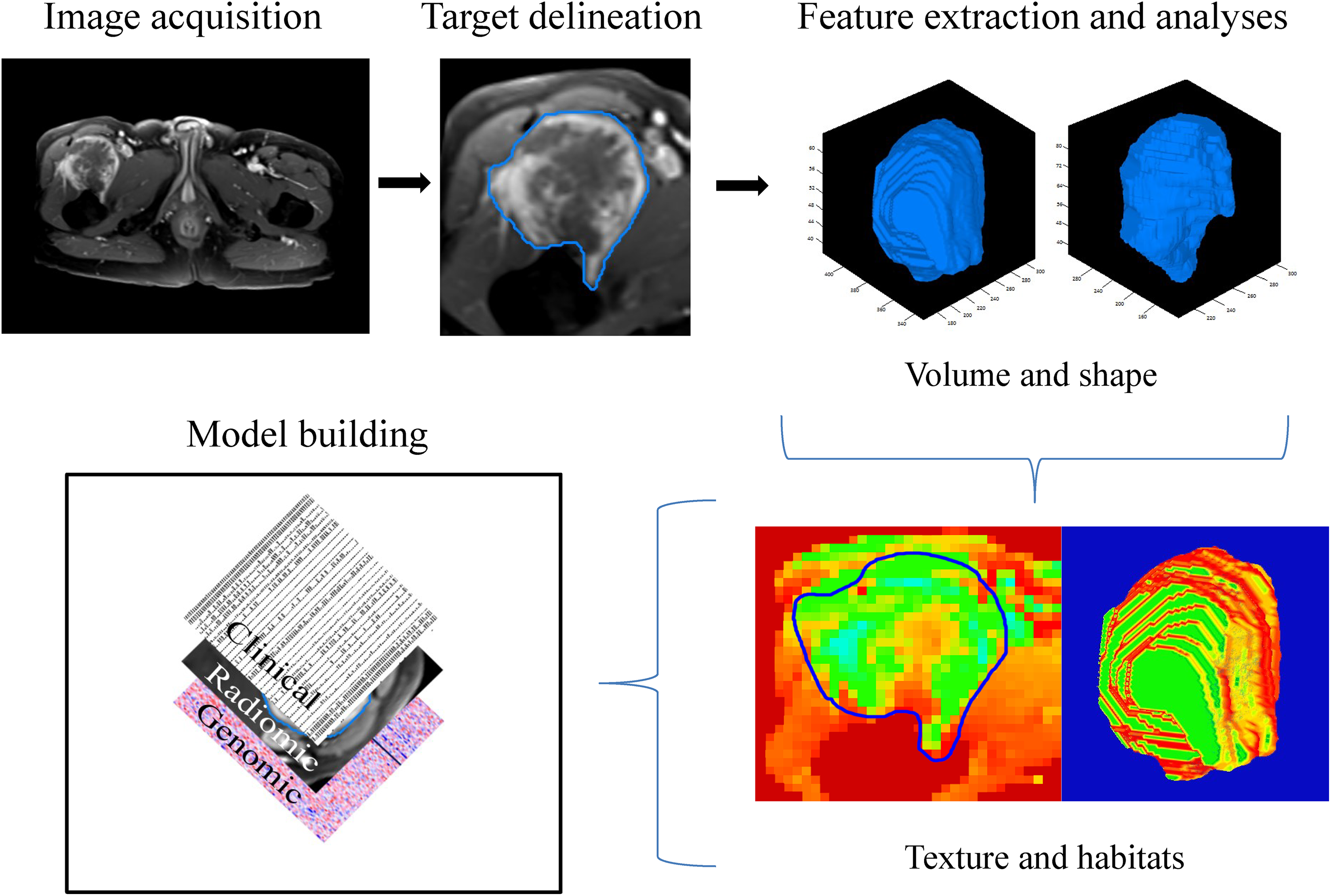
Proposed trial design and schematic for radiomic incorporation of data.
With the current understanding of genomically predicted radiosensitivity (RSI/GARD) and immunity (12-CK), futures studies are being employed to validate the clinical utility of these assays in regard to tumor response and patient outcome. This treatment approach, mirroring the work performed by Torres-Roca et al, 20 will guide us on decision-making in the treatment of STS. The next step is to identify the radiomic correlates for these genomically validated studies, offering a noninvasive approach of identifying genomic intra-/intertumor heterogeneity. The radiation dose delivered will then be adjusted based on tumor biology and utilize dose painting approaches to offer the best effective dose required to elicit a response in the entire tumor and radioresistant regions within the tumor. Immunomodulators will be added for patients who would likely benefit from it based on their radiogenomic findings. The goal is to achieve very good tumor response prior to surgery (>90%-95% necrosis), which we will be able to monitor during the course of treatment with radiomic analysis of our weekly images, allowing an actionable real-time update of the tumor status and response during treatment. Personalizing the care based on the patient will allow us to safely escalate or de-escalate treatment with precision and to offer the optimal patient outcome with mitigated toxicity.
Conclusions
The future of radiation therapy for STS is one that should take full advantage of a new era of precision medicine tools. The one-size-fits-all treatment approach yields suboptimal results in a diverse disease like STS, and current methods of stratifying STS (eg, grade, size, histology, and so on) limits large clinical trial accrual. Therefore, STS is the ideal disease to develop and employ genomic and radiomic tools to guide us in decision-making. The future of radiation oncology in STS will utilize precision medicine and personalized medicine, deliver treatment based on the tumor biology, adapt our treatment based on tumor response, and provide patients with the most ideal outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.