
Abstract
Background
We retrospectively aimed to assess the prognostic significance of somatostatin receptor (SSTR) standardized uptake value (SUVmaxsstr), SSTR representative tumor volume (RTVsstr) and total lesion SSTR expression (TLsstr) obtained by [68Ga]Ga-edotreotide PET/CT ([68Ga]Ga-SSTR PET/CT) in patients with primary gastroenteropancreatic neuroendocrine tumors (GEP-NET) before surgery.
Material and Methods
We analyzed patients who underwent [68Ga]Ga-SSTR PET/CT 3-6 weeks before surgery from February 2020 to April 2022. The mean SUVmaxsstr value, the RTVsstr (cm3; 42% threshold) and the TLsstr (g) were registered. Thereafter the patients were followed up 10.3 months (range 3-27). The PET/CT results were compared to the event free survival (EFS).
Results
Forty-two patients (61 ± 13 years) have been enrolled. At multivariate analysis only RTVsstr values were predictive. The Kaplan-Meier survival analysis for RTVsstr showed a significant better EFS in patients presenting lower values as compared to those having greater (P = .003, log-rank test). SUVmaxsstr was not suitable for predicting EFS, TLsstr mildly.
Conclusion
RTVsstr represents a valuable volumetric parameter able to predict the outcome in GEP-NET patients who underwent surgery. The magnitude of the SSTR representative tumor burden holds a predominant value for determining the response to therapy in GEP-NET patients before surgery, rather than the maximal SSTR representation at single voxel.
Keywords
Introduction
Neuroendocrine tumors (NETs) represent a group of highly heterogeneous neoplasms that can occur in different organs with an estimated incidence of less than 1/100.000 cases. They generally present an indolent growth rate.1,2 Gastroenteropancreatic (GEP) NETs constitute the second most common digestive cancer showing low tendency to metastasize but once they diffuse can rapidly progress. Contrarily, those of the small intestine exhibit high malignant potential even if they have a slow grown pattern when in metastatic setting. 3 GEP NETs are classified as grade 1 or 2 when well- or moderately differentiated, respectively, with only few cases grade 3, poorly differentiated aggressive, neuroendocrine carcinoma (NEC).4,5 The survival and outcome of NET patients with similar stage and grade varies considerably in reason of a significant plethora of prognostic factors, mostly unreliable. Overall, these patients show mainly disease steadiness rather than progression during their long-term follow-up.6,7 Several studies have demonstrated that morphological imaging and conventional parameters are useful for assessing both location and extent of NETs as well as for monitoring therapy response, while their role for survival and outcome prediction is still limited.8,9 Functional imaging, based on tumor somatostatin receptors (SSTRs) overexpression, constitutes an ideal target for diagnosis and therapy with radiolabeled somatostatin analogues. Over the past decade, [68Ga]Ga-SSTR (such as [68Ga]Ga-DOTA-TOC/NOC/TATE/EDOTREOTIDE) positron emission tomography-computed tomography (PET/CT) has taken gradually the place of conventional SSTR scintigraphy for assessing NETs due to its superior sensitivity and accuracy.10,11 Although [68Ga]Ga-SSTR PET/CT is widely employed in this setting, only limited data are currently available concerning the new PET/CT quantitative parameters for the prediction of disease outcome and survival in patients diagnosed with NETs. High maximum standardized uptake (SUVmax) values have been demonstrated to match with a lower grade tumor and a better event-free survival (EFS) whereas it predicts an elevated risk of disease progression when low.12,13 Recently, PET/CT volumetric parameters based on SSTR distribution, such as SSTR representative tumor volume (RTVsstr) and total lesion SSTR expression (TLsstr) have been implemented for a wide tumor assessment. 14 The aim of this retrospective study is to investigate, at staging, the correlation between the PET/CT functional parameters SSTR-based (SUVmaxsstr, RTVsstr, and TLsstr) and the EFS in patients complying with primary GEP NETs who shortly will undertake surgery.
Materials and Methods
Patients
We retrospectively reviewed data of two hundred 6 patients with positive biopsy for gastro-entero-pancreatic-neuroendocrine tumor (GEP-NET). Patients were addressed for a baseline [68Ga]Ga-edotreotide PET/CT scan from February 2020 to April 2022. The enrolled patients satisfied the inclusion criteria, such as: age at entry above 18 years, primary GEP-NET with G1 or G2 grading and only locoregional disease, scan performed before surgery. Exclusion criteria were: Patients who previously underwent surgery for GEP-NET, patients with metastatic disease, if any, patient who formerly received radioligand therapy, chemotherapy or somatostatin analogues. Patients with grade 3 NEC, multiple endocrine neoplasia as well as patients with less than 6 months follow-up period after PET/CT (apart from the ones with early tumor progression), constituted additional exclusion criteria. A flowchart of patient selection is shown in Figure 1. Diagnoses were confirmed according to the WHO 5th ed. (2019) classification. Flowchart of patient selection. Not enrolled: metastatic, previous surgery, radioligand therapy, chemotherapy, somatostatin analogues. Excluded: PET negative, insufficient follow-up, Multi Endocrine Neoplasia.
Patients had undergone comprehensive baseline standard assessment including clinical and laboratory data, chest, abdomen, and pelvis CT or MRI. Data as tumor grading, histological specimen, Ki67 values, WHO classification and type of surgery were collected from patients' medical record. Distribution and proliferation rate of cells were determined from Ki-67-stained sections of tissue specimens.
Basilicata Independent Ethics Committee (CEUR) and IRCCS CROB review board gave approval for the study (approval number: #2022-001470; date: February 15, 2022). All patients undergoing PET/CT signed an informed consent form in accordance with the Declaration of Helsinki. The reporting of this study conforms to REMARK guidelines. 15
Imaging Technique
All patients underwent [68Ga]Ga-edotreotide PET/CT. The patients received [68Ga]Ga-edotreotide intravenously (median:181; range:148-259 MBq; weight-based). Sixty minutes after the tracer injection, PET and modulated low dose CT were carried out with a PET/CT scanner (GE Discovery VCT scanner; Waukesha, WI) that combined a PET scanner and a Light Speed VCT sixty-four row MDCT system. MDCT (pitchx 1.5; 120 mAs; 120 kVp) was performed without contrast medium. The PET scanning was subsequently performed, acquiring 3 minutes per bed position and 6 to eight beds per patient depending on patient height encompassing the whole skeleton. The raw CT data were reconstructed into transverse images with a 3.75-mm section thickness. Sagittal and coronal CT images was generated by reconstruction of the transverse data. Raw PET data were reconstructed with and without attenuation correction into transverse, sagittal, and coronal images. Attenuation correction was based on CT attenuation coefficients, which were determined by iterative reconstruction.
Imaging Evaluation
All images were reviewed by using PET/CT fusion software (Volumetrix for PET-CT and AW volume share 4.5, GE Healhcare, Waukesha, WI, USA). Each PET/CT study was interpreted, in consensus, by three experienced nuclear medicine physicians with 15 years of expertise, one of them was a radiologist. The examiners first evaluated only the CT images. Lesion sizes were visually estimated and measured at least in two maximum diameters by using a vendor-provided software (Volumetrix for PET-CT; GE Healthcare, Waukesha, WI, USA). Any lesion ≥1.0 cm in maximal transverse or maximal sagittal dimensions, with soft tissue/abdominal window settings, was considered target. The CT volume computation was diameter-based according to the formula: V = d craniocaudal × d antero-posterior × d lateral × π/6) being the lesions assumed as ellipsoid.
The PET studies were evaluated both visually and semi-quantitatively. Afterward, the maximum standardized uptake values and body weight corrected (SUVmaxsstr) as well as the SSTR expression representative tumor volume (RTVsstr; cm3; 42% threshold) and total lesion SSTR expression (TLsstr; g) were determined by using the same vendor-provided software. The RTVsstr was defined as the volume that SUV is more than 42% of SUVmaxsstr. TLsstr was derived from the multiplication of RTVsstr and SUVmean in RTVsstr, as the product of SUVavg multiplied by the number of voxels
Briefly, focal, or diffuse [68Ga]Ga-edotreotide uptake in a location mismatched with normal anatomy or physiology was interpreted as abnormal and ultimately was considered to be indicative of GEP-NET lesion. A composite score based on RTVsstr and SUVmaxsstr aggregation was used to further stratify the patients.
Follow-up Assessment
Patients were categorized into two groups according to the cut-off points, determined by receiver-operator-curve (ROC) analysis, for SUVmaxsstr, RTVsstr and TLsstr. The status of disease was followed up 10.3 months thereafter (range 3-27). The evaluation was carried out considering clinical and hematological parameters during scheduled or unscheduled visits, on the basis of diagnostic imaging (i.e. CT, MRI) findings, as well as by phone interview.
Failure to respond without progression (e.g. residual/stable disease and/or indication for therapy changes), progression and/or disease-related death constitute main events. They were considered surrogate endpoints. Clinical parameters and PET/CT findings were correlated to the disease outcome (event free survival; EFS). EFS was defined as the time from PET/CT until end point occurrence or the time of last censor.
Progression was recognized as evidence of a new lesion or relapse of a previous existing lesion; when there was missing information, the date of unscheduled new somatostatin analogues treatment was considered.
Statistical Analysis
Continuous data are expressed as percentage, means ± SD, and median as appropriate. Correlation analysis was used to assess the relationship between variables, when requested. Optimal cut-off of SUVmaxsstr, RTVsstr and TLsstr for differentiating patients at high risk of main events were derived from ROC analysis. The ROC analysis was additionally performed for any other parameter, if requested. Event-free survival curves were constructed using the Kaplan-Meier method to account for censored survival times and were compared with the log-rank test. A P value<.05 was considered statistically significant. Survival analysis was performed by multivariate Cox proportional hazard regression analysis. The proportional hazard assumption of the Cox model was checked separately for each covariate by a graphical method before performing the regression analysis. Our hypotheses were tested using Bonferroni adjusted alpha levels. The Ki-67 values and age at diagnosis, intended as ordinal variable, were included in the final model.
Results
Patient Characteristics
Individual Data of GEP-NET Patients.

GEP-NET, Gastroenteropancreatic-Neuroendocrine Tumor; Ki-67, protein.
Imaging Evaluation
The median SUVmaxsstr value was 8.55 (range 2.4-37.6), median RTVsstr was 4.94 cm3 (range 1.15-49.2) and median TLsstr was 306.9 g (range 74.0-1928). The ROC curve analysis recognizing cut off values of SUVmaxsstr, RTVsstr and TLsstr for EFS are showed in Figure 2. The area-under-curve (AUC) for SUVmaxsstr was .585 (95% CI 0.42-.73) and the established cut off value was ≤16.3. The AUC for RTVsstr and TLsstr was .673 (95% CI 0.51-.81) and .590 (95% CI 0.42-.73), respectively whereas RTVsstr and TLsstr cut off values were >2.47 (cm3) and >219.3 (g), respectively. ROC curve analysis establishing the cut off value of RTVsstr, TLsstr and SUVmaxsstr for predicting Event Free Survival. The cut off value of RTVsstr (A), TLsstr (B) and SUVmaxsstr (C) for stratifying patients was >2.47 (cm3), >219.3 (g) and ≤16.3, respectively. SUVmaxsstr, standardized uptake value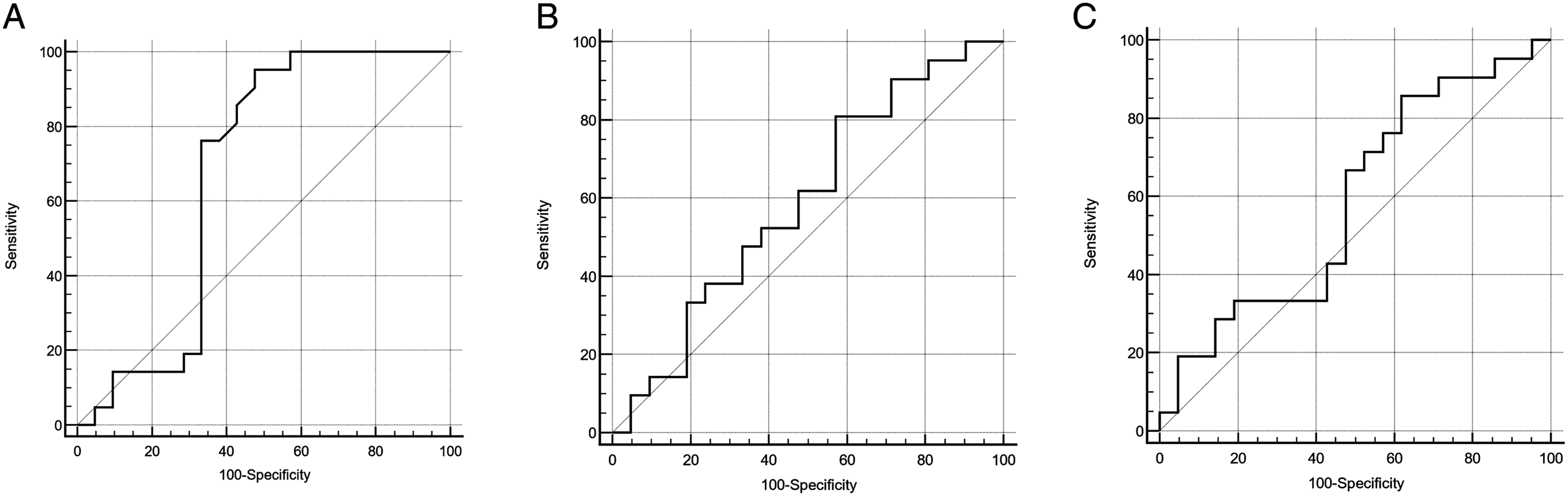
Clinical Endpoints, Follow-up, and Correlations
Twenty-one of forty-two patients (50%) reached the endpoint, 5 showed progression, 11 were unresponsive to the therapies, 5 died. Twelve patients had RTVsstr < 2.47 (cm3), 11 showed no evidence of disease, 1 died. The median follow up was 10.3 months (range 3-27 months).
Univariate Cox Proportional Hazard Regression Analysis.

aDichotomized variables on ROC analysis basis.
bOrdinal variable.
HR, hazard ratio; CI, confidence interval; SSTR, somatostatin receptor; RTVsstr, sstr expression representative tumor volume; TLsstr, total lesion sstr expression; SUVmaxsstr, sstr maximum standardized uptake value.

Kaplan-Meier survival graphs indicate a significant difference in EFS between the group of patients categorized by RTVsstr. (A), Kaplan-Meier graph of RTVsstr and EFS showing RTVsstr above (dotted line) and below (solid line) the cut off of >2.47 (cm3). Low RTVsstr is coupled with prolonged Event Free Survival (P = .003, log-rank test). (B), Kaplan-Meier graph of TLsstr and EFS with TLsstr above (dotted line) and below (solid line) the cut off of >219.3 (g); P = .04. (C), Kaplan-Meier graph of SUVmaxsstr and EFS with SUVmaxsstr above (dotted line) and below (solid line) the cut off of ≤16.3; P = ns.

Survival by combination of RTVsstr and SUVmaxsstr values. Kaplan-Meier graph of both RTVsstr and SUVmaxsstr and Event Free Survival. RTVsstr + and RTVsstr - indicate values of RTVsstr above and below the cut off of >2.47 (cm3), respectively. SUVmaxsstr + and SUVmaxsstr - indicate values of SUVmaxsstr above and below the cut-off, respectively; (P = .01 across categories, log-rank test).
Discussion
Present treatment approaches are valuable in GEP-NET while the implementation of more precise and timely therapy, tailored to the specific risk stratification, may represent a further clinical progress. Although, these tumors have a slow growth and a relatively favorable prognosis,12-14,16 they can have various clinical features and outcomes. This scenario urges for valid prognostic factors generally missing in the neuroendocrine tumors management. Here, we found that the RTVsstr, a new PET/CT volumetric parameter, may help for stratifying patients with primary GEP-NET undergoing surgery. Increased RTVsstr discriminates subjects with worse prognosis compared to those who did not. RTVsstr had a better prognostic significance than SUVmaxsstr in this setting. Although already described in metastatic and all grades of pancreatic NET,14,17-22 the finding is novel since linked to patients with primary GEP-NET complying with loco-regional disease, whose curative intent surgery was shortly performed. Generally, considering the relative quiescence of GEP-NET, it seems appropriate to measure the prognostic potential of different indicators by progression- or event free survival (PFS; EFS) rather than overall survival as partially reported below. Some authors indicated that RTVsstr have prognostic value of progression free survival in well differentiated NET patients.
14
That study enrolled ninety-two surgical or medical patients whose summed values of RTVsstr, calculated in metastatic subjects, were demonstrated to perform better than SUVmaxsstr. Pauwels et al
18
analyzed pretherapeutic [68 Ga]Ga-SSTR PET tumor uptake and the volumetric parameters in patients undergoing 90Y-DOTATOC peptide receptor radionuclide therapy (PRRT). They found that high [68Ga]Ga-DOTATOC-avid tumor volume predicts better outcome in NET patients treated with [90Y]Y-DOTATOC. Similar findings were reported by other authors
22
in patients treated with [177Lu]Lu-DOTATATE but, the value of volumetric parameters in predicting outcome was only partially confirmed. Both the latest studies were performed in patients necessitating PRRT hence, a priori, metastatic. Ohlendorf et al
19
also focused their analysis on RTVsstr as predictive factor in advanced-stage GEP-NET showing that this parameter constitutes a valuable imaging biomarker of tumor burden. Some other authors
21
demonstrated the prognostic value of the volumetric indices in patients with locally advanced, unresectable NETs, in terms of both PFS and disease-specific mortality. Ohnona et al
20
indicated the total functional tumor volume measured by [68Ga]Ga-SSTR PET as a relevant prognostic biomarker in patients with all stages of well-differentiated pancreatic NETs. At present, there are still few trials on operable GEP-NET cases at staging time. The same as for volumetric parameters, only few studies focused on SUVmax as a predictive parameter in GEP-NET.13,23 Low SUVmax on [68Ga]Ga-SSTR PET was associated with worse prognosis in well-differentiated GEP-NET predicting early failure on SSA monotherapy. In addition, [68Ga]Ga-SSTR PET/CT, via SUVmax, impacted on the management of NET patients, leading to a change in treatment decision in about one-third of patients.
24
Ambrosini et al
12
also reported that high [68Ga]Ga-DOTANOC SUVmax correlates with better outcome in stages III or IV pancreatic NETs. In our study a volumetric parameter, the RTVsstr, predicts event free survival being it prognostic of worst outcome when higher, and it appears to work better than SUVmaxsstr in operable GEP-NET. Moreover, on a patient basis, lower RTVsstr values seem to be protective also when coupled with SUVmaxsstr for prognostic, as patients with low RTVsstr tend to exhibit a longer EFS irrespective of SUVmaxsstr (Figure 5). [68Ga]Ga-edotreotide PET/CT in patient with pancreatic GEP-NET. Left anterior oblique surface rendering image of the lesion (arrow) (A), axial PET image with lesion volume computation (box and master region of interest) (B), axial CT image (C), axial PET/CT fused image (D).
The SUVmax represents a validated measurement confined to the detection of the hyper-metabolic activity of the tumor at single site (the site most representative of SSTR concentration), which does not consider the whole representative tumor volume. On the other hand, SSTR expression representative tumor volume (RTVsstr) estimates the tumor SSTR representation through the volume of the entire lesion above a minimum threshold designed to exclude background activity.
It is well known that survival time differs among patients with NETs, even those with the same site, stage, and grade of primary tumor. This finding can be partially due to tumor heterogeneity which may translate tracer’s uptake heterogeneity between lesions of the same histologic subtype. At present, a variety of imaging-derived parameters have been reported to predict prognosis or treatment outcome, even if none have been translated into routine clinical practice so far. Recently, Paiella et al 25 reported that the combined use of [68Ga]Ga-SSTR and [18F]F-FDG PET/CT may be valuable in the diagnostic workup of pancreatic NETs, especially in G2 setting, with an aggregate sensitivity of 99.2%. The PET/CT methodology may help to overcome quantitative and heterogeneousness concerns, since the whole tumor burden can be comprehensively assessed both in solid tumors and hematological malignancies.26-28 In our study patients presenting higher values of RTVsstr showed a shorter event free survival as compared to those having lower, indicating that the lower the magnitude of tumor volume is -representing SSTR expression- the better the response to subsequent therapy. The SUVmax, and the individual features were not predictive, yet we tested the association of SUVmax with RTVsstr trying to couple their potentialities in the abovementioned heterogeneous environment of GEP-NET. Noteworthy, patients with higher RTVsstr worsened irrespective of SUVmaxsstr. Overall, lower RTVsstr values showed tendency to be protective regardless of SUVmaxsstr. It is conceivable that patients with primary tumor and locoregional disease presenting low values of global RTVsstr would respond better since the magnitude of the SSTR representative burden, rather than the maximal SSTR representation at single voxel, appears to be the key determinant. Tumor heterogeneity cannot be comprehensively depicted by a single “hypermetabolic” voxel. Accordingly, SUVmax did not influence the outcome of our patients. Concerning the TLsstr, we noted a prediction tendency like RTVsstr, even barely significant. It was probably due to the preponderant use of non-predictive SUVmax in TLsstr computation.
From a patho-physiological point of view, these findings are not surprising since RTVsstr may better represent the real tumor volume in this setting and, the well-known heterogeneous texture of GEP-NET whereas SUVmax conveys an index of cell SSTR expression within a well-defined and circumscribed volume. In fact, RTVsstr reflects better than SUVmax the aggregated GEP-NET pathological features such as the degree of cellularity of lesions, the number of neoplastic cells, the degree of SSTR expression and the various histological architecture that may include trabeculae, nests, glandular formation, gyriform, and pseudorosettes.29-31 Indeed, in this set-up the endoscopic ultrasound holds a prognostic value for stratifying NET patients with solid pancreatic lesions, detecting malignancy-related features as well as identifying the tumor grading reliably.32,33
The abovementioned characteristics of NETs can lead to pitfalls when considering only the SUVmax.34-36 In this environment the comprehensive volumetric indices, such as RTVsstr, are expected to work better. The prognostic impact of [68Ga]Ga-SSTR PET/CT volumetric parameters in GEP-NET patients undergoing surgery remains to be completely established. In view of that, our results demonstrate that RTVsstr was predictive for event free survival in this setting endorsing the use of [68Ga]Ga-SSRT PET/CT in daily clinical practice and for tailoring subsequent therapy.
This study included GEP-NET patients that strictly fulfilled inclusion criteria, enrolled at staging, before curative intent surgery. It was performed on a single center basis which gives reason for the small samples size. Additionally, the impact on EFS of subsequent medical therapies, if any, has not been figured.
Conclusion
The quantitative assessment by RTVsstr rather than SUVmax on [68Ga]Ga-SSTR PET/CT may be helpful to manage patients with GEP-NET before surgery. In this setting, the response to therapy seems to depend upon the tumor burden extent rather than the magnitude of SSTR expression.
Footnotes
Appendix
Acknowledgments
The Authors wish to thank Mrs Piccolella A. and Mr Volpicelli F. for their valuable contribute to performing the studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; they have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Data Availability Statement
Data that generated the manuscript are guarded in digital form by the corresponding author and are available upon request, if any.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Basilicata Ethics Committee and IRCCS CROB institutional review board gave approval for the study (approval number: #2022-001470). All patients undergoing PET/CT signed an informed consent form in accordance with the Declaration of Helsinki.