
Abstract
Background
The aim was to evaluate the causes of death for patients with localized, regional and metastatic penile cancer (PeCa) after diagnosis.
Methods
PeCa patients diagnosed during 2004-2018 in the Surveillance, Epidemiology, and End Results program database were identified. Causes of deaths including PeCa, second malignant tumors (SMTs) and non-tumor diseases were analyzed, as well as the standardized mortality ratio (SMR) of each cause.
Results
For localized PeCa, 800 of 2155 patients died during the follow-up. 24.9% of all deaths were due to PeCa. 18.0% and 57.1% deaths were due to SMTs and non-tumor causes. Main SMTs included cancers of lung and bronchus (n = 40) and skin (n = 11) with significantly increased SMRs of 1.71 (1.22-2.33) and 4.82 (2.41-8.63). Mortality risks of other SMTs were mostly similar with the general populations. Main causes of non-tumor diseases included diseases of heart [n = 172, SMR: 1.66 (1.42-1.93)], COPD and allied cond [n = 38, SMR: 1.63 (1.15-2.24)], and cerebrovascular diseases [n = 33, SMR: 1.71 (1.17-2.4)]. For regional PeCa, 679 of 1310 patients died including 43.5% PeCa, 14.8% SMTs and 26.6% non-tumor causes. The mortality risks of cancers from lung and bronchus [SMR: 2.41 (1.53-3.62)], skin [SMR: 6.41 (2.35-13.95)] and testis [SMR: 149.35 (18.09-539.5)] were significantly increased. Main non-tumor causes of death included diseases of heart [n = 71, SMR: 1.77 (1.38-2.23)], COPD and allied cond [n = 17, SMR: 1.85 (1.08-2.95)] and diabetes mellitus [n = 16, SMR: 3.62 (2.07-5.88)]. For distant diseases, 109 of 132 patients died including 76 (69.7%) died for PeCa itself, 24 (22.0%) died for SMTs and 9 (8.3%) died for non-tumor diseases. The majority of PeCa deaths (67.1%) and SMTs deaths (79.2%) occurred within 1 year after the diagnosis of PeCa.
Conclusions
We firstly analyzed the SMTs and non-tumor causes of death and morality risks of each cause for PeCa patients, which provided valuable information for PeCa patients on disease prevention and health care during their survivorship.
Keywords
Introduction
Penile cancer (PeCa) is a rare malignancy worldwide, accounting for less than 1% of all malignancies in men. 1 The overall incidence rate is approximately .69 cases per 100 000 persons in the US. 2 It was estimated that the number of new PeCa patients was 34 475 and deaths cases was 15 138 each year worldwide. 3 The survival rates still vary greatly with the stages of patients’ disease. It was reported that about 40% of new cases were diagnosed with localized PeCa, with a 5-year overall survival rate of approximately 90%. 4 The survival rates decrease dramatically once patients are in the regional or distant metastasis stage. The 5-year overall survival rate is approximately 80% with unilateral inguinal lymph node involvement, 10%-20% with bilateral or pelvic lymph node involvement, and <10% with extranodal extension. 4
Since the 1990s, substantial progress has been made in the prevention, diagnosis and treatment of PeCa. The prognosis has been greatly improved in PeCa patients, especially those who have not progressed to the metastatic stage. With the prolonged survival time, the proportion of other causes of death such as second malignant tumors (SMTs) and non-tumor diseases has been increasing among all deaths of PeCa patients. Since few previous studies have focused exclusively on other causes of death of PeCa patients, an analysis of causes of death among PeCa patients is warranted. Our study aimed to evaluate the main causes of death including SMTs and non-cancer causes for PeCa patients, and calculate the standardized mortality ratio (SMR) for each reason of death compared with the normal population.
Methods
Data Sources
The data of this study was derived from the Surveillance, Epidemiology, and End Results (SEER) program 18 registries, which is an authoritative source of information on cancer incidence and survival in the United States. SEER currently collects and publishes cancer incidence and survival data from population-based cancer registries covering approximately 27.8% of the U.S. population, and it collects data concerning patient demographics, tumor morphology, stage at diagnosis, primary tumor site, the first course of treatment, and follow-up for vital status. Meanwhile, the data for the general population comes from the Centers for Disease Control and Prevention (CDC) of the United States. All data in this study has been removed identifiable information and can be available freely online. Thus, this study was regarded as exempt research by the institutional review.
Study Population and Study Variables
Patients with PeCa as the first primary malignancy and clear stage information according to the definition of Summary Stage 2000 (1998+) between 2004 and 2018 were included. The patients who had unclear follow-up time, living status at the end of follow-up and detailed causes of death were excluded.
Patients were divided into 3 groups by their stages (localized, regional and distant metastasis). The following variables of all patients and the dead patients were analyzed, including age (15-54, 55-64, 65-74, 75-84, and >85 years), year of diagnosis (2004-2008, 2009-2013, and 2014-2018), race (white, black. American Indian/Alaska native and Asian or Pacific Islander), grade (well-differentiated, moderately differentiated, poorly differentiated, and undifferentiated), main pathological type, Radiotherapy (beam radiation, radioactive implants/brachytherapy and none/unknown) and Chemotherapy (yes and no/unknown).
Outcome Assessments
The causes of death after the diagnosis of PeCa included PeCa deaths, SMTs, and non-cancer deaths were regarded as the main outcomes. The standardized mortality ratio (SMR) with the 95% confidence interval (95% CI) of each cause was also calculated to evaluate the mortality risks compared with the general population. The last follow-up time was December 31, 2018, which was the latest data updated in the SEER database.
Statistics Analyses
For the baseline characteristics of 3 groups of patients with different PeCa stages, we analyzed the number of all included patients and observed deaths stratified by the above variables. The SMRs for each variable were calculated by comparing the observed number of deaths to the expected number. The expected number of deaths was based on the total number of patient-year and the excess risk of the general population. The causes of death and related SMRs and 95% CI were also analyzed in localized, regional, and distant metastasis PeCa patients. Statistical significance for SMR is a two-sided test of P < .05. All these analyses were performed using SEER*Stat version 8.4.0.1. Pie charts of the proportion of different causes of death were drawn with Microsoft Excel 2016.
Results
A total of 3597 PeCa patients were included, 1588 (44%) of them died during the follow-up. The majority of patients was in the localized stage (n = 2,155, 60%) and regional stage (n = 1310, 36%), whereas only 4% (n = 132) had distant disease. For patients with localized PeCa, 800 (37.1%) of them died with a SMR of 2.12 (1.97-2.27). 679 (51.8%) regional PeCa patients [SMR: 4.61 (4.27-4.97)] and 109 (82.6%) patients with distant metastatic PeCa [SMR: 27.68 (22.73-33.39)] died during the follow-up.
Baseline Characteristics of All Patients and Dead Cases During Follow-Up With Localized, Regional, and Distant Penile Cancer.
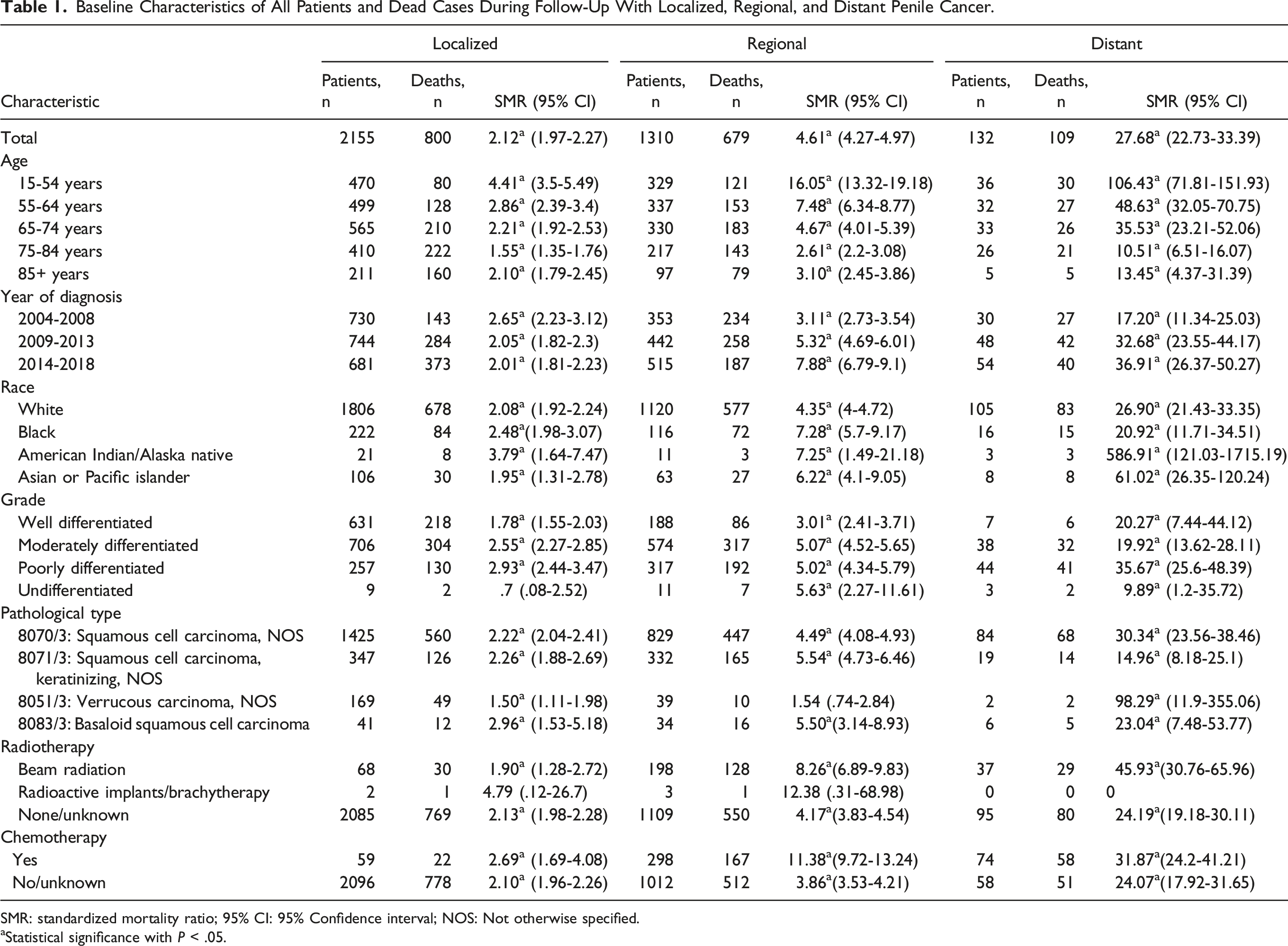
SMR: standardized mortality ratio; 95% CI: 95% Confidence interval; NOS: Not otherwise specified.
aStatistical significance with P < .05.

The number of newly diagnosed of penile cancer from 2004 to 2018.
Causes of Death for Patients With Localized Penile Cancer
Main causes of death for patients with localized penile cancer.
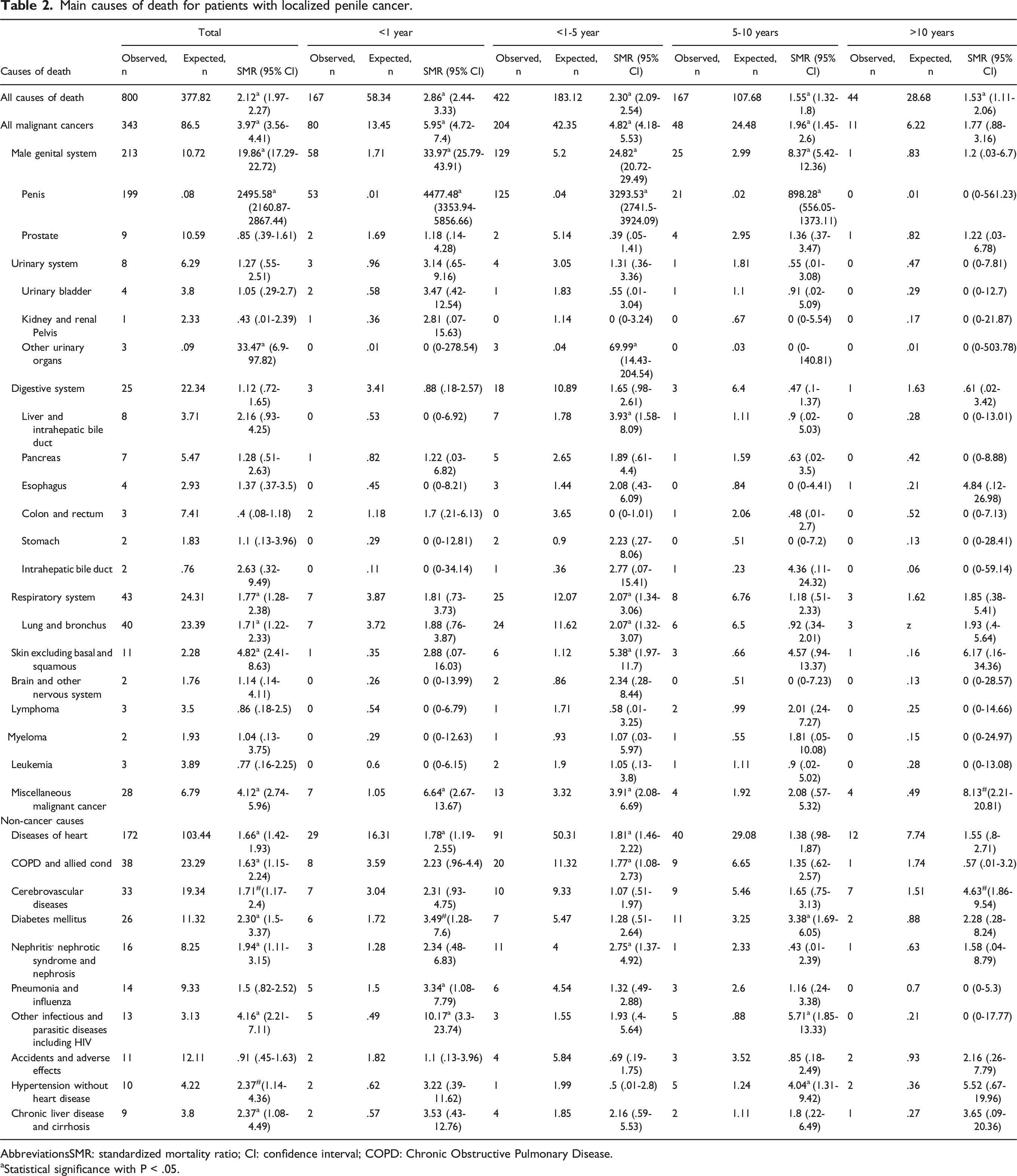
AbbreviationsSMR: standardized mortality ratio; CI: confidence interval; COPD: Chronic Obstructive Pulmonary Disease.
aStatistical significance with P < .05.

Mortality rate of all causes of death, PeCa, SMTs and non-tumor causes for patients diagnosed with localized, regional and distant metastasis penile cancer. (A) Patients with localized penile cancer; (B) patients with regional penile cancer; (C) patients with distant metastasis penile cancer.

The percentages of main causes of death in penile cancer patients. (A) Patients with localized penile cancer; (B) patients with regional penile cancer; (C) patients with distant metastasis penile cancer.
Causes of Death for Patients With Regional Penile Cancer
Main causes of death for patients with regional penile cancer.
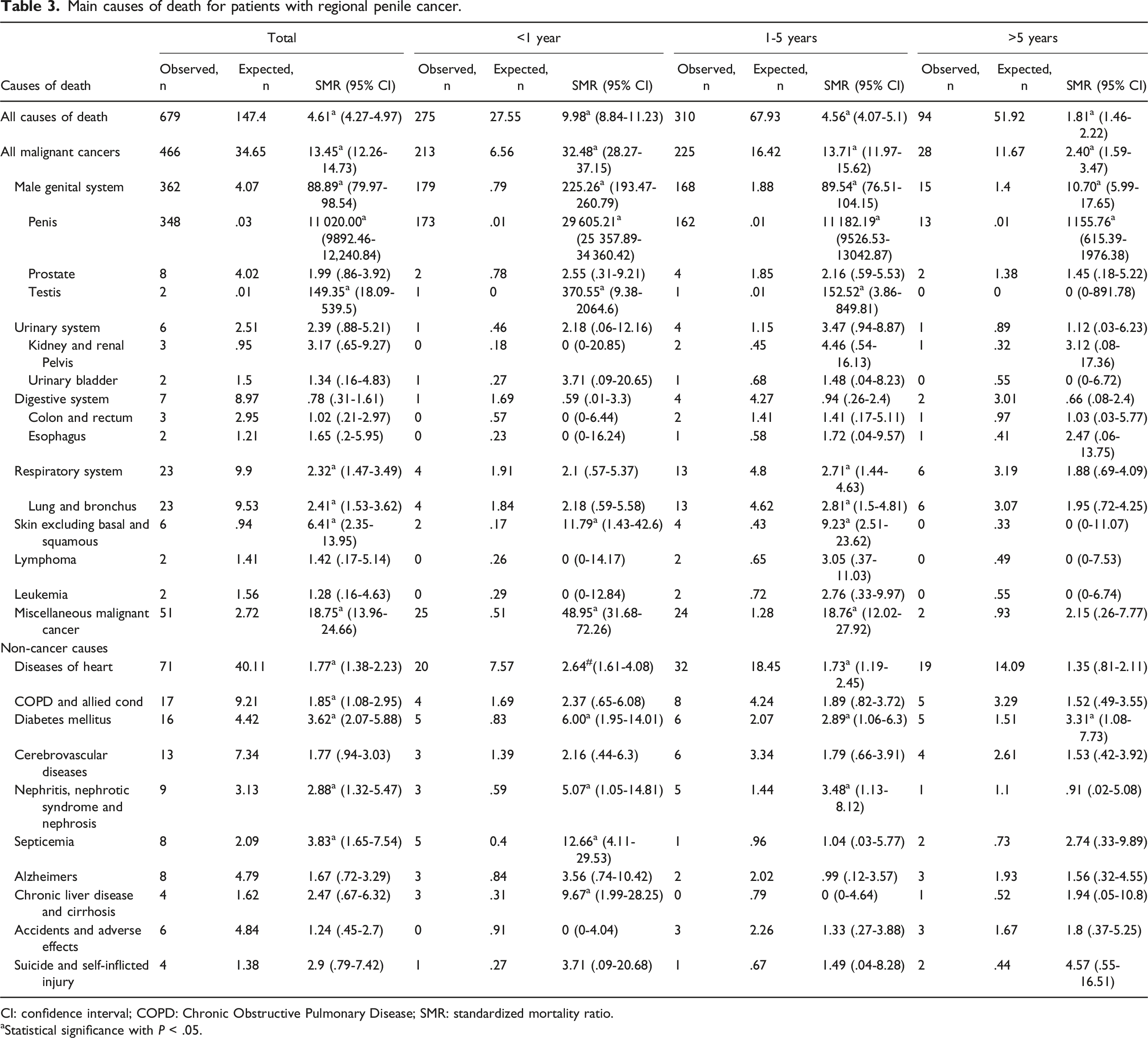
CI: confidence interval; COPD: Chronic Obstructive Pulmonary Disease; SMR: standardized mortality ratio.
aStatistical significance with P < .05.
Causes of Death for Patients With Distant Metastatic Penile Cancer
Main Causes of Death for Patients With Distant Penile Cancer.
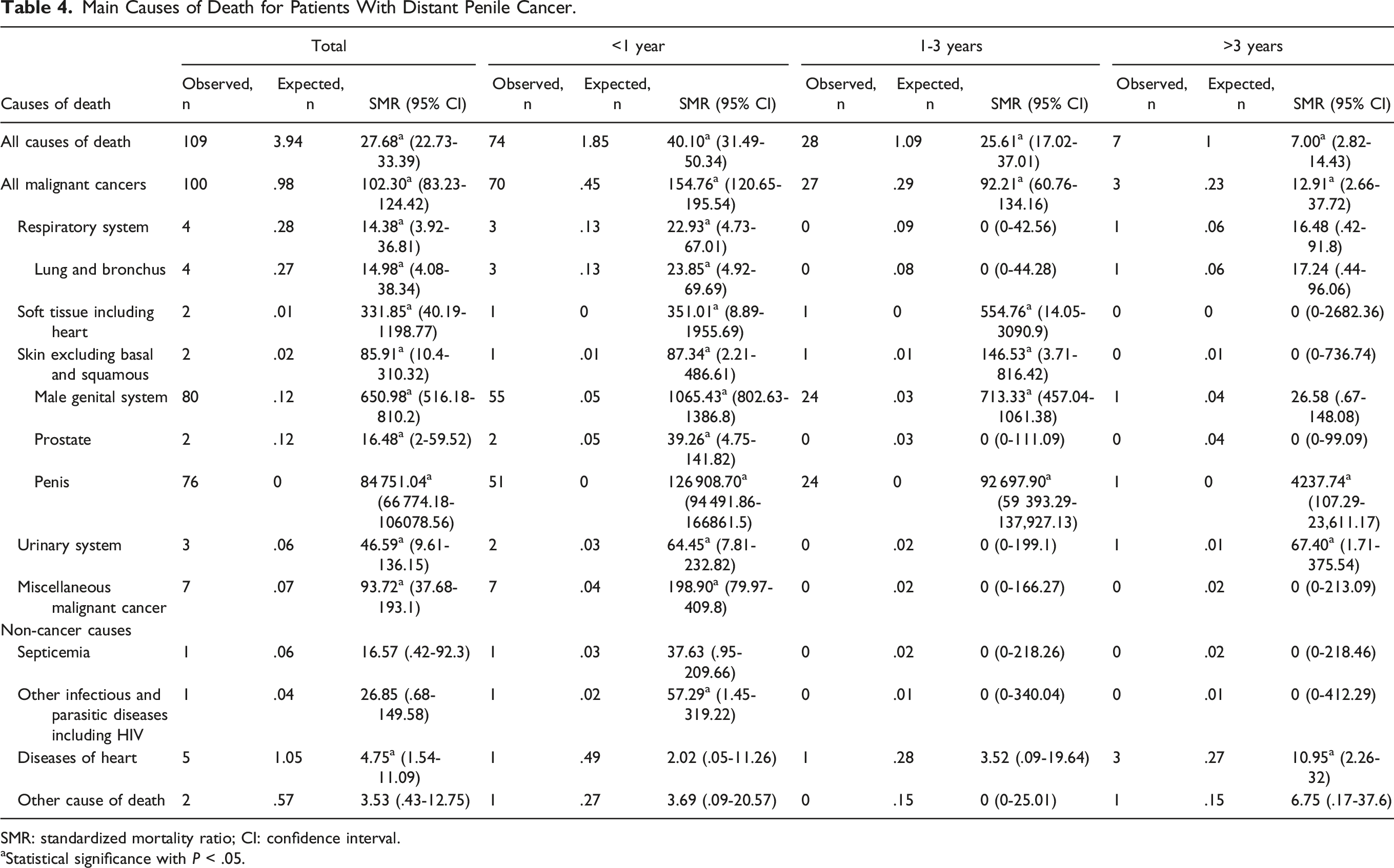
SMR: standardized mortality ratio; CI: confidence interval.
aStatistical significance with P < .05.
Discussion
With the high and increasing survival rate of PeCa, deaths from other causes account for a very high proportion of total deaths and tend to increase. 5 Therefore, other causes of death including SMTs and non-tumor diseases should be taken seriously. Besides, whether these causes have relationships with the diagnosis of PeCa is unclear. In current literature, studies on the SMTs for the primary PeCa were quite rare. Our study, as far as we can know, is the first study focusing on the SMTs and non-cancer causes of death for primary PeCa patients. We also relate these causes to the time period after diagnosis of penile cancer and provide results stratified by tumor stage and patient characteristics to provide valuable insights into the prognosis and management of penile cancer.
According to the basic characteristic of dead patients, people diagnosed with penile cancer between 15 and 54 years had obviously higher SMRs than other age groups. As the number of deaths among 15-54 years old were not obviously higher than other age groups, this result was due to the lower excess risk of the general population. For the general population among 15-54 years, most of them have better physical conditions and a lower rate of all kinds of deaths when compared with the population with elderly age. We also found that the mortality risk continued to decrease with the year of diagnosis from 2.65 in 2004-2008 to 2.01 in 2014-2018 in localized disease. This may be the result of improved cancer treatment and disease management after diagnosis for PeCa over time. However, this result was reversed in regional and distant metastatic disease. White people accounted for a higher proportion of all deaths, but black people had a higher risk of death in localized and regional diseases. Previous studies reported that the mortality rate of blacks was higher than that of whites among American penile cancer patients. 6 This may be due to earlier exposure of blacks to HPV through early sexual contact, leading to an earlier diagnosis of penile cancer.6,7
For localized and regional diseases, deaths from SMR accounted for a certain percentage of total deaths. A study identified 3641 PeCa patients in the Swedish Family-Cancer Database from 1958 to 2015. They found that SMTs occurred in 16.8% of primary PeCa patients and 45.9% of these patients dead for SMTs rather than PeCa. 8 The main SMTs included prostate cancer, colorectum cancer, lung cancer, bladder cancer, skin squamous cell cancer and stomach cancer. These results were similar to ours. This study also reported that SMTs was associated with HPV and smoking. 8 Another study with 1634 men with PeCa found a 2-3-fold increased risk of a second human papillomavirus (HPV) associated cancer of the oral cavity, oropharynx and anal canal among PeCa patients. 9 For the occurrence of PeCa, there were some important risk factors of PeCa including lack of circumcision, smegma retention, chronic balanitis, lichen sclerosis, obesity, smoking, HPV infection and immune-compromised states.10,11 It may be the consequences of treatment for penile cancer and the more widely spread of HPV.12-14
For the non-tumor deaths, it accounted for a large proportion among all deaths in localized and regional stages. A previous study reported that 65.7% of deaths were due to non-cancer causes among PeCa patients without SMTs and only 28.4% were due to penile cancer. 8 Cardiovascular disease is still a major cause of death in PeCa patients. Statistics in recent years from a study had shown that more than 20% of PeCa patients died from cardiovascular disease. 15 It was also reported that the risk of cancer patients dying from cardiovascular diseases was inversely related to the age at diagnosis. 15 For this kind of cancer with a good prognosis but still a high risk of cardiovascular death, patients may benefit from clinical intervention by a cardiologist at the time of diagnosis. There were some relationships between diabetes mellitus and PeCa. Previous studies reported that diabetes was associated with phimosis, which could increase the risk of penile cancer.16-18 Men with diabetes, mainly type 2 diabetes, were associated with an increased incidence of penile squamous cell carcinoma compared with men without diabetes. 19 Localized and advanced PeCa and the associated treatments have profound physical and psychological effects on the survivors’ quality of life. Due to potentially crippling surgery, patients with penile cancer increased psychological stress and therefore have an increased need for psychosocial care.20-22 However, in our study, we didn’t find a significantly increased risk of suicide and self-inflicted injury. 22
For patients with distant metastatic PeCa, the prognosis was poor with a mortality rate of 82.6%. The main cause of death in patients was the penile cancer tumor itself. Other causes of death only account for only a small fraction of all deaths. Therefore, active and effective treatment for metastatic penile cancer is still the most important measure to prevent deaths and prolong survival durations.
Our study is the first to provide the most comprehensive comparison and description of the risk of death from all causes in PeCa patients using tumor stage and time after diagnosis. However, there were some limitations in our study. Firstly, we used Summary Stage 2000 (1998+) to distinguish local, regional and distant diseases, but these classifications maybe not the same in different periods. Therefore, the results of this study can’t fully represent the current staging results. Secondly, some important information of patients in this database was available, such as the basic illness, detailed treatments and socioeconomic status, etc. The information might have certain impacts on the survival and prognosis of patients. Our results might be influenced by the missing information. Thirdly, the sample size selection was not estimated by power calculations. It was also a limitation of our study.
Conclusion
Our study provided a detailed analysis of the causes of death for patients with locally, regionally, and distant metastatic PeCa after diagnosis. This information could be useful for disease prevention and health care during patients’ survivorship.
Supplemental Material
Supplemental Material - Second Malignant Tumors and Non-Tumor Causes of Death for Patients With Penile Cancer During Their Survivorship
Supplemental Material for Second Malignant Tumors and Non-Tumor Causes of Death for Patients With Penile Cancer During Their Survivorship by Pan Song, Xiaotian Wu, Luchen Yang, Kai Ma, Zhenghuan Liu, Jing Zhou, Junhao Chen, Qing Zhu, and Qiang Dong in Cancer Control
Footnotes
Author Contributions
P.S., X.W. and L.Y.: project development, data collection and analysis, manuscript writing. K.M., Z.L.: data collection and analysis, manuscript writing. J.Z., J.C. and Q.Z.: manuscript writing. Q.D.: project development. All authors confirm that they read and approved the final draft for submission. All authors are also responsible for the manuscript content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Key Project of National Natural Science Foundation of China; Grant ID: 8177060452; Project of Science and Technology Department of Sichuan Province, Grant ID: 2021YFS0117; and Project of Science and Technology Department of Chengdu City, Sichuan Province, Grant ID: 2021YF0500717SN.
Ethical Approval
All data were obtained from the public available database. All patients’ data we obtained from the database was de-identified. Therefore, our study was exempted by the ethics committee of West China Hospital of Sichuan University.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.