
Abstract
Background:
Data about the risk factors and pancreatic cancer in developing countries remain limited. We investigated for the first time the role of a number of risk factors (family cancer history, smoking, alcohol consumption, diabetes, inflammation disease, HBV infection) associated with pancreatic cancer among Vietnamese patients.
Methods:
We included all patients hospitalized at 4 Northern Vietnamese hospitals (Vietnam National Cancer Hospital, Bach Mai, Viet Duc, Thai Nguyen) and diagnosed with pancreatic cancer during the period from 2017 to 2019. Risk factors of eligible patients were collected and assessed the associations using a matched control study and logistic regression model analysis.
Results:
We identified 196 patients with diagnosis of pancreatic cancer of which 114 males and 82 females. The average age of the patient at the time of diagnosis was 58.28 years (standard deviation of 12.94, ranging from 25 to 87). Most of patients were diagnosed at advanced stage (85%). Smoking, diabetes, inflammation disease significantly increased the cancer risks (OR and 95% CI were 2.42 (1.38-4.37), 3.09 (1.54-6.68), 2.21 (1.42-3.45), respectively). HBV infection demonstrated a significant link with pancreatic cancer in univariate model (OR = 2.94 (1.08-9.36)), but not in multivariate model. However, cancer family history and alcohol drinkers did not show any significantly increased risk related to pancreatic cancer.
Conclusions:
Our finding showed smoking, diabetes, inflammation disease significantly increased the risk of pancreatic cancer in Vietnam.
Background
Pancreatic cancer is a poor prognostic cancer and considered as “a silent killer.” Due to the lack of early detection, most pancreatic cancers are diagnosed at an advanced stage (approximately 50% of all pancreatic cancers are diagnosed after metastases). In fact, no strong evidence of an effective treatment for localized pancreatic cancer has been found, and no screening policy for pancreatic cancer has been well established until now. Worldwide, pancreatic cancer caused 432,242 deaths in 2018 (with 458,918 cases) according to GLOBOCAN 2018. 1 In the United States, the incidence of new pancreatic cancer in men and women ranked ninth and tenth, respectively; however, the mortality rate is even higher, ranking fourth for both male and female. 2 Pancreatic cancer has the lowest overall survival rate after 5 years (5%-6%) and the shortest life expectancy (6 months) in comparison to other cancers. 2,3 In addition, while the new incidence and mortality rates of other cancers decreased, the incidence of pancreatic cancer increased by 1.5% per year, 2,4,5 with no significant improvement in mortality rate over the past 4 decades. 5,6 It is important to note the increasing incidence, because it is possibly due to environmental factors. Actually, mortality increases in parallel with the incidence because there is no effective treatment, whatever the cancer stage. The choices of pancreatic cancer treatment are also limited. Indeed, for advanced stages, chemotherapeutic agents are mostly inefficient. Even at localized stages, 5-year survival rate for potentially curative resection is only about 20% (39.4% for localized cancer and 13.3% for regional cancer). 7,8 Hence, there is an urgent need to identify risk factors to possibly control pancreatic cancer. In fact, there were more than 50 specific modifiable and non-modifiable risk factors related to pancreatic cancer that were well described in 100 meta-analytical or pooled reports. 9 Fortunately, about two-thirds of these risk factors are potentially modifiable. Smoke, alcohol consumption, chronic pancreatitis, obesity, diabetes mellitus, unhealthy dietary behavior, and physical activity could majorly contribute to the risk of pancreatic cancer. 9 -14 In this study, we intended to assess the association between some risk factors and pancreatic cancer to evaluate whether the known association between these risk factors and pancreatic cancer could be replicated in our cohort study related to Vietnamese patients.
Methods
Data Source and Pancreatic Cancer Case and Control Identification
We identified all patients aged 18 years or above who were diagnosed with primary pancreatic cancer and hospitalized at 4 Northern Vietnamese hospitals (Vietnam National Cancer Hospital, Bach Mai, Viet Duc, and Thai Nguyen) during the period from January 1, 2017, to June 30, 2019. We then only included patients with the confirmed diagnosis of pancreatic cancer based on histopathology, computed tomography (CT), magnetic resonance imaging with magnetic resonance cholangiopancreatography, or endoscopic ultrasound. Primary tumor (T), regional lymph nodes (N), and metastasis (M) status were evaluated using the criteria of AJCC 7th Cancer Staging Manual. Disease stage was identified by assessment of TNM mentioned above. 15 We excluded patients who had a history of any other cancer at any time prior to the pancreatic cancer diagnosis date or who disagreed to participate in the study. The calculated sample size was not required because we applied the convenience sampling method, and this was a preliminary study based on Vietnamese population.
For each pancreatic cancer case, we randomly selected one control subject from the cohort of healthy control patients who had a cancer screening at our hospitals without a diagnosis of pancreatic cancer or of any other cancers. The chosen control was also matched on age, sex, and calendar time (i.e., using the same index date as for cases) with the corresponding case.
Medical records reviews followed by patient interviews (if needed in case of missing data) have been carefully conducted to identify sociodemographic characteristics, lifestyle factors including tobacco and alcoholism situation (alcohol consumption with amount of alcohol intake at least 30 g/day or 150 g/week), and history of selected medical conditions including diabetes, inflammation diseases (asthma, autoimmune diseases, celiac disease, glomerulonephritis, hepatitis, inflammatory bowel disease, transplant rejection, or other similar conditions), and hepatitis B virus (HBV) infection.
The study was performed in accordance with the Declaration of Helsinki, and written informed consent was obtained from patients before participating in the study. The study protocol was reviewed and approved by the Institutional Review Board of Vietnam National Cancer Hospital. Patients were given a full explanation of the purposes and nature of study, and they could voluntarily withdraw at any time during the research process. The collected data would be kept confidentially for the purpose of research only.
Statistical Analyses
We mainly analyzed the information related to age, gender, smoking, alcohol drinking, diabetes, inflammation disease, and HBV infection of all eligible patients. Continuous variables were described by mean (±SD), and categorical variables were described by frequency and percentage. For comparison of parameters between case and control groups, Fisher’s exact test or chi-square tests were applied for categorical variables, and Student’s test (t-test) was applied for continuous variables. Odds ratios (OR) were used to describe the links of pancreatic cancer and risk factors. Univariate and multivariate logistic regression models associated with selected lifestyles and other suggested risk factors were used to estimate OR and its 95% confidence interval (CI). Correspondingly, variables like age (continuous variable), gender (male, female), family history of cancer (yes, no), history of diabetes (yes, no), previous alcohol drinking (yes, no), history of smoking (yes, no), any inflammation disease (yes, no), and HBV infection (yes, no) were included in the models. Factors significantly increase the risk of pancreatic cancer if the lower bound of 95% CI is >1 and significantly reduce the risk of pancreatic cancer if the upper bound of 95% CI is <1. R version 3.4.4 (released on March 15, 2018) was used to perform the statistical analysis. 16
In order to have similar characteristics in terms of age, gender, and calendar time between cases and controls, we used the random pairing technique (1:1 ratio) by using the MatchIt package based on R. 17
Results
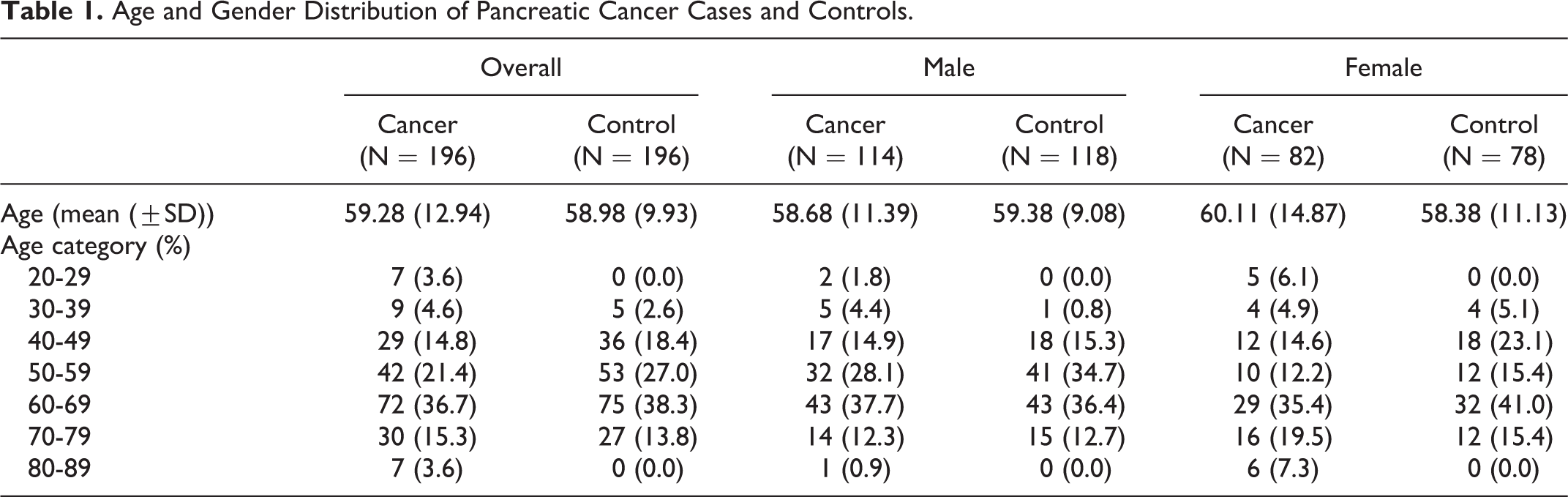
We identified 196 pancreatic cancer patients and 196 matched controls for the analysis. The mean age of the case group and control group was 59 years, with a sex ratio (male/female) of 1.76 (Table 1). We also found pancreatic cancer patients mainly aged from 50 to 69 years (58.1%).
Age and Gender Distribution of Pancreatic Cancer Cases and Controls.
Among pancreatic cancer patients, 149 cases (78%) were newly diagnosed, and 43 cases (22%) were diagnosed before January 2017. Most of them were diagnosed at an advanced stage (stage III-IV, accounting for 85% of patients) (Table 2). CT was the main diagnosis method for pancreatic cancer (69%), followed by histopathology (28%).
Clinical Characteristics of Pancreatic Cancer Patients.

Table 3 presents the characteristics of some selected risk factors. The results show that patients in the control group had more family history of cancer than pancreatic cancer patients. Especially in the women subgroup, there is a higher frequency of smoking, alcohol consumption, and diabetes among pancreatic cancer patients. Overall, we found significant differences in terms of presence of family cancer history (p < 0.001) between cases and controls, whereas no difference was found between the 3 groups for tobacco, alcohol consumption, and diabetic comorbidity.
Description of Some Risk Factors of Pancreatic Cancer Cases and Controls.

Table 4 presents ORs and their 95% CI of pancreatic cancer calculated using univariate and multivariate models for selected risk factors. Only family history of cancer did not increase the risk in both adjusted models. Smoking, past or present history diabetes, and inflammation disease significantly increased the risks of cancer (ORs were 2.42 (1.38-4.37), 3.09 (1.54-6.68), and 2.21 (1.42-3.45), respectively). Current alcohol drinkers did not show any significantly increased risk related to pancreatic cancer in the univariate and multivariate models.
Risk Factors Associated With Pancreatic Cancer.

a The multivariate regression model is adjusted by age and gender.
b The multivariate regression model was adjusted by age, gender, family history of cancer, diabetes, smoking, inflammation disease and HBV infection.
Discussion
Majority of pancreatic cancer cases are diagnosed at the advanced stage; therefore, curative treatment is usually inapplicable. Until now, there is currently no official guideline nor consensus on screening individuals for this disease. By analyzing the pathogenesis related to both genetic and environmental factors in this study, we could contribute to the existing knowledge of pancreatic cancer in the context of developing countries.
In our matched case–control study based on Vietnamese patients, alcohol consumption and diabetes were identified as risk factors of pancreatic cancer. The risk related to diabetes was even more significant in the women subgroup, whereas it mitigated in the men subgroup. Until now, the mechanism of increased risk of pancreatic cancer in people with diabetes is still unknown. However, the link between diabetes and the risk of pancreatic cancer has been reported in many recent studies. In the study of Gupta et al., the incidence of pancreatic cancer in diabetic patients was 2.2 times higher than that of nondiabetic patients and highest in the first 2 years since the diagnosis of diabetes.
18
The incidence of pancreatic cancer significantly decreased in the following years of follow-up (p < 0.0008). The relationship between diabetes and pancreatic cancer is most pronounced in younger patients. In an 11-year follow-up study of 2,186,196 Israeli population, hazard ratios (HR) for pancreatic cancer were significant and nearly the same between men and women (HR = 3.25, 95% CI 2.85-3.69 and HR = 3.10, 95% CI 2.72-3.52, respectively).
19
However, in a Czech Republic study, the proportion of pancreatic cancer in diabetic men was significantly higher than that of women (43.9% versus 25%), while this rate in the group without diabetes is equivalent (22.1% compared to 17.2%).
20
Once again, our finding confirmed the diabetes-related pancreatic cancer risk and is in favor that women are at higher risk than men (see
It is well known that smoking is associated with pancreatic cancer, as the continuation and cessation of smoking were correlated with the increase and plateau of the disease incidence in Japan for about 40 years of surveillance. 8 Research showed that quitting smoking immediately could decrease 15%-20% cases of pancreatic cancer and mortality rate. 21 -23 Hence, nontobacco exposure is the best way to reduce the incidence of pancreatic cancer.
In a pool analysis of 6507 pancreatic cases and 12,890 controls, Bosetti et al. pointed out an increase of pancreatic cancer risk in smokers with an OR of 2.2 for current smokers and only 1.2 for former smokers, and the risk was strongly related to the amount and duration of tobacco exposure. 24 A cohort study in the Netherlands conducted by Heinen et al. demonstrated that the risk of pancreatic cancer increased for every period of 10 years of smoking (HR = 1.15, 95% CI 1.08-1.22) and for every amount of 10 cigarettes/day (HR = 1.08, 95% CI 0.98-1.19). 22 It is also commonly accepted that the impact of smoking on cancer may vary between populations. Therefore, some ethnic differences may exist regarding susceptibility to the effects of smoking. In a study by the International Agency for Research on Cancer, smoking was confirmed to be highly associated with pancreatic cancer and correlated with smoking duration and number of cigarettes per day 25,26 In a meta-analysis including 82 studies, the risk of pancreatic cancer was significantly elevated for current and former smokers (risk relative values were 1.74 and 1.2, accordingly). 27 A recent meta-analysis publication of Ben et al. involving 20 studies and 2,517,623 participants also showed similar results, in both the Western regions and the Asia-Pacific regions. 28 Our finding was in favor of the results above.
Regarding alcohol use, research shows that alcohol intake was significantly associated with an increased risk of pancreatic cancer, especially high alcohol intake. 29 The results of a prospective study conducted by Gapstur et al. and a pooled analysis of 10 case-control studies in the International Pancreatic Cancer Case–Control Consortium conducted by Lucenteforte et al. strongly pointed out that alcohol consumption, particularly heavy intake, was an independent risk factor for pancreatic cancer regarding smoking status. 30,31 In a pooled analysis of 14 cohort studies, consuming 30 g or more of alcohol daily increases the risk of pancreatic cancer compared with non-alcohol users (pooled multivariate RR = 1.22, 95% CI 1.03-1.45). 3 Despite no clear biological mechanism and association of alcohol intake and pancreatic cancer, alcohol drinking remains an important cause of chronic pancreatitis, which could induce pancreatic cancer. However, our finding did not show a similar result. Indeed, the association of the risk factor with pancreatic cancer could vary among populations due to difference in sociodemographic characteristics and lifestyles.
The risk of pancreatic cancer increases with age, with 80% of cases diagnosed at age 60-80. 32 Only about 10% of patients have pancreatic cancer under 50 years old, and pancreatic cancer is a rare condition at the age of under 25. 32 In the United States, 81.4% of patients are diagnosed with pancreatic cancer over 60 years old. In the past 6 decades, only 1 in every 100,000 Americans aged 20-29 had pancreatic cancer; however, at the age of over 80, this figure reached 87.2 in every 100,000 people. People over the age of 70 have 4 times the risk of pancreatic cancer compared to those under 50 years old. 33 However, in our study, we found 86 (43.9%) patients under 50 years old, of which 3 patients are 25 years or below, as well as a striking observation in young patients with pancreatic cancer. Compared to a series of patients from Western countries, our patients were relatively younger at the time of diagnosis. Our findings were also different from the results of a study conducted by Hana et al. in Kuwait in terms of patient age 32 and were not in favor of the general concept about this cancer: the incidence rates were the highest in older than 70 years and increased with age. 14,34 However, similar to Western countries, pancreatic cancer in this region occurs more in men than in women. This is probably related to the higher prevalence of smoking and some other risk factors among males. 35
Family history presents as one of the risk factors of pancreatic cancer, and about 5%-10% of individuals with pancreatic cancer report a history of pancreatic cancer in first-degree relatives. 36,37 In people with a family history of pancreatic cancer, the risk of pancreatic cancer was 1.68-30 times higher than those without a family history of pancreatic cancer. 38 -41 However, the role of family history of cancer did not show a similar result in our study.
Many human cancers result directly from chronic inflammation, which has been shown to play an important role in pancreatic carcinogenesis for more than 150 years, especially chronic pancreatitis. 42 Although the mechanisms involved in inflammation associated with pancreatic cancer are not completely understood, the results of our study suggest a link between any inflammation situation and pancreatic cancer.
Few studies have reported the association between pancreatic cancer and some chronic infections such as HBV. 43 The global prevalence of HBV infection also varies widely. In Asian countries, it is divided in 3 groups: low, intermediate, and high endemic areas of HBV. Vietnam is now considered as high endemic area of HBV, especially in rural area. 44 Therefore, it could be in favor of the association between pancreatic cancer and HBV in our study.
Our study had several potential limitations. The use of administrative data may result, to some extent, in selection bias. An under-detection or under-diagnostic of cancer situation is inevitable because not all healthy patients performed specific image scanning in the hospitals. Besides, the incomplete information regarding the exact amount of tobacco and alcohol consumption as well as diet history, inflammation diseases, and diabetic situation in the study could potentially modify the risk of pancreatic cancer. Finally, the data were not sufficient to confirm all the risk factors mentioned above; therefore, further studies evaluating these associations are required. A number of methodological issues relevant to the case–control study also need to be carefully considered. Regarding possible biases, we collected and validated the data by hospital-based cancer medical records combined with patient interviews to ensure the quality of data. In addition, we applied the 1:1 ratio matching technique in order to put the cases and controls in the similar setting. Besides, our finding reflected, to some extent, the pancreatic cancer picture in a developing country, and the results from the 4 sizable hospitals in our study could be represented for the real situation in Northern Vietnam. The added value of our study was linked to the specific population concerned in the context of resource-limited settings. Risk factors of pancreatic cancer could be modified under the different contexts related to genetics, sociodemographic features, alimentary behaviors, and lifestyles. When compared with the results of published meta-analysis studies (whose data were mainly from Western countries), our study could contribute and shed some light on the existing data and knowledge about the risks related to pancreatic cancer throughout the world.
Conclusions
In conclusion, we observed significant associations of smoking, diabetes, and inflammation disease to pancreatic cancer risk in Vietnam. However, alcohol consumption and family history of cancer did not show an increased risk of pancreatic cancer. Further studies are required to confirm these risk factors as well as give clues to the interactions of other environmental or endogenous factors related to pancreatic cancer, including the genetic background.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274821989320 - Risk factors of Pancreatic Cancer in Vietnam: A Matched Case–Control Hospital-Based Study
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274821989320 for Risk factors of Pancreatic Cancer in Vietnam: A Matched Case–Control Hospital-Based Study by Thuan Van Tran, Tu Van Dao, Khac-Dung Nguyen, To van TA, Khanh Truong Vu, Son Hong Trinh, Hoang Cong Nguyen, Oanh Thi Bui, Quang Tien Nguyen, Hoan Duc Vu, Hiep Le Nguyen and Huong Thanh Tran in Cancer Control
Footnotes
Authors’ Note
Thuan Van TRAN, MD, PhD and Tu Van DAO, MD, PhD, equally major contributed to this work. Our study was approved by National Ethic Committee (approval No.3165/QD-BKHCN, 26th October 2016). All patients provided written informed consent prior to enrollment in the study.
Acknowledgments
The authors would like to thank Pr Guilhem Bousquet (MD, PhD) for critically revising the manuscript. The authors would also like to thank ENAGO for the English language review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received the governmental financial support for the research related to content of this article [KC.10/16-20].
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.