
Abstract
Objectives
To evaluate the feasibility, safety, and efficacy of computed tomography(CT)-guided percutaneous radiofrequency ablation (RFA) in medically inoperable older adults with clinical stage I non-small cell lung cancer (NSCLC).
Patients and Methods
We retrospectively reviewed the records of medically inoperable older adults (≥70 years) with clinical stage I NSCLC who underwent percutaneous multi-tined electrode RFA at our institution between January 2014 and December 2018. We analyzed the patients’ characteristics, therapy response, survival, as well as the procedure-related complications.
Results
Eighteen patients (10 men and 8 women) with a mean age of 75.9 (71−85) years were treated in during the study period. The median tumor size was 25 mm (range, 19−43 mm); 10 and 8 cases involved stage T1 and T2a disease, respectively. The median follow-up duration was 25 (11–45) months. RFA was technically successful for all 18 lesions, with no treatment-related mortality. The disease control rate was 83.3% (15/18 lesions). There were 6 cases of pneumothorax: one symptomatic case requiring thoracic drainage, and five requiring no treatment. Minor complications, including pulmonary infection, chest pain, fever, and cough, were treated within 4 days (range, 1−4 days). The progression-free survival rates were 83.3%, 64.9%, and 51.9% 1, 2, and 3 years, respectively. The corresponding overall survival rates were 92.2%, 81.5%, and 54.3%, respectively.
Conclusions
CT-guided percutaneous RFA is safe and effective in medically inoperable patients with stage I NSCLC and could be an alternative therapeutic strategy, particularly in older adults with early-stage peripheral lung cancer.
Keywords
Introduction
Lung cancer is one of the most common malignant tumors and the leading cause of cancer-related death in both men and women worldwide. Among malignant tumors, the incidence and mortality of lung cancer rank first in China. 1 Although surgical treatment is considered the gold standard for patients with early-stage non-small cell lung cancer (NSCLC), only one-fourth to one-third of patients are eligible for surgery in clinical settings. Some cardiovascular, pulmonary, and other medical-related comorbidities may make patients ineligible for surgical treatment,2,3 and a large proportion of older adults with NSCLC could have such comorbidities. 4
For patients with medically inoperable stage I NSCLC, stereotactic body radiation therapy (SBRT) has been considered as the standard of care. SBRT has been shown to be particularly effective in eradicating primary and metastatic tumors.5-7 However, radiation pneumonitis is a potentially life-threatening complication, particularly in patients with impaired lung function or synchronous multiple tumors in the lungs.8-10 Therefore, other alternative therapies are needed for patients with medically inoperable early-stage NSCLC.
In the last several years, minimally invasive nonsurgical treatment of lung cancer has become more established. Particularly, image-guided percutaneous ablation has been successfully used in selected patient groups. At present, radiofrequency ablation (RFA), microwave ablation, and cryoablation are the main methods of percutaneous ablation in clinical practice. The purpose of lung ablation for malignant tumors is to achieve complete ablation, including a margin of normal surrounding parenchyma, avoid injury to critical structures, and create an ablation zone quickly. 11 Percutaneous lung ablation is most suitable for patients who are ineligible for surgery due to medical comorbidities, poor lung function, postoperative recurrence, or refusal of surgery. 12
As an accurate, minimally invasive, and reproducible treatment, RFA has been widely used for various types of cancer, including lung, 13 liver, 14 kidney, 15 and bone cancers. 16 Under the guidance of computed tomography (CT), percutaneous RFA has been applied for over a decade in the treatment of primary and secondary liver tumors with impressive and promising therapeutic outcomes.17,18 This approach has also recently been evaluated for primary and metastatic lung cancer.19,20 Some preliminary results suggested that CT-guided RFA is a safe and feasible treatment, and can achieve satisfactory local control and survival in patients with early-stage lung cancer.21-23 However, although most patients with early-stage lung cancer are older adults, there has been no specific analysis on the efficacy of RFA in patients older than 70 years.
In this study, we retrospectively evaluated our results regarding the use of CT-guided percutaneous RFA in the treatment of older adults aged ≥70 years with medically inoperable stage I NSCLC to determine its feasibility, safety, and efficacy.
Patients and Methods
Population
This study was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Hainan Medical University (No. HMU0140023), China. All patients gave written informed consent before RFA. The therapeutic indications, efficacy, and risk of death were explained to the patients and their guardians.
The research was conducted and reported in accordance with the STROBE guidelines. We retrospectively reviewed the records of patients with clinical stage I (T1-2aN0M0) NSCLC who underwent CT-guided RFA in our institution in the period from January 2014 to December 2018. The inclusion criteria were as follows: (1) age ≥70 years; (2) histopathologically confirmed NSCLC; (3) ineligibility for surgery (medically inoperable or refused surgical resection); and (4) tumors accessible by the percutaneous route. Patients with metastatic NSCLC were excluded from the analysis.
All patients were stratified according to the 7th edition of the TNM staging classification. The tumor size and tumor-bronchus relationship were evaluated by thin-slice CT in all patients. The absence of lymph node involvement was confirmed by contrast-enhanced chest CT. Patients with hilar or mediastinal nodes with a short axial diameter greater than 10 mm on CT images underwent positron emission tomography (PET) to exclude N1 or N2 disease. To evaluate extra-thoracic distant metastasis, abdominal CT, brain magnetic resonance imaging, and isotopic bone scanning were performed. In some adenocarcinoma patients, genetic analysis of tumors was performed, including epidermal growth factor receptor (EGFR) gene analysis. All cases were discussed with a multi-disciplinary team that comprised medical oncologists, thoracic surgeons, radiation therapists, and interventional radiologists. Patients taking anti-coagulation and anti-platelet medications were advised to stop usage 7 days before the procedure.
Treatment and Technique
RFA was performed using the RITA system (MEDSPHERE S-1500, MEDSPHERE, Shanghai, China), powered by 100 W generators with a 17-gauge multi-tined expandable electrode. The maximal power used was 90 W, depending on the lesion size, vascularity, and location, and the patients’ tolerance. Patients were trained to breathe at rest 1 day before the procedure and fasted water for 2 hours before treatment. CT (Siemens 64-slice Somatom Sensation, Erlangen, Germany) was used for lesion localization. The patient’s position during the procedure was determined according to the tumor location. The skin entry site that allowed the shortest route that avoided bullae, interlobar fissures, or pulmonary vessels was selected. After the skin was cleansed with iodine and alcohol, local infiltration anesthesia was performed at the predetermined puncture point from the skin and subcutaneous tissue to the pleura using 2% lidocaine. Next, the electrode needle was placed into the distal end of the tumor. When it was confirmed on CT that the needle was in the predetermined position, RFA of the target lesion was performed. The ablation time for each target lesion was 10−20 min and the maximum tissue temperature was 90°C. The purpose of ablation was to induce coagulation necrosis of the surrounding tissue in a radius of 5−10 mm beyond the lesion margins. At electrode retrieval, the electrocoagulation mode was turned on to ablate the tracts for preventing tumor cell seeding and bleeding. If pneumothorax occurred during the procedure, closed thoracic drainage was performed according to the clinical symptoms.
Post-ablation complications were classified as major (hypertensive crisis, hemothorax, and pneumothorax) and minor (pain, post-ablation syndrome, and skin irritation). All patients underwent post-RFA chest CT and were hospitalized and monitored for complications. If no complication occurred, they were discharged within 24 h.
Follow-up chest contrast-enhanced CT was performed at 1, 3, 6, 9, and 12 months after RFA and every 6 months thereafter. CT images were evaluated by at least two experienced radiologists (at least 5 years experience), including a lung RFA ablation operator. Local tumor progression was defined when the ablation zone exhibited a continued increase in size after reduction. The appearance of an irregular, scattered, nodular, or eccentric enhancement focus in the ablation zone on imaging was also considered local progression. 24 For suspicious lesions, enhanced CT follow-up was closer, usually once a month. If follow-up CT confirms the progression, the time of disease progression is when the first time was suspicious.
The response to RFA was evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST). Complete remission (CR) was defined when all target lesions disappeared completely and no new lesions appeared over at least 4 weeks. Partial remission (PR) was defined when the maximum diameter of target lesions decreased by ≥ 30% after treatment and this decrease was maintained for at least 4 weeks. Progressive disease (PD) was defined when the sum of the maximum diameters of the target lesion increased by at least ≥ 20% after treatment or new lesions appeared. Stable disease (SD) was defined when the maximum diameter of the target lesion decreased by less than 30% or increased by less than 20% over at least 3 months after RFA. The disease control rate (DCR) was calculated based on the cases of CR, PR, and SD. Progression-free survival (PFS) was defined as the period from RFA treatment initiation to tumor progression. Overall survival (OS) was defined as the period from RFA treatment initiation to death or last follow-up.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics version 18 (IBM Corp, Armonk, NY, USA). The OS and PFS were calculated using the Kaplan–Meier method.
Results
Patients’ Characteristics
From January 2014 to December 2018, a total of 58 patients with NSCLC underwent CT-guided RFA at our center. Of these, 40 patients were excluded; 13 due to metastatic NSCLC and 27 due to age <70 years. Finally, 18 patients were included in this study.
Clinical characteristics of the enrolled patients.
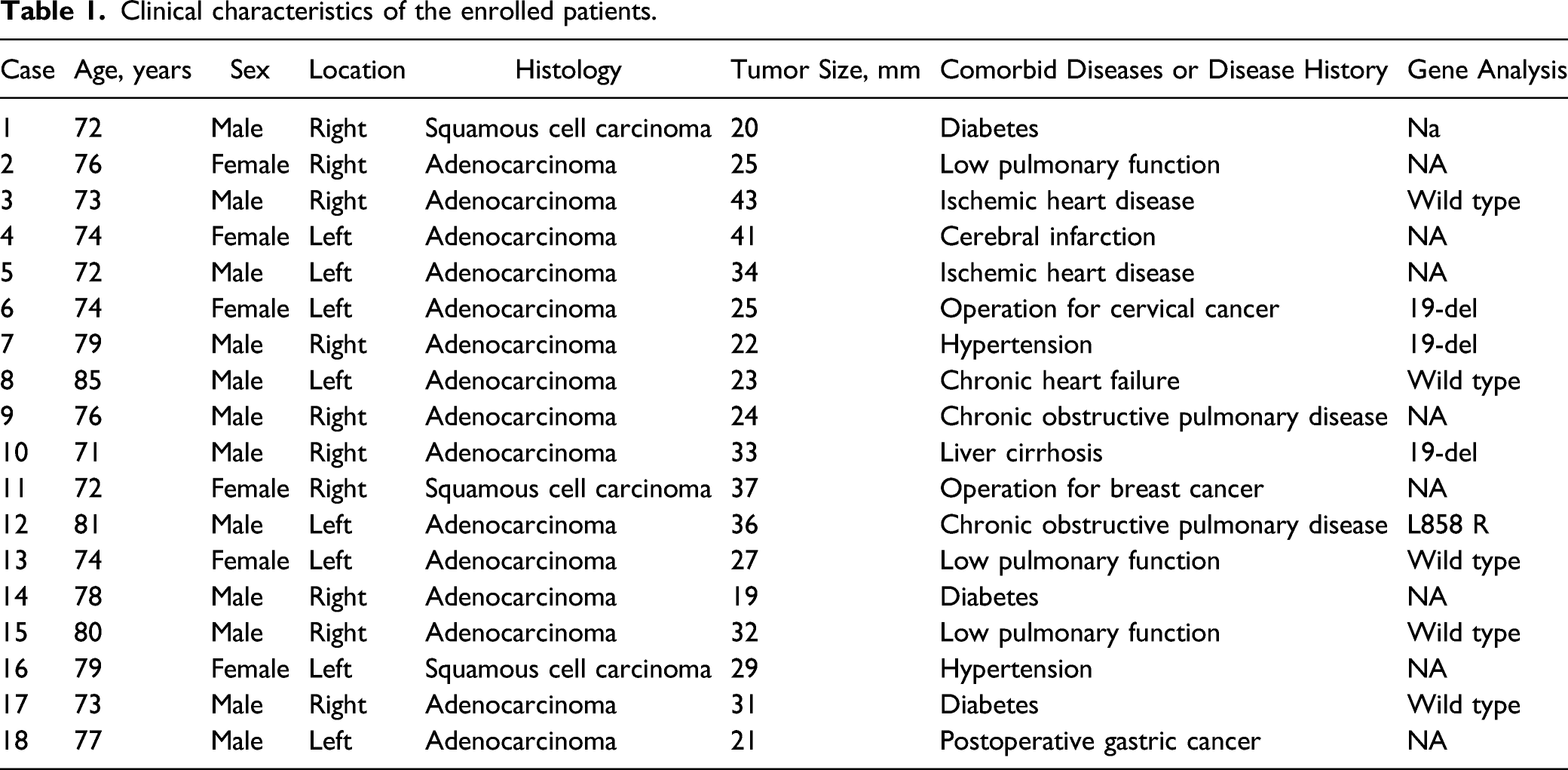
Three patients (cases 6, 11, and 18) had a history of prior surgery for cervical, breast, and gastric cancer, respectively, and refused thoracic surgery. The remaining patients were considered to have medically inoperable NSCLC due to coexistence of pulmonary, cardiovascular, and other medical comorbidities (five cases due to impaired pulmonary function, three due to cardiovascular diseases, three due to diabetes, two due to hypertension, one due to liver cirrhosis, and one due to cerebral infarction). There were four cases of tumors positive for EGFR mutations (cases 6, 7, and 10 for 19-del, and case 12 for L858 R).
Local Control Rate of CT-Guided RFA
Responses to initial CT-guided RFA and clinical outcomes.

CR, complete remission; CT, computed tomography; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PR, partial remission; RFA, radiofrequency ablation; SD, stable disease.
Survival
The median follow-up period was 25 months, ranging from 11 to 45 months. Six patients died during the follow-up. The cause of death was lung cancer progression in three cases, pneumonia unrelated to lung cancer in two cases, and heart failure in one case. The PFS and OS are shown in Figure 1. The median PFS and OS did not reach. The PFS rate was 83.3% at 1 year, 64.9% at 2 years, and 51.9% at 3 years. The OS rate was 92.2% at 1 year, 81.5% at 2 years, and 54.3% at 3 years. Kaplan–Meier curves of progression-free (A) and overall (B) survival.
Complications
There was no treatment-related death. One patient developed symptomatic pneumothorax requiring thoracic drainage, and five patients required no treatment. No other major complications, such as bronchial bleeding, hematoma, or hemothorax, were observed. Minor complications included: chest pain in six patients, moderate-grade fever <38.5°C in five patients, and cough in two patients. Three patients developed pulmonary infection. Most of these complications were resolved within several days. The median hospital stay was 2 days (range, 1−4 days).
Discussion
This study summarized and analyzed the efficacy and toxicity of CT-guided RFA in older adults with early-stage lung cancer in our hospital. RFA treatment achieved good results with a DCR of 83.3%, a 3-year PFS rate of 51.9%, and a 3-year OS rate of 54.3%. . Our results suggest that CT-guided RFA has the potential to become an effective treatment for medically inoperable older adults with early-stage lung cancer.
The treatment of inoperable early-stage lung cancer is complicated. RFA is an effective local treatment, and its effectiveness has been confirmed for lung cancer. The survival rate of patients with clinical stage I NSCLC after RFA has been reported to be 78−100% at 1 year, 57−84% at 2 years, and 36−74% at 3 years.20,25,26 In our study, the patients had a median age of 75 years and severely impaired pulmonary function and/or considerable comorbidities; however, the survival rates were similar to those previously reported. Therefore, it can be stated that percutaneous RFA has found clinical application in patients with medically inoperable lung tumors with good reported results.
After the initial RFA, the local control rate in our study was 77.8%, and the local tumor progression rate was 22.2%, consistent with the results of previous studies.20,25,26 Cases 1, 2, and 4 with local recurrence underwent repeated ablation and achieved effective control again. It is worth mentioning that in our treatment, CT-guided RFA has achieved good therapeutic effects, which may be related to multi-tined electrodes. Multi-tined RFA helps to control the extent and shape of the ablation area. 27 Multi-tined is suitable for larger tumors (3-5 cm), while Mono-tined RFA is suitable for smaller tumors (tumors less than 3 cm). 28 A retrospective multicentric study compared mono-tined RFA with multi-tined RFA and concluded that multi-tined RFA was associated with a lower rate of local tumor recurrence, even in cases of small hepatocellular carcinoma. 29 For inoperable early-stage lung cancer, SBRT and RFA are both effective treatment options. Although SBRT can achieve a higher local control rate, the survival rates of the two treatments for early-stage lung cancer was similar. 30 A systematic review analysis found that SBRT had a 31% incidence of radiation pneumonitis. 31 For patients with poor lung function, particularly those with interstitial lung disease and chronic obstructive pulmonary disease (COPD), radiation pneumonitis increases the risk of death. 30 Therefore, for these patients, RFA is a good treatment option. It is suitable for lung tumors because the radiofrequency energy is trapped within the targeted tumor by the insulating effect of the air-filled lung tissue surrounding the tumor. 32 Since the electrode is placed percutaneously directly into the tumor under CT guidance, pneumothorax, which is an undesirable adverse event for patients with pulmonary function impairment, occurs infrequently.12,33 In our study, there were five cases with impaired pulmonary function, including COPD. Symptomatic pneumothorax requiring thoracic drainage occurred in one case, and in other five cases, it was only seen on imaging with no need for treatment. No other major complications were observed. Minor complications were resolved within several days. The mortality rate, major complication rate, and minor complication rate of lung RFA have been reported to be 0−5.6%, 3.0−24.5%, and 21.3−64.9%, respectively. 34 We reported a technical success of 100%, with no treatment-related mortality, and a low morbidity rate of complication. Our results indicated that percutaneous CT-guided RFA is a safe and efficient therapeutic approach for medically inoperable older adults with stage I NSCLC.
The difficulty in accurate response evaluation after RFA may be a clinical concern. The residual opacity on chest CT after RFA may include surviving malignant cells and RFA-induced inflammation, necrosis, or fibrosis. It is difficult to distinguish remaining viable tissue from the ablated area after RFA therapy. This situation is particularly prominent in patients with SD after RFA, according to RECIST. Therefore, in our study, SD was determined if there was disease stabilization as per CT findings for at least 3 months after RFA. Thus, serial CT scans are necessary during follow-up for patients receiving RFA treatment. Findings of multiple serial CT scans may provide more information regarding the response or local progression after RFA. One retrospective study showed that PET/CT after RFA could reflect the effect of RFA treatment early; 35 however, such conclusions required more supportive evidence, and the cost of therapeutic effect monitoring was too high.
It is well known that EGFR-TKIs have proven efficacy for advanced non-NSCLC with EGFR sensitive mutations. The long-term survival is significantly better with TKIs than with conventional chemotherapy with two drugs containing platinum. At present, TKI therapy is considered the standard first-line treatment for advanced non-NSCLC. It has been reported that TKI postoperative adjuvant therapy is beneficial to patients with completely resected NSCLC (stages IB, II, or IIIA). 36 The efficacy of TKI adjuvant therapy after RFA is unknown. In our study, three of four cases with positive EGFR gene mutation received TKI therapy after RFA. The target lesions of cases 6 and 12 remained as PR after the initial RFA, while that of case 7 showed SD. TKI therapy was maintained for 2 years. Their OS was 31, 25, and 34 months, respectively. Two patients died of pneumonia during follow-up. We cannot exclude the possibility that the pneumonia complications were not TKI-induced interstitial lung disease-type events. Nonetheless, we found that TKI adjuvant therapy is effective for patients who reached PR and SD after RFA. It is not clear whether there is a relationship between the occurrence of pneumonia complications and RFA combined with TKI therapy.
Our study has several limitations. First, this was a retrospective study with a limited number of patients and a relatively short follow-up period. Secondly, this was a single center study, which further reduces extrapolability of results to other institutions since RFA ablation technique is highly dependent on the experience and skills of operators. In addition, it was impossible to compare the efficacy of SBRT and RFA technology in the treatment of older adults with early-stage peripheral lung cancer at the same time. The main reason lied in the late application of SBRT technology in the treatment of early lung cancer in our center, and there are too few cases treated by SBRT. Furthermore, the enrolled patients were highly selected and treated with other therapies (TKIs, chemotherapy), which may have affected the efficacy analysis of RFA treatment.
Conclusion
Our study shows that CT-guided percutaneous RFA is safe and effective in medically inoperable older adults with stage I NSCLC. This technique could be an alternative therapeutic approach, particularly in older adults with early-stage peripheral lung cancer, which need more study to confirm in future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hainan Provincial Natural Science and Technology Foundation (Youth Project) of China (NO. 819QN369).
Author’s Note
These authors contributed equally to this work.
Ethics Statement
This study was approved by the Hospital Review Board of the First Affiliated Hospital of Hainan Medical University (No. HMU002173), Hainan, China.